



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
A 25-bed rural hospital running a Medicare chronic care management program with 200 enrolled patients needs the work of three full-time care coordinators and usually has only one. AI now replaces three specific workflow FTEs: intake coordinator, documentation specialist, and patient outreach FTE, without replacing clinical judgment. The math, the mechanisms, and the Rural Health Transformation Program funding pathway are below.
Opening: The “We’re Integrated” Conversation
I have integrated rural hospital EHRs fourteen times, and every single deployment started with the same conversation: the CMIO says their EHR is “integrated,” and by the end of day one, we have confirmed that what they meant is the EHR exports CSVs to a shared drive at 2 a.m. nightly. Someone manually reviews them in the morning. Sometimes.
This used to be a tolerable arrangement. A rural CAH with 25 beds, 200 chronic care management enrollees, and one IT person on staff could explain to the payer auditor that “integration” meant a batch job. The auditor shrugged. The PHI technically moved. Billing got done.
That era ends on July 1, 2026. ONC’s USCDI v3 mandate goes into effect, the 21st Century Cures Act information blocking rule has teeth the enforcement team is now willing to use, and state RHTP program offices are scoring technology proposals on actual integration capability. A CSV shared drive does not pass USCDI v3. It does not produce FHIR R4 resources. It does not support SMART on FHIR launches. And any rural hospital applying for RHTP technology funding in Q3 2026 will have their integration maturity scored against real standards, not vendor marketing claims.
The baseline to beat is lower than most vendors advertise. KLAS Research’s 2024 Arch Collaborative survey of more than 500,000 clinicians found only 44% agreed their EHR provides the level of integration with outside organizations that they expect, and clinician satisfaction with data sharing has barely moved since 2018. KLAS also documented that Epic Community Connect captured nearly 70% of rural and smaller-hospital EHR decisions in 2024, meaning most rural integration projects now have to fit Epic Community Connect affiliate constraints specifically rather than treat Epic as a generic vendor. That market concentration affects how integrations get scoped.
This is the piece I wish I had fourteen integrations ago. What rural EHRs actually run, how they actually integrate, where they actually break, and what RHTP pays for.
What EHRs Do Rural Hospitals Actually Run?
Urban hospitals run Epic and Cerner. Rural hospitals run a long tail.
Based on the market data I see in the rural CAH and RHC populations we work with, the approximate EHR distribution is:
- Meditech (Expanse, Magic, and Client-Server), roughly 22% of rural hospitals. The legacy Magic and Client-Server installs are a distinct integration problem from the modern Expanse deployments.
- Epic Community Connect, roughly 20%. Affiliate installs sharing the Epic instance of a regional anchor hospital. Different capabilities than standalone Epic.
- Cerner CommunityWorks, roughly 18%. Oracle Health’s rural-tier offering, SMART on FHIR capability improving.
- Athenahealth, roughly 15%. Cloud-native, strongest REST API maturity among the rural-common options.
- Praxis, Evident, NextGen, CPSI, others, roughly 25% combined. Proprietary APIs with varying FHIR support.
None of these run Epic’s standalone deployment patterns, and none of them should be assumed to behave like the Epic integration documentation suggests. The rural tier is where integration patterns get vendor-specific in ways the generic health IT vendor decks do not cover.
Why Rural EHR Integration Is Different (and Harder)
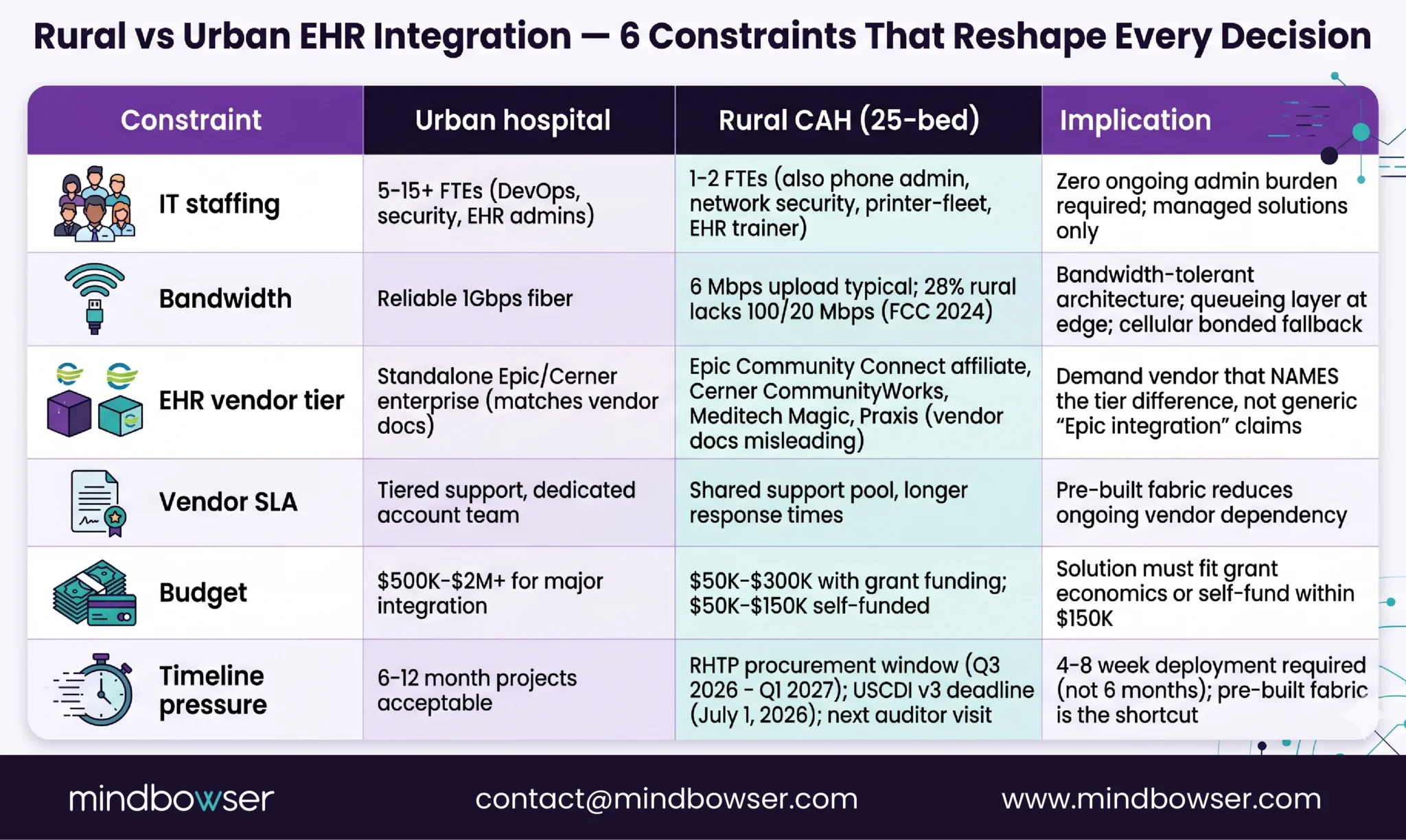
Picture the IT director at a 25-bed Critical Access Hospital at 3 p.m. on a Wednesday. She is the entire IT department. She is also the phone system administrator, the network security lead, the printer-fleet manager, and the person who trains new clinical staff on the EHR. When a vendor calls and wants “30 minutes on the Friday integration planning call,” she is balancing that against three other fires.
What rural EHR integration needs:
- Zero ongoing administration burden on the 1-2 IT FTEs rural hospitals actually have
- Bandwidth-tolerant architecture that does not assume reliable high-speed connectivity
- Compatibility with the specific EHR tier the hospital actually runs (not the enterprise tier the vendor sales team demos)
- HIPAA-grade PHI handling built in, not bolted on
- A timeline that matches the RHTP procurement window and grant-reporting deadlines, not the vendor’s six-month standard integration project
- An audit trail the next auditor will accept without a side call to the vendor
The rural-tier integration engines (Mirth Connect, Rhapsody at smaller scale, Iguana) and pre-built FHIR gateways exist precisely because the rural constraint set is different. Layering on top of the EHR’s native integration capability with a managed interop fabric is the architectural shortcut that compresses the timeline.
EHRConnect is the pre-built zero-code interop fabric that sits inside the hospital’s AWS VPC and turns the traditional 6-month EHR integration project into a 6-day one. It handles the Epic/Cerner/Athenahealth connection patterns natively and covers the mid-market tier with less custom work than a ground-up integration engine deployment. For rural hospitals, the deployment timeline compression is not a nice-to-have, it is the difference between launching a care management program before the next auditor visit and not launching at all.
FHIR R4 vs HL7 v2: What You Actually Translate Between
Every rural EHR integration conversation I have had in the last three years eventually arrives at the same technical reality: modern healthcare apps need FHIR R4 resources, most rural EHRs still natively speak HL7 v2, and the translation layer between them is where 80% of integration failures live.
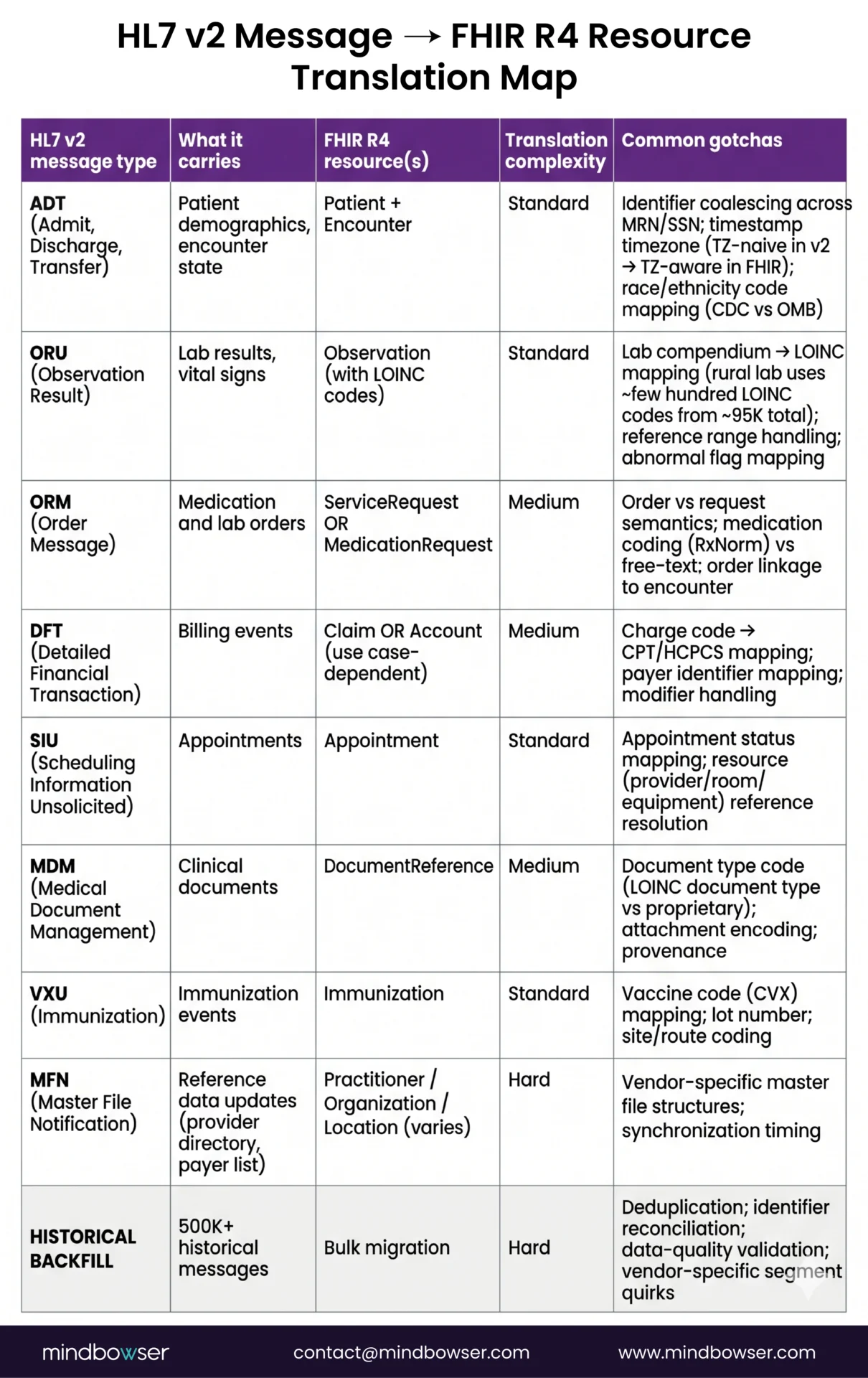
HL7 v2 messages the rural EHRs produce:
- ADT (Admit, Discharge, Transfer), patient demographics, encounter state. Translates to FHIR Patient, Encounter resources.
- ORU (Observation Result), lab results, vital signs. Translates to FHIR Observation resources with LOINC codes.
- ORM (Order Message), medication and lab orders. Translates to FHIR ServiceRequest or MedicationRequest.
- DFT (Detailed Financial Transaction), billing events. Translates to FHIR Claim or Account (depending on use case).
- SIU (Scheduling Information Unsolicited), appointments. Translates to FHIR Appointment.
- MDM (Medical Document Management), clinical documents. Translates to FHIR DocumentReference.
Translating a single ADT message to a conformant FHIR R4 Patient resource is not hard. Translating the hospital’s 500,000 historical ADT messages to FHIR Patient resources with deduplication, identifier reconciliation, and data-quality validation is a project. The difference is where most vendor integration demos quietly skip past.
HealthConnect CoPilot is the central interop fabric that handles the v2-to-FHIR translation as a managed capability, with pre-built profiles for the resource types rural EHRs produce. Custom ETL still matters for the historical backfill and the vendor-specific segment quirks, but the baseline translation is not something rural programs should rebuild from scratch.
Epic Community Connect Integration: The Reality
Rural hospitals running Epic Community Connect have a specific set of integration possibilities that are different from standalone Epic, and vendor documentation routinely conflates the two.
Workflow needs for a Community Connect integration
- Read access to patient demographics, problem list, medications, lab results, and care team assignments
- Write access for care plan updates, care management enrollments, and encounter notes where the parent Epic instance allows affiliate write-back
- SMART on FHIR launch context so clinician-facing apps can open in-chart
- Bulk data export for population-level reporting (CCM enrollments, HEDIS measures, RHTP reporting)
What Community Connect affiliates can actually do:
- Epic App Orchard registration, required for any third-party app launch. The parent Epic instance’s account typically sponsors the affiliate’s app registrations.
- FHIR R4 sandbox access, Epic’s sandbox supports R4 resource testing, but the specific resource availability depends on the parent instance’s Epic version and the App Orchard tier.
- Bulk FHIR (Flat FHIR), useful for population-level extracts. Rate-limited and often requires parent-instance IT team approval for each bulk export window.
- SMART on FHIR launch from the EHR, supported but requires App Orchard registration and parent-instance clinician permissions.
What Community Connect affiliates cannot do without parent instance coordination:
- Custom FHIR profile creation beyond the US Core profiles
- Webhook-style real-time subscription to clinical events
- Direct SQL access to the Caboodle data warehouse (that stays at the parent level)
- App Orchard production promotion without parent sponsorship
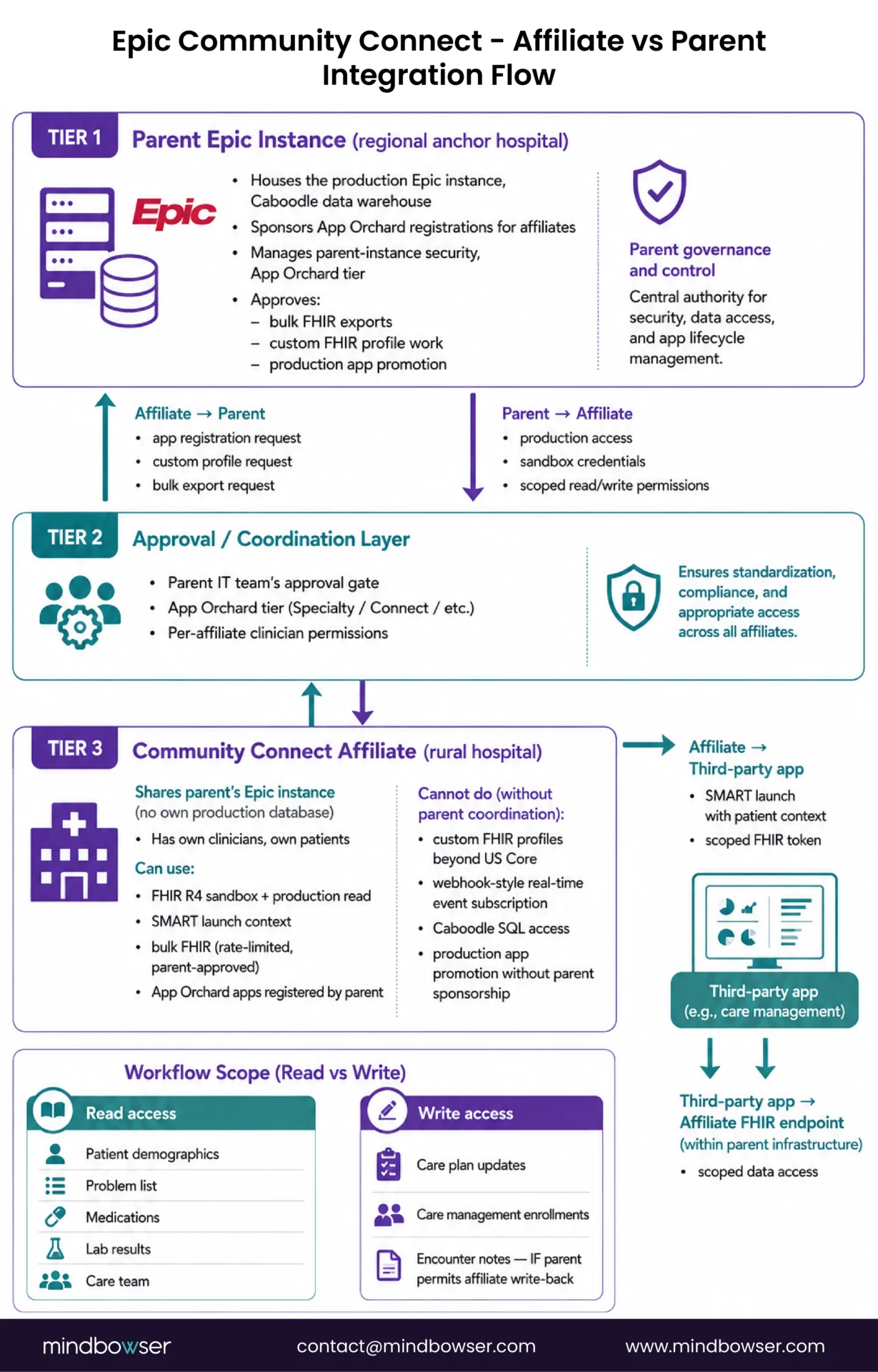
For a rural hospital evaluating an integration vendor, the question is not “can you integrate with Epic”, it is “can you integrate with Epic Community Connect as the affiliate, with our specific parent instance’s App Orchard tier.” Vendors that cannot name the difference between Community Connect and standalone Epic should not be shortlisted.
📥 Resource: EHRConnect, zero-code Epic Community Connect integration with pre-built SMART launch and bulk FHIR support.
Cerner CommunityWorks and Meditech: The Mid-Market EHR Stack
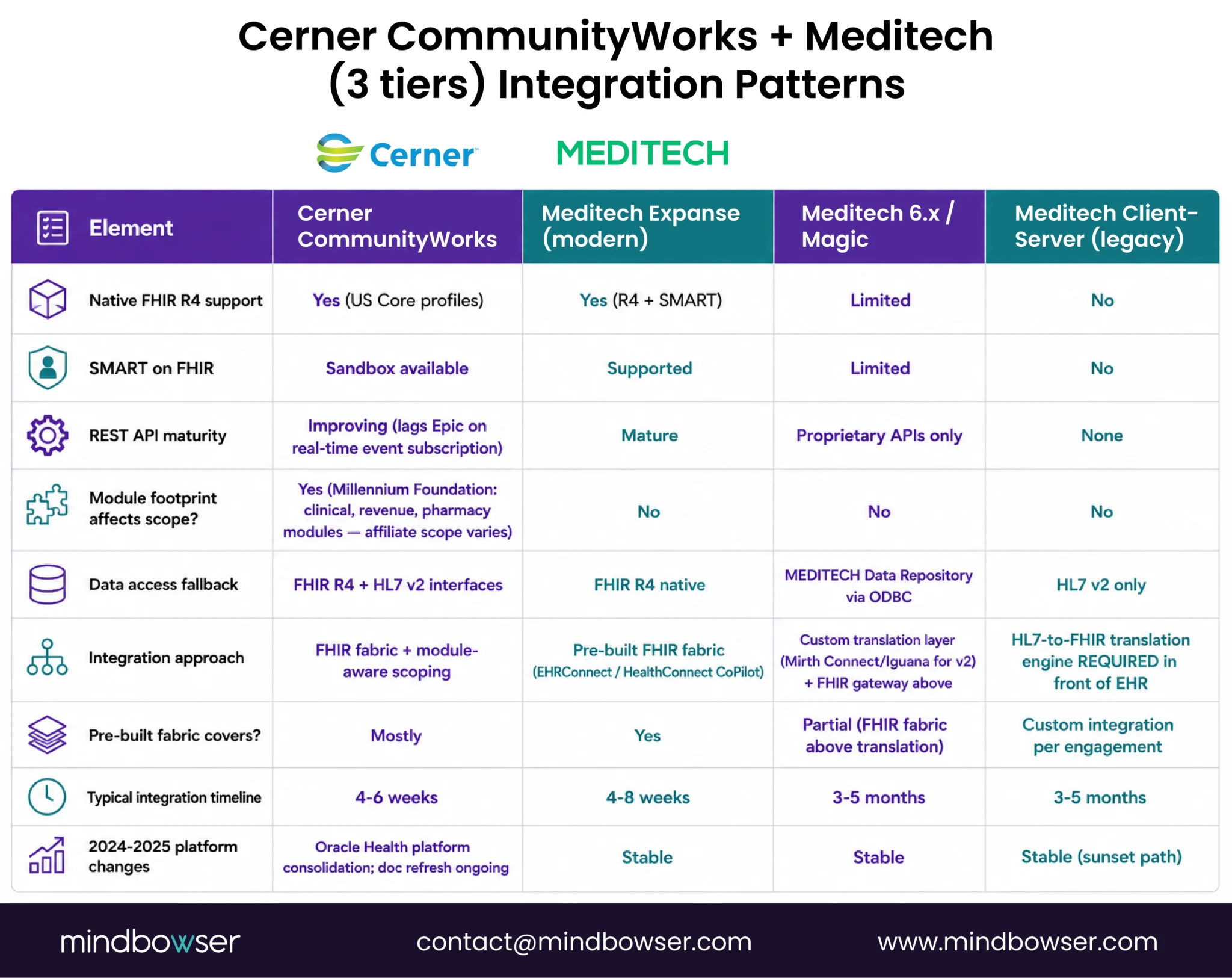
Cerner CommunityWorks (Oracle Health’s rural tier) and Meditech cover roughly 40% of rural hospitals between them, and each has integration quirks worth naming.
Cerner CommunityWorks:
- SMART on FHIR sandbox (cerner.com developer portal), improving steadily, though lags Epic App Orchard on real-time event subscriptions
- FHIR R4 support for US Core profiles
- Millennium Foundation requires identifying which modules the affiliate has enabled (clinical, revenue, pharmacy, etc.), integration scope varies by module footprint
- Oracle Health’s 2024-2025 platform consolidation has shifted some integration patterns; documentation refresh ongoing
Meditech, three distinct integration realities:
- Meditech Expanse (modern), FHIR R4 API, SMART on FHIR support, REST endpoints. The integration story that matches the vendor marketing.
- Meditech 6.x / Magic, proprietary APIs, MEDITECH Data Repository access via ODBC, limited FHIR support. Custom translation layer required.
- Meditech Client-Server (legacy), HL7 v2 interfaces only. No native FHIR. Integration requires an HL7-to-FHIR translation engine in front of it.
Rural hospitals running Meditech Magic or Client-Server installs face a bigger integration project than rural hospitals running Expanse. The legacy Meditech deployments are a custom-build scenario that no pre-built fabric covers end-to-end, the middleware layer (Mirth Connect, Iguana) handles the v2 side, and a FHIR gateway handles the modern app side.
No-accelerator step: Meditech Magic and Client-Server proprietary API work is custom integration per engagement. HealthConnect CoPilot covers the FHIR fabric above the translation layer, but the MEDITECH-specific segment quirks, repository schema mapping, and legacy API auth patterns are project work, not a product.
Athenahealth and Praxis: Cloud-Native and Legacy Proprietary
Athenahealth is the rural EHR with the cleanest modern integration story:
- Well-documented REST API (developer.athenahealth.com)
- FHIR R4 support with US Core profiles
- OAuth 2.0 authentication
- SMART on FHIR support
- Webhook subscriptions for key clinical events
- Sandbox environment that reliably matches production behavior
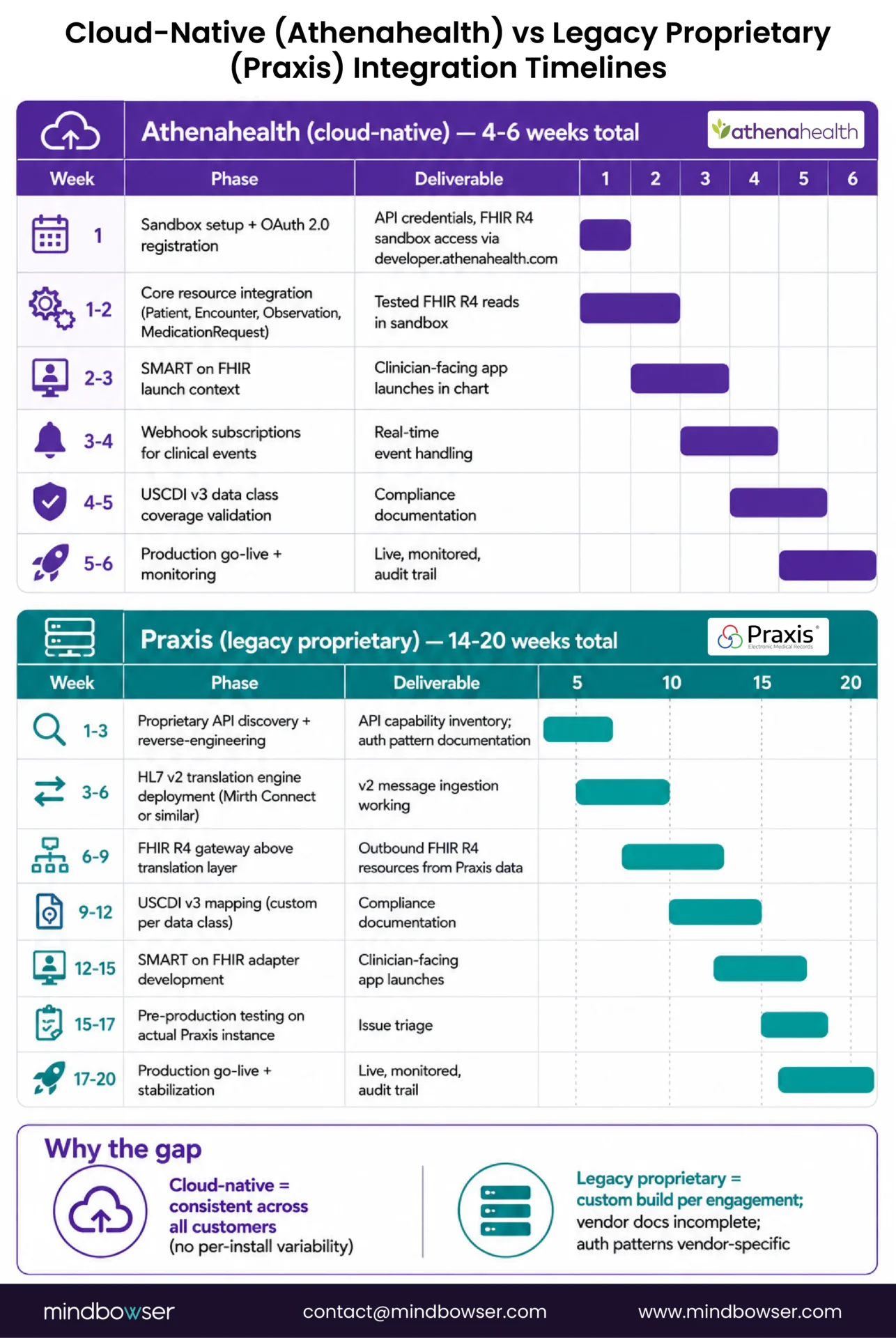
A rural hospital on Athenahealth can get a working FHIR-based integration up in weeks, not months. The cloud-native architecture means the integration patterns are consistent across all customers, there is no “your specific install quirks” problem because there is no on-premise variability.
Praxis and the small-vendor tail:
- Praxis, proprietary API with limited FHIR support. Integration requires custom work per use case.
- Evident / CPSI, partial FHIR support, mostly HL7 v2 for legacy interfaces. Mid-market rural tier.
- NextGen, FHIR R4 support varies by deployment; REST API matured in 2023-2024.
- Netsmart, ChartLogic, others, varying integration maturity. Evaluate case-by-case.
Rural hospitals on Praxis or similar proprietary EHRs face a longer integration runway than hospitals on Athenahealth. The custom integration work is not optional, it is the only path, and it is the kind of project that benefits most from a pre-built FHIR gateway on top, so the downstream apps consuming the integration do not have to be rewritten when the hospital eventually migrates to a FHIR-capable EHR.
📥 Resource: Patient Questionnaire Form, FHIR-compliant form data collection that works with any EHR in this stack via the HealthConnect CoPilot fabric.
Need help navigating rural EHR integration, FHIR interoperability, or USCDI v3 readiness?
SMART on FHIR Auth and OAuth 2.0: What Actually Works
If the EHR integration is the engine, SMART on FHIR is how clinician-facing apps hitch a ride.
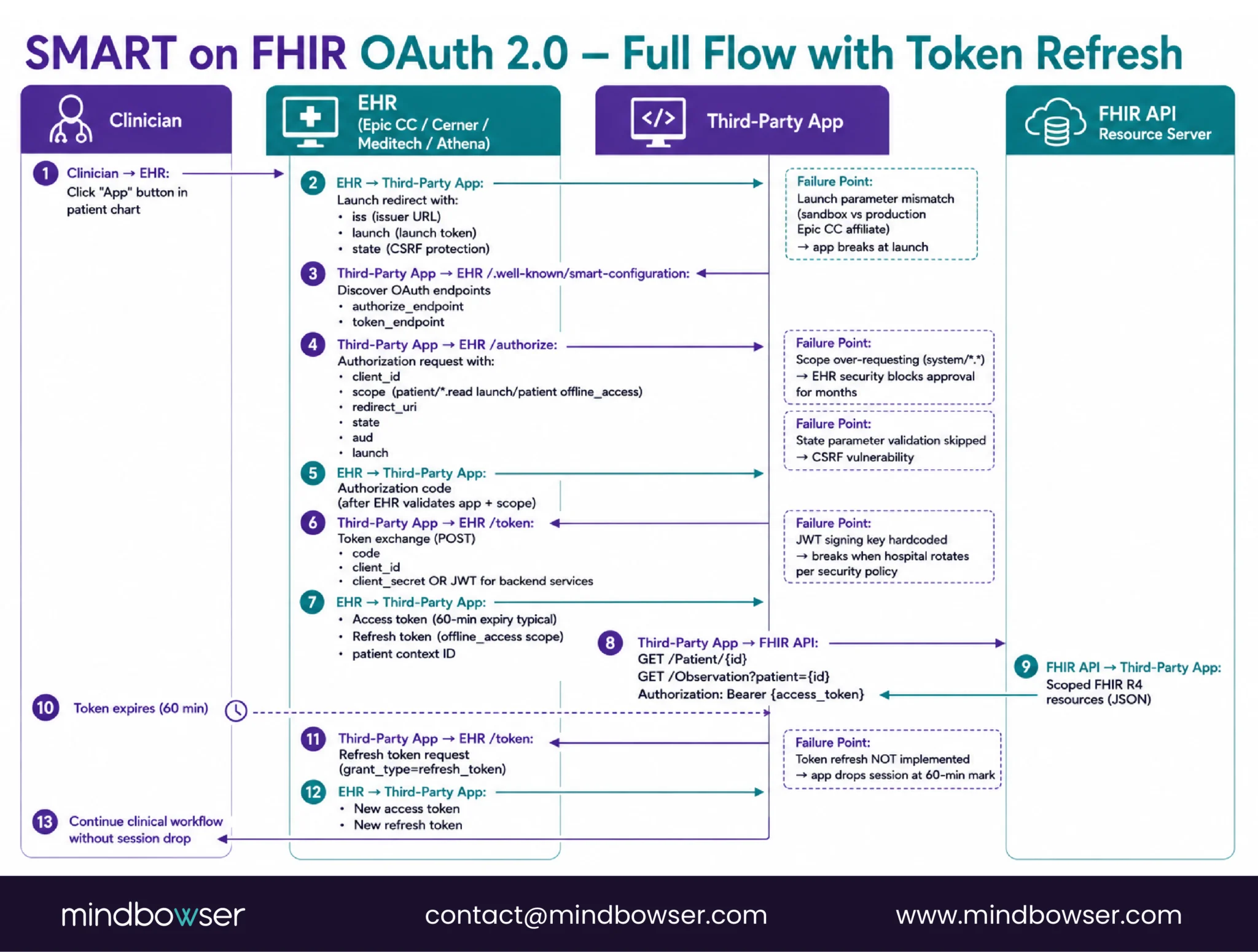
SMART 2.1 Implementation Guide defines two critical flows:
- EHR launch context, clinician clicks the app from within the EHR, EHR passes a launch token with patient context, app exchanges token for OAuth 2.0 bearer token, app has scoped access to that patient’s data.
- Backend services flow, service-to-service authentication for bulk data extracts and server-side integrations. Requires pre-registered JWT with public-key auth.
What rural integrations actually need to handle:
- Patient context launch from the EHR chart (clinician workflow)
- Backend bulk extract for population-level reporting (CCM panels, HEDIS measures, RHTP reports)
- Token refresh flow (access tokens expire; integrations that do not handle refresh drop sessions mid-encounter)
- Scope definition (what the app can read and write, typically
patient/*.read,launch/patient,offline_access, sometimesuser/Patient.read) - Launch parameter handling (especially
launch,iss,stateparameters)
Common failure modes I see at production:
- Token refresh not implemented, app works in demo, drops sessions in production after the first token expiry
- Scope over-requesting, app requests
system/.and the EHR security team blocks approval for months - Launch parameter mismatches, sandbox passes launch params correctly, production Epic Community Connect affiliate passes them slightly differently, app breaks
- OAuth state parameter handling, apps that skip state validation have a CSRF vulnerability
- JWT signing key rotation, backend services flows require JWT auth; apps that hardcode keys break when the hospital rotates them per security policy
Data Mapping: SNOMED, LOINC, USCDI v3
This is the unglamorous integration layer that earns the most money in production and gets the least attention in vendor demos.
What needs to be mapped:
- SNOMED CT for diagnoses and clinical findings (roughly 350,000 concepts; rural EHRs use a subset)
- LOINC for laboratory and clinical observation codes (roughly 95,000 codes; rural labs use a few hundred)
- RxNorm for medications (normalizes across brand/generic/formulation variants)
- CPT / HCPCS for billing codes (CCM 99490, 99491, 99487, 99489; RPM 99453-99458)
- ICD-10-CM for diagnosis codes (still widely used in revenue cycle, increasingly joined to SNOMED in clinical data)
USCDI v3 data classes that the EHR must expose:
- Allergies and Intolerances
- Assessment and Plan of Treatment
- Care Team Members
- Clinical Notes
- Diagnostic Imaging
- Encounter Information
- Goals
- Health Concerns
- Immunizations
- Laboratory
- Medications
- Patient Demographics
- Problems
- Procedures
- Provenance
- Smoking Status
- Unique Device Identifier
- Vital Signs
- (Plus v3-added classes: Clinical Tests, Encounter Diagnosis, Reason for Visit, SDOH Assessment, etc.)
The fields within each class and the mandatory vs optional designations are specified in the ONC USCDI v3 spec.
Quality measure mapping is custom-build per program. HEDIS, CMS Star Ratings, state-specific measures, payer-contract-specific measures, each rural program has a different measure mix based on their payer contracts and RHTP requirements. There is no packaged accelerator for quality measure reporting because the measure selection, numerator/denominator logic, and reporting cadence are program-specific. This is engagement scope, not a product.

ONC USCDI v3 July 2026 Compliance for Rural Hospitals
July 1, 2026, is the compliance date for USCDI v3 for certified health IT. What this means for rural hospitals:
The requirement: Certified health IT (which most rural EHRs are) must support USCDI v3 data classes via FHIR R4 APIs by the deadline. The EHR vendor is responsible for the EHR side. The hospital’s integration partner is responsible for ensuring downstream apps and reporting workflows handle v3 data correctly.
What rural hospitals should demand from their EHR vendor by Q2 2026:
- USCDI v3 source attribute document (per ONC HTI-1 rule) naming which data classes are supported and via which API endpoints
- FHIR R4 sandbox access with USCDI v3 profile support
- Production upgrade timeline for any USCDI v3 data classes not yet supported
- Documented information blocking policy compliance per 45 CFR 171
Information blocking enforcement: The 21st Century Cures Act information blocking rule is actively enforced. Rural hospitals that fail USCDI v3 compliance face penalties under the rule, and state RHTP program offices are including information blocking compliance as a screening criterion in Q3 2026 technology procurements. A rural hospital that cannot demonstrate USCDI v3 readiness will not score well on RHTP technology proposals.
How non-compliance affects RHTP eligibility: Every state RHTP plan I have reviewed includes interoperability and data exchange as scored criteria. The states naming USCDI v3 compliance explicitly in their procurement requirements include Massachusetts, Texas, Utah, and Maine. A hospital that cannot produce USCDI v3 resources via FHIR is automatically scored lower on interoperability maturity.
How RHTP Funding Pays for Rural EHR Integration
The Rural Health Transformation Program funds EHR integration as a named activity in state plans where interoperability and technology modernization are explicit initiatives.
States with EHR integration in their RHTP plans:
- Massachusetts, Initiative I Activity 5 covers interoperability infrastructure including FHIR gateway deployment and EHR integration engines for CAH-tier hospitals
- Texas, $281M total award with technology modernization across rural hospital HIE connections, state-level data sharing, and EHR upgrade paths
- Utah, Clinical AI Hub infrastructure includes EHR integration layer for AI-augmented care management
- Maine, Rural AI Hub requires EHR integration across participating CAHs as a prerequisite for the AI layer
- Montana, AI monitoring for chronic disease requires EHR integration at each Frontier-designated hospital site
What RHTP funds for EHR integration:
- Integration engine deployment (Mirth Connect, Rhapsody, managed FHIR fabric like EHRConnect)
- FHIR gateway licensing
- Data mapping work (USCDI v3 class coverage, SNOMED/LOINC concept mapping)
- SMART on FHIR app development and deployment
- Care coordinator training on integrated workflows
- Compliance infrastructure (HTI-1 source attribute documentation, HIPAA BAA)
What RHTP does not typically fund:
- Ongoing EHR subscription fees
- EHR platform replacement (that is a different procurement)
- Integration work that should be the EHR vendor’s responsibility under their existing contract
Where Rural EHR Integrations Fail (and How to Avoid It)
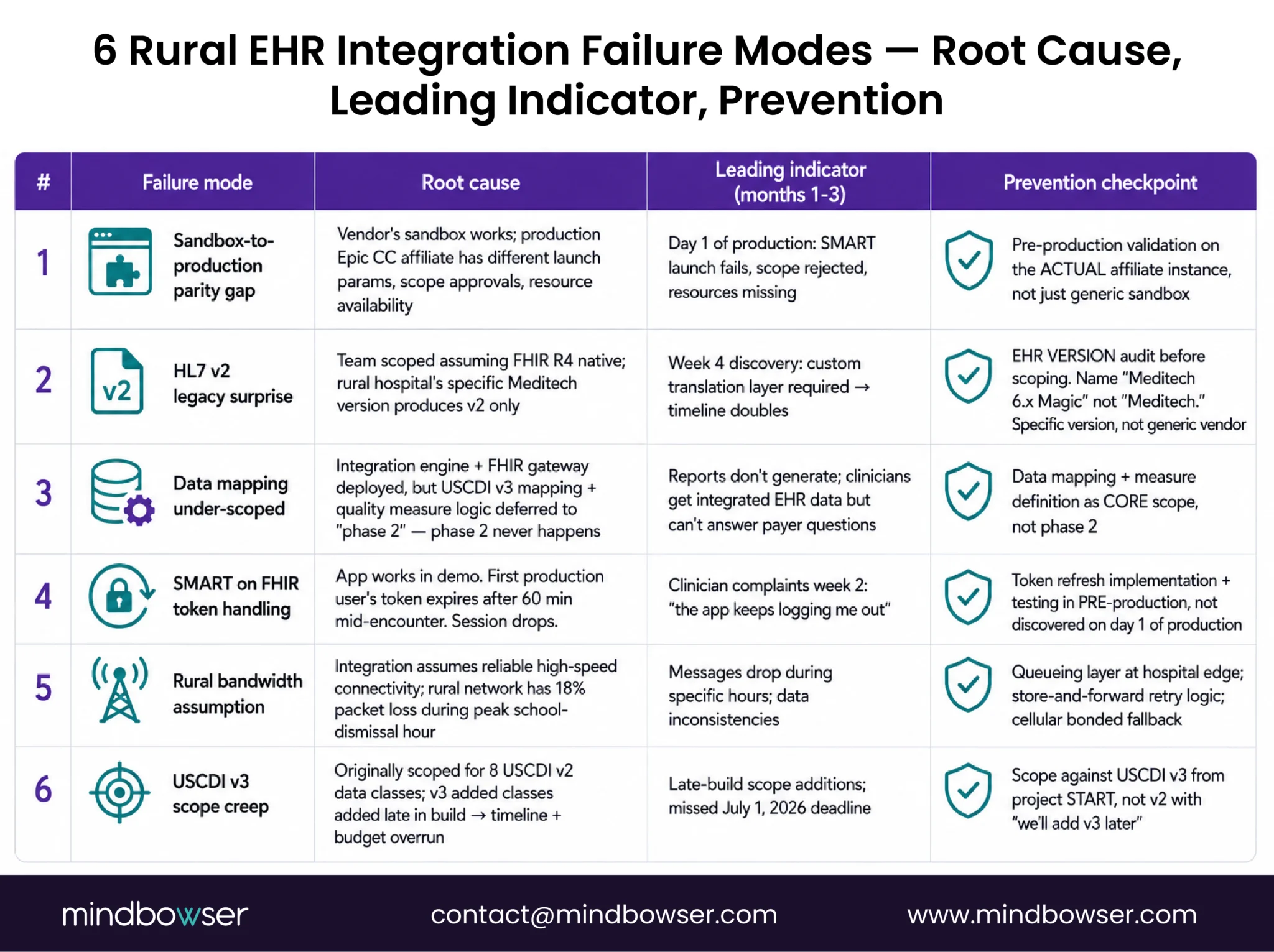
Six failure patterns I have seen repeatedly.
- Failure 1: Sandbox-to-production parity gap: The vendor’s FHIR sandbox works perfectly. Production Epic Community Connect affiliate instance has different launch parameter behavior, different scope approvals, different resource availability. Integration works in dev, breaks on day one of production. Avoidance: pre-production validation on the actual affiliate instance, not just the generic sandbox.
- Failure 2: HL7 v2 legacy surprise: Team scopes the integration assuming FHIR R4 native support, discovers the rural hospital’s specific Meditech version produces HL7 v2 only, custom translation layer doubles the project timeline. Avoidance: EHR version audit before scoping. Name the EHR version, not just the vendor.
- Failure 3: Data mapping under-scoped: Integration engine deployed, FHIR gateway running, but USCDI v3 mapping and quality measure logic were scoped as “phase 2.” Phase 2 never happens. Integration works technically but does not produce the reports the hospital needs. Avoidance: data mapping and measure definition as core scope, not phase 2.
- Failure 4: SMART on FHIR token handling: App works in demo. First production user’s token expires after 60 minutes mid-encounter. App drops session. Clinician stops using it. Avoidance: token refresh implementation and testing in pre-production, not discovered on day one of production.
- Failure 5: Rural bandwidth assumption: Integration assumes reliable high-speed connectivity between the hospital and the cloud-hosted integration platform. Rural network has 18% packet loss during peak school-dismissal hour because the whole town is on one cellular tower. Integration drops messages. Avoidance: queueing layer at the hospital edge, store-and-forward retry logic, cellular bonded fallback.
- Failure 6: USCDI v3 scope creep: Integration originally scoped for 8 USCDI v2 data classes, project adds v3’s additional classes late in the build, timeline slips, budget overruns. Avoidance: scope against USCDI v3 from project start, not v2 with a “we’ll add v3 later” tag.
How Mindbowser Helps Rural Hospitals Integrate Their EHRs
The promise rural hospitals need is integration that goes live in weeks, not quarters, with USCDI v3 compliance baked in, SMART on FHIR apps that actually launch in production, and an audit trail the next auditor will accept.
Mindbowser approaches rural EHR integration as a workflow transformation with pre-built integration fabric as the shortcut. EHRConnect compresses the traditional 6-month Epic, Cerner, Athenahealth integration into 6-day production deployments. HealthConnect CoPilot handles the v2-to-FHIR translation as a managed capability. Patient Questionnaire Form and AI Medical Summary sit on top as the FHIR-native data collection and summary generation layers. PHISecure covers the HIPAA PHI de-identification required for any AI/analytics workload touching integrated data.
The custom-build scope, legacy Meditech Magic APIs, Praxis proprietary integrations, state-specific HIE connections, USCDI v3 quality measure mapping per program, is explicitly engagement work, not a product. Rural programs get the pre-built fabric where it exists and the custom integration work where it does not, with timeline and budget accounted for both.
For state RHTP program offices evaluating technology partners, the pitch is deployment risk reduction: the integration fabric is built and running in production at other rural hospitals, the USCDI v3 compliance path is documented, the SMART on FHIR auth patterns are battle-tested. State RHTP dollars go further when they are not paying for 6 months of integration-engine-from-scratch.
HL7 v2 is the legacy messaging standard most rural EHRs natively produce (ADT, ORU, ORM messages). FHIR R4 is the modern REST-based standard modern apps require. Most rural integrations need a translation layer between v2 and FHIR R4. Translation patterns are standardized for common resource types (Patient, Observation, Encounter), but vendor-specific quirks in the v2 segments require custom mapping work.
Certified health IT must support the USCDI v3 data classes via FHIR R4 APIs. EHR vendors are responsible for the EHR side; hospitals are responsible for ensuring their integration partners handle v3 data correctly in downstream workflows. Non-compliance affects information blocking enforcement and RHTP eligibility.
Community Connect affiliates share the Epic instance of a parent hospital. They can use FHIR R4 sandbox, App Orchard-registered apps, SMART on FHIR launch context, and bulk FHIR exports, but all subject to parent-instance permissions. They cannot create custom FHIR profiles beyond US Core, access the Caboodle data warehouse directly, or register production apps without parent sponsorship.
Meditech Expanse has native FHIR R4 support. Meditech 6.x / Magic has limited FHIR support and primarily uses proprietary APIs plus ODBC data repository access. Meditech Client-Server has HL7 v2 only. Integration approach depends on which Meditech version the rural hospital runs, ask for the specific version before scoping.
SMART on FHIR 2.1 is the spec that defines how third-party clinician-facing apps launch inside an EHR with OAuth 2.0 authentication and scoped FHIR access. For rural hospitals, SMART support determines whether care management apps, CDS tools, and AI-augmented workflows can run inside the clinician’s native EHR experience instead of being separate systems the clinician switches between.
Yes. State RHTP plans in Massachusetts, Texas, Utah, Maine, and others fund EHR integration as a named activity, integration engine deployment, FHIR gateway, USCDI v3 mapping, SMART on FHIR apps, compliance infrastructure. RHTP does not typically fund existing EHR subscription fees or full platform replacement.
For Epic Community Connect, Cerner CommunityWorks, Meditech Expanse, or Athenahealth: 4-8 weeks from contract signature to production go-live using a pre-built fabric like EHRConnect. For Meditech Magic / Client-Server or Praxis proprietary APIs: 3-5 months due to the custom translation layer work. USCDI v3 data mapping adds 2-4 weeks on top of the base integration timeline.

