



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
A 25-bed rural hospital running a Medicare chronic care management program with 200 enrolled patients needs the work of three full-time care coordinators and usually has only one. AI now replaces three specific workflow FTEs: intake coordinator, documentation specialist, and patient outreach FTE, without replacing clinical judgment. The math, the mechanisms, and the Rural Health Transformation Program funding pathway are below.
Opening: The Math Nobody Wants to Say Out Loud
A 25-bed rural hospital running a Medicare chronic care management program with 200 enrolled patients needs the equivalent of three full-time care coordinators to do the work correctly, and most rural hospitals have one.
I have sat in enough CMIO conversations to watch the same thing happen. A rural CNO says the CCM program is “running.” I ask how many patients are enrolled. She says 200. I ask how many care coordinators are on the team. She says one, maybe one and a half with a float nurse. I pull up my notepad and walk through the math on the back of it.
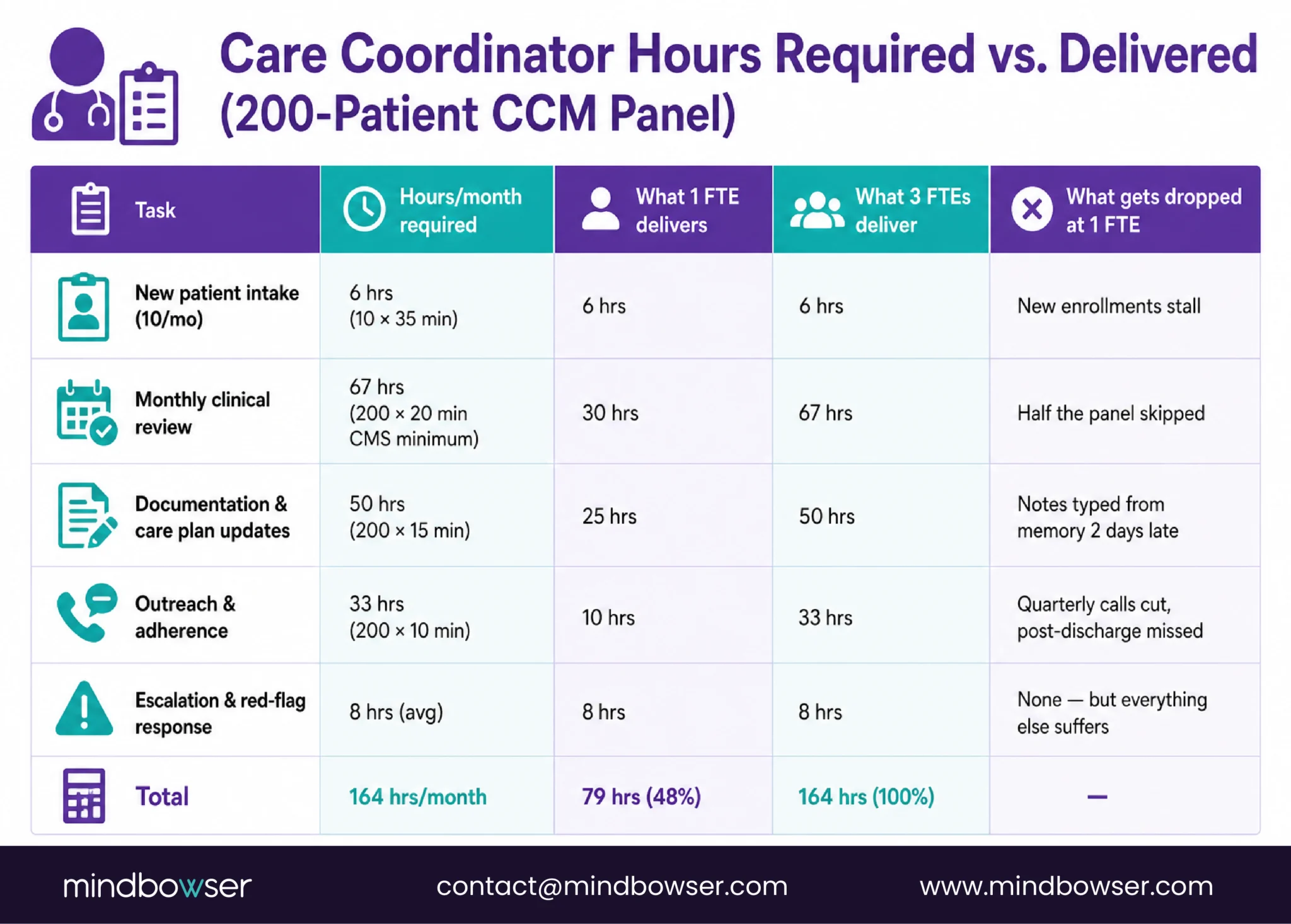
CMS requires at least 20 minutes of clinical staff time per patient per month to bill the standard chronic care management code. That is 200 patients × 20 minutes = 4,000 minutes per month, or 67 hours. One full-time care coordinator has 160 productive hours per month after meetings, documentation time, lunches, and the occasional clinic coverage. 67 hours is 42 % of that FTE’s month, which on paper looks doable.
But care coordination is not billing time alone. It is intake, consent, care plan creation, monthly chart review, medication reconciliation, patient outreach, documentation, adherence checks, escalation management, and the thousand small calls that keep a chronic disease population out of the ED. Those hours do not fit in 42 % of one FTE’s month. They fit in three FTEs’ months. And rural hospitals have one.
That is the problem. AI is the solution, but only the part of it I am about to describe.
Why Rural Care Management Is Mathematically Impossible Without Automation
Before I tell you which FTEs AI replaces, I want to show you the math that forces the conversation.
The Medicare chronic care management codes, CPT 99490 (standard, 20 min), CPT 99491 (provider-delivered, 30 min), CPT 99487 (complex CCM, 60 min), CPT 99489 (complex add-on, 30 min), require documented clinical time. CMS audit trails require the documentation to name what was done, when, and by whom. The 20-minute floor is a floor, not a ceiling.
The workforce math behind this is severe. HRSA’s nursing workforce projections document a 25 % rural (non-metro) nursing shortage for 2026, compared to just 5 % in metro areas, a five-to-one gap. Over the 2026-2036 decade, HRSA projects the rural shortage averaging 14 % versus 2 % metro. AAMC’s March 2024 physician workforce projection warns of a national shortage of up to 86,000 physicians by 2036, with the gap most severe in nonmetro areas and primary care disciplines. The national RN vacancy rate sat at 9.6 % in 2024, and that figure materially understates what the rural segment faces. The median rural hospital employing a CCM program has one or two care coordinators covering what larger systems staff at three to five. The shortage is structural: rural nursing supply is thin, competition with urban hospitals within driving distance siphons talent, and travel-nurse premiums have eaten the salary math that used to keep rural retention reasonable.
Here is what I see fail when one FTE is doing three FTEs of work:
- Patient outreach gets dropped first: The quarterly adherence calls, the refill check-ins, the post-discharge phone calls. None of these are billable individually, so they are the first thing to slide when the month runs out of hours.
- Documentation lags behind care: Notes get written two days after the call, from memory. The 20-minute floor is hit on paper because the note says so, but nobody can reconstruct whether it actually was. Audit risk.
- Escalations get missed: A medication adherence drop that should trigger a 72-hour call becomes a two-week gap. By then the patient is in the ED.
- New enrollments stall: Intake is front-loaded work. When the care coordinator is already underwater on existing panels, she stops enrolling new patients. The program stops growing at the moment rural Medicare populations most need it to grow.
This is not a staffing problem you can solve by hiring. The nurses are not available at the price the rural P&L supports. It is an automation problem. The pieces of the care coordinator’s job that are structured and repetitive can be done by AI. The pieces that require clinical judgment stay with the human. That is the entire argument.
Which 3 FTEs Does AI Actually Replace?
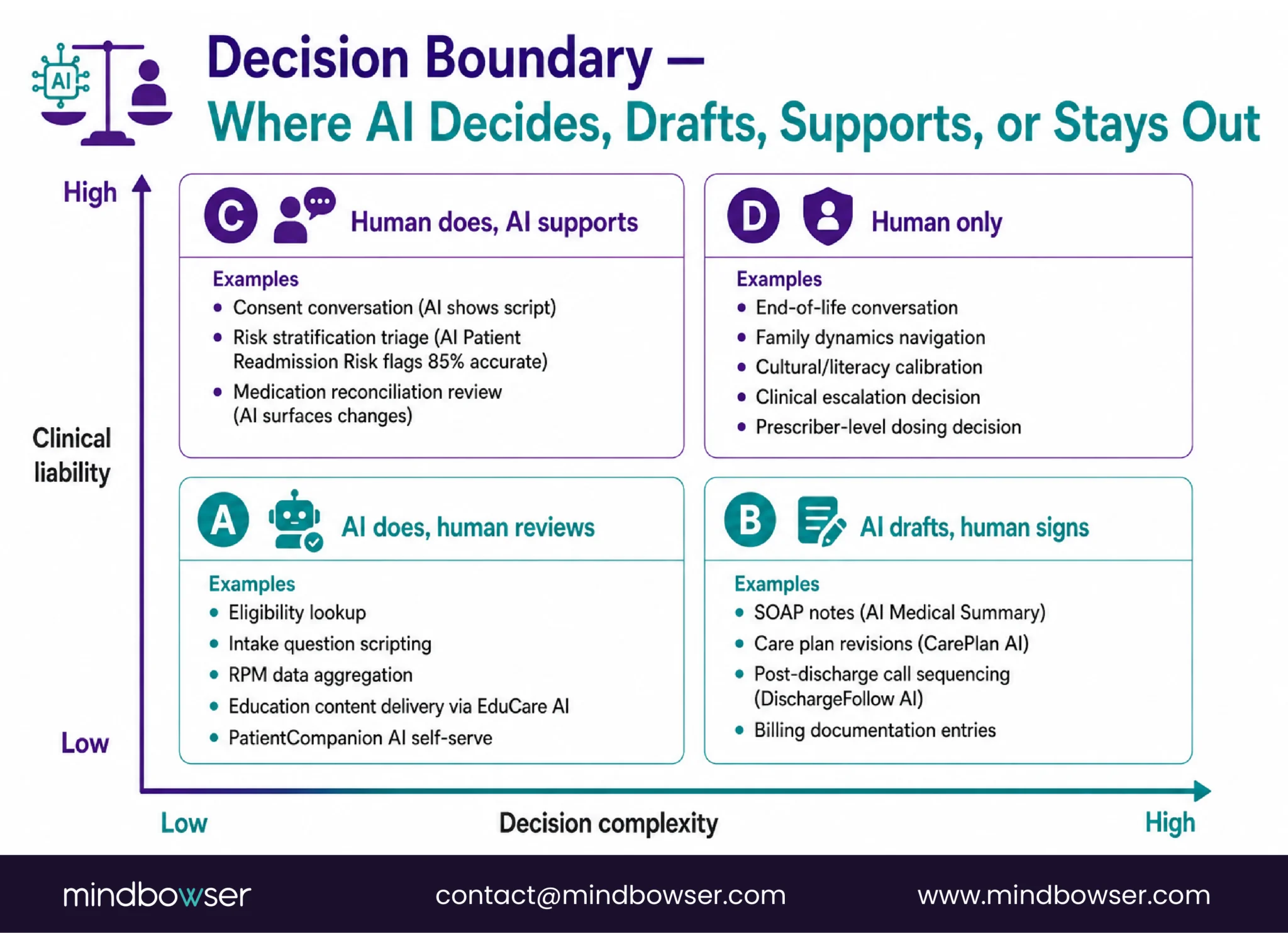
I get asked this question as “can AI replace the care coordinator.” The answer is no. AI cannot replace the care coordinator’s clinical judgment, escalation decisions, or patient relationship. AI replaces three specific functional FTEs that the care coordinator has to do because there is no one else to do them.
The three FTEs AI replaces:
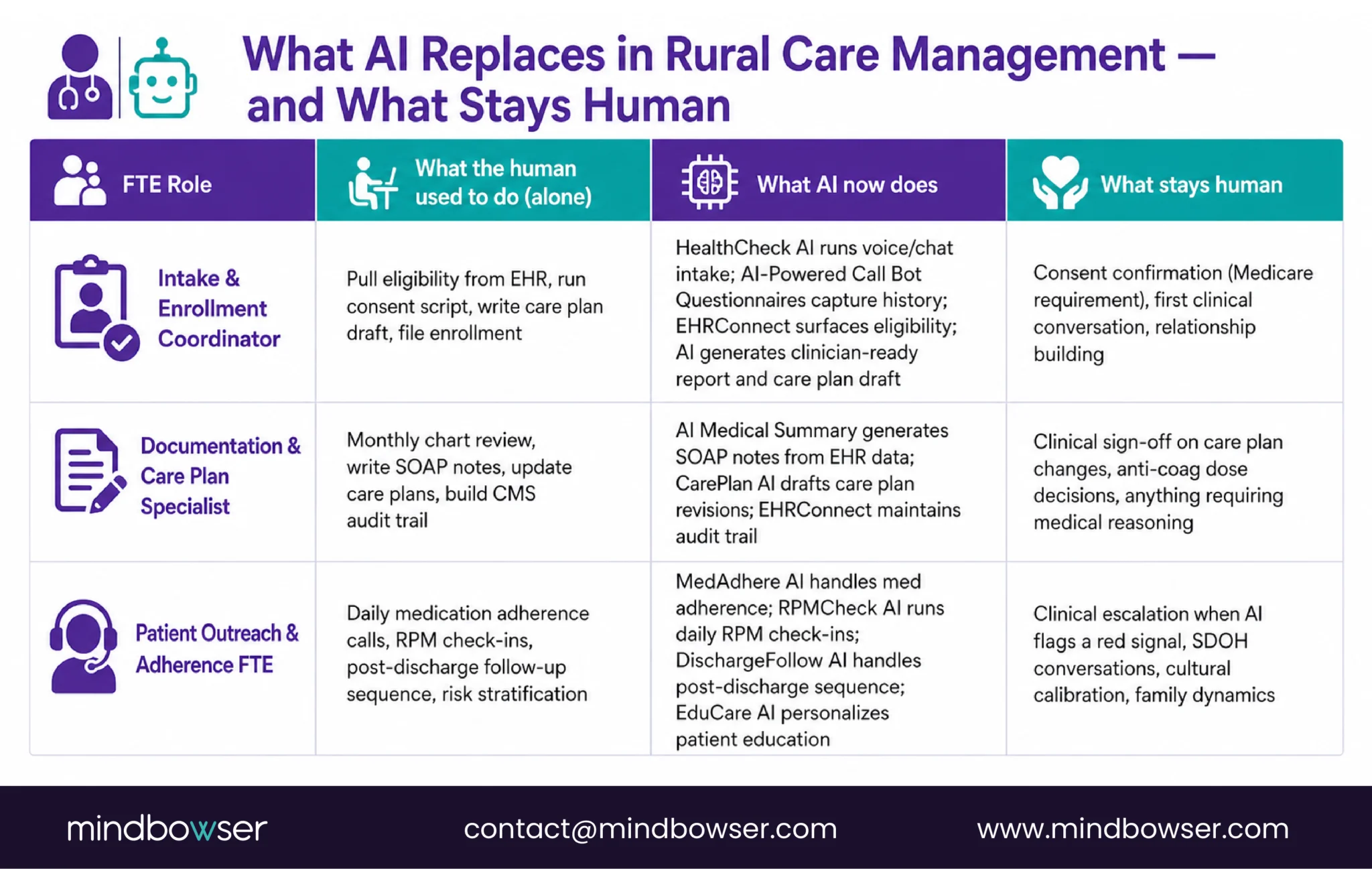
- The Intake & Enrollment Coordinator FTE: Eligibility screening, consent scripts, initial care plan drafts, enrollment into the CMS-billable CCM program. Structured, repeatable, high-volume.
- The Documentation & Care Plan Specialist FTE: Monthly chart review, care plan updates from the latest labs and vitals, encounter notes from virtual check-ins, CMS billing audit trail. Structured, time-consuming, detail-sensitive.
- The Patient Outreach & Adherence FTE: Scheduled check-ins, medication adherence monitoring, post-discharge calls, risk stratification for prioritized attention. Structured, high-volume, emotionally thankless when done well.
What stays human: clinical escalation decisions, care plan changes that require medical reasoning, end-of-life conversations, family dynamics navigation, the patient relationship itself.
The rest of this piece walks through each FTE in workflow detail. The goal is not to convince you AI is magic. It is to show you the specific workflow handoffs that work in a 25-bed rural hospital, the ones that don’t, and what the Rural Health Transformation Program will fund.
FTE 1: AI Replaces the Intake & Enrollment Coordinator
Picture the care coordinator at 9 a.m. on a Tuesday. Her first scheduled task is enrolling a new CCM patient, Mrs. R, 71, two chronic conditions, Medicare-eligible, referred from the primary care clinic downstairs. On paper this takes 30 minutes. In practice she spends 10 minutes trying to find Mrs. R’s most recent lab draw in the EHR because the PCP’s note referenced a result that isn’t in the problem list. She spends 12 minutes on the intake phone call, half of which is Mrs. R describing which grandchild has been visiting. She spends 8 minutes on the consent conversation. She spends 15 minutes writing the initial care plan. She has not yet entered the billing code. And she has nine more enrollments on her list for this week.
That is what FTE 1 looks like, structured work wrapped in unstructured human time, every patient getting the same rough script in the same rough order. The structured portion is what AI handles. The unstructured portion stays human.
What the workflow actually needs, step by step:
- Eligibility signals pulled from the EHR before the phone call, not during it
- A voice or chat intake that captures patient-reported history in the patient’s preferred channel
- A structured clinician-ready report ready for the care coordinator before she picks up the phone
- Consent confirmation through a human (Medicare requires it; the AI drafts the script)
- The first real clinical conversation, patient relationship, tone calibration, edge cases, as a human touchpoint
- FHIR-compliant logging of everything so the billing audit trail holds up
Four of those six steps can be handled by pre-built AI agents. Two stay human.
On the AI side: HealthCheck AI is already running the pre-checkup intake in production via voice or chat and generating the structured clinician report (+32 % check-up completion, -50 % manual outreach time). For rural programs that want voice-first intake at scale, AI-Powered Call Bot Questionnaires is the underlying agent with FHIR logging built in; AI-Powered Chat-Based Questionnaire covers the text-preferring patient segment. The EHR integration that ties it all together runs through HealthConnect CoPilot, the FHIR fabric that collapses the “6-month custom integration project” into weeks instead of quarters.
On the human side: consent confirmation, first clinical touch, relationship-building. No accelerator replaces these. The care coordinator does them. AI gives her 40 more minutes per enrollment to do them well.
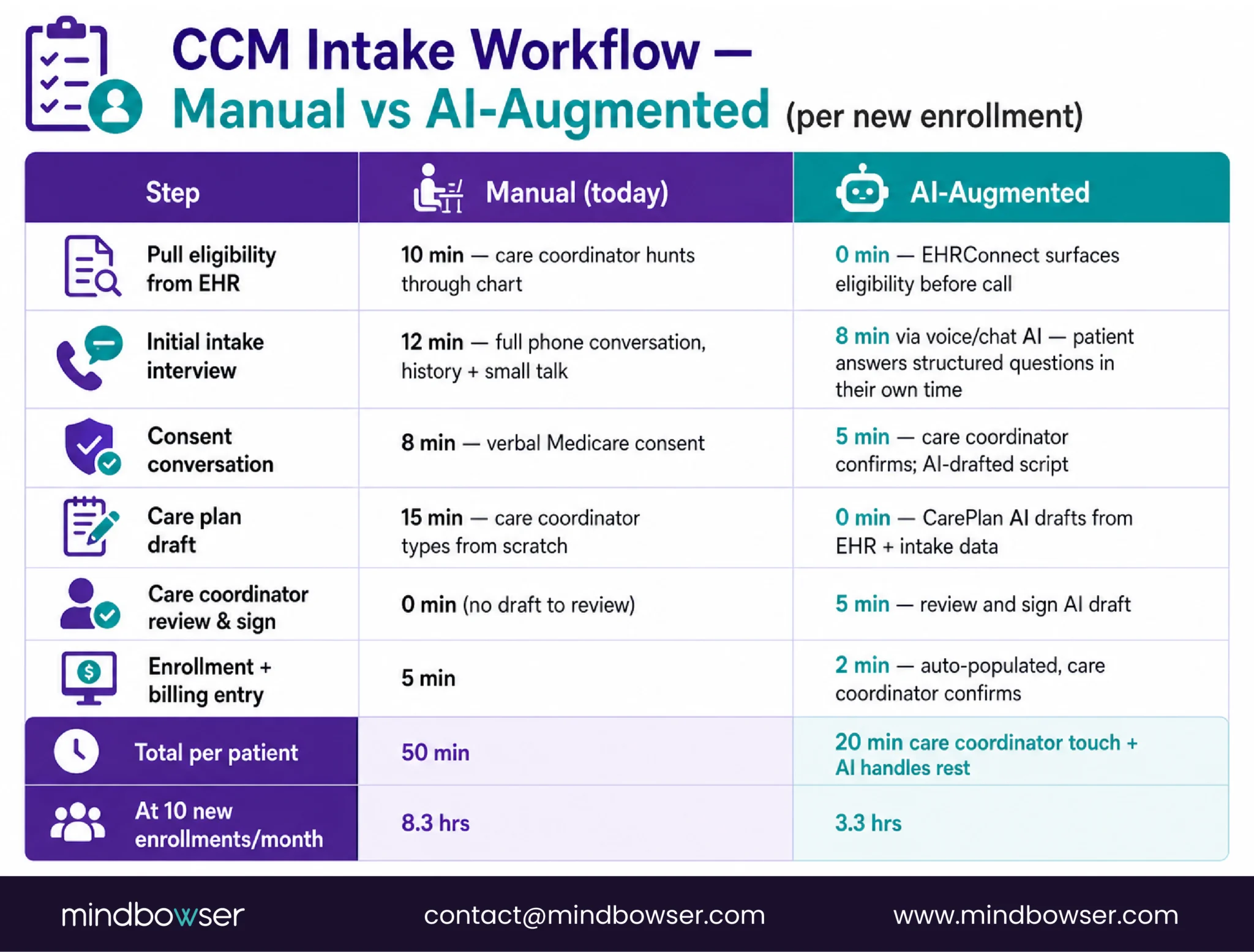
The math: a rural hospital enrolling 10 new CCM patients per month previously burned 5-7 hours of care coordinator time on intake alone. An AI-augmented flow takes that to under 2 hours. Four to five hours per month, back to the care coordinator’s panel.
FTE 2: AI Replaces the Documentation & Care Plan Specialist
It is 6:47 p.m. on a Thursday. The care coordinator has done eight patient calls today. She is trying to write eight monthly CCM notes from memory, two of them from calls she took on Tuesday. She opens the first chart, clicks through three screens to reach the care management documentation field, and types a sentence that sounds vaguely like what the call was about. The patient mentioned a new medication. She thinks it was Tuesday. She thinks it was a blood pressure medication. She writes “patient reports medication change, reconciled” and moves on.
That is 4,000 minutes of documentation every month on 200 patients, much of it reconstructed two days later in fields three clicks deep. CMS wants it to name the intervention, capture the clinical reasoning, and hold up to an audit. The fraction that actually does is smaller than any CMO wants to admit.
What the workflow actually needs:
- Real-time capture of the clinical conversation, ambient if possible, structured regardless
- A SOAP-style note generated from the conversation, reviewed and signed by the human clinician
- A care plan revision drafted from the latest labs, vitals, and medication changes, ready for sign-off
- A billing-ready audit trail that names who did what, when, and why
- Clean integration with whichever EHR the rural hospital already runs (Meditech, Epic Community Connect, Athenahealth, Cerner CommunityWorks, Praxis, others)
- Quality measure population (HEDIS, CMS Star Ratings, state-specific measures), which is NOT an accelerator, it’s a custom reporting layer built per-program against the specific measure set the payers and state require
Two of those six have pre-built agents: AI Medical Summary produces SOAP-style documentation from raw EHR records (-50 % documentation time, +45 % accuracy, 3x faster patient insight access). CarePlan AI drafts the care plan revision from current clinical data (+37 % patient understanding of the resulting plan, plans nobody understands are plans nobody follows).
One of them is integration infrastructure: EHRConnect is the zero-code interop fabric that turns a 6-month Epic or Athenahealth integration into a 6-day one. For a rural program deciding between full EHR integration up front or “temporary” manual data entry that never gets fixed, the pre-built fabric makes the right choice affordable.
One of them, the quality measure reporting layer, has no packaged accelerator and usually shouldn’t. Every rural program has a different measure mix based on their payer contracts, state RHTP requirements, and clinical priorities. The custom reporting layer is part of the engagement, not a product purchase.
What stays human: the clinical judgment on care plan changes that matter. AI drafts the care plan update; the care coordinator reviews it and signs off. If the AI suggests adjusting an anti-coagulation dose based on a recent INR, that suggestion goes to the provider, not into the chart. The care plan AI is a draft engine, not a prescriber.
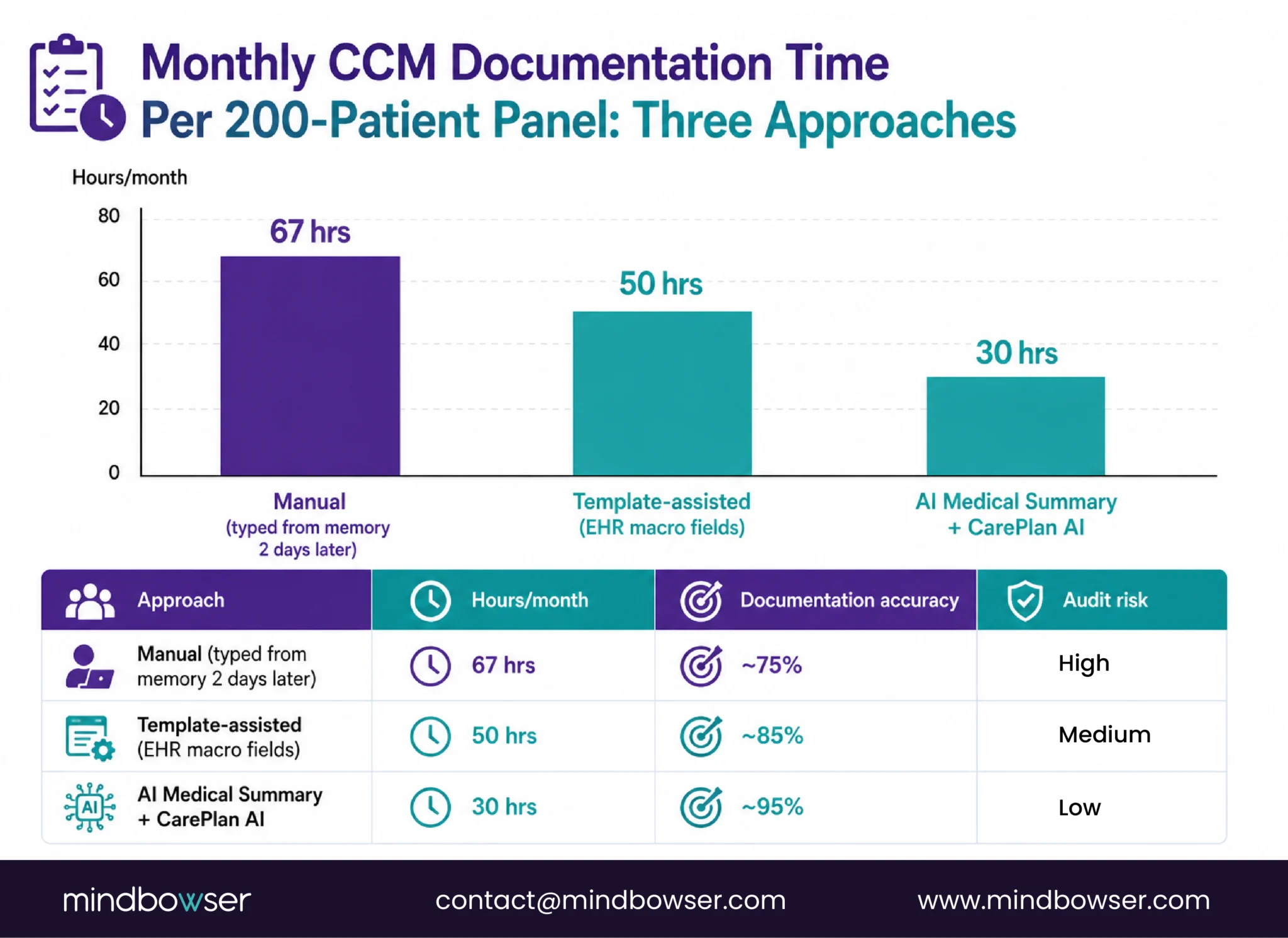
The math I show rural CNOs: for 200 enrolled patients, AI Medical Summary and CarePlan AI pull 30-50 documentation hours per month back into the care coordinator’s panel. Combined with the intake savings, that is closing in on one full FTE recovered from automation alone.
FTE 3: AI Replaces the Patient Outreach & Adherence FTE
It is Friday afternoon. The care coordinator has a list of 47 patients she was supposed to call this week for refill check-ins and post-discharge follow-ups. She has called 19 of them. Fourteen went to voicemail. She left messages, in voice she tries to keep warm, knowing most of those patients will not call back. The remaining 28 patients on her list get pushed to next week, where they will compete with next week’s 47 new calls. Three months of this pattern and the CHF patient who stopped taking her diuretic six weeks ago shows up in the ED with acute decompensation. Her chart says the care coordinator “attempted outreach.” Nobody is wrong; the math was always going to end here.
That is FTE 3. High-volume, mostly voicemail, emotionally draining when done right, the first thing that slides when the month runs out of hours.
What the workflow actually needs:
- Medication adherence monitoring with multi-channel outreach that meets patients where they are (SMS, email, app, voice)
- Daily RPM check-ins that capture vitals and symptom responses without requiring the care coordinator to chase them
- A 7/14/30-day post-discharge follow-up sequence with red-flag escalation
- Escalation to a human clinician ONLY when the data says a human is needed
- SDOH screening and response, food insecurity, housing, transportation, caregiver burden, which is NOT primarily an AI workflow. It’s a human conversation supported by community-resource referral. AI helps identify who to screen; humans do the screening.
- Culturally calibrated communication for rural multi-generational households, also human, also no accelerator
Three pre-built agents cover the core outreach volume in production: MedAdhere AI for medication adherence (+26 % adherence, -12 % ER visits from missed meds), RPMCheck AI for daily RPM check-ins (+38 % check-in completion), and DischargeFollow AI for the post-discharge window (-38 % 30-day readmissions, -40 % manual follow-up call volume). Each one replaces an FTE-hour category the rural care coordinator cannot afford to do well right now.
Two more fill supporting roles: EduCare AI handles personalized patient education by condition, language, and literacy level, important for rural populations with varied health literacy. PatientCompanion AI lets patients self-serve their own EHR data instead of calling the care coordinator to ask what their A1c was (-30 % admin follow-up calls). The device data underneath flows through WearConnect, 300-plus wearables and trackers unified into a single FHIR interface, so the AI agents respond to real data instead of guessing.
Two parts of FTE 3 have no accelerator on purpose: SDOH screening and culturally-calibrated communication. These are human work that AI can flag into but cannot replace. A rural program that tries to automate the SDOH conversation will damage trust with the population most likely to drop out of the CCM program as a result. The engagement includes workflow design for the human-led pieces, not a product stand-in.
For a rural program, the architectural question is which FTE-3 function has the highest current ROI, MedAdhere for a diabetes-heavy panel, DischargeFollow for a CHF population with readmission pressure, and which pre-built agent addresses it. Start there, expand from there, keep SDOH and cultural work human.
What stays human: clinical escalation. When MedAdhere AI flags a patient who has missed three doses of a blood thinner, the next step is a human clinical call, not another automated message. When DischargeFollow AI detects a patient reporting new-onset chest pain, the care team gets paged immediately and a human takes over.
Looking to optimize rural care management with AI-driven workflows?
What AI Cannot Replace (and Should Not)
I am as enthusiastic about AI in care management as anyone on this roster, and I will draw the line clearly. There are things AI cannot replace in rural care management, and there are things it can but should not.
- Clinical judgment on escalation: AI Patient Readmission Risk, our predictive model, flags patients at 30-day readmission risk with 85 % accuracy. That is excellent for a prediction tool. It is not a clinical decision. The case manager looks at the flag, pulls the chart, looks at the SDOH factors, talks to the patient if possible, and decides whether to call the provider or wait another 48 hours. The AI informs the decision; the human makes it. If you deploy a predictive risk model and configure it to auto-escalate to the provider without a human review step, you will produce alert fatigue and the model will be ignored within 90 days.
- End-of-life conversations: These cannot be delegated to an AI and should not be attempted by one. The care coordinator who has the relationship with the patient has the conversation. Full stop.
- Family dynamics. Rural populations run multi-generational and often have complicated family care structures. The daughter who has the power of attorney, the son who thinks he does, the spouse who is in denial about the diagnosis. AI cannot navigate this. The care coordinator does.
- Cultural context and literacy calibration: AI models are trained on population-level data. The rural care coordinator knows that this particular patient with a sixth-grade education and a skepticism of the medical system needs a different conversation than the retired teacher two counties over. Those are human judgment calls.
- Clinical liability: The care coordinator signs the note. The AI does not have malpractice insurance. Any workflow design that puts AI in the decision seat for something that a human should be deciding is a compliance and liability failure waiting to happen.
The hospitals that deploy AI well in care management treat it as an augmentation of the care coordinator, not a replacement. The ones that treat it as a full replacement generate adoption resistance, clinical incidents, and eventually a lawsuit.
Rural AI Deployment Constraints: What Makes Rural Different
I want to be direct about why rural AI deployments fail when they follow urban playbooks.
- Low bandwidth: The FCC’s 2024 Section 706 Broadband Deployment Report documents that roughly 16.9 % of rural Americans lack access at the older 25/3 Mbps threshold and approximately 28 % lack access at the current 100/20 Mbps standard. AI models that assume cloud inference over reliable high-bandwidth connections degrade in rural environments. Cellular-first architecture with edge inference for latency-sensitive workflows is not optional; it is how rural AI deployments work.
- Low IT staff: The median rural CAH has one to two IT people. They cannot operate a complex AI-ops stack. Deployments have to run with minimal ongoing administration, which means managed cloud infrastructure with healthcare-grade compliance built in.
- Older patient demographics: Rural patient median age is 72. Digital literacy varies. The outreach AI has to gracefully handle patients who prefer voice, patients who use SMS through a caregiver, and patients who will not touch an app regardless. This is solvable but only if the deployment is designed for it.
- EHR diversity: Rural hospitals run Meditech, Epic Community Connect, Athenahealth, Cerner CommunityWorks, Praxis, and half a dozen others. The AI layer has to integrate with whatever EHR the hospital already has. Ripping and replacing the EHR is not on the table.
- HIPAA + AI compliance: Running AI workloads on PHI without the compliance layer is a regulatory incident. PHISecure handles PHI de-identification from DICOM, NIfTI, video, and standard image formats, 18 identifiers removed automatically, so AI workloads run on compliant data. This is table stakes for any rural AI care management deployment.
The rural hospitals that get AI deployment right choose architecture that fits rural constraints upfront. The ones that port an urban AI stack to rural connectivity discover the failure modes three months into production.
ONC AI Transparency Rule and FDA AI/ML CDS: What Compliance Looks Like in 2026
Two regulatory fronts shape what rural AI care management deployments can legally do in 2026.
ONC HTI-1 Final Rule (Predictive Decision Support Interventions): The HTI-1 rule from ONC went into effect in 2025-2026 and requires transparency for predictive decision-support interventions baked into certified health IT. If your EHR surfaces a predictive risk score, the vendor has to provide a source attribute document, what data trained the model, on what population, with what performance characteristics. Rural CMOs evaluating AI vendors should ask for this document on day one. Vendors that cannot produce it are not compliant with the rule that their EHR integration partners will ask about.
FDA Software as a Medical Device (SaMD) AI/ML guidance: Clinical AI that changes treatment decisions crosses into medical device territory. A predictive risk score that informs a care coordinator is decision-support. A predictive risk score that auto-adjusts an insulin dose is a medical device. The FDA’s AI/ML guidance governs which bucket a tool falls into. For rural care management, most AI stays on the decision-support side of the line, but as autonomous care plan adjustment becomes more common, hospitals will need to evaluate SaMD classification on a tool-by-tool basis.
Vendor evaluation checklist I use:
- HTI-1 source attribute document available for every predictive model
- FDA SaMD classification status (or clear argument for why not applicable)
- HIPAA BAA signed before any PHI touches the vendor infrastructure
- Audit trail for every AI-generated documentation entry (who saw it, who accepted it, what changed)
- Model performance data on a rural patient population (not just urban academic medical center data)
- Clinician-override capability on every AI recommendation
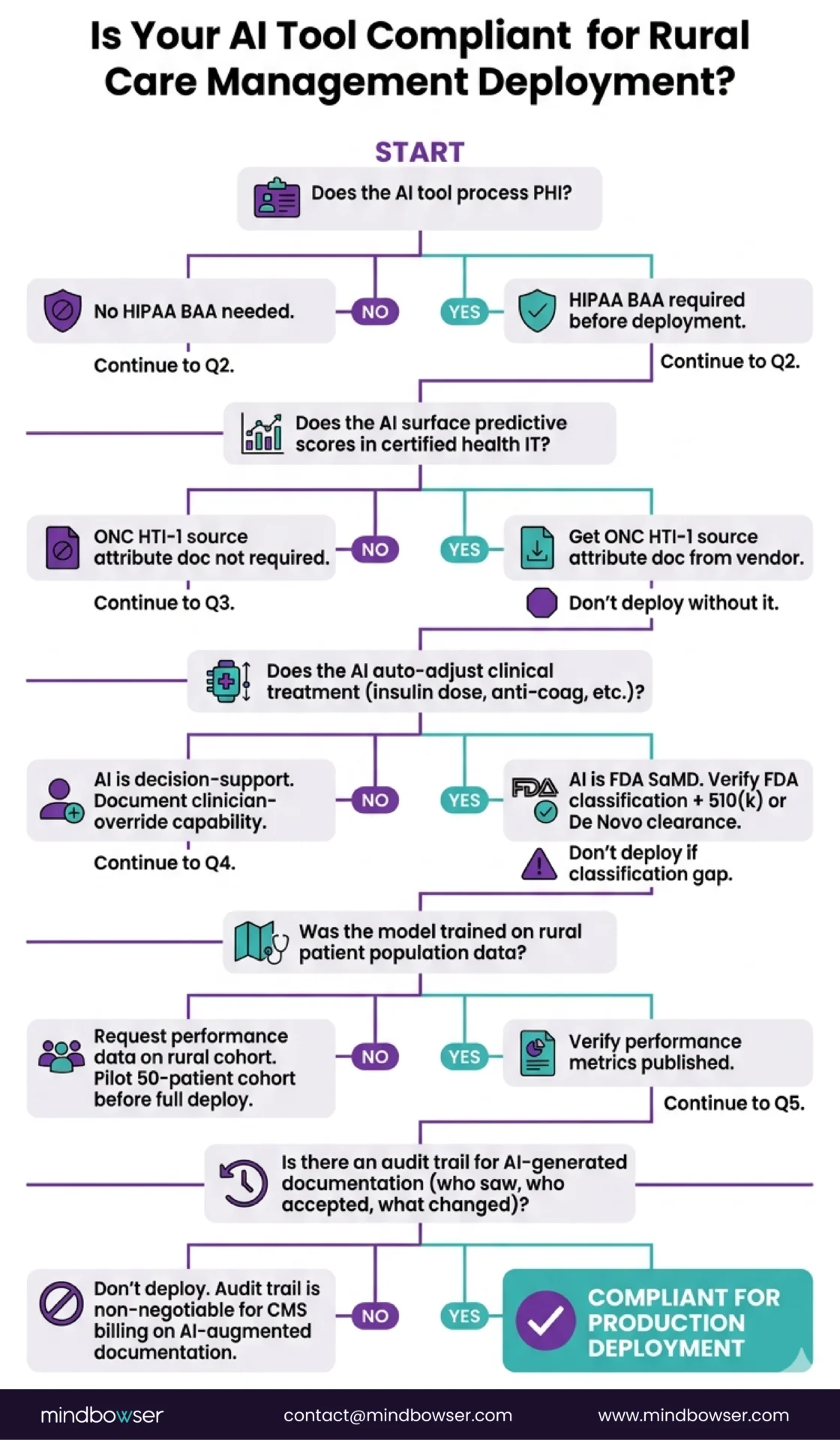
Compliance is not a reason to avoid AI in rural care management. It is the reason to pick the right AI.
How RHTP Funding Pays for Rural AI Care Management Deployment
The Rural Health Transformation Program, 50 billion dollars across all 50 states, FY2026 through FY2030, is the largest rural healthcare capital injection in a generation. Clinical AI is a named funded activity in multiple state RHTP plans.
States with explicit clinical AI funding in their RHTP plans include:
- Utah, clinical AI agents across rural primary care and post-acute workflows
- Maine, the Rural AI Hub initiative connecting CAHs with a statewide AI delivery platform
- Montana, AI monitoring for chronic disease management in Frontier-designated counties
- Multiple other states include clinical AI under broader rural specialty access or workforce initiatives
What RHTP funds for rural AI care management:
- Platform licensing and deployment capital
- Integration services (EHRConnect deployment, FHIR layer setup)
- Care coordinator training on AI-augmented workflow
- Clinical quality measurement infrastructure
- Patient onboarding for outreach and RPM AI layers
- Network upgrades not covered by FCC Rural Health Care Program
What RHTP does not typically fund:
- Ongoing operating losses on AI tools that should be self-sustaining via billable workflows
- Replacement of existing CMS-reimbursable infrastructure
- Capital that should come from FCC RHCP or USDA DLT
The procurement windows opened in Q3 2026 and most state RFPs will close by Q1 2027. Rural hospitals positioning for RHTP clinical AI funding should scope their applications as integrated care management transformation programs rather than as AI tool purchases. State program offices are scoring proposals on measurable rural access and outcomes improvement, not on technology line items.
State RHTP program managers evaluating AI care management proposals are looking for: clinical workflow redesign already scoped (not just “we will buy an AI tool”), care coordinator staffing model that assumes augmentation not replacement, compliance documentation in place, measurement framework specified.
Where Rural AI Care Management Deployments Fail (and How to Avoid It)
Six failure patterns I see in rural AI care management deployments.
- Failure 1: Vendor pilot trap: Hospital signs a six-month pilot with a vendor. The pilot produces great-looking metrics on a 20-patient cohort. Hospital scales to 200 patients and the metrics collapse because the pilot had hand-selected patients, dedicated vendor support, and a coordinator who was freed up specifically for the pilot. Avoidance: scale the pilot to production conditions before signing the full contract.
- Failure 2: No clinician in the design loop: IT and vendor configure the AI workflow. Care coordinators see it for the first time at go-live. Adoption dies within 60 days because the workflow was designed without the people who run it. Avoidance: care coordinators in the design loop from week one. This is not negotiable.
- Failure 3: Integration shortcuts: Deployment team decides to launch on a “temporary” manual data entry workflow because full EHR integration is behind schedule. Six months later the manual workflow is still in place, care coordinators are doing double-entry, and AI-generated documentation is drifting from EHR truth. Avoidance: full integration before production launch, not after.
- Failure 4: Compliance as afterthought: Team deploys AI tools on PHI without running the HIPAA BAA process, the HTI-1 source attribute documentation, or the audit trail configuration. Nine months in, the first audit surfaces the gaps. Avoidance: compliance review in parallel with technical deployment, not after.
- Failure 5: No measurement framework: Program runs for 18 months without reliable data on adherence lift, readmission reduction, or FTE recovery. Renewal decisions get made on anecdote. Avoidance: measurement framework, enrollment, completion rates, clinical outcomes, financial performance, defined upfront. Tracked from day one.
- Failure 6: AI-as-feature, not AI-as-program: Hospital treats AI as a product the care coordinator uses instead of as a workflow transformation. The care coordinator keeps doing the work manually and the AI becomes a second system to maintain. Avoidance: workflow redesign is the project, not AI procurement.
How Mindbowser Helps Rural Hospitals Deploy AI in Care Management
The transformation rural hospitals need is to turn one care coordinator into the equivalent of three functional FTEs without replacing clinical judgment. That is a workflow redesign, not a product purchase.
Mindbowser approaches it as a workflow redesign with pre-built agents as the shortcut. The three FTE functions map to agents that already run in production, HealthCheck AI, AI Medical Summary, CarePlan AI, MedAdhere AI, RPMCheck AI, DischargeFollow AI, EHRConnect, and the supporting integration and compliance layers. Rural programs starting from this stack skip 6-9 months of from-scratch build and go live in 90-120 days instead.
The engagement includes workflow design, care coordinator training on augmented workflow, compliance scoping (ONC HTI-1 source attribution, FDA SaMD classification, HIPAA BAA), EHR integration via the pre-built interop fabric, and RHTP funding application support where the rural program is positioning for state technology procurements.
For state RHTP program offices evaluating technology partners, the value is deployment risk reduction: the accelerators are already built and already producing outcome data (cited throughout this piece). State dollars funded under RHTP plans go further when they do not have to pay for a ground-up build.
Intake & Enrollment Coordinator (eligibility, consent, care plan draft, enrollment), Documentation & Care Plan Specialist (chart review, care plan updates, encounter notes, billing documentation), and Patient Outreach & Adherence FTE (scheduled check-ins, medication adherence, post-discharge follow-up, risk stratification). Clinical judgment, escalation decisions, and the patient relationship stay with the human care coordinator.
Clinical escalation decisions, end-of-life conversations, family dynamics navigation, cultural context calibration, clinical liability signing authority, and the care coordinator’s patient relationship. AI informs these; it does not decide.
AI-generated documentation is billable under standard CMS CCM codes (99490, 99491, 99487, 99489) as long as clinical time is documented and a human clinician reviews and signs. The AI is a documentation tool; the billable event is still the human clinical time. Audit trails must capture who reviewed the AI-generated note and when.
Source attribute documentation for every predictive decision-support intervention in certified health IT, what data trained the model, on what population, with what performance metrics. Rural hospitals should require this document from AI vendors before contract signature.
Via cellular-first architecture with edge inference for latency-sensitive workflows and managed cloud inference for batch/analysis workloads. Voice-based AI outreach (MedAdhere, RPMCheck, DischargeFollow) runs over cellular voice networks, which have better rural coverage than broadband.
Yes. Clinical AI is a named funded activity in RHTP plans from Utah, Maine, Montana, and others. RHTP can fund platform licensing, integration services, care coordinator training, patient onboarding, and compliance infrastructure. Procurement windows opened Q3 2026 and extend through Q1 2027.
90-120 days from contract signature to production go-live is the target for a 25-bed rural hospital deploying the full stack (intake + documentation + outreach AI). First 30 days: workflow design + EHR integration. Days 31-60: AI configuration + care coordinator training. Days 61-90: pilot cohort of 25-50 patients. Days 91-120: scale to production enrollment.

