



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
The Rural Health Transformation Program allocates $50 billion over five years, $10 billion per year, from FY2026 through FY2030. CMS announced awards to all 50 states on December 29, 2025. FY2026 awards range from $147 million (New Jersey) to $281 million (Texas), averaging $200 million per state. Half the fund is distributed equally among approved states; half is workload-weighted. Technology is a major spending category in most state applications. State procurement windows open Q3 2026 through Q1 2027. What the program’s announcement coverage often underplays: RHTP was created in the same reconciliation law that cuts $137 billion in federal Medicaid spending from rural areas over ten years, per KFF analysis. The $50 billion is an offset to a larger reduction, not net new funding, and how rural hospitals position technology investments around that reality determines whether RHTP stabilizes rural healthcare delivery or becomes another round of unmet expectations. This guide covers what RHTP actually is, how the $50 billion gets allocated against the broader funding picture, what states are building, when RFPs post, who can partner, and which technical capabilities matter most.
Watch the RHTP 2026 Guide
Texas finalized its Budget Period 1 Project Narrative on April 7, 2026, becoming one of the first states to clear CMS approval for implementation work. Nine weeks from now, the state’s procurement team starts posting RFPs for $281 million in rural health technology investments. Forty-nine other states are on similar timelines.
Massachusetts counts 160 rural jurisdictions across 351 cities and towns. That’s 57% of the state’s land mass, home to 700,000 residents, served by six rural hospitals. The state’s application for RHTP funding asks for $1 billion over five years to rebuild the technology infrastructure serving those residents. Massachusetts received $162 million in its first-year award.
Multiply that calculation by 50 states and the scale of the Rural Health Transformation Program becomes difficult to overstate. $50 billion is roughly 5% of total annual Medicare spending on hospital services. It exceeds the combined FY2024 budgets of HRSA, AHRQ, and the CDC Center for Surveillance, Epidemiology, and Laboratory Services. It is one of the largest single federal investments in rural health infrastructure in United States history.
The scale conversation needs a second number to stay honest. The reconciliation law that created RHTP also cut approximately $911 billion in federal Medicaid spending over ten years, of which approximately $137 billion falls on rural areas specifically, per KFF’s November 2025 analysis. On net, rural healthcare loses roughly $87 billion across the decade when the RHTP allocation is subtracted from the Medicaid reduction. This reality is load-bearing for rural hospital financial planning. The UNC Cecil G. Sheps Center for Health Services Research has tracked 152 rural hospital closures and conversions since 2010 (87 complete closures, 65 converted to non-acute care models). The Center for Healthcare Quality and Payment Reform (CHQPR) estimates that 760 rural hospitals, roughly one-third of the nation’s rural facilities, are currently at risk of closing, with 314 at immediate risk within three years; 23 rural hospitals closed in 2025 alone. AHA’s April 2025 financial analysis found that Medicare reimbursed only 83 cents for every dollar hospitals spent caring for patients in 2023, and from 2022 to 2024 general inflation rose 14.1% while Medicare inpatient payment rates increased only 5.1%. RHTP is landing on a rural healthcare system already in financial distress, and the program is positioned to offset Medicaid cuts rather than to expand capacity beyond prior baselines.
That framing changes how technology investments under RHTP should be scoped. A rural hospital treating RHTP as net-new growth capital makes different decisions than a rural hospital treating it as a bridge to stabilize operations while Medicaid cuts phase in. State program offices scoring vendor proposals understand this distinction, the technology investments that pass scoring are the ones that produce measurable financial stabilization, not the ones that require RHTP to be renewed in 2031 to avoid stranded costs.
The consulting firms that wrote the state applications are now pivoting to implementation support. A different question sits beneath their pivot: who actually builds the technology? State health departments don’t have software engineering teams. Rural hospitals operate with 1-2 IT staff. The EHR vendors (MEDITECH, Epic, Oracle Health) cover their own platforms but rarely build custom integration layers. The off-the-shelf SaaS companies sell their product.
That gap is the RHTP technology implementation market, and it’s opening now.
This is the complete 2026 guide.
What Is the Rural Health Transformation Program?
The Rural Health Transformation Program (RHTP) is a $50 billion federal grant program that allocates $10 billion per year across all 50 states from FY2026 through FY2030. Authorized by Section 71401 of Public Law 119-21 and administered by CMS, the program funds rural healthcare access, workforce, and technology initiatives at state discretion.
That’s the definitional answer. The operational answer has more layers. The program was authorized under the One Big Beautiful Bill Act signed in mid-2025, with Funding Opportunity Number CMS-RHT-26-001. Its statutory purpose is to strengthen rural communities by improving healthcare access, quality, and outcomes through transformation of the rural healthcare delivery ecosystem.
Translated from legislative language: the program gives states $10 billion per year for five years to fix what’s broken in rural healthcare. Every state decides its own priorities within seven broad categories defined by the statute. Every state writes a five-year plan. Every state runs its own procurement for the technology, workforce, and facility investments that plan requires.
Three things distinguish RHTP from prior rural health funding:
- Scale: The Federal Office of Rural Health Policy’s discretionary budget historically ranges from $350-400 million per year. RHTP allocates 25 times that annually to states. It’s not a continuation of prior programs. It’s an order-of-magnitude shift.
- State discretion: Previous rural health funding flowed through categorical grants with tight restrictions on use. RHTP gives states flexibility within a broad statutory framework. A state can spend its share on EHR modernization, workforce housing, facility renovation, AI deployment, or new care models. The plan documents that tradeoff.
- Implementation emphasis:
- A. Evidence-based, evidence-informed interventions in rural population health: Chronic disease management programs, preventive care infrastructure, community health workers, behavioral health access.
- The statutory scoring favors plans that demonstrate operational capability to execute, not just need. States that can show existing infrastructure, interagency coordination, and vendor-ready procurement processes scored higher. This has downstream effects on how states will buy.
An NEJM Perspective piece published in early 2026 framed RHTP as “an avenue for states to modernize rural healthcare delivery” while cautioning that implementation quality will determine whether the program produces measurable outcomes or another round of unmet expectations. That framing matters for vendors and primes: CMS is watching execution, not just procurement spend.
Academic analysis reinforces the implementation-quality emphasis. A Health Affairs Scholar article tracking projected RHTP scores against actual state awards found meaningful variance between what CMS’s rubric rewarded on paper and where awards actually landed, suggesting that scoring favored operational credibility alongside stated scope. The Bipartisan Policy Center’s explainer on RHTP technology innovation frames the program as a test of whether federal rural healthcare investment can produce durable infrastructure or whether the funding dissipates into operational gap-filling. Both framings point to the same vendor implication: state program offices are scoring for deployment credibility and sustainability, not for feature breadth.
Is This the Same as the HRSA Rural Health Transformation Program?
No. This confusion appears often enough that it deserves a direct answer.
The RHT Program is administered by CMS under the One Big Beautiful Bill Act. HRSA (Health Resources and Services Administration) runs separate rural health programs including the Rural Hospital Flexibility (Flex) Program, the Small Hospital Improvement Program (SHIP), and the Rural Health Clinic program. State applications sometimes reference HRSA resources or build on HRSA-funded infrastructure, but the $50 billion is CMS money, not HRSA money.
Searches for “HRSA Rural Health Transformation Program” typically land on this CMS program. The terminology has consolidated informally even though the formal administration is CMS.
Hospital at Home Platform Requirements Checklist: Score your AHCAH platform readiness before you build or apply.
How $50 Billion Gets Allocated
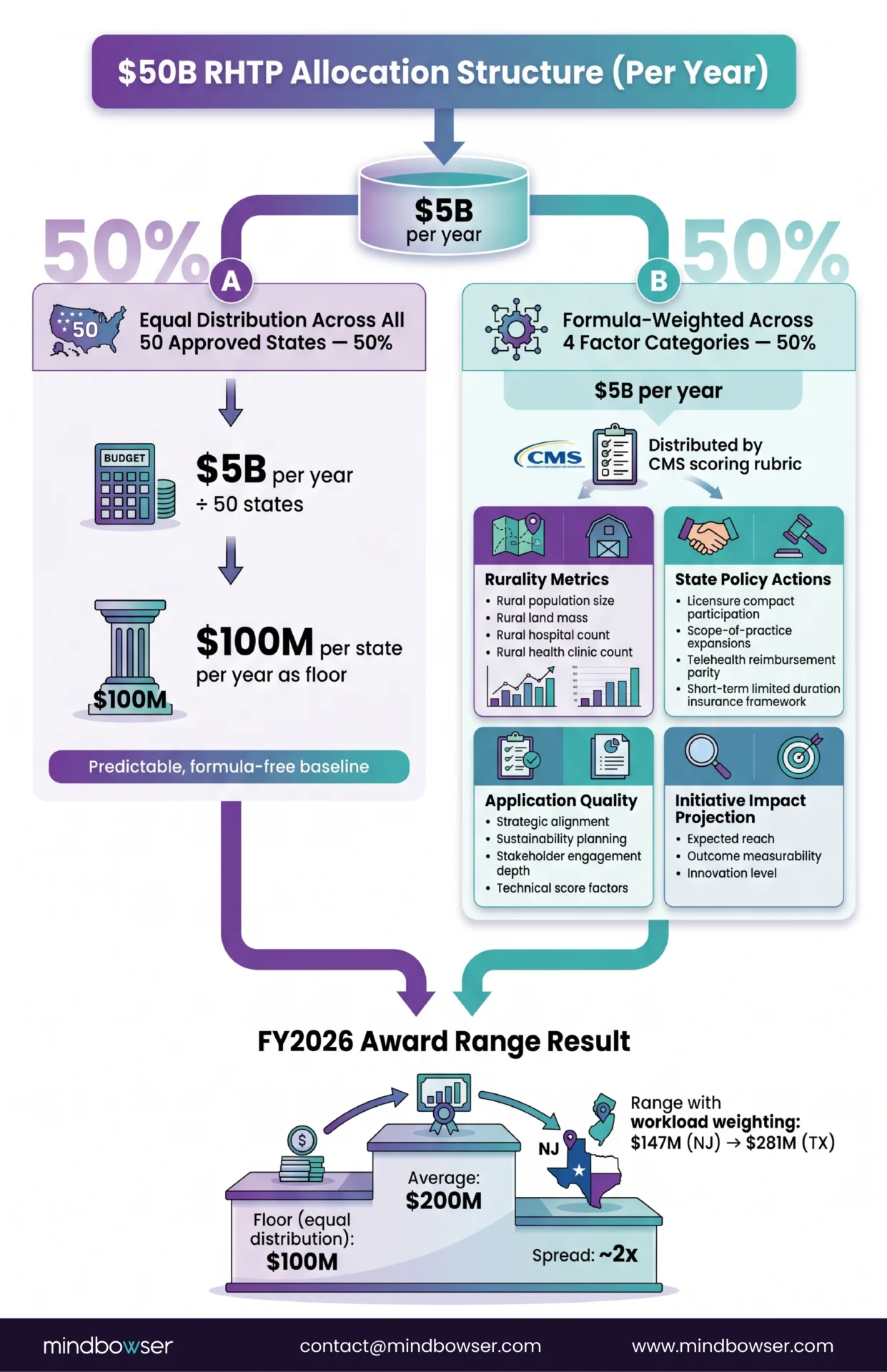
The allocation formula is public and determines why Rhode Island receives $6,305 per rural resident while Texas receives $66.
50% of each year’s $10 billion is distributed equally among all approved states. With 50 states approved, that’s $100 million per state per year as a floor.
The remaining 50% is formula-weighted across several factors defined in CMS’s scoring rubric:
- Rurality metrics: Rural population size, rural land mass, rural hospital count, rural health clinic count
- State policy actions: Licensure compact participation, scope-of-practice expansions, telehealth reimbursement parity, short-term limited duration insurance framework
- Application quality: Strategic alignment, sustainability planning, stakeholder engagement depth, technical score factors
- Initiative impact projection: Expected reach, outcome measurability, innovation level
FY2026 awards ranged from $147 million (New Jersey) to $281 million (Texas). The average award was $200 million.
The Per-Rural-Resident Breakdown
| Tier | Award Range | Example States |
|---|---|---|
| $66-$100 per rural resident | Texas, Ohio, North Carolina, Pennsylvania, Michigan, California, Georgia, Tennessee | Populous states with dense rural populations. Lower per-capita, larger total |
| $100-$200 per rural resident | Wisconsin, New York, Illinois, Missouri, Indiana, Minnesota, Mississippi, Virginia, Alabama, Iowa, Oklahoma, Arkansas, Washington, Oregon, South Carolina, Louisiana, Kansas | Mid-range states. The largest tier |
| $200-$500 per rural resident | Florida, Colorado, Arizona, West Virginia, New Mexico, Maine, Nebraska, Idaho, New Hampshire, Maryland, South Dakota, Utah, Montana, Vermont, Connecticut, Wyoming | States with smaller rural populations but meaningful total awards |
| $500-$6,305 per rural resident | Hawaii, North Dakota, Nevada, Delaware, Massachusetts, Alaska, New Jersey, Rhode Island | Small rural populations, formula treats them generously. Rhode Island at $6,305 is the outlier |
Alaska deserves specific mention: $272 million for roughly 275,000 rural residents, or $990 per person. Alaska’s geography (frontier isolation, tribal health context, limited road infrastructure) produced the highest per-capita allocation outside Rhode Island’s statistical anomaly.
Why Texas Got the Largest Total Award
Texas received $281,319,361 for FY2026 despite having one of the lowest per-rural-resident allocations ($66). The answer is raw scale. Texas counts roughly 4.3 million rural residents across 172 rural hospitals and 5 rural health care regions spanning the Gulf Coast, West Texas, the Panhandle, East Texas, and the border. No other state approaches that rural population base.
CMS approved Texas’s revised Budget Period 1 Project Narrative on April 7, 2026, making it one of the first states to finalize its implementation plan.
What Are the Seven Statutory Elements?
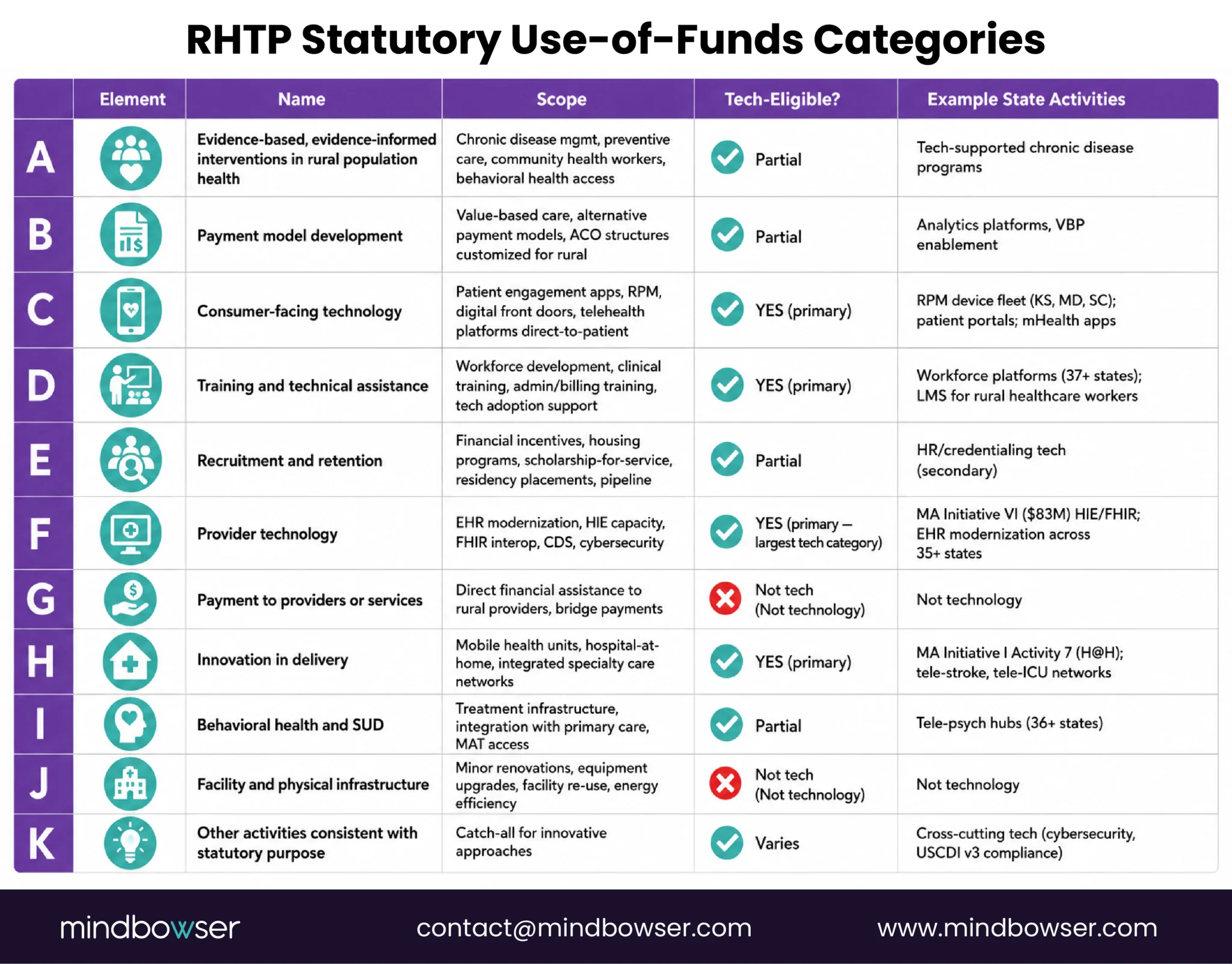
Every state plan must align to seven statutory use-of-funds categories identified as A through K (with some letters skipped in the original legislation):
- A. Evidence-based, evidence-informed interventions in rural population health: Chronic disease management programs, preventive care infrastructure, community health workers, behavioral health access.
- B. Payment model development: Value-based care programs, alternative payment models, accountable care organization structures customized for rural populations.
- C. Consumer-facing technology: Patient engagement applications, remote monitoring, digital front doors, telehealth platforms available directly to patients.
- D. Training and technical assistance: Workforce development, clinical training programs, administrative and billing training, technology adoption support.
- E. Recruitment and retention: Financial incentives, housing programs, scholarship-for-service commitments, residency placements, pipeline development.
- F. Provider technology: EHR modernization, health information exchange capacity, interoperability infrastructure, clinical decision support, cybersecurity.
- G. Payment to providers or services: Financial assistance to rural providers, bridge payments, reimbursement mechanism improvements.
- H. Innovation in delivery: Mobile health units, hospital-at-home programs, integrated specialty care networks, new care models.
- I. Behavioral health and substance use disorder services: Treatment infrastructure, integration with primary care, medication-assisted treatment access.
- J. Facility and physical infrastructure: Minor renovations, equipment upgrades, facility re-use, energy efficiency.
- K. Other activities consistent with the statutory purpose: Catch-all for innovative approaches not covered by A-J.
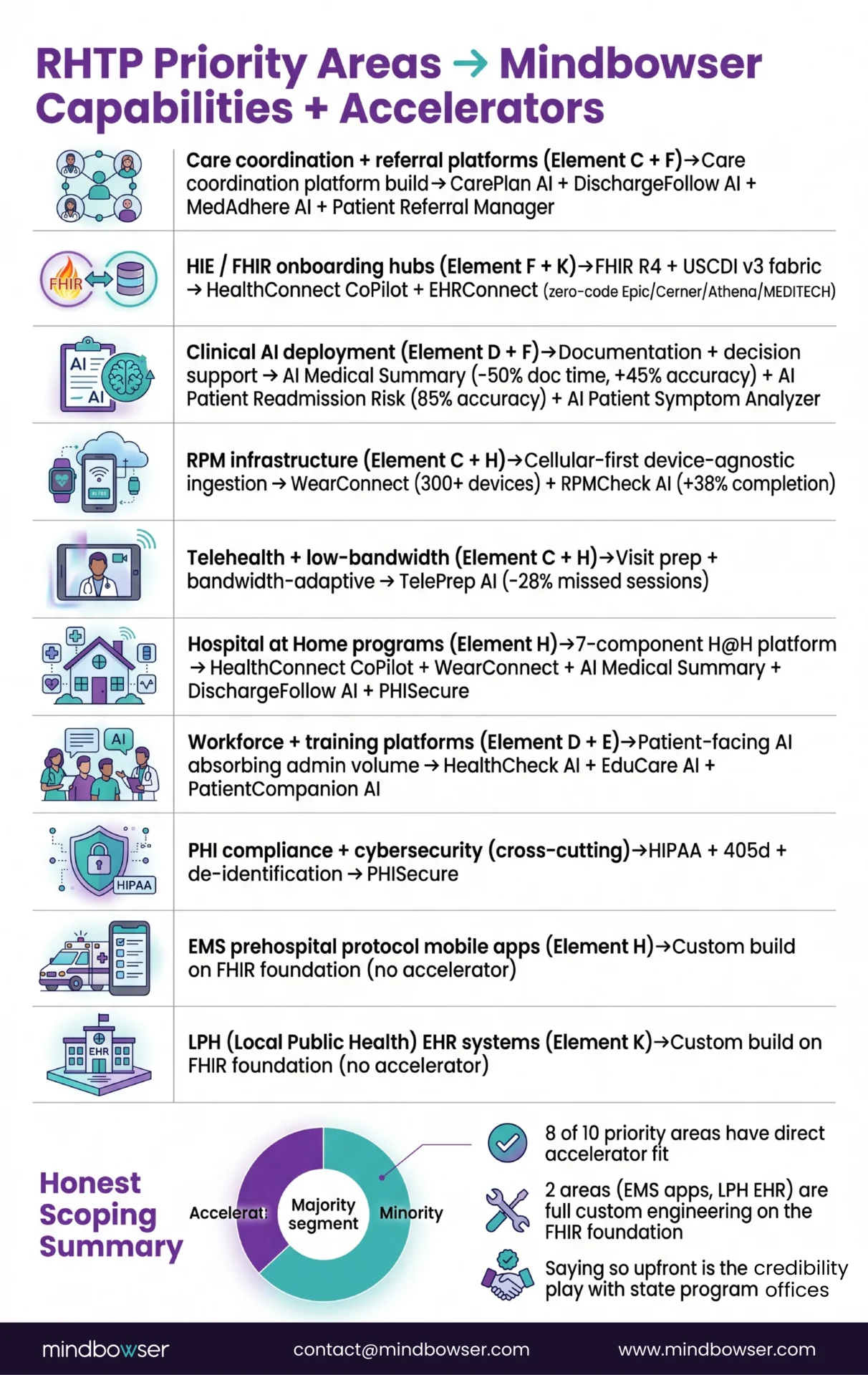
Most state plans allocate across 7-10 of these categories through 5-7 initiatives. Technology touches categories C, D, F, and H most directly. Facility modernization (J) and workforce (D, E) account for significant spending but are less technology-intensive.
Technical Score Factors
CMS evaluated applications against technical score factors labeled B.1 through F.3 covering: application quality, stakeholder engagement, strategic alignment, technical capability, state policy alignment, and sustainability. States’ application narratives reference which score factors each proposed initiative addresses, which provides a secondary signal of what states prioritized during application.
What Are States Actually Building?
The most useful analysis of RHTP funding is cross-state: what technology do multiple states plan to buy?
We synthesized all 50 state application narratives. Patterns emerged across seven technology categories.
Category 1: Care Coordination and Referral Platforms
Multiple states proposed bi-directional technology platforms that connect clinical providers with social service organizations and community-based organizations. These platforms unite clinical care, social support, and community resources through electronic referrals, closed-loop tracking, EHR integration, care management workflows, and billing supports.
Named examples:
- Massachusetts: “Rural MA Connect” (modeled on Missouri’s ToRCH program)
- Missouri: Transformation of Rural Community Health (ToRCH) program expansion
- Multiple states reference similar shared-service coordination platforms
Technical requirements: FHIR-based APIs, HL7 integration, real-time directory services, EHR vendor partnerships across Epic, MEDITECH, Cerner/Oracle, Athena, eClinicalWorks.
Category 2: Real-Time Bed and Service Availability Tracking
States are addressing emergency department boarding, transfer delays, and capacity mismatches through real-time cross-agency data platforms. The model: make capacity visible, match patients to beds dynamically, reduce transport delays.
Named examples:
- Massachusetts: “RISE” (Rural Innovation for Systems Change & Effectiveness), modeled on Mayo Clinic Admission Transfer Center
- Multi-state: Connection to CMS’s Automated Capacity and Occupancy Reporting Network (ACORN) is a widely named activity
Technical requirements: Real-time data exchange, hospital census integration, EMS dispatch integration, dashboard development.
Category 3: AI Clinical Documentation and Adverse Event Monitoring
Clinical AI appears in applications from Texas, Maine, Utah, West Virginia, Tennessee, Massachusetts, and others. The use cases range from administrative automation (Texas AI-automated fax processing) to clinical assistance (Utah clinical AI agents for note-taking, chart summarization, and treatment recommendations) to safety monitoring (Massachusetts AAEM — Automated Adverse Event Monitoring, modeled on the Betsy Lehman Center’s hospital pilot).
Named examples:
- Maine: “Rural AI Hub and Innovation Institute”
- Utah: Clinical AI agents across documentation and decision support
- Massachusetts: AAEM (AI scanning of EHR data for real-time adverse event detection)
- Texas: AI-automated fax processing
- Multiple: AI for patient scheduling, clinical note scribing, virtual ASL interpreting, referrals management
Technical requirements: EHR integration for real-time data access, HIPAA-compliant model infrastructure, clinical validation workflows, integration with physician attestation processes.
Category 4: Remote Patient Monitoring Infrastructure
RPM expansion is a named activity in Massachusetts, Kansas, Maryland, South Carolina, and others. The focus in rural contexts: cellular-enabled devices (not WiFi-dependent), patient onboarding workflows for elderly populations, Medicare RPM billing codes (99453-99458), integration with primary care and chronic disease management.
Technical requirements: Device-agnostic ingestion layers, FHIR-compatible data streams, cellular connectivity management, patient-facing applications with minimal-tech onboarding.
Category 5: Telehealth Infrastructure and Connectivity
Telehealth investment appears in nearly every state plan, with specific depth in Arizona, Arkansas, Maine, Florida, and Utah. The rural specificity matters: low-bandwidth video solutions, store-and-forward capabilities, satellite connectivity for frontier regions, tele-pharmacy and tele-dental services, school-based tele-behavioral health.
Technical requirements: Bandwidth-adaptive streaming, offline-capable documentation, peripheral device integration (digital stethoscope, otoscope, dermatoscope), multi-platform patient access.
Category 6: Health Information Exchange and FHIR Onboarding
HIE expansion is Initiative VI-equivalent in most state plans. Massachusetts describes a “HIE Technical Assistance Hub” providing shared onboarding, training, and implementation playbooks for rural providers connecting to state and national networks (Mass HIway, ACORN, TEFCA/QHIN, NCPDP). The target in Massachusetts: move rural provider interoperability baseline from 25% to 100% over five years.
Technical requirements: FHIR R4 APIs, FHIR bulk data, TEFCA/QHIN compliance, USCDI v3 compliance (mandatory July 2026 for certified health IT), practice-level event notifications, query-based exchange.
Category 7: Local Public Health EHR Systems
Several states including Massachusetts proposed centralized, state-funded EHR platforms for local public health (LPH) agencies. These systems enable electronic claims submission, immunization reporting, chronic disease case management, and integration with state public health registries.Technical requirements: HL7 and FHIR compliance, integration with state immunization registries, Medicaid clearinghouse connectivity, billing module.
Cross-State Technology Matrix
| Technology Category | States with Named Initiatives | Typical Procurement Vehicle |
|---|---|---|
| Care coordination platforms | MA, MO, plus 10+ states with similar named programs | Direct state contract or prime subcontract |
| Real-time bed/service tracking | MA, plus multi-state ACORN integrations | Direct contract to state health department |
| AI clinical documentation/monitoring | TX, ME, UT, WV, TN, MA | Mix: prime contracts, state innovation sandboxes |
| RPM infrastructure | MA, KS, MD, SC, plus most states | State health department or regional rural health org |
| Telehealth infrastructure | AZ, AR, ME, FL, UT, plus most states | State telehealth authority or prime contractor |
| HIE/FHIR onboarding | Most states (Initiative VI equivalent) | State HIE organization (e.g., Mass HIway) |
| LPH EHR systems | MA, plus several others with similar proposals | Direct state public health department contract |
Planning an RHTP-funded rural healthcare transformation initiative?
When Do RFPs Actually Post?
The most common operational question about RHTP is timing. Here’s the answer based on public state workplans.
Phase 0: Setup (Q1 2026 – Q3 2026)
States hire staff, establish governance teams and Community Advisory Councils, complete needs assessments, and develop procurement strategies with stakeholder input. No RFPs post during this phase. Some states post Requests for Information (RFIs) to scope vendor capacity.
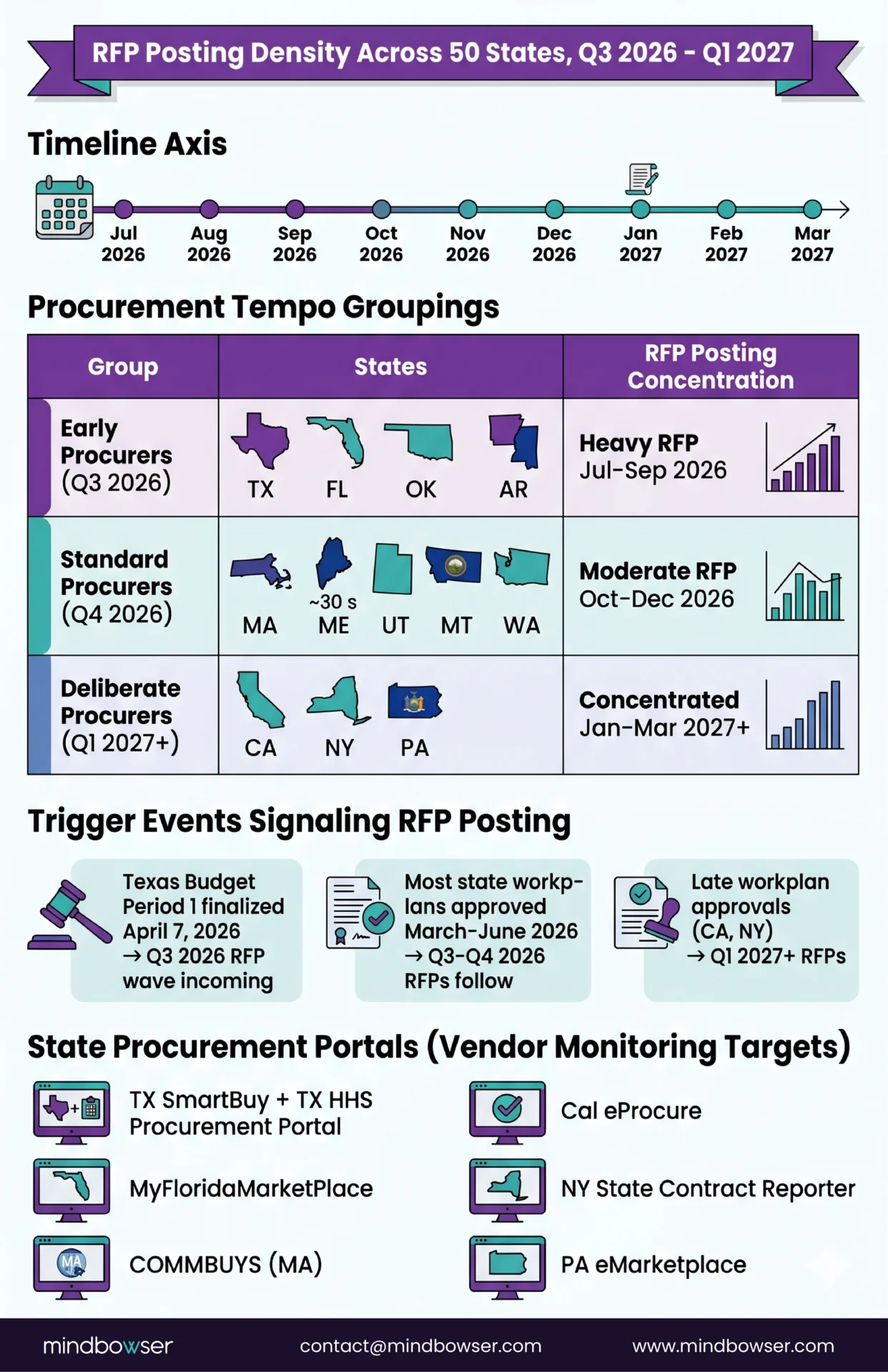
Phase 1: Procurement (Q3 2026 – Q2 2027)
This is the window. States post RFPs, evaluate vendors, and award contracts. Some initiatives (Facility Modernization, Workforce) begin procurement earlier because they’re lower-risk. Technology procurements typically cluster in Q4 2026 through Q1 2027.
Expect cohort-based awards. Massachusetts, for example, plans to award “round one facilities” in Q1 2027 and “round two facilities” in Q2 2027. Most states will similarly stage awards across sub-populations.
Phase 2: Implementation (Q1 2027 – Q4 2028)
Technology development begins. Data sharing agreements execute. Training and onboarding roll out. Pilot implementations kick off. For multi-year technology programs, initial go-lives happen Q3-Q4 2027.
Phase 3: Scale (Q1 2028 – Q1 2030)
Programs expand to full scope. Quarterly evaluation cycles begin. States start sustainability planning in Year 4 (2029) because the RHTP funding ends September 2030.
Phase 4: Transition (Q1 2030 – Q4 2030)
Final outcomes evaluation. Transition to sustainable non-federal funding sources. Policy actions to extend successful pilots beyond the RHTP window.
Where to Watch for RFPs
Public state procurement portals are the primary posting location. For priority states:
- Texas: Texas Health and Human Services Provider Finance Department website + Texas Electronic State Business Daily (ESBD)
- Massachusetts: COMMBUYS (Commonwealth’s procurement portal)
- California: Department of General Services eProcurement System (DGS Cal eProcure)
- Other states: State health department pressrooms, state procurement portals
Federal opportunities related to RHTP may also post on grants.gov when they involve federal pass-through funding.
Who Can Partner on RHTP Implementation?
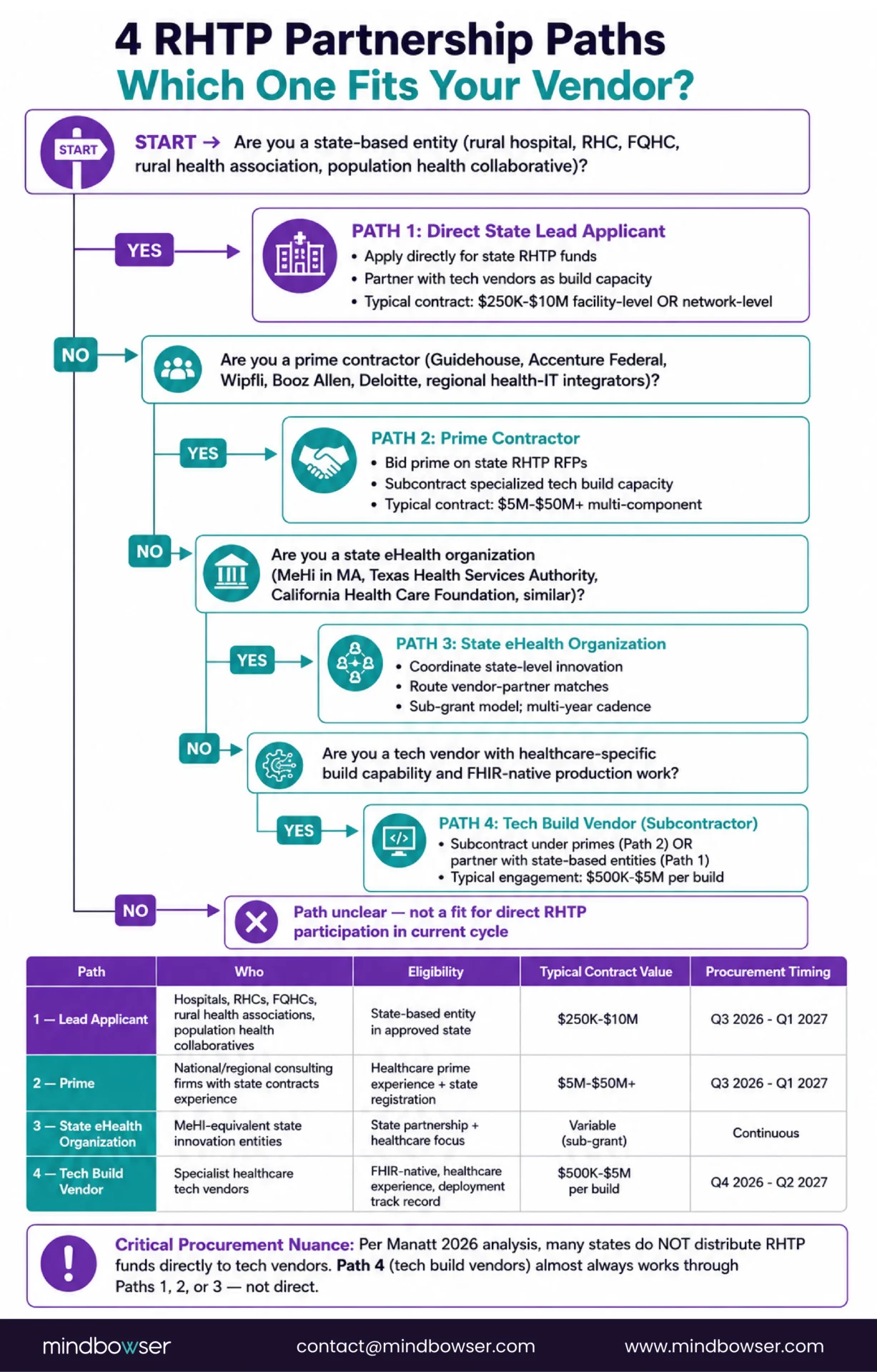
Four partnership paths exist. Most technology vendors access RHTP work through one of them.
Path 1: Direct State Contract
Vendors can bid directly on state-issued RFPs. This path requires:
- State-level registration and vendor credentialing
- Capacity to meet state contracting requirements (insurance, bonding, MBE/WBE certifications where applicable)
- Experience comparable to the scope of work
- Often, an established relationship or RFI response demonstrating capability
Direct state contracts tend to be the highest-value opportunities ($2M-$10M+) but have the highest bar for entry.
Path 2: Prime Contractor Subcontract
Large consulting firms (Accenture Federal, Guidehouse, Chartis, Wipfli, PwC Public Sector) and large systems integrators will prime technology contracts and subcontract to specialists. This path works well for vendors with deep technical capability but limited state-level BD infrastructure.
The prime contractor brings the state relationship, program management, and compliance infrastructure. The technology subcontractor brings the custom build capability.
Path 3: State eHealth Organization Partnership
Every state has an equivalent of Massachusetts eHealth Institute (MeHI). These organizations often serve as the state’s designated gatekeeper for digital health vendor selection, innovation sandboxes, and cybersecurity coordination.
Examples:
- Massachusetts: MeHI
- California: California Health Care Foundation (CHCF)
- Texas: Texas Health Services Authority (THSA)
- New York: New York eHealth Collaborative
Participation in their programs (sandbox grants, vendor directories, technical assistance hub contracts) creates visibility to state procurements.
Path 4: Rural Hospital Network and Population Health Collaborative
Some states channel RHTP investments through existing rural hospital networks or population health collaboratives rather than running state-level procurements. Vendors who partner with these networks can implement across multiple rural hospitals under a single agreement.
Which Path Fits Which Vendor
| Vendor Type | Best Path | Why |
|---|---|---|
| Large federal contractor | Direct state contract | Have infrastructure for state-level BD |
| Mid-size specialist (healthcare software development, FHIR, clinical AI) | Prime subcontract + state eHealth org partnership | Prime brings state relationship, specialist brings technical build |
| Startup / smaller specialist | State eHealth org partnership | Innovation sandboxes and TA programs provide entry |
| Regional healthcare-specific consultancy | Rural hospital network partnership | Existing relationships, low-friction path |
What Technology Capabilities Do States Need Most?
Synthesizing across all 50 state plans, six technology capabilities surface repeatedly. A vendor that demonstrates all six is positioned for the broadest set of RHTP opportunities.
Capability 1: FHIR R4 Interoperability
Every state plan that addresses Initiative VI equivalents mentions FHIR. USCDI v3 compliance becomes mandatory July 2026 for certified health IT, which means FHIR R4 API exposure is functionally a prerequisite for any technology connecting to clinical systems. Specific requirements include: bulk FHIR data exchange, FHIR resource mapping across patient/encounter/observation/medication/condition resources, FHIR-based prior authorization (CMS mandate), SMART on FHIR app integration.
Mindbowser applied these patterns across Epic FHIR integrations, device-to-FHIR normalization layers for RPM ecosystems, and multi-EHR care coordination architectures designed to support longitudinal patient workflows and cross-system interoperability.
Capability 2: Clinical AI That Clinicians Actually Use
States are funding AI with specific use cases: documentation reduction, alert filtering, adverse event detection, treatment recommendation support. The failure mode is generic AI dropped into clinical workflows without integration or trust-building. Capabilities that matter: ambient documentation that integrates with existing EHR flowsheets; alert filtering calibrated to clinical protocol thresholds; adverse event detection integrated with clinician attestation workflows; clinical validation and bias monitoring.
Mindbowser’s AI Medical Summary accelerator captures the documentation reduction pattern. Our broader clinical AI work covers the integration patterns that make AI usable at the bedside rather than a dashboard clinicians ignore.
Capability 3: Care Coordination Platform Development
Named state platforms (Rural MA Connect, ToRCH, similar) require: bi-directional EHR integration across multiple vendors; real-time closed-loop referral tracking; social services directory integration; care plan sharing across clinical, social, and community stakeholders; billing module for care coordination CPT codes.
HealthConnect CoPilot demonstrates the care coordination architecture applied to clinical workflows. The social service integration layer is the extension RHTP-scale platforms require.
Capability 4: Remote Patient Monitoring Infrastructure
Rural RPM deployments differ from urban deployments in specific ways: cellular-first device selection (23% of rural Americans lack broadband); patient onboarding workflows that work with minimal technical skill; Medicare RPM billing code handling (99453, 99454, 99457, 99458); integration with primary care, chronic care management, and hospital-at-home programs.
WearConnect’s device-agnostic architecture handles 14 device manufacturers through a single FHIR-compatible data stream. The abstraction layer prevents vendor lock-in as device standards evolve.
Capability 5: EHR Integration for Rural Legacy Systems
Rural hospitals disproportionately run MEDITECH Expanse, Epic Community Connect, Athenahealth, eClinicalWorks, and older versions of larger EHRs. Integration requires HL7v2 messaging alongside FHIR, ADT feed management, middleware for systems lacking modern API surfaces, and pragmatic workarounds for systems that were never designed for deep third-party integration.
This is where generic FHIR expertise fails in rural contexts. The technical reality at a Critical Access Hospital with 25 beds and 1-2 IT staff does not look like Epic at Massachusetts General Hospital.
Capability 6: HIPAA-Compliant Cloud Infrastructure with Rural Connectivity Awareness
Managed cloud infrastructure is table stakes. The rural specificity: infrastructure that tolerates intermittent connectivity, provides offline-capable clinical workflows, manages cellular data costs, and delivers acceptable performance over satellite connections for frontier deployments.
PHISecure handles the HIPAA compliance infrastructure. The connectivity-resilience layer is where most enterprise platforms break when deployed in actual rural environments.
Capability Map
| RHTP Priority | Mindbowser Capability | Accelerator | Adjacent Proof |
|---|---|---|---|
| FHIR interoperability | FHIR R4 implementation, SMART on FHIR | HealthConnect CoPilot | Epic FHIR integration deployments |
| Clinical AI | Documentation, alerts, adverse events | AI SummaryAssist | CDS Hooks implementation experience |
| Care coordination | Cross-org platforms | HealthConnect CoPilot | Chronic care management platforms |
| RPM infrastructure | Device-agnostic monitoring | WearConnect | Rural RPM deployments |
| EHR integration (legacy) | MEDITECH, Epic CC, Athena, eCW | HealthConnect CoPilot | Multi-EHR deployments |
| HIPAA cloud infra | Secure, connectivity-aware | PHISecure | National-scale healthcare platforms |
How Does Mindbowser Help States Operationalize Their RHTP Plans?
Mindbowser helps states, health systems, and rural providers operationalize FHIR-based interoperability, care coordination, and AI-enabled workflows from pilot to statewide scale.
We’re a healthcare technology development firm with eight-plus years building custom clinical software for health systems, digital health startups, and rural providers. Our delivery focus sits exactly where RHTP implementations need the most depth: custom development on top of existing EHRs, FHIR-based interoperability across multiple systems, clinical AI deployment, and rural-constraint-aware architecture.
The accelerator stack we’ve built (HealthConnect CoPilot for care coordination, WearConnect for device-agnostic RPM, AI Medical Summar for clinical documentation, PHISecure for HIPAA-compliant cloud infrastructure) compresses 18-24 month builds into 12-16 week MVPs, then scales from there. This matters for RHTP because state procurement timelines assume vendors who can move fast, and the five-year RHTP funding window does not reward multi-year waterfall projects.
We work alongside consulting firms that hold state relationships, state eHealth organizations that coordinate innovation pilots, and prime contractors that need custom build partners. Our role is the technology execution layer of the state RHTP plan: turning approved application language into production software that meets CMS reporting requirements and clinical workflow needs.
How We Engage on RHTP Implementation
Three typical engagement patterns:
- Direct state contract: We respond to state RFPs for technology implementation work where our capability matches the scope. This typically involves a primary technology deliverable (care coordination platform, FHIR integration layer, clinical AI deployment) over 18-36 months.
- Prime contractor subcontract: We partner with a prime contractor holding the state relationship. The prime handles program management, compliance, and state reporting. We handle technology development. This pattern works well when a consulting firm wins the state contract and needs a custom build partner.
- State eHealth organization partnership: We participate in state innovation programs (sandboxes, vendor directories, technical assistance hubs) to access a wider set of smaller projects and build relationships with state program staff.
What State Program Staff Should Expect
For state RHTP program offices evaluating Mindbowser as a vendor or subcontractor:
- Healthcare-specific compliance posture: HIPAA, HITRUST certification path, SOC 2, state-level requirements we’ve met on prior engagements.
- Rural deployment experience: Our accelerators deployed in resource-constrained environments, not only enterprise settings.
- Implementation-focused timelines: Typical engagements: 12-16 week MVP builds followed by scale phases. Not multi-year waterfall projects.
Conclusion:
The Rural Health Transformation Program is more than a funding initiative. It is a five-year push to stabilize and modernize rural healthcare at a national scale. States now have a rare window to invest in interoperability, care coordination, RPM, clinical AI, and rural-ready care delivery models that can survive beyond the 2030 funding sunset. The organizations that move early and focus on practical, scalable infrastructure instead of disconnected pilot projects will be the ones that strengthen clinician capacity, improve patient access, and create long-term operational stability for rural communities.
The Rural Health Transformation Program (RHTP) is a federal grant program authorized by Section 71401 of Public Law 119-21, administered by CMS. It allocates $50 billion over five fiscal years (FY2026-FY2030) across all 50 states to strengthen rural healthcare access, quality, and outcomes. Each state received an approved five-year plan and runs its own procurement to execute the plan.
All 50 states received FY2026 awards ranging from $147,250,806 (New Jersey) to $281,319,361 (Texas). The complete state-by-state award table is available in the 50-state comparison.
Most states complete internal setup through Q3 2026, then post RFPs between Q3 2026 and Q2 2027. Implementation begins Q1 2027. Technology-specific RFPs tend to cluster in Q4 2026 and Q1 2027. Watch the specific state procurement portal and health department pressroom for posting notifications.
CMS (Centers for Medicare & Medicaid Services) administers the program at the federal level under Funding Opportunity Number CMS-RHT-26-001. At the state level, administration typically sits within the state’s Executive Office of Health and Human Services, Medicaid agency, or equivalent public health coordinating body.
No. Despite frequent informal conflation in search queries, the RHT Program is a CMS program authorized under the One Big Beautiful Bill Act (PL 119-21, Section 71401). HRSA administers separate rural health programs including the Flex Program, SHIP, and Rural Health Clinic program. State plans sometimes reference HRSA programs or build on HRSA-funded infrastructure, but the $50 billion is CMS funding, not HRSA funding.
Yes. Four partnership paths exist: direct state contract (highest value, highest bar to entry), prime contractor subcontract (partner with consulting firms that win state contracts), state eHealth organization partnership (participate in innovation sandboxes and technical assistance hubs), and rural hospital network partnership (implement across multi-hospital networks under a single agreement). Most technology vendors access RHTP work through Paths 2 and 3.
Technology spending can align to several statutory elements: consumer-facing technology (C), training and technical assistance (D), provider technology including EHR, HIE, interoperability, cybersecurity (F), and innovation in delivery including mobile health, hospital-at-home, telehealth (H). Most state plans detail specific technology platforms to build within these elements.
RHTP funding is authorized for five fiscal years: FY2026 through FY2030. The final award cycle happens in FY2030. States begin sustainability planning in Year 4 (2029) to transition funded activities to sustainable non-federal revenue streams (Medicaid reimbursement, value-based payment models, state appropriations) before federal support ends September 30, 2030.
The Rural Health Transformation Program was authorized by Section 71401 of Public Law 119-21, informally known as the One Big Beautiful Bill Act. The One Big Beautiful Bill Act is the full piece of legislation containing many provisions; RHTP is one program within it. When people say “the $50 billion rural health program,” they mean RHTP specifically, which is the Section 71401 authorization.
The exact % varies by state. Massachusetts allocates roughly $374 million of its $1 billion request across the two most technology-heavy initiatives (Population Health Advancement at $291 million, Technology Interoperability at $83 million), or about 37% of the total. Other states run similar or higher technology allocations.
Direct RHTP applications closed in November 2025. CMS awarded all 50 states on December 29, 2025, so individual hospitals, health systems, and vendors cannot apply directly for the $10 billion per year. Instead, engagement happens through state procurement: each state runs its own RFP cycle (most between Q3 2026 and Q1 2027) for the technology, workforce, and facility investments its approved plan requires. Vendors and health systems engage by (1) bidding on state-issued RFPs, (2) subcontracting through prime consulting firms that win state contracts, (3) partnering with state eHealth organizations like MeHI that manage innovation sandboxes, or (4) joining rural hospital networks that share-service across state RHTP allocations.
