



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
A Critical Access Hospital (CAH) is a federal Medicare designation for small rural hospitals that meet four criteria: 25 beds or fewer, 35-mile distance from other hospitals, 96-hour average stay, and 24/7 emergency services. Per HRSA Rural Health Information Hub data, approximately 1,380 CAHs operate across 45 states, serving communities that would otherwise lose inpatient access. The designation was created in 1997 to stop rural hospital closures. It has kept most small rural hospitals open. It has not made them financially healthy. The Rural Health Transformation Program now directs billions toward CAH modernization, shifting the economics again.
The Critical Access Hospital designation was not built to make rural hospitals thrive. It was built to stop them from closing.
The University of North Carolina’s Cecil G. Sheps Center for Health Services Research has tracked 153 rural hospital closures and conversions since 2010 (85 complete closures and 68 converted to non-acute care). CAHs account for the large majority of rural hospitals still open, a share that would have been smaller without the designation. Without CAH protection, the closure count would be significantly higher. The program works. Programs that work rarely get enough credit.
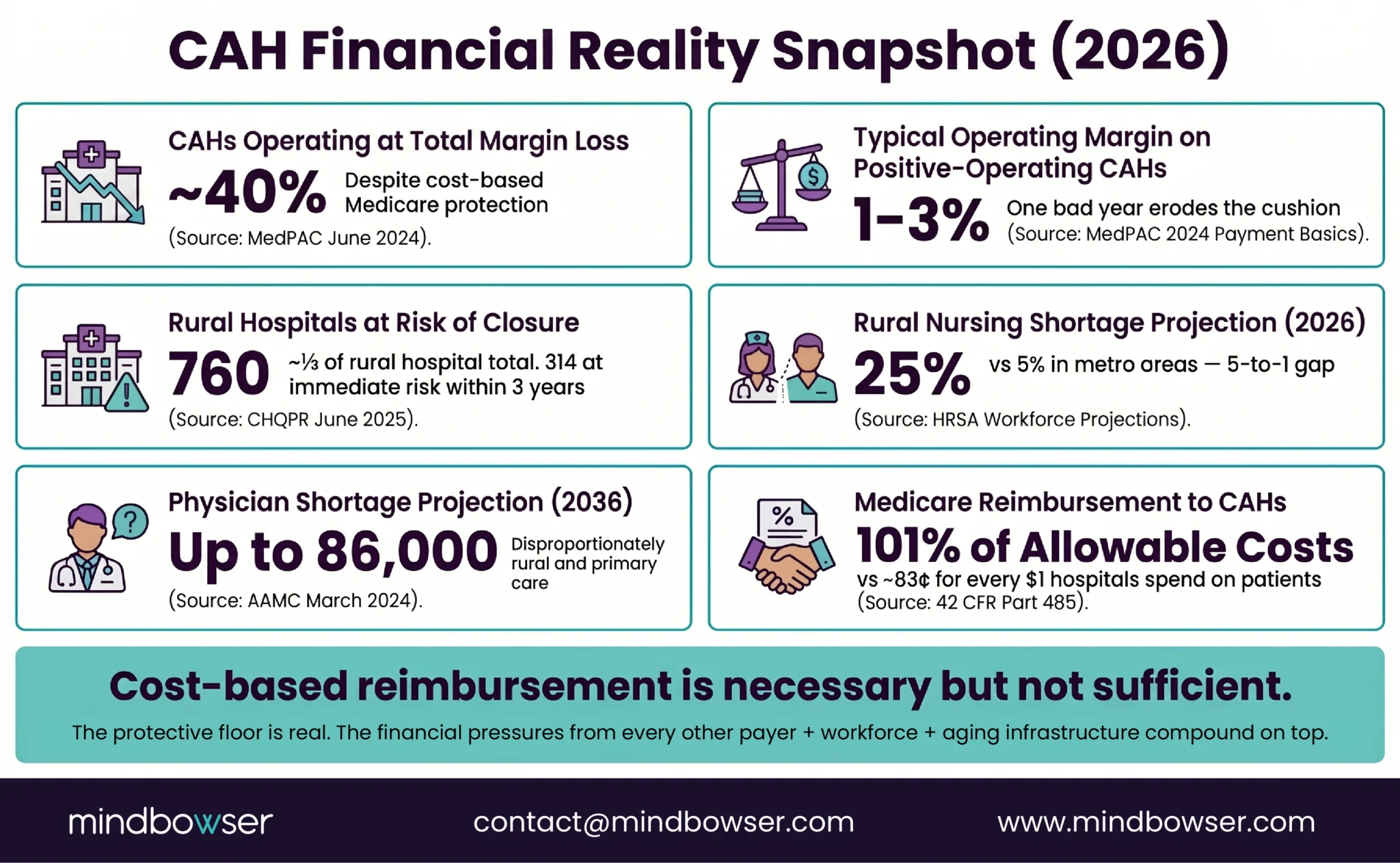
The program also has real limits. MedPAC’s 2024 Payment Basics analysis documented that while cost-based reimbursement provided the average CAH with approximately $4 million more per year on Medicare Fee-for-Service than it would have received under the Prospective Payment System, the average all-payer profit across CAHs was only $1 to $2 million annually, thin enough that a single bad year can push a facility into vulnerability. CHQPR (Center for Healthcare Quality and Payment Reform) estimates that 760 rural hospitals, roughly one-third of the rural hospital total , are currently at risk of closing, with 314 at immediate risk within three years. Cost-based Medicare reimbursement pays for today’s operations, not tomorrow’s modernization. A designation that keeps the doors open does not automatically pay for the EHR migration, the RPM program, or the AI scribe tools that determine whether a CAH can retain clinical staff.
That is the context for the current moment. The $50 billion Rural Health Transformation Program (RHTP), authorized in 2025 and now flowing to all 50 states, targets CAHs as primary stakeholders. Every state’s RHTP plan includes CAH-specific activities. For the first time since 1997, the federal government is funding what cost-based reimbursement cannot: the technology and facility investments that decide whether rural hospitals survive the decade. The scale of the RHTP funding must be read alongside the reconciliation law’s approximately $137 billion reduction in federal Medicaid spending in rural areas over the same decade, per KFF’s (formerly Kaiser Family Foundation) November 2025 analysis, RHTP is partial offset, not net new capital.
This guide covers what a Critical Access Hospital is, how the designation came to be, the exact requirements, how reimbursement works, the current state of the approximately 1,380 CAHs operating today, the challenges they face in 2026, and how RHTP funding is changing the technology economics.
What Is a Critical Access Hospital?
A Critical Access Hospital (CAH) is a federal Medicare designation for small rural hospitals that receive cost-based Medicare reimbursement in exchange for meeting strict operational criteria. CAHs must maintain 25 or fewer acute care beds, be located more than 35 miles from another hospital, maintain an average patient stay under 96 hours, and provide 24/7 emergency services.
The designation is codified at 42 CFR Part 485 Subpart F (Conditions of Participation) and administered by CMS under the Medicare Rural Hospital Flexibility Program. Unlike most hospitals, which are reimbursed by Medicare through the Prospective Payment System (PPS), CAHs receive 101% of their allowable costs for inpatient and outpatient services delivered to Medicare beneficiaries.
The CAH designation differs from several adjacent rural hospital classifications:
- Rural Emergency Hospital (REH): A newer designation (effective 2023) that allows former CAHs to provide emergency and outpatient services without operating inpatient beds
- Rural Referral Center (RRC): Higher-volume rural hospitals that serve as regional hubs; larger than CAHs
- Sole Community Hospital (SCH): A PPS-based designation for rural hospitals that are the only provider in their service area
- Prospective Payment System (PPS) Hospital: Standard reimbursement model for non-CAH hospitals
A hospital’s designation determines its reimbursement rules, regulatory flexibility, and federal grant eligibility. CAH status is the most protective for small rural hospitals that meet the criteria, but it is also the most restrictive on growth (hence the 25-bed cap).
How Did the CAH Designation Come to Be?
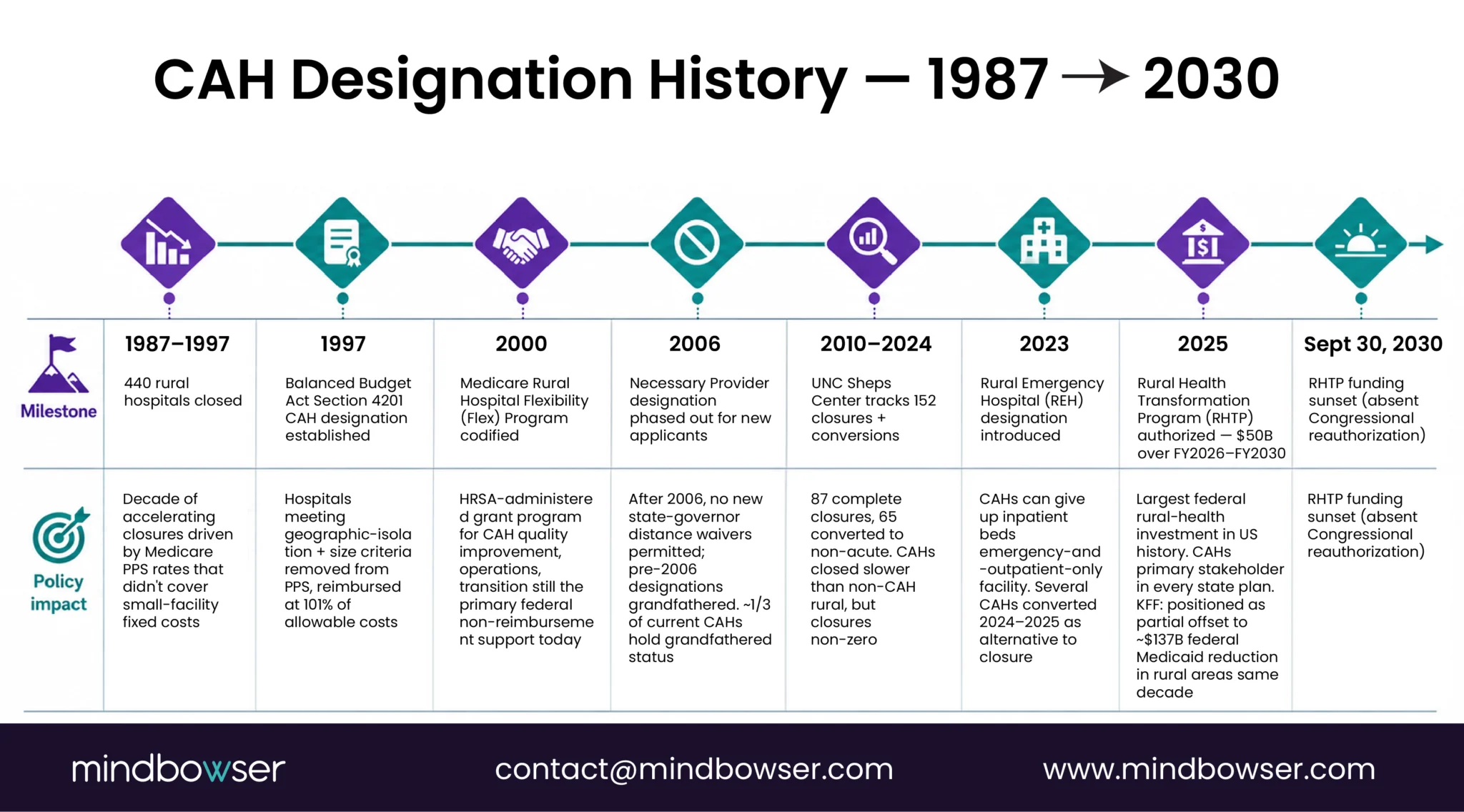
The Critical Access Hospital program was established under Section 4201 of the Balanced Budget Act of 1997. That legislation came at the end of a decade of accelerating rural hospital closures. Between 1987 and 1997, 440 rural hospitals closed, driven by Medicare PPS reimbursement rates that did not cover the fixed costs of maintaining small facilities with low patient volume.
The original policy logic was direct: rural America needed a minimum level of acute care access, and the market was not going to provide it at PPS rates. CAH was the response. Hospitals that met the geographic isolation and size requirements would be removed from PPS and reimbursed at cost. In exchange, they accepted the 25-bed cap and the 96-hour average stay requirement (both designed to keep CAHs functioning as stabilization-and-transfer facilities rather than full-service acute care).
Three policy evolutions shaped the program after 1997:
- 2000: Medicare Rural Hospital Flexibility Program (Flex) codified. Federal grant program administered by HRSA to support CAH quality improvement, operations, and transition. Flex funding is the primary federal non-reimbursement support CAHs access today.
- 2005-2006: Necessary Provider status phased out for new applicants. Before 2006, state governors could designate a hospital as a Necessary Provider, waiving the 35-mile distance requirement. After 2006, no new Necessary Provider designations are permitted, though existing designations continue. This matters because roughly a third of current CAHs hold Necessary Provider status and could not qualify as CAHs under the strict distance rule today.
- 2023: Rural Emergency Hospital (REH) designation introduced. REH allows CAHs and rural PPS hospitals to give up inpatient beds and become emergency-and-outpatient-only facilities. Several CAHs converted to REH in 2024-2025 as an alternative to closure. This is a consequential fork in the rural hospital roadmap: CAHs that cannot make the economics work now have a graceful exit from inpatient care.
- 2025: Rural Health Transformation Program (RHTP) authorized. The $50 billion program is the largest federal investment in rural health infrastructure in US history. CAHs are a primary stakeholder in every state RHTP plan. We cover the RHTP implications for CAHs in detail in our Rural Health Transformation Program guide.
What Are the Requirements to Qualify?
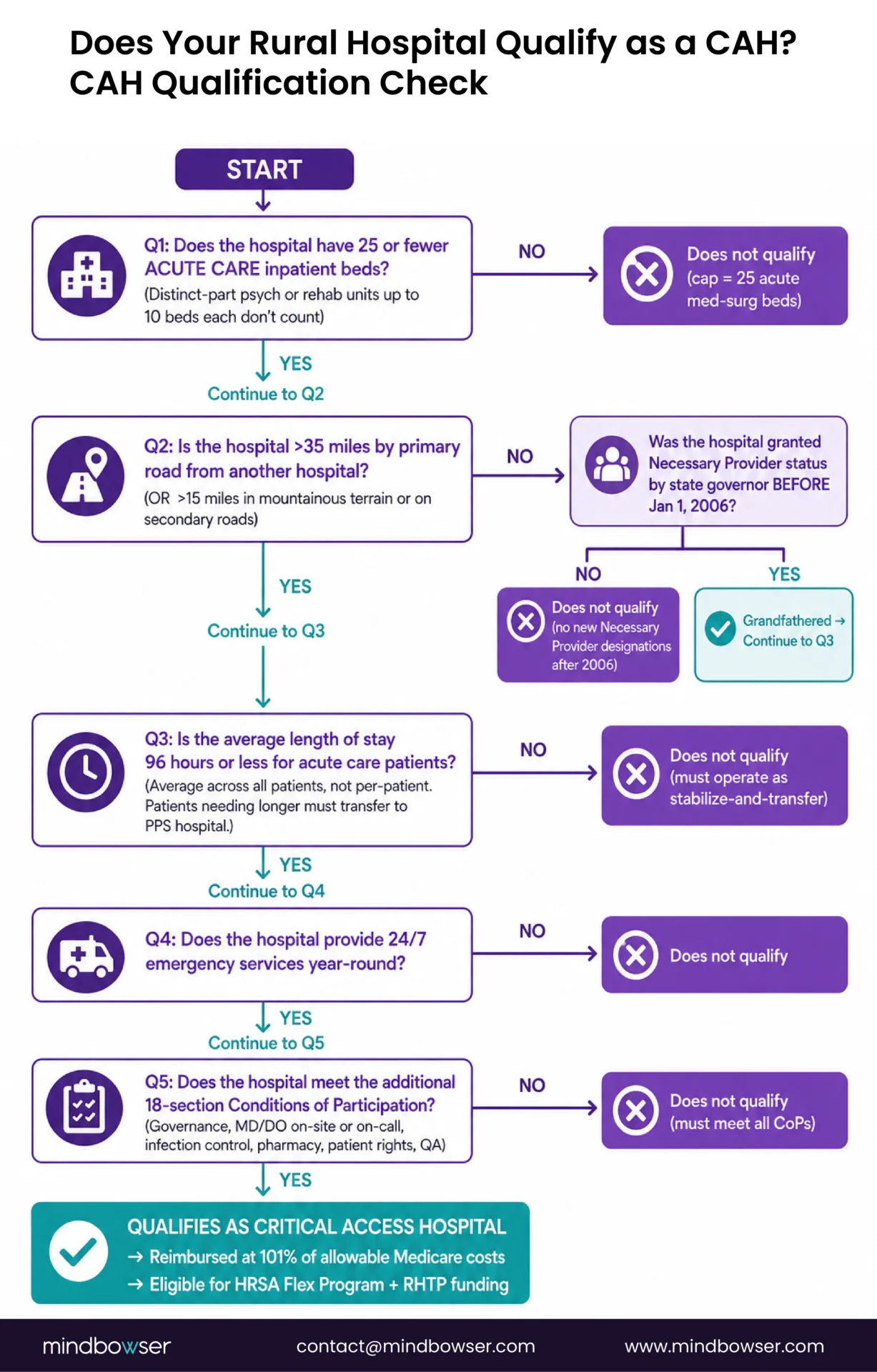
Critical Access Hospital status requires meeting four core criteria, codified at 42 CFR Part 485 Subpart F. All four apply simultaneously.
- 25 or fewer acute care inpatient beds: Psychiatric or rehabilitation distinct-part units (up to 10 beds each) do not count against the 25-bed cap. The cap applies to acute medical-surgical beds only.
- More than 35 miles by primary road from another hospital, or more than 15 miles in mountainous terrain or on secondary roads: Distance is measured point-to-point between facilities. Hospitals that received Necessary Provider designation from their state governor before January 1, 2006 are grandfathered under the waived distance rule.
- Average length of stay of 96 hours or less for acute care patients: This is the most operationally consequential rule. Patients requiring longer stays must be transferred to a PPS hospital. This shaped CAH operations into stabilize-and-transfer models rather than long-term acute care.
- 4. 24/7 emergency services: CAHs must maintain emergency coverage year-round, which drives a significant share of their operating cost burden.
Additional Conditions of Participation cover governance, staffing (minimum of one MD or DO available for on-site or on-call coverage), infection control, pharmacy services, patient rights, and quality assurance programs. The full Conditions of Participation run 18 sections under 42 CFR Part 485 Subpart F.
Does a Critical Access Hospital Have an ICU?
CAHs generally do not maintain dedicated ICU units, though they may provide intensive-care-level monitoring in specific beds. The 96-hour stay limit and 25-bed cap work against sustaining a full ICU. Patients requiring ICU care are typically stabilized and transferred.
How Are Critical Access Hospitals Reimbursed?
Medicare reimbursement is the financial foundation of the CAH model. The mechanics matter more than most non-healthcare readers realize.
- Cost-based reimbursement at 101%: Medicare pays CAHs 101% of their reasonable costs for services delivered to Medicare beneficiaries, per MedPAC’s 2024 Payment Basics publication on CAHs. This differs fundamentally from PPS hospitals, which receive fixed payments per Diagnosis-Related Group regardless of actual cost.
- What cost-based reimbursement covers: Labor, supplies, utilities, depreciation on existing capital equipment, and administrative overhead allocated to Medicare services. The 1% above cost is intended to provide a small operating margin.
- What cost-based reimbursement does not cover: New capital investment in facilities or major equipment. Technology investments that are capitalized rather than expensed. Growth beyond the Medicare service volume. The cost-plus-1% math works for maintaining today’s operations, not for building tomorrow’s capabilities.
- The commercial payer mix matters enormously: CAHs that serve a higher share of Medicare patients get more benefit from cost-based reimbursement. CAHs in commercially insured service areas effectively subsidize their Medicare operations with commercial revenue. The payer mix is the hidden variable that determines whether a CAH operates at a surplus, breaks even, or loses money.
- Medicaid and commercial payers: CAHs negotiate separately with Medicaid programs (rates vary by state) and commercial insurers (rates vary by contract). Cost-based reimbursement is a Medicare construct. It does not extend to other payers.

For a deeper analysis of the financial mechanics, including how technology investments intersect with cost-based reimbursement, see our Critical Access Hospital reimbursement and ROI guide.
Need help modernizing your Critical Access Hospital technology and reimbursement strategy?
How Many Critical Access Hospitals Exist and Where?
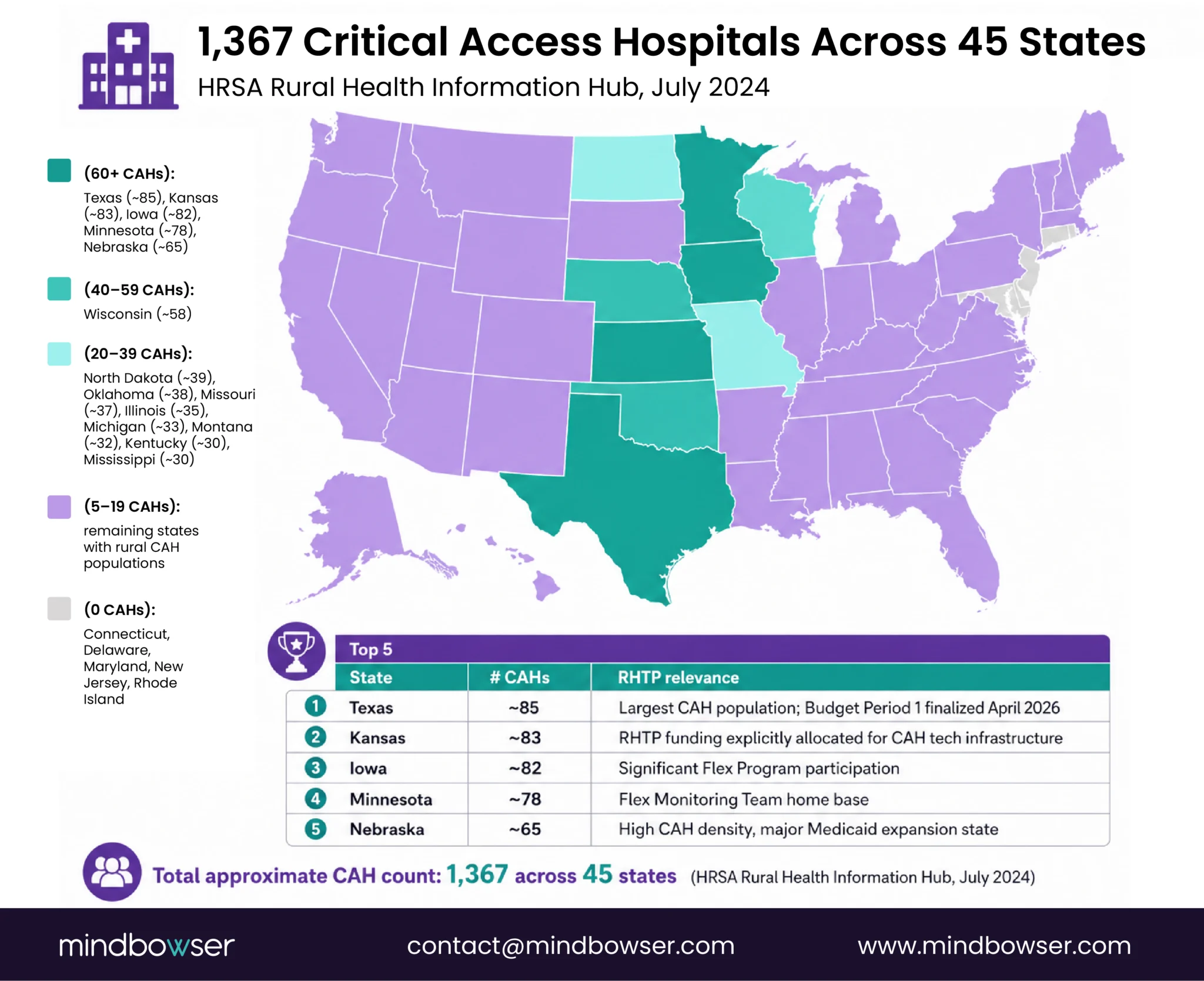
The Flex Monitoring Team (a joint project of the University of Minnesota, University of North Carolina, and University of Southern Maine) maintains the authoritative list of CAHs. As of 2024-2025 tracking, approximately 1,380 CAHs operate across 45 states.
Largest CAH populations by state:
- Texas (~85 CAHs)
- Kansas (~83)
- Iowa (~82)
- Minnesota (~78)
- Nebraska (~65)
- Wisconsin (~58)
- North Dakota (~39)
- Missouri (~37)
States with no CAHs: Connecticut, Delaware, Maryland, New Jersey, Rhode Island (all predominantly urban states without rural communities meeting the geographic isolation criteria).
Trend: Net closures continue despite the designation. CAHs have closed at a slower rate than non-CAH rural hospitals since 2010, but closures are not zero. Some former CAHs converted to Rural Emergency Hospital (REH) status rather than closing entirely.
What Challenges Do CAHs Face in 2026?
The Medicare Payment Advisory Commission June 2024 Report to Congress documented the operating reality most CAH administrators know firsthand.
- Financial fragility: About 40% of CAHs operate at a loss in any given year. The margin on positive-operating CAHs is typically 1-3%. One bad year erodes the cushion.
- Workforce shortages: Most CAHs operate with 1-2 IT staff, zero to two full-time specialists outside primary care, and rotating physician coverage. HRSA projects a 25% rural nursing shortage by 2026 versus 5% in metro areas, and Association of American Medical Colleges (March 2024) projects up to 86,000 physician shortage by 2036 with rural disproportionately affected. The hiring market for rural clinical staff is structurally tight, and has been tightening since 2020.
- Aging infrastructure: Many CAHs operate in facilities built in the 1960s-1970s. Aging HVAC, plumbing, and structural issues require capital investment that cost-based reimbursement does not fund.
- Reimbursement mechanics: Cost-based at 101% is protective but limiting. A CAH that grows its commercial patient base cannot expand beyond 25 beds without losing designation. A CAH that wants to add service lines faces capital constraints.
- Regulatory complexity: Conditions of Participation require documentation and compliance capacity that small administrative teams struggle to maintain. Audits can surface issues that drive certification risk.
- Patient volume instability: Rural populations are aging and, in many communities, declining. A 10% decline in population translates into a larger decline in hospital admissions as healthier residents leave and the remaining population has higher chronic disease burden but lower inpatient needs.
UNC Sheps Center, Center for Healthcare Quality and Payment Reform (CHQPR), and AHA’s annual rural reports track these trends. The consistent finding: rural hospitals are fragile and getting more fragile, despite the protective effect of the CAH designation. CHQPR data shows 760 rural hospitals at risk of closure and 314 at immediate risk.
How Does Technology Change CAH Economics?
Technology does not rescue a CAH. It does shift where the margin is.
Why technology is complicated for CAHs: Capital investment is not recovered through cost-based reimbursement at the rate of deployment. The 101% of costs formula captures depreciation, but not the capital intensity required to modernize an aging technology stack. This is why CAHs historically underinvest in IT, and why the RHTP funding matters.
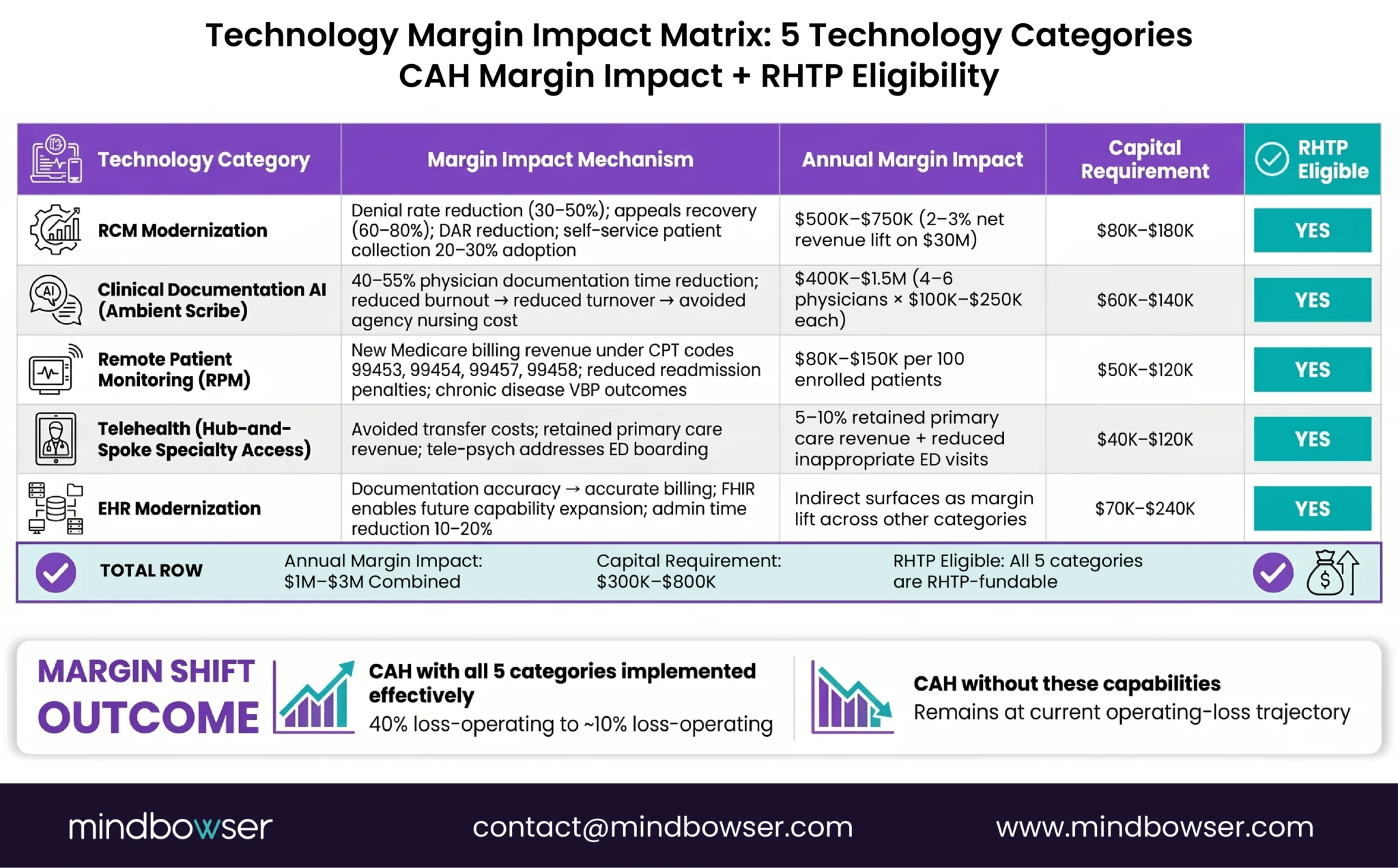
Where technology produces measurable margin impact:
- Revenue cycle management (RCM) modernization: Automated claims submission, denial management, and patient financial services reduce write-offs and speed cash collection. A 2-3% improvement in net revenue from RCM upgrades is typical for small hospitals moving from legacy to modern RCM platforms.
- Clinical documentation AI: Ambient AI scribe tools reduce clinical documentation burden and physician note time significantly, based on KLAS pilot reporting and internal deployment observations, and our own AI Medical Summary deployments. For a CAH that cannot recruit a second physician, saving two hours per physician per day is the difference between staffing sustainability and burnout-driven turnover.
- Remote Patient Monitoring (RPM): CAHs can participate in Medicare RPM billing (Current Procedural Terminology 99453-99458) for chronic disease management, capturing reimbursement that cost-based rates do not cover. Cellular-enabled devices work for rural patients without broadband.
- Telehealth for specialty coverage: Hub-and-spoke telehealth arrangements extend specialty access to CAH patients without the CAH adding specialists to payroll. This preserves primary care revenue at the CAH while improving outcomes.
- EHR modernization: Most CAHs run MEDITECH Expanse, Epic Community Connect, Athena, or eClinicalWorks. Fast Healthcare Interoperability Resources R4 API exposure (mandatory July 2026 for certified health IT) enables integration work that older CAH systems cannot support natively. The path from legacy EHR to FHIR-enabled clinical workflows requires either middleware or migration, neither of which cost-based reimbursement covers.
- HIPAA and cybersecurity infrastructure: Managed security operations are table stakes but operationally hard for a 1-IT-person hospital. PHISecure and similar managed platforms handle compliance posture without a full internal team.
The throughline: technology shifts the margin at the edges. A CAH that gets all five technology categories right can move from 40% loss-operating to 10% loss-operating, which is a meaningful survival margin. A CAH that gets them wrong stays where it is.
For the specific technology stack recommendations, see our technology stack for a 25-bed rural hospital guide.
What Does RHTP Mean for Critical Access Hospitals?
The Rural Health Transformation Program is the most consequential thing to happen to CAHs since the 1997 designation itself.
Every state’s RHTP plan names CAHs as a primary stakeholder. Most state plans include specific initiatives targeting CAH modernization: EHR integration with state Health Information Exchange systems, RPM infrastructure expansion, telehealth hub build-outs, workforce retention programs, and facility modernization grants.
State examples:
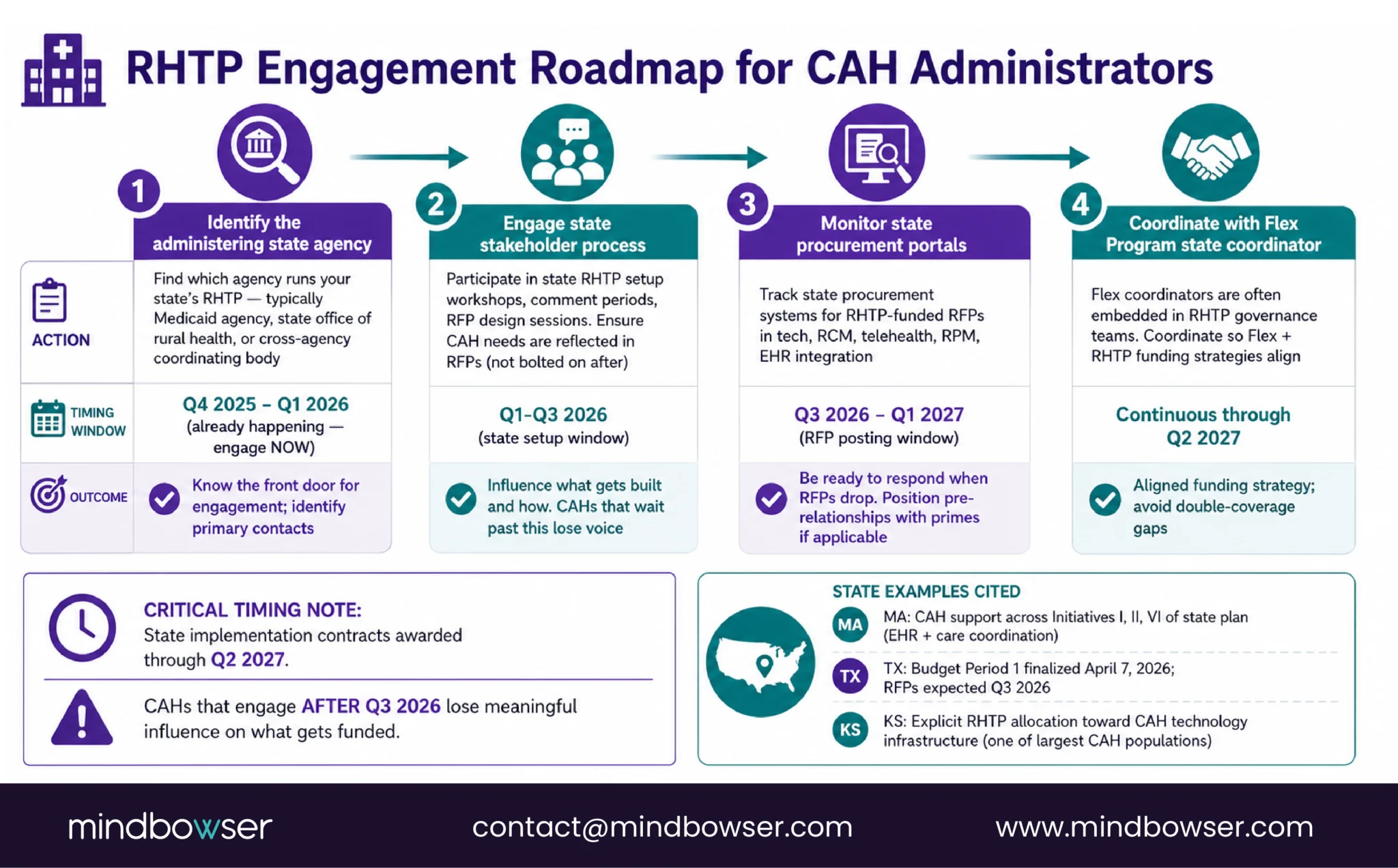
- Massachusetts lists CAH support across Initiatives I, II, and VI of its plan, with specific technology assistance for CAH EHR modernization and care coordination platform integration
- Texas’s approved Budget Period 1 (finalized April 7, 2026) includes RFPs expected for rural hospital technology investment beginning Q3 2026
- Kansas, which has one of the largest CAH populations in the country, explicitly allocates RHTP funding toward CAH technology infrastructure
What CAH administrators should do:
- Identify the state agency administering your state’s RHTP program (typically the Medicaid agency, state office of rural health, or a cross-agency coordinating body)
- Engage the state’s stakeholder process during the Q1-Q3 2026 setup window to ensure CAH needs are reflected in RFPs
- Monitor state procurement portals for RHTP-funded RFPs starting Q3 2026
- Coordinate with Flex Program state coordinators, who are often embedded in RHTP governance teams
The procurement window is finite. States will post RFPs between Q3 2026 and Q1 2027, with implementation contracts awarded through Q2 2027. CAHs that wait past this window to engage lose influence on what gets built and how.
How Mindbowser Supports CAH Technology Modernization
Mindbowser builds custom healthcare technology for small and rural hospitals whose constraints exceed what off-the-shelf platforms accommodate. Our work with small hospital deployments has produced a stack of accelerators that match CAH operational reality:
- HealthConnect CoPilot handles rural EHR integration across MEDITECH Expanse, Epic Community Connect, Athena, and eClinicalWorks. FHIR-based data exchange lets CAHs meet United States Core Data for Interoperability v3 compliance (mandatory July 2026) without replacing their legacy EHR.
- WearConnect provides device-agnostic RPM infrastructure with cellular-first connectivity, which works for rural patients without broadband. The abstraction layer supports 14 device manufacturers, so a CAH is not locked into a single vendor.
- AI SummaryAssist reduces clinical documentation time by 40-55% per encounter. For a CAH with one or two physicians covering nights and weekends, this capacity is survival-level.
- PHISecure covers HIPAA-compliant cloud infrastructure and managed security operations for small hospitals without in-house security teams.
Typical engagement model: 12-16 week Minimum Viable Product builds that go live fast and scale from there. Payment can be structured against RHTP-funded state contracts or traditional hospital capital budgets, depending on funding source.
The Future of Rural Hospitals Depends on What Happens Next
Critical Access Hospitals were created to keep rural hospitals from closing, and nearly three decades later, that mission still matters. While cost-based reimbursement has helped many CAHs survive, it has not solved the deeper challenges of aging infrastructure, workforce shortages, thin margins, and outdated technology systems. The Rural Health Transformation Program now creates a rare opportunity for CAHs to modernize through investments in interoperability, telehealth, RPM, clinical AI, and revenue-cycle infrastructure that were previously out of reach for many rural facilities. The hospitals that move early on modernization and state RHTP engagement will be better positioned to strengthen care access, improve operational stability, and remain long-term healthcare anchors for their communities.
A Critical Access Hospital (CAH) is a federal Medicare designation for small rural hospitals that meet four criteria: 25 or fewer acute care beds, 35-mile distance from other hospitals (or 15 miles in mountainous terrain), 96-hour average patient stay, and 24/7 emergency services. CAHs receive Medicare reimbursement at 101% of allowable costs rather than through the Prospective Payment System. The designation was established in 1997 to prevent rural hospital closures.
Three differences define the CAH classification. First, regulatory: CAHs operate under 42 CFR Part 485 Subpart F, a distinct set of Conditions of Participation that includes the 25-bed cap, 35-mile distance, and 96-hour average stay. Regular (PPS) hospitals have no such caps. Second, financial: CAHs receive cost-based Medicare reimbursement (101% of allowable costs), while regular hospitals receive fixed payments per Diagnosis-Related Group regardless of actual cost. Third, operational: CAHs function primarily as stabilize-and-transfer facilities for acute care, while regular hospitals manage the full range of inpatient durations.
A CAH is limited to 25 or fewer acute care inpatient beds. Distinct-part psychiatric or rehabilitation units (up to 10 beds each) do not count against the 25-bed limit. The cap applies to acute medical-surgical beds only and is a hard requirement of CAH designation.
CAHs receive Medicare reimbursement at 101% of reasonable costs for services provided to Medicare beneficiaries, per 42 CFR Part 485 Subpart F. This differs from non-CAH hospitals, which receive fixed Diagnosis-Related Group payments under the Prospective Payment System. Medicaid and commercial payer rates are negotiated separately and are not cost-based. Full payment mechanics are documented in MedPAC’s Payment Basics publication on CAHs.
CAHs do not make money in the traditional margin-expansion sense. Cost-based Medicare reimbursement at 101% produces a small operating margin (1% ) on Medicare services, plus whatever margin they generate from commercial and Medicaid patients. About 40% of CAHs operate at a loss in any given year despite cost-based reimbursement. The Medicare Rural Hospital Flexibility (Flex) Program provides federal grant funding to supplement operations. The Rural Health Transformation Program (RHTP) now provides additional capital for CAH modernization.
The primary benefit is cost-based Medicare reimbursement, which pays for the fixed costs of maintaining a small rural hospital that PPS rates would not cover. Secondary benefits include eligibility for the Medicare Rural Hospital Flexibility (Flex) Program grants, 340B drug pricing participation, regulatory flexibility on certain Conditions of Participation, and federal grant priority for rural health initiatives. The RHTP funding flowing to states in 2026 adds a new benefit tier: CAH-specific modernization investment.
The 96-hour rule requires CAHs to maintain an average length of stay of 96 hours or less for acute care patients. The rule applies to the average across all acute care patients, not to individual patients. Patients requiring longer stays are typically stabilized and transferred to a Prospective Payment System hospital. The rule shapes CAH operations into stabilize-and-transfer models rather than long-term acute care.
Yes. The CMS Acute Hospital Care at Home waiver explicitly allows CAH participation, and several CAHs operate H@H programs under the waiver (extended through September 2030). Technology platform requirements account for CAH-specific constraints: cellular-enabled RPM devices, operationally simple dashboards, managed cloud infrastructure that does not require a DevOps team. RHTP funding in multiple states covers CAH H@H program launches. See our Hospital at Home technology platform guide for the full architecture. This page references the following primary federal sources. All citations link directly to the official Federal Register, CFR, or agency record.
