



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
Technology decisions at a 25-bed Critical Access Hospital are shaped by three constraints that do not exist at any larger hospital: a 1-2 person IT team, cost-based Medicare reimbursement that does not fund capital, and a rural patient population facing significant broadband gaps at modern benchmarks. The right stack covers seven components: EHR (typically MEDITECH Expanse, Epic Community Connect, or Athena), revenue cycle management, clinical documentation AI, remote patient monitoring, telehealth specialty access, cybersecurity, and an integration layer pulling them together. RHTP funding shifts the capital equation for the first time in the program’s history, with state procurement windows opening Q3 2026.
Technology decisions at a 25-bed Critical Access Hospital are shaped by three constraints that do not exist at any larger hospital: a 1-2 person IT team, cost-based Medicare reimbursement that does not fund capital, and a patient population facing significant broadband gaps at modern speed standards.
These constraints get treated as edge cases in most healthcare technology guides. At a 25-bed hospital they are the design center.
The 1-IT-person reality means operationally simple beats feature-rich every time. A platform that requires a DevOps engineer to maintain is not a deployment option, regardless of how good its capabilities are. The cost-based reimbursement reality means capital investment cannot be amortized through Medicare margin in the way PPS hospitals can. Capital comes from grants (HRSA Flex, RHTP, state rural health), from facility renovation budgets, or from operating reserves that most CAHs do not have. The broadband reality means patient-facing technology often defaults to cellular rather than WiFi. The FCC’s 2024 Section 706 Broadband Deployment Report found that approximately 28% of rural Americans lack access to the current 100/20 Mbps broadband standard (with roughly 16.9% of rural Americans still lacking the older 25/3 Mbps threshold). RPM devices and telehealth platforms that assume consumer home WiFi exclude a meaningful share of the rural patient population. Cellular-first architecture is not a nicety; it is the default that fits rural deployment reality.
This guide covers what we would build for a 25-bed rural hospital today, given those constraints and given the new RHTP funding environment.
I. What Technology Stack Does a Critical Access Hospital Actually Need?
Seven components. Not five, not twelve. The boundary between them matters because each component has different vendor markets, different funding mechanisms, and different operational footprints.
| # | Component | Purpose at a 25-bed hospital | Typical lead vendor patterns |
|---|---|---|---|
| 1 | EHR | Clinical documentation, orders, results, billing | MEDITECH Expanse, Epic Community Connect, Athena, eClinicalWorks |
| 2 | Revenue Cycle Management (RCM) | Claims, denials, patient financial services | Athena, Cerner, R1, third-party RCM services |
| 3 | Clinical Documentation AI | Reduce physician documentation burden | Suki, Abridge, Nuance DAX, Mindbowser AI Medical Summary |
| 4 | Remote Patient Monitoring (RPM) | Chronic disease, post-acute monitoring | WearConnect, vendor-specific platforms |
| 5 | Telehealth | Specialty consults, behavioral health access | Hub-and-spoke arrangements with academic medical centers, telepsych vendors |
| 6 | Cybersecurity + HIPAA Compliance | Managed security, HIPAA posture | PHISecure, Managed Security Service Providers (MSSPs), state Health-ISAC participation |
| 7 | Integration Layer | FHIR, HL7, API gateway, event routing | HealthConnect CoPilot, Mirth Connect, Redox, Rhapsody |
The order matters. EHR is the operational anchor. Everything else integrates with it. The integration layer is the connective tissue that makes the rest of the stack function as a coherent system rather than a collection of unrelated point tools.
For the broader CAH context including history, requirements, and reimbursement mechanics, see What Is a Critical Access Hospital.
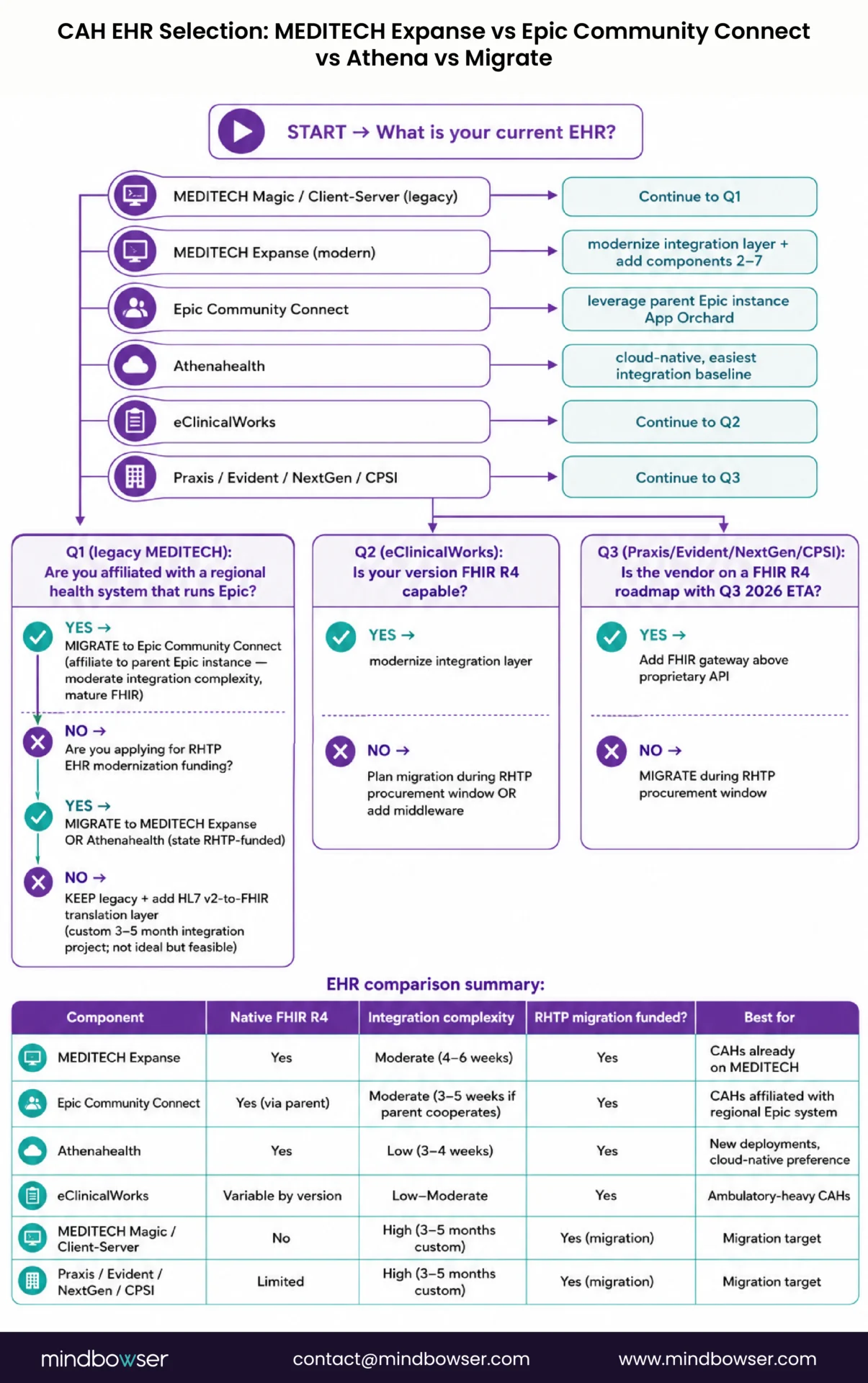
II. EHR: MEDITECH Expanse, Epic Community Connect, or Migrate?
The EHR decision is the most consequential technology choice a CAH makes. It shapes the integration layer, the workforce training burden, the data architecture, and the realistic scope of every other technology component for the next 7-10 years.
Three viable paths exist for most CAHs in 2026:
- Path 1: MEDITECH Expanse (most common). Roughly half of CAHs run some version of MEDITECH. Expanse is the modern web-based version (replacing legacy MAGIC and Client/Server). It supports FHIR R4 APIs (mandatory July 2026 under United States Core Data for Interoperability (USCDI) v3, has a web-native interface that runs on standard hardware, and integrates with most third-party point solutions through MEDITECH’s API surface. The downside: the API surface is narrower than Epic’s, and certain integrations require MEDITECH-certified middleware partners.
- Path 2: Epic Community Connect. A CAH joins a larger Epic instance hosted by a regional health system. Meaningful adoption among CAHs that affiliate with academic medical centers or large hospital systems. The strength: full Epic capability, deep integration ecosystem, regular upgrades. The cost: 5-7 figure annual hosting fees plus reduced operational autonomy. The CAH effectively runs on the host system’s Epic instance and inherits its workflows and upgrade timing.
- Path 3: Athena, eClinicalWorks, or migration to a cloud-native EHR. A smaller subset of CAHs run Athena or eClinicalWorks (typically ambulatory-heavy CAHs with limited inpatient volume). Migration to a cloud-native EHR is technically feasible but operationally disruptive, and most CAHs cannot fund the migration without significant grant capital.
Decision factors:
- Existing system age and vendor support: A CAH on legacy MEDITECH MAGIC or Client/Server faces an expensive upgrade-or-migrate decision. Expanse is the in-place upgrade path.
- Affiliation with a larger health system: If the CAH is part of a regional system that runs Epic, Community Connect is operationally simpler than maintaining standalone Expanse.
- Specialty mix: Heavy ambulatory CAHs may find Athena or eClinicalWorks workflows more native than MEDITECH’s inpatient-first design.
- RHTP funding eligibility: Several state RHTP plans include EHR modernization line items. A CAH considering migration should align timing to state procurement windows opening Q3 2026 through Q1 2027.
III. Revenue Cycle Management for a 25-Bed Hospital
Revenue Cycle Management is where margin gets captured at a CAH. Because cost-based Medicare reimbursement covers operating costs, the margin lever sits in commercial and Medicaid revenue plus denials reduction across all payers.
Where modern RCM moves the needle:
- Automated claims submission and scrubbing. Reduces denial rates by 30-50% compared to manual or partially automated workflows. For a CAH submitting 200 claims per week, this represents meaningful net revenue capture.
- Denials management workflow. Routes denied claims to appropriate staff with appeal templates and tracking. CAHs that implement structured denials workflows recover 60-80% of denied claims that would otherwise become write-offs.
- Patient financial services automation. Self-service patient billing portals, automated payment plans, propensity-to-pay scoring. CAH patient bases skew older and rural, which means traditional self-service adoption is lower than urban hospitals, but a 20-30% self-service rate is achievable and reduces collection overhead.
- Eligibility verification at registration. Real-time payer eligibility checks at the point of registration prevent downstream denials and improve patient communication about expected costs.
RCM vendor patterns for CAHs:
- Athena RCM (popular among Athena-EHR CAHs)
- Cerner RCM (less common at CAH scale)
- R1 RCM and similar managed RCM services (some CAHs outsource the entire function)
- Custom workflow integrations on top of MEDITECH or Epic Community Connect
Operating margin impact: A typical CAH that moves from legacy RCM to modern integrated RCM captures 2-3% net revenue improvement, primarily from denial reduction and faster cash collection. For a CAH with $30M annual net patient revenue, this translates to roughly $600K-$900K in additional annual margin. This is consequential for facilities operating with 1-3% margins.
For the deeper financial mechanics, see our Critical Access Hospital reimbursement and ROI guide.
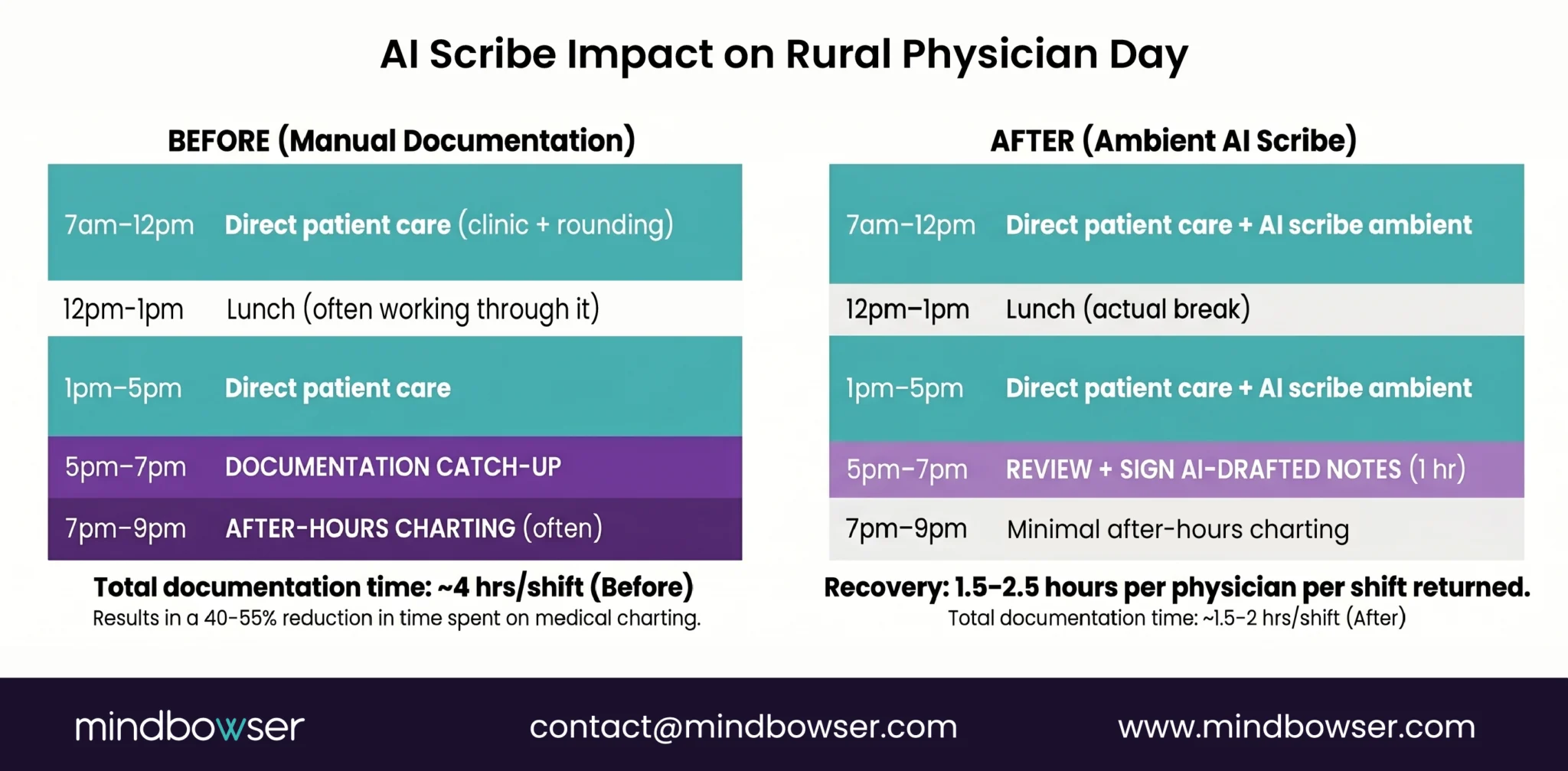
IV. Clinical Documentation: AI Scribes for Rural Clinical Staff
Clinical documentation AI is the technology category with the largest workforce impact at a CAH. The mechanism is simple: ambient AI scribes listen to physician-patient encounters, generate structured clinical notes, and integrate the output into the EHR. Physicians review and accept rather than dictate from scratch.
Documented impact (from KLAS pilots and our AI SummaryAssist deployments):
- 40-55% reduction in documentation time per encounter
- 1.5-2.5 hours per shift recovered per physician
- Reduced after-hours charting (the “pajama time” that drives physician burnout)
- Faster note completion improving claims submission speed
Why this matters for a CAH: A 25-bed rural hospital cannot easily recruit a second physician. Saving two hours per physician per day is the difference between staffing sustainability and burnout-driven turnover. The AI scribe is not just an efficiency tool. It is a workforce retention mechanism.
Vendor patterns:
- Suki: Strong physician adoption, broad EHR integration, ambient capture
- Abridge: Conversational AI focus, strong with academic medical centers, expanding to community settings
- Nuance DAX (Microsoft): Embedded in many Epic environments
- Mindbowser AI SummaryAssist: Custom deployments where vendor platforms do not fit specific clinical workflows or compliance requirements
Implementation considerations:
- EHR integration depth matters more than the AI itself. A scribe that produces excellent text but does not write to the EHR flowsheet adds cognitive overhead instead of removing it.
- Physician change management is the make-or-break factor. CAHs that succeed with AI scribes invest in 2-4 weeks of physician onboarding and feedback loops.
- Specialty-specific tuning: ambient AI trained on emergency medicine performs differently than AI tuned for primary care or hospital medicine.
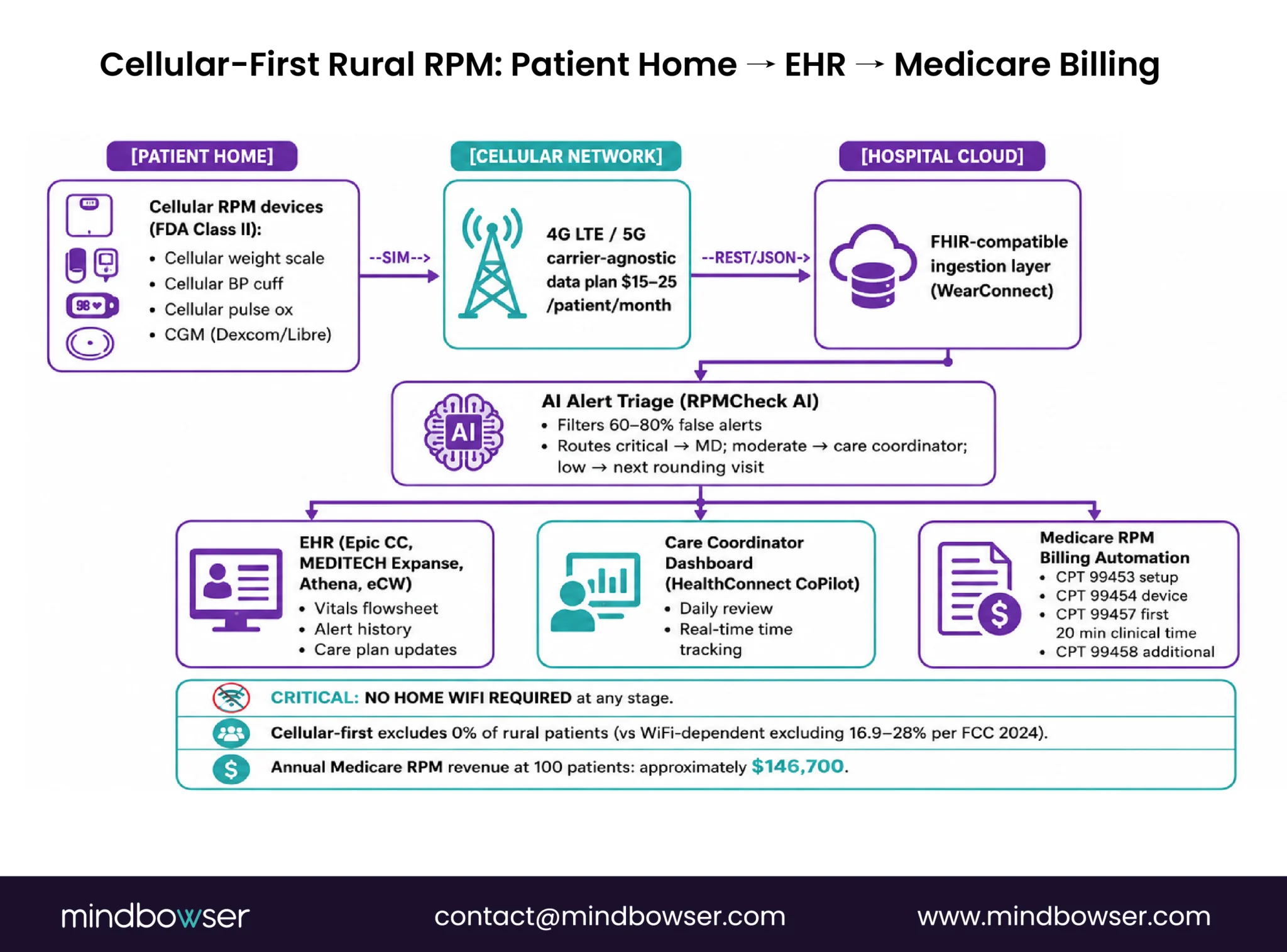
V. Remote Patient Monitoring: Cellular-First Architecture
Remote Patient Monitoring at a CAH is fundamentally different from RPM at an urban hospital. The architectural decisions all flow from the connectivity reality: Approximately 28 percent of rural Americans lack access to 100/20 Mbps broadband
The cellular-first architecture means:
- RPM devices must operate on cellular networks (4G LTE or 5G), not require home WiFi
- Cellular data plans are budgeted as a line item: cellular connectivity cost
- Device selection prioritizes manufacturers with strong cellular SKUs (BodiMetrics, iHealth Cellular, Tytocare, others)
- Patient onboarding must work for elderly patients with minimal tech experience: pre-configured devices, large buttons, voice-guided setup
Medicare RPM billing for CAHs:
CAHs can bill Medicare Current Procedural Terminology (CPT) RPM codes (99453, 99454, 99457, 99458) for chronic disease management. The codes capture revenue that cost-based reimbursement does not specifically cover. For a CAH enrolling 100 chronic disease patients in RPM, the annual revenue addition runs $80K-$150K depending on patient acuity mix and care management hours.
Architecture decision: device-agnostic ingestion layer.
Locking into a single device vendor creates supply chain risk and limits future device upgrades. WearConnect normalizes data from 300+ RPM devices into a single FHIR-compatible data stream. The abstraction layer means a CAH can change device vendors without rewriting the integration. The extra three weeks of upfront development saves six months of rework when device markets shift.
RPM use cases that work at CAH scale:
- Chronic congestive heart failure (CHF) monitoring with daily weight + symptom check-in
- Diabetes management with continuous glucose monitoring (CGM) for high-risk patients
- COPD with pulse oximetry and symptom tracking
- Post-discharge monitoring for high-readmission-risk patients
- Hypertension management with home BP monitoring
For the rural-specific RPM deployment model including 90-day launch plan, see RPM for Rural Hospitals: Architecture, Cost, and 90-Day Launch Plan.
Planning the right technology stack for your rural hospital?
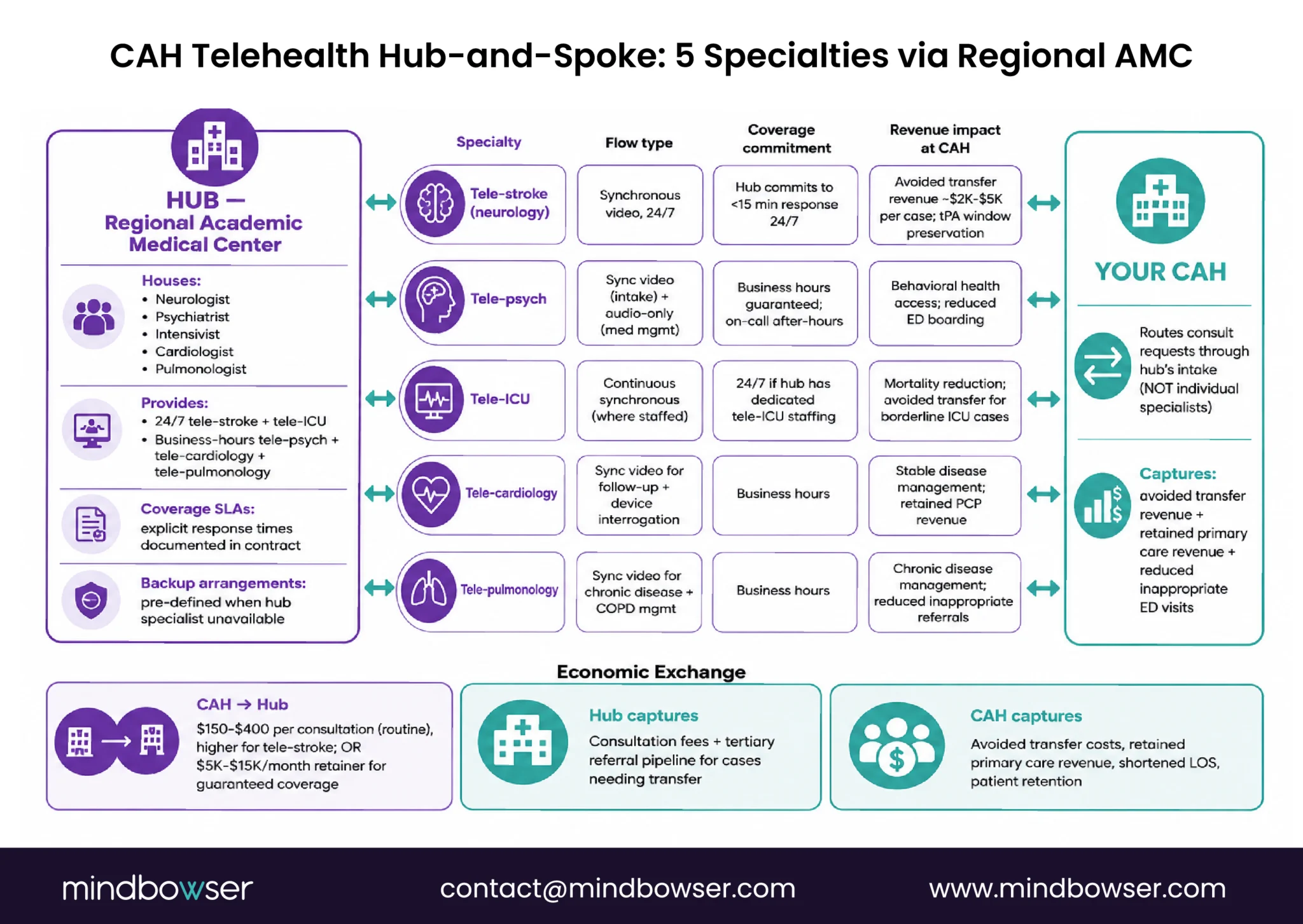
VI. Telehealth Hub Connection for Specialty Coverage
Telehealth at a CAH solves a specific economic problem: how to provide specialty care access without adding specialists to payroll. The answer is hub-and-spoke arrangements.
The model:
The CAH partners with a regional academic medical center, large hospital system, or specialty telehealth vendor (the “hub”). Specialty consultations (cardiology, neurology, behavioral health, pulmonology, infectious disease) happen via real-time video between the CAH bedside and the hub specialist. The CAH preserves primary care revenue and avoids the unsustainable economics of recruiting low-volume specialists to a 25-bed setting.
Common telehealth specialty patterns at CAHs:
- Tele-stroke: Neurology consultation within minutes of patient presentation, enabling tissue plasminogen activator (tPA) administration at the CAH rather than transfer
- Tele-psychiatry: Behavioral health consultation, often the only psych access available in the service area
- Tele-ICU: Continuous remote monitoring for higher-acuity inpatients, often through electronic ICU (eICU) programs operated by larger systems
- Tele-cardiology: Cardiology consultations, EKG interpretation, follow-up management
- Tele-pulmonology / tele-infectious disease: Specialty consultation for complex cases that would otherwise require transfer
Technical requirements:
- Sub-500ms latency video for clinical assessment
- Bandwidth-adaptive streaming (graceful degradation for limited rural connectivity)
- Peripheral device integration (digital stethoscope, otoscope, dermatoscope feeds piped into the video session)
- EHR integration so the consult note flows into the patient’s chart
- Documentation workflows that satisfy CMS billing requirements for telehealth consults
Vendor and partner patterns:
- Academic medical center hub-and-spoke contracts (most common for CAHs in states with strong AMC presence)
- Telepsych vendors (Iris Telehealth, others) for behavioral health-only programs
- Tele-stroke vendors (TeleSpecialists, others) for stroke-only programs
- Custom telehealth platforms for CAHs that need specific specialty mix not covered by standard vendors
For the rural-specific telehealth deployment model including low-bandwidth solutions, see How Rural Hospitals Can Build Telehealth Without Hiring a Tech Team.
VII. Cybersecurity and HIPAA Compliance Without an Internal Security Team
Cybersecurity is the technology category most likely to be under-invested at a CAH and most likely to cause a catastrophic incident when neglected. The HHS 405(d) Program consistently rank small rural hospitals as high-risk targets for ransomware.
The CAH security reality:
Most CAHs do not have a Chief Information Security Officer. The IT director handles security alongside everything else. Internal security monitoring is rarely 24/7. Vulnerability scanning is often quarterly at best. Incident response plans, when they exist, are not exercised regularly.
This is fixable through managed security operations:
- Managed Detection and Response (MDR): 24/7 monitoring outsourced to a security operations center with healthcare expertise. Detects threats in minutes rather than days.
- Vulnerability management: Continuous scanning of network and endpoint vulnerabilities with prioritized remediation guidance.
- Endpoint detection and response (EDR): Modern endpoint protection that goes beyond traditional antivirus.
- Identity and access management (IAM): Single sign-on, multi-factor authentication, privileged access management.
- Backup and disaster recovery: Immutable backups with tested recovery procedures. The defense against ransomware that does not depend on prevention working.
- Security awareness training: Phishing simulation, ongoing education for clinical and administrative staff.
HIPAA compliance posture:
- HIPAA Privacy Rule documentation and policies
- HIPAA Security Rule technical, administrative, and physical safeguards
- Business Associate Agreement (BAA) management with all third-party vendors handling PHI
- Annual risk assessment and remediation
- Breach notification procedures and tested communication plans
- 21st Century Cures Act information blocking compliance
State Health-ISAC participation: Several states operate health-information-sharing-and-analysis centers that share threat intelligence and incident data among healthcare organizations. CAH participation is typically free and provides early warning on active threats.
PHISecure is our managed compliance platform that handles HIPAA posture and security operations for healthcare organizations without internal security teams. Implementation runs 4-8 weeks depending on scope.
VIII. Integration Layer: How These Components Talk to Each Other
The integration layer is the technology component that determines whether the other six function as a coherent system or as a collection of unrelated tools that the IT director maintains separately.
Why this matters now:
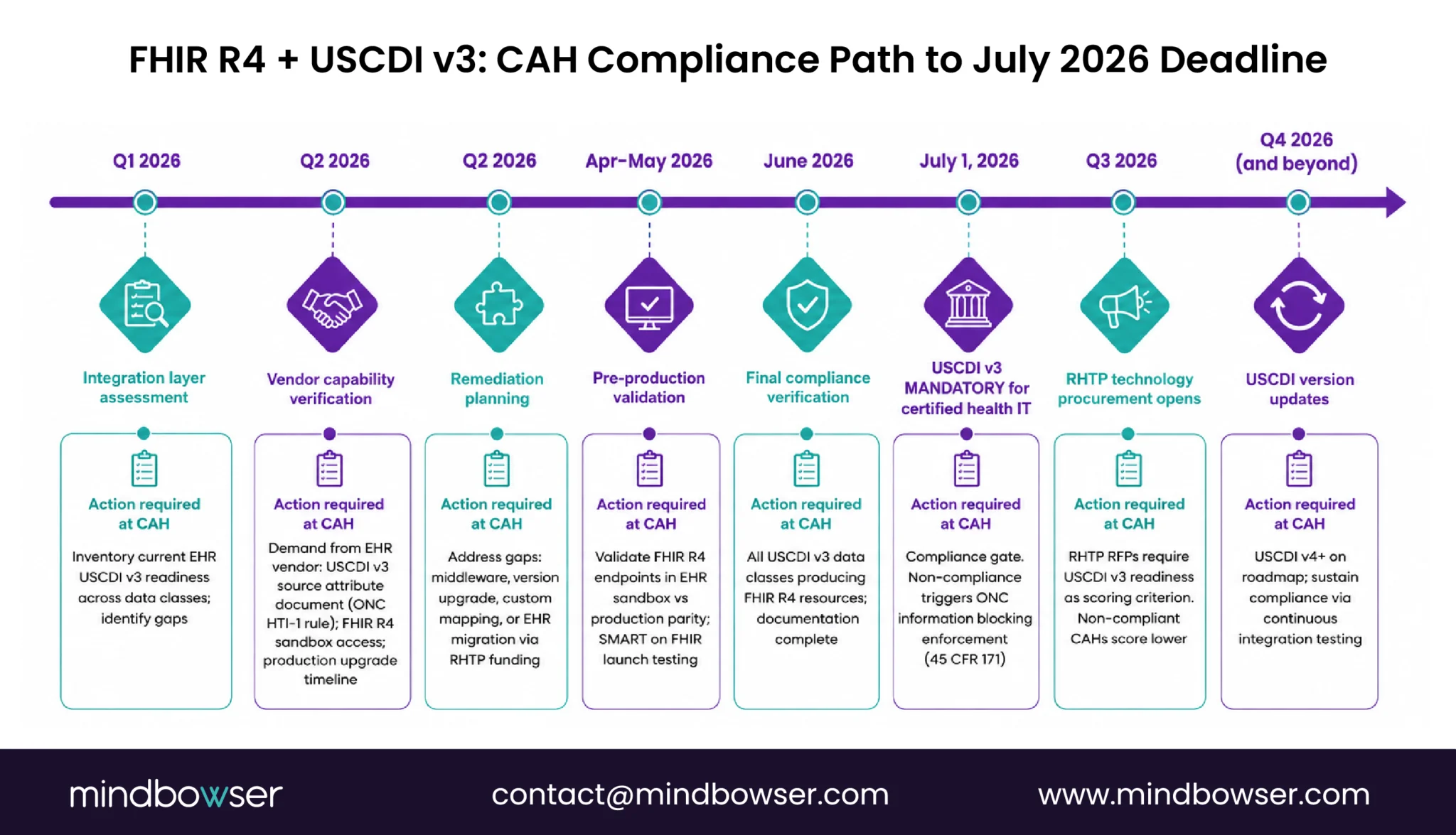
United States Core Data for Interoperability (USCDI) v3 compliance becomes mandatory July 2026 for certified health IT. This means EHR vendors must expose Fast Healthcare Interoperability Resources (FHIR) R4 APIs for the United States Core Data for Interoperability v3 dataset. For CAHs, this is a forcing function: the integration layer needs to be FHIR-capable by mid-2026 even if the CAH is not actively pursuing new integrations.
What the integration layer does:
- API gateway: Single point of entry for external systems that need to interact with CAH data
- Health Level 7 (HL7 v2) messaging: Legacy hospital messaging standard still required for many integrations (lab results, Admit-Discharge-Transfer (ADT) feeds, orders)
- FHIR R4 API exposure: Modern RESTful API for clinical data exchange, mandatory under USCDI v3
- Event routing: Messaging queues that route clinical events (admissions, discharges, transfers, results) to subscribed systems
- Identity matching: Resolving patient identifiers across systems (the enterprise Master Patient Index (eMPI) problem)
- Data quality and normalization: Ensuring data exchanged across systems is consistent, complete, and clinically usable
Vendor patterns:
- Mirth Connect (open source): Long-standing healthcare integration engine, technically capable but requires internal expertise to operate
- Redox: SaaS healthcare API platform, popular with digital health vendors integrating into hospital systems
- Rhapsody (Lyniate): Commercial integration engine, common at larger systems, used at CAHs through MEDITECH or Epic partnerships
- HealthConnect CoPilot: Mindbowser’s care coordination and integration platform, FHIR-native, designed for environments where internal integration expertise is limited
The CAH-specific design constraint: Whatever integration layer the CAH chooses must be operationally sustainable for a 1-2 person IT team. Mirth Connect is technically powerful but operationally heavy. Managed integration platforms reduce operational burden but increase recurring costs.
For deeper EHR integration patterns specific to rural hospitals running MEDITECH Expanse, Epic Community Connect, and state HIE connectivity, see Rural Hospital EHR Integration.
IX. What This Costs and Where RHTP Funding Fits
Honest cost ranges for the seven-component CAH technology stack, based on small-hospital deployments and current vendor pricing.
| Component | Annual cost range | Capital vs operating | Typical funding source |
|---|---|---|---|
| EHR (MEDITECH Expanse / Epic CC / Athena) | $200K-$600K | Mostly operating, periodic capital for upgrades | Operating budget; RHTP for migration |
| RCM (managed services or platform) | $80K-$200K | Operating | Operating budget |
| Clinical AI scribe | $60K-$180K (for 5-15 physicians) | Operating | Operating; RHTP for initial deployment |
| RPM platform + devices | $50K-$150K platform + $50-150 per patient per month | Capital + operating | Medicare RPM billing offsets cost; RHTP for infrastructure |
| Telehealth hub-and-spoke | $30K-$120K (vendor or partnership fees) | Operating | Operating; some grant funding for telepsych |
| Cybersecurity managed services | $40K-$120K | Operating | Operating; RHTP eligible |
| Integration layer | $40K-$150K | Operating + initial implementation capital | Operating; RHTP for FHIR onboarding |
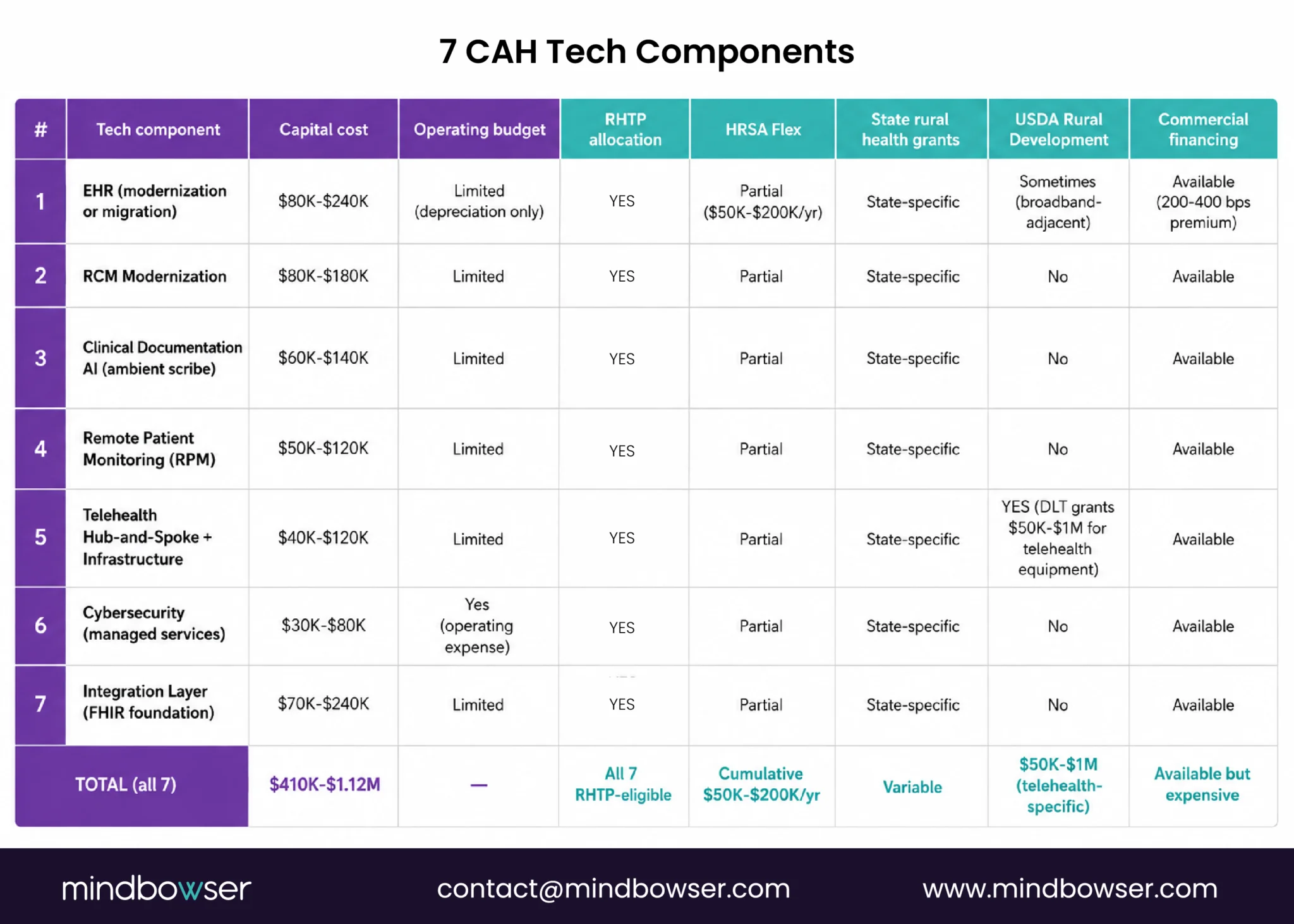
Total annual technology stack: $500K-$1.5M for a 25-bed CAH, depending on scope and vendor selections.
Capital investments not in the table:
- EHR migration (one-time): $500K-$3M depending on source/destination systems
- Network and infrastructure modernization: $100K-$500K
- Facility-specific technology buildout (radiology, lab): variable
Where RHTP changes the math:
The Rural Health Transformation Program is the first federal funding source designed to address CAH capital constraints in technology. State RHTP plans include line items specifically for CAH technology modernization. The procurement window opens Q3 2026 through Q1 2027, with implementation contracts awarded through Q2 2027.
For a CAH planning technology investment in 2026-2027, the funding sequence to evaluate:
- State RHTP allocation: Often the largest available capital source for technology in 2026-2030
- HRSA Flex Program grants: Operational support and quality improvement
- State rural health office grants: State-specific funding sources, often complementary to RHTP
- USDA Rural Development: Infrastructure grants, often facility-focused
- Commercial financing: For investments not eligible under above sources
The full RHTP allocation framework, statutory elements, and state-by-state procurement timeline is in our Rural Health Transformation Program guide.
X. How Mindbowser Approaches CAH Technology Modernization
Mindbowser builds custom healthcare technology for small and rural hospitals whose constraints exceed what off-the-shelf platforms accommodate. Our work with small-hospital deployments has produced an accelerator stack that maps directly to the seven CAH technology components above.
- HealthConnect CoPilot provides care coordination and integration layer infrastructure. FHIR R4 native, designed for environments where the IT team is two people and the integration burden is real. Handles MEDITECH Expanse, Epic Community Connect, Athena, and eClinicalWorks. Operationally sustainable for a CAH IT team.
- WearConnect delivers device-agnostic RPM with cellular-first architecture. Supports 14 RPM device manufacturers through a single FHIR-compatible data stream. The abstraction layer prevents vendor lock-in and accommodates rural connectivity reality.
- AI SummaryAssist reduces clinical documentation time by 40-55% per encounter. Embedded in clinical workflow rather than adjacent to it. The integration depth that determines whether AI scribes save physician time.
- PHISecure handles HIPAA compliance posture and managed security operations for hospitals without internal security teams. Covers MDR, vulnerability management, EDR, IAM, and HIPAA documentation.
Engagement model:
- 12-16 week MVP builds rather than 18-24 month waterfall projects
- Phased scaling with measurable milestones
- Funding-aware project structuring that aligns to state RHTP procurement windows where applicable
- Operational handoff designed for 1-2 person IT teams to maintain
Download the 25-Bed Rural Hospital Technology Stack Reference Map
Rural Hospital Technology Will Be Defined by Simplicity, Not Size
The technology stack for a 25-bed rural hospital does not fail because the tools are unavailable. It fails when systems are built for large enterprise hospitals instead of the operational reality of a 1-2 person IT team, limited capital, and rural connectivity gaps. The hospitals that succeed over the next five years will focus on practical infrastructure: interoperable EHRs, cellular-first RPM, AI documentation support, telehealth specialty access, reliable cybersecurity, and integration layers that reduce operational burden instead of adding to it. RHTP funding creates a rare opportunity to modernize these systems at scale, but the procurement window is finite. Rural hospitals that align technology decisions with workflow simplicity, reimbursement realities, and long-term sustainability will be the ones that strengthen care delivery without overwhelming already stretched clinical teams.
A 25-bed Critical Access Hospital needs seven technology components: an EHR (typically MEDITECH Expanse, Epic Community Connect, or Athena), revenue cycle management, clinical documentation AI, remote patient monitoring with cellular-first connectivity, telehealth specialty access through hub-and-spoke arrangements, managed cybersecurity and HIPAA compliance services, and an integration layer (FHIR R4 native) connecting these components. Total annual technology stack cost runs $500K-$1.5M depending on scope.
The most common EHRs at CAHs are MEDITECH Expanse (the largest market share), Epic Community Connect (CAHs hosted by larger Epic-running health systems), Athena Clinicals (CAHs with heavy ambulatory mix), and eClinicalWorks. Smaller numbers of CAHs run Cerner Community Works (now Oracle Health), CPSI, or other vendors. The choice is shaped by existing system age, affiliation with larger health systems, specialty mix, and RHTP funding eligibility for migration.
Annual technology operating cost for a 25-bed CAH runs $500K-$1.5M depending on scope, with capital investments (EHR migration, infrastructure) layered separately. The cost concentration is in the EHR ($200K-$600K annually) and clinical AI ($60K-$180K). RHTP funding flowing in 2026-2030 changes the capital calculus significantly, with state RHTP plans including CAH technology modernization line items.
Yes, through Epic Community Connect. A CAH joins a larger Epic instance hosted by a regional health system or academic medical center. This carries $250K-$2M annual hosting fees but provides full Epic capability with reduced operational autonomy. The CAH inherits the host system’s workflows and upgrade timing. Epic Community Connect is one of three viable EHR paths for CAHs in 2026, alongside MEDITECH Expanse and Athena/eClinicalWorks.
Cellular-enabled RPM devices that operate on 4G LTE or 5G networks without requiring home WiFi. Several manufacturers (BodiMetrics, iHealth Cellular, Tytocare, others) produce cellular SKUs for chronic disease monitoring. Budget $15-25 per patient per month for cellular data plans. The architectural recommendation: deploy a device-agnostic ingestion layer (such as WearConnect) so device selection can adapt as cellular RPM markets evolve.
Yes. The Rural Health Transformation Program is the first federal funding source designed to address CAH capital constraints in technology. State RHTP plans include CAH-specific technology modernization line items across statutory elements C (consumer-facing technology), D (training and TA), F (provider technology including EHR and HIE), and H (innovation in delivery). The procurement window opens Q3 2026 through Q1 2027. CAHs should engage their state RHTP program during the Q1-Q3 2026 stakeholder process to ensure their needs are reflected in RFPs.
Through managed services and operationally sustainable platform choices. The pattern that works: managed EHR hosting (MEDITECH or Epic Community Connect), managed RCM (third-party or vendor-operated), managed cybersecurity (MDR + EDR), and integration platforms designed for low-touch operations (HealthConnect CoPilot, Redox, or similar). The IT director becomes a vendor manager and clinical workflow advocate rather than an infrastructure operator. This is operationally feasible for a 1-2 person IT team if the platform choices are made with this constraint in mind from the start. This page references the following primary federal sources. All citations link directly to the official Federal Register, CFR, or agency record.
