



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
A rural hospital can launch a functional Hospital-at-Home program in 90 days if the CMS waiver application, clinical protocols, staffing model, technology platform, and patient selection criteria are sequenced correctly. The 419 CMS-approved H@H programs include several CAH and rural participants, demonstrating that rural-specific H@H launch is operationally feasible. RHTP funding flowing Q3 2026 through Q1 2027 changes the capital math that previously blocked rural H@H deployment. This guide covers the six-step launch sequence, the common failure modes that trip rural programs in months two and three, and how to structure the launch to qualify for RHTP state procurement.
A rural hospital CEO calls with the same question most rural H@H inquiries start with: “can we actually do this?”
The answer is yes, conditionally. Rural hospitals that launch Hospital-at-Home without sequencing the clinical, staffing, technology, and regulatory preparation fail in months two and three on clinical risk events, staffing burnout, or CMS compliance gaps. Rural hospitals that follow the sequencing launch in 90 days, stabilize operations in the first 30 days post-launch, and scale from 3-5 initial patients to 15-30 concurrent patients within 12 months.
Three conditions shape rural H@H in 2026 in ways that did not exist three years ago. The CMS Acute Hospital Care at Home waiver was extended through September 30, 2030 by Section 6210 of the Consolidated Appropriations Act of 2026 (Public Law 119-75), signed into law in February 2026. That five-year runway gives rural hospitals the time horizon to justify the operational investment. The Rural Health Transformation Program flowing to all 50 states in 2026 makes the capital math work for the first time, with state procurement windows opening Q3 2026 through Q1 2027. And Commonwealth Fund research on hospital-at-home programs has concluded that the model improves outcomes and lowers costs by 30 percent or more compared to traditional inpatient care , though MedPAC’s June 2024 Report to Congress (Chapter 6) cautioned that even among the 328 hospitals approved at the time of that report, many had not implemented programs, and patient acceptance remained a challenge. Rural H@H is feasible, and the financial case has strengthened, but the operational execution gap between approval and patient-serving capacity is real.
This guide covers the six-step 90-day launch sequence, the operational details rural hospital leaders need to make go-or-hold decisions, and the RHTP funding pathway that makes the economics work.
For the comprehensive H@H platform architecture (all seven technology components, build-vs-buy analysis, implementation timeline).
Can a Rural Hospital Actually Launch Hospital-at-Home?
Yes, if the facility meets four prerequisites. The 419 hospitals currently operating H@H programs under the CMS AHCAH waiver include several CAH and rural participants, which establishes feasibility. The prerequisites filter which rural hospitals can realistically launch versus which should wait.
Prerequisite 1: Active CMS hospital certification including CAH status.
Critical Access Hospitals are explicitly eligible to participate in the AHCAH waiver. Rural Prospective Payment System (PPS) hospitals are also eligible. Rural Emergency Hospitals (REH) have a different pathway that excludes inpatient services, so REHs cannot launch traditional H@H under the current waiver.
Prerequisite 2: Patient population with minimum sustainable volume.
A rural H@H program needs 15-25 H@H-eligible admissions per month to sustain fixed operating costs. Below that volume, per-patient costs exceed the reimbursement captured, and the program runs at a loss that operating margin cannot absorb. Rural hospitals with sub-15 monthly eligible admissions should either partner with a neighboring hospital to share H@H infrastructure or defer launch.
Prerequisite 3: Clinical staff capacity or contracted partnership.
H@H requires physician or APP rounding 1-2 times daily (via video or in-person), plus 1-2 daily home nursing visits per active patient, plus 24/7 clinical command center coverage. Rural hospitals with fewer than two physicians or APPs need either expanded clinical staffing (often infeasible in rural workforce markets) or contracted partnership with a neighboring health system for rounding coverage. Home nursing visits can be provided by employed RNs or through contracted home health agency partnerships.
Prerequisite 4: Technology platform capability.
Technology is where the capital gap has historically killed rural H@H programs. The six-component technology stack (RPM, video rounding, AI alert filtering, EHR integration, patient-facing app, care coordination dashboard, logistics dispatch) runs $300K-$700K upfront plus $9K-$23K monthly operating. Rural hospitals cannot fund this from cost-based Medicare operating margin. RHTP funding closes that gap.
Rural-specific considerations across all four prerequisites: the 23 percent broadband gap in rural patient populations is handled via cellular-first RPM architecture; workforce constraints are handled via AI clinical documentation and telehealth specialty consultation; 45-90 minute transportation distances are handled via home nursing partnerships and community paramedicine contracts.
The rural hospitals that clear these four prerequisites are candidates for 90-day launch. The ones that do not should address the gaps before attempting launch rather than attempting launch and accepting predictable failure.
What the 90-Day Launch Timeline Looks Like at a Rural Hospital
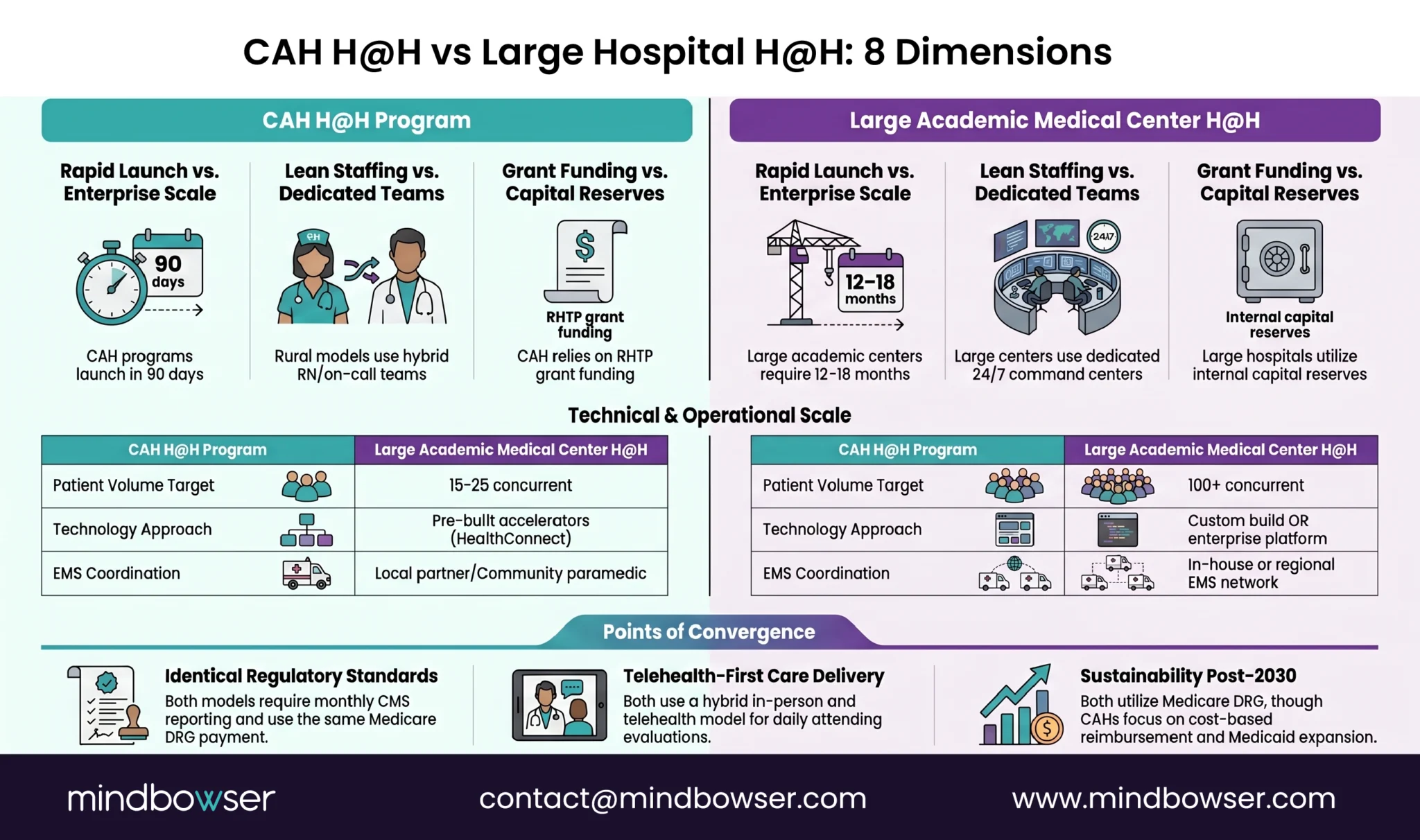
The 90-day launch sequence compresses the timeline large academic medical centers typically run at 12-18 months. The compression comes from two sources: rural facilities use pre-built accelerators or RHTP-funded platforms rather than building proprietary systems from scratch, and rural facilities launch at smaller initial patient volumes that reduce the operational complexity of go-live.
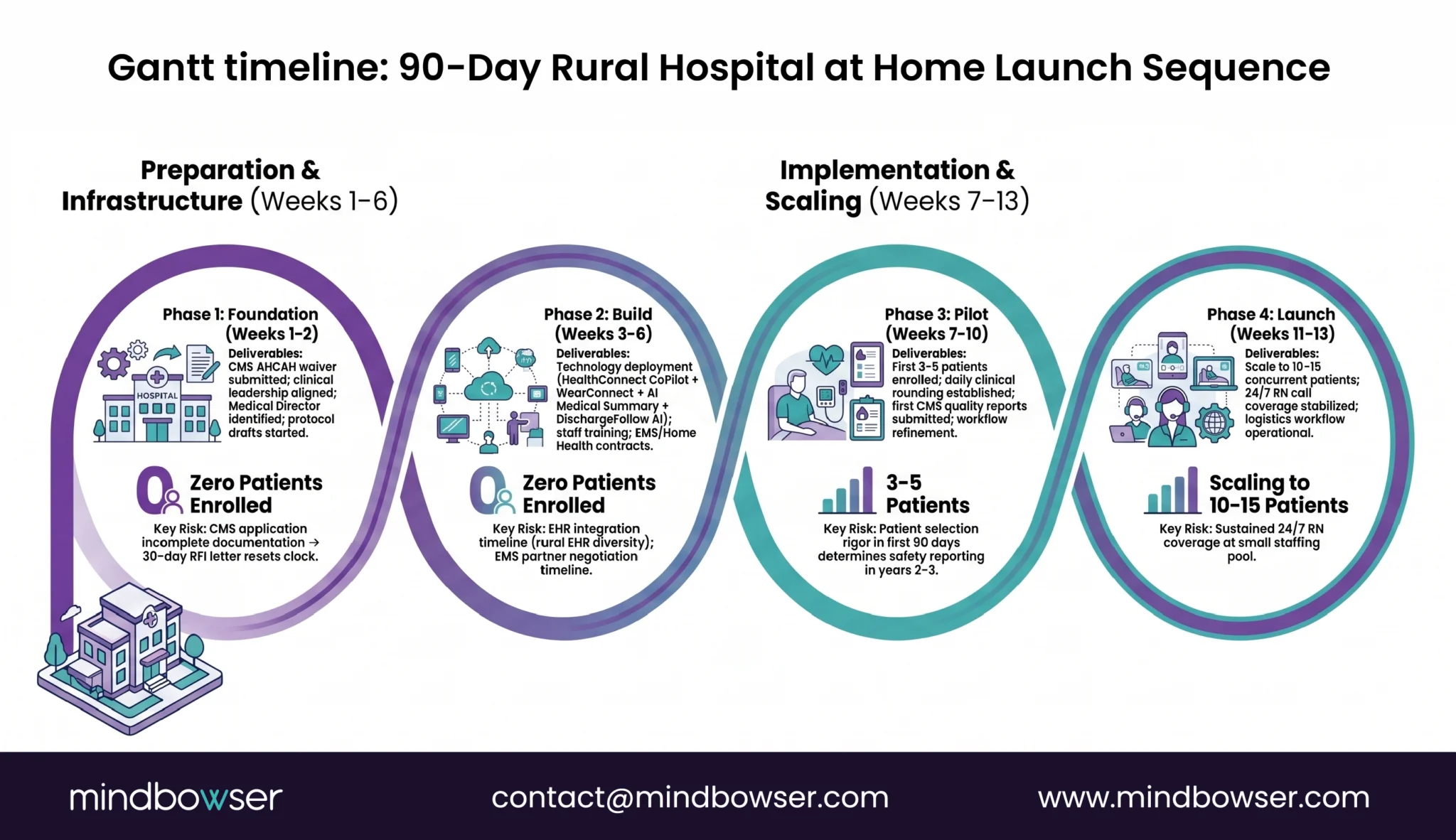
| Phase | Weeks | Deliverables | Key Risk |
|---|---|---|---|
| Foundation | 1-2 | CMS waiver application submission, clinical leadership alignment, initial staffing model decision, technology platform contracting | Incomplete waiver application returns from CMS; extends timeline 2-4 weeks |
| Build | 3-6 | Technology platform deployment, clinical protocol documentation, initial staff training, logistics partner contracts (home nursing, EMS, medication delivery) | Technology integration surprises on rural EHR systems (MEDITECH, Athena); extends build phase |
| Pilot | 7-10 | Pilot with 3-5 patients, workflow refinement, home assessment process validation, alert threshold calibration | Clinician friction surfaces in pilot; needs rapid iteration to address |
| Launch | 11-13 | Go-live expansion to 10-15 concurrent patients, 24/7 clinical coverage operationalization, billing and documentation validation | Alert fatigue and home nursing visit delays surface in first scaling phase |
Mass General Brigham’s Home Hospital program and Mount Sinai’s HaH took 12-18 months to reach comparable operational maturity. The reasons: both built proprietary technology platforms from scratch, both operated in large-scale urban settings with higher clinical complexity, and both launched before pre-built RPM and integration platforms were commercially available.
Rural hospitals compressing to 90 days typically use pre-built platforms (or RHTP-funded platforms that share infrastructure across multiple state facilities), smaller initial patient panels, and narrower initial diagnosis lists. The 90-day timeline is not aspirational. It is the observed pattern across the rural H@H launches we have scoped.
Step 1: CMS Waiver Application and Regulatory Preparation
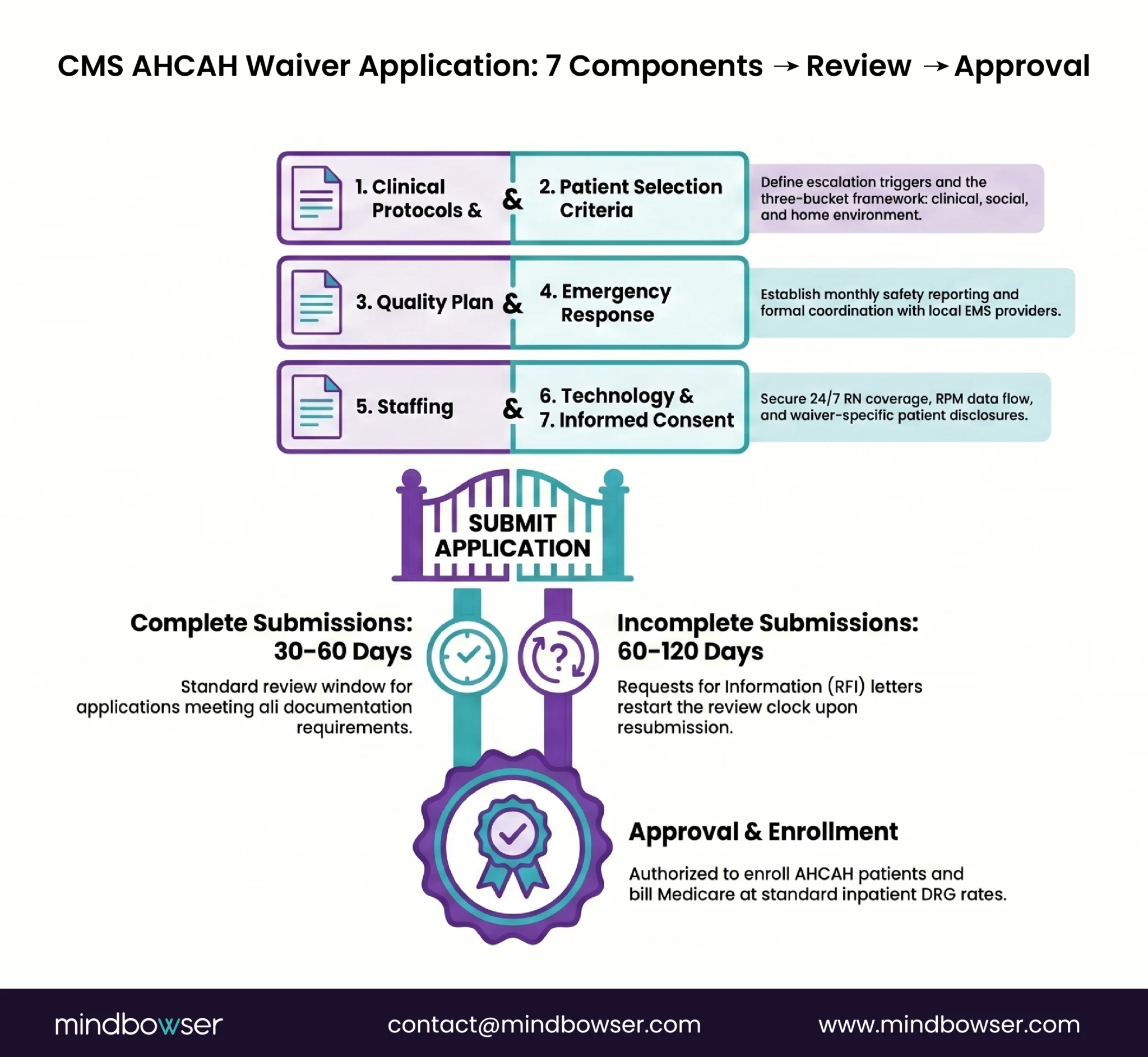
The CMS Acute Hospital Care at Home waiver application is the gating regulatory step. CMS review typically takes 4-8 weeks after submission. Applications returned for clarification extend the timeline by 2-4 weeks.
Required application components:
- Clinical protocols covering patient admission criteria, monitoring standards, rounding frequency, emergency response pathways, and discharge criteria
- Patient selection criteria specifying which diagnoses the program will accept and what clinical stability thresholds apply
- Quality measurement plan covering 30-day readmission rates, patient safety events, mortality, and patient experience measurement
- Emergency response plan specifying 911 coordination, clinical team notification, and transfer protocols to brick-and-mortar facility
- Staffing plan documenting physician, APP, and nursing coverage
- Technology platform documentation covering monitoring capability, communication infrastructure, and EHR integration
- Informed consent documentation specific to H@H admission
State-level requirements (vary by state):
- State hospital licensure provisions for home-delivered acute care
- Scope-of-practice rules for APPs managing H@H patients independently
- State Medicaid coordination for dual-eligible patients
- State emergency response coordination requirements
CAH-specific considerations:
Critical Access Hospitals are explicitly eligible for AHCAH waiver participation. Necessary Provider status does not affect waiver eligibility. CAHs participate in AHCAH while maintaining cost-based Medicare reimbursement for H@H services, which is a meaningful financial advantage relative to PPS hospitals.
Common waiver application failures:
- Incomplete emergency response plans that do not document specific transfer timeframes
- Patient selection protocols that are too broad (CMS prefers narrower initial scope)
- Missing or underdeveloped quality measurement infrastructure
- Staffing plans that do not clearly address 24/7 coverage
For the regulatory depth including specific waiver language and the complete Conditions of Participation.
Step 2: Clinical Protocols and Staffing Model for a Rural H@H Program
Clinical protocol documentation is the largest regulatory and operational workstream in the launch sequence. Rural H@H programs need documented protocols in seven categories before accepting first patient.
Clinical protocol categories:
- Patient admission criteria: Specific diagnosis list, clinical stability thresholds, home environment requirements, consent process
- Continuous monitoring protocols: Vital sign measurement frequency, alert thresholds, response timeframes
- Rounding protocols: Physician or APP rounding frequency, video vs in-person requirements, documentation standards
- Escalation pathways: Alert severity classification, clinical team notification, transfer thresholds
- Medication management: Home medication administration, controlled substance handling, pharmacy coordination
- Emergency response: 911 coordination, clinical team notification, transfer logistics
- Discharge criteria: Clinical stability requirements, transition to outpatient follow-up, care plan continuity
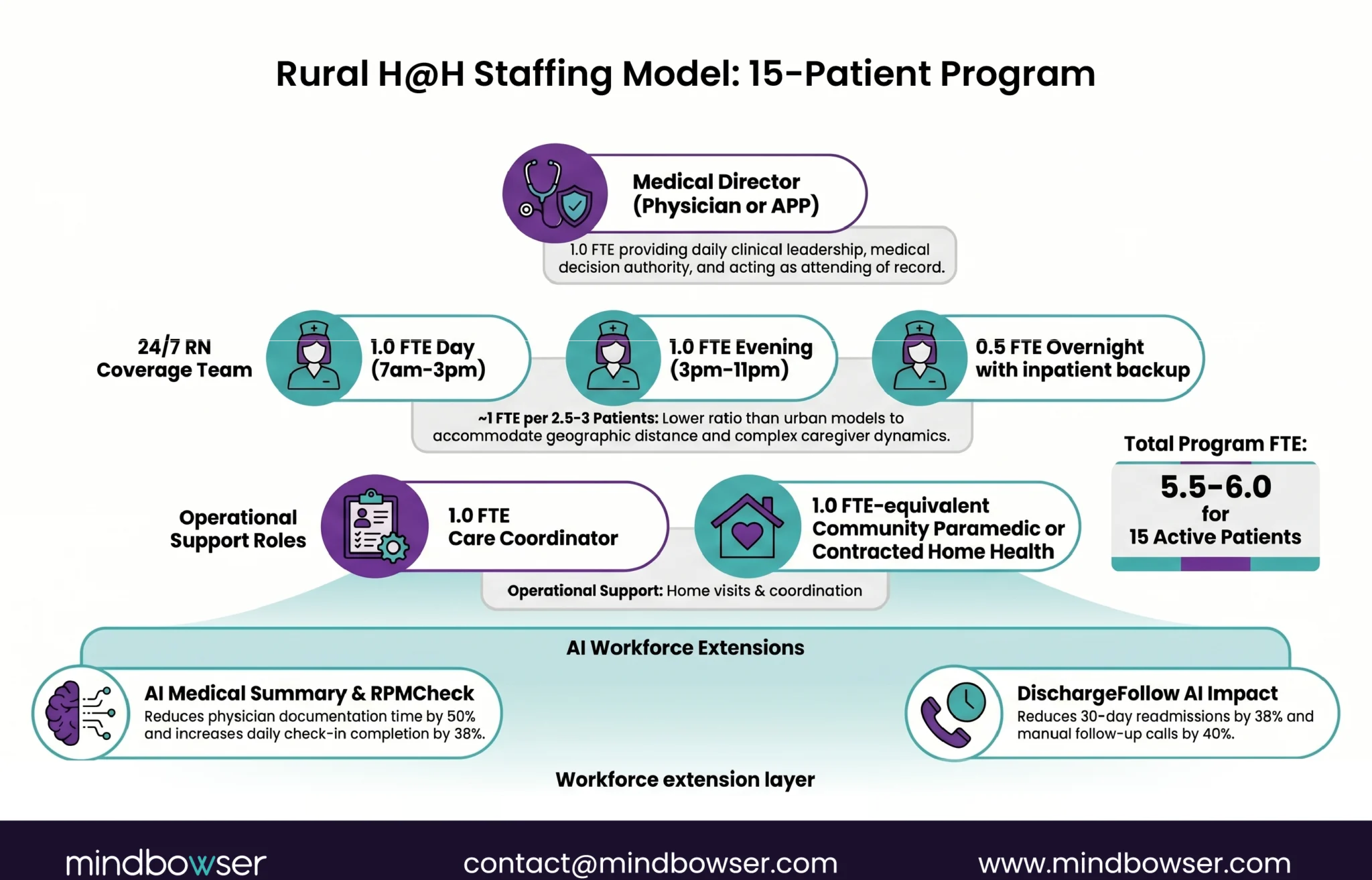
Staffing model for a 15-patient rural H@H program:
- 1 physician or APP serving as medical director, rounding 2x daily via video, available for escalation calls
- 2-3 RNs covering home visits and command center rotation, 24/7 coverage across three shifts
- 1 care coordinator managing patient scheduling, logistics, and family communication
- 1 community paramedic or contracted home health nurse for emergency response and complex home visits
- Administrative support (shared with facility) for billing, documentation review, quality measurement
How rural workforce constraints affect the model:
Rural workforce shortages make traditional staffing expansion infeasible at most facilities. Three operational mitigations extend rural workforce capacity:
- AI clinical documentation (ambient scribe tools) reduces physician documentation time by 40-55 percent per encounter, allowing one physician to sustain 15-20 H@H patient panels alongside other clinical duties
- Telehealth specialty consultation eliminates the need to recruit specialists for low-volume rural H@H scenarios; cardiology, infectious disease, and behavioral health consults happen via regional academic medical center partnerships
- Community paramedicine contracts fill emergency response capability without requiring the hospital to expand employed EMS workforce
Several RHTP state plans explicitly fund community paramedicine as a rural H@H enabler, addressing the workforce and capital challenge together.
State scope-of-practice rules matter here. States with full-practice APPs (Massachusetts, most Northeast and Midwest states, Arizona, Utah, and others) allow APPs to independently manage H@H patient panels. States with restricted APP practice authority require physician supervision at rates that may not be operationally feasible at small rural facilities.
Links to How AI Replaces 3 FTEs in Rural Care Management Teams for the clinical documentation workforce expansion mechanics.
Step 3: Technology Platform Selection Under Rural Constraints
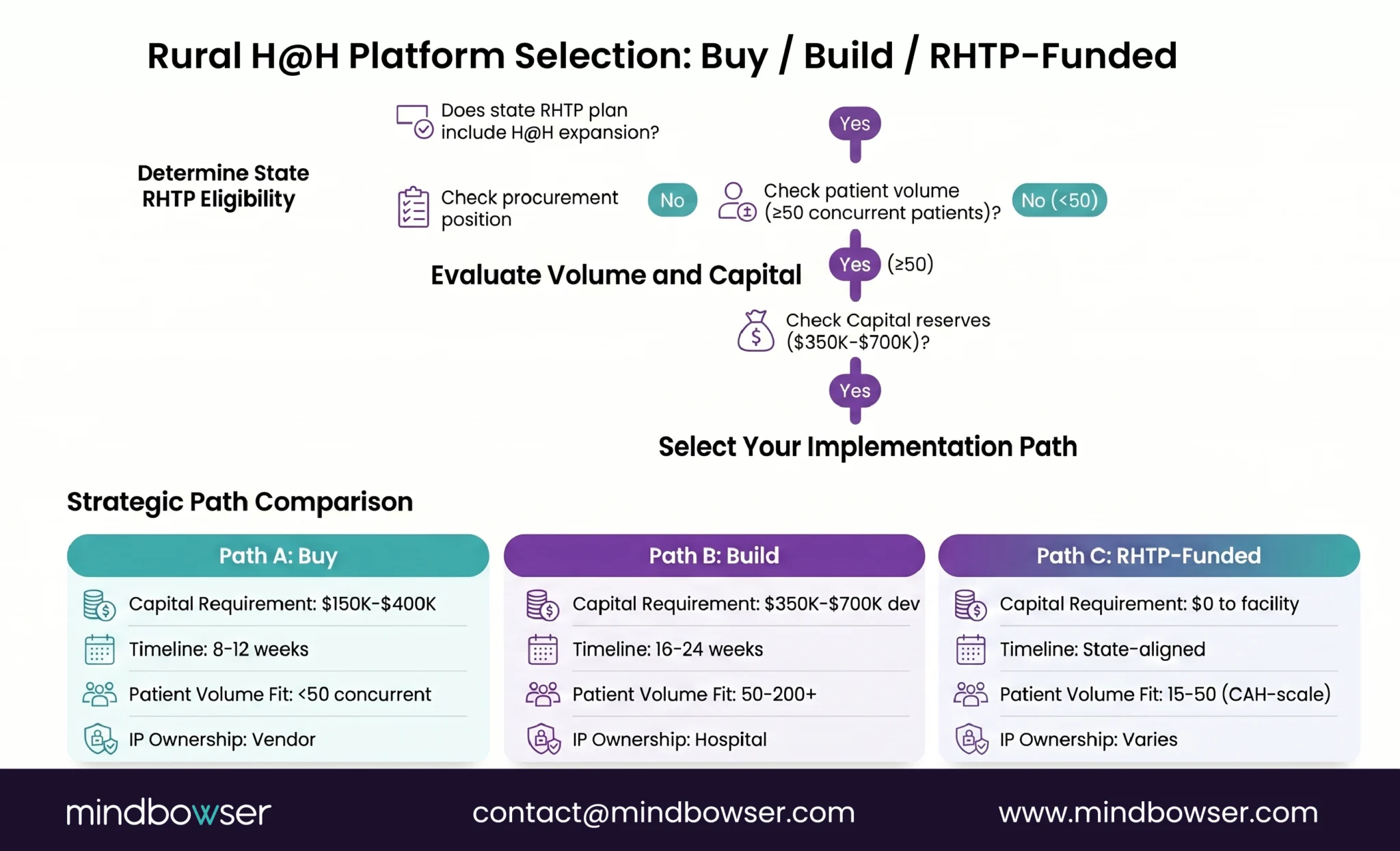
Three paths exist for rural H@H technology platforms. Each path fits different facility circumstances and RHTP funding positions.
Path 1: Buy a vendor platform:
Fastest path to launch (8-12 weeks technology deployment). Lowest upfront capital ($150K-$400K licensing + implementation). Operational simplicity (vendor manages infrastructure). Constraints: per-patient-per-month fees that scale linearly with patient volume ($75-150 per patient per month), limited customization, vendor lock-in on data and workflows, no IP ownership.
Best fit: Facilities launching with <30 monthly patient volume, tight timeline constraints, and no RHTP state procurement access.
Path 2: Custom build:
Longest timeline (16-24 weeks). Highest upfront capital ($350K-$700K development). Full IP ownership and customization. Lower ongoing operating cost ($5K-$15K per month infrastructure + maintenance) that does not scale with patient volume. Requires engineering partner or internal development capability.
Best fit: Facilities planning 100+ monthly patient volume, strategic positioning as a regional H@H center, or RHTP-funded builds where state procurement covers the capital cost.
Path 3: RHTP-funded shared platform:
Facility participates in state-level H@H platform deployment funded by RHTP procurement. State or state eHealth organization administers the platform. Participating facilities access capability without bearing full capital cost. Timeline depends on state procurement schedule (Q3 2026 through Q1 2027 for most states).
Best fit: Facilities in states with H@H as named RHTP activity (Massachusetts Initiative I Activity 7 and similar in other state plans), facilities without capital to fund independent deployment, facilities willing to accept shared platform constraints in exchange for access.
Rural-specific technology requirements across all three paths:
- Cellular-first RPM: FCC 2024 Section 706 data shows 16.9 percent of rural lacks 25/3 Mbps and 28 percent lacks 100/20 Mbps, requiring cellular-enabled devices rather than WiFi-dependent equipment
- Low-bandwidth video rounding: Bandwidth-adaptive streaming that maintains clinical quality on rural connectivity
- Operationally simple dashboards: 1-2 person rural IT team cannot maintain complex enterprise platforms
- Managed cloud infrastructure: HIPAA-compliant hosting without in-house DevOps capability
- EHR integration for rural systems: MEDITECH Expanse, Epic Community Connect, Athena, eClinicalWorks depending on facility
- FHIR R4 API support: USCDI v3 mandate takes effect July 2026
For the comprehensive seven-component platform architecture, see Hospital at Home: The Complete Technology Platform Guide. For the broader rural hospital technology stack that integrates with H@H, see Technology Stack for a 25-Bed Rural Hospital.
Mindbowser accelerators that map to H@H technology components: HealthConnect CoPilot for care coordination and EHR integration, WearConnect for cellular-first RPM across 14 device manufacturers.
Want to explore Hospital-at-Home for your rural facility?
Step 4: Patient Selection Criteria and Enrollment Workflow
Patient selection discipline is the operational control that prevents most rural H@H programs from clinical events that could shut them down. Enrolling a patient who should remain inpatient produces the clinical risk event that makes CMS notice, makes clinical staff lose confidence, and makes administrators question the program.
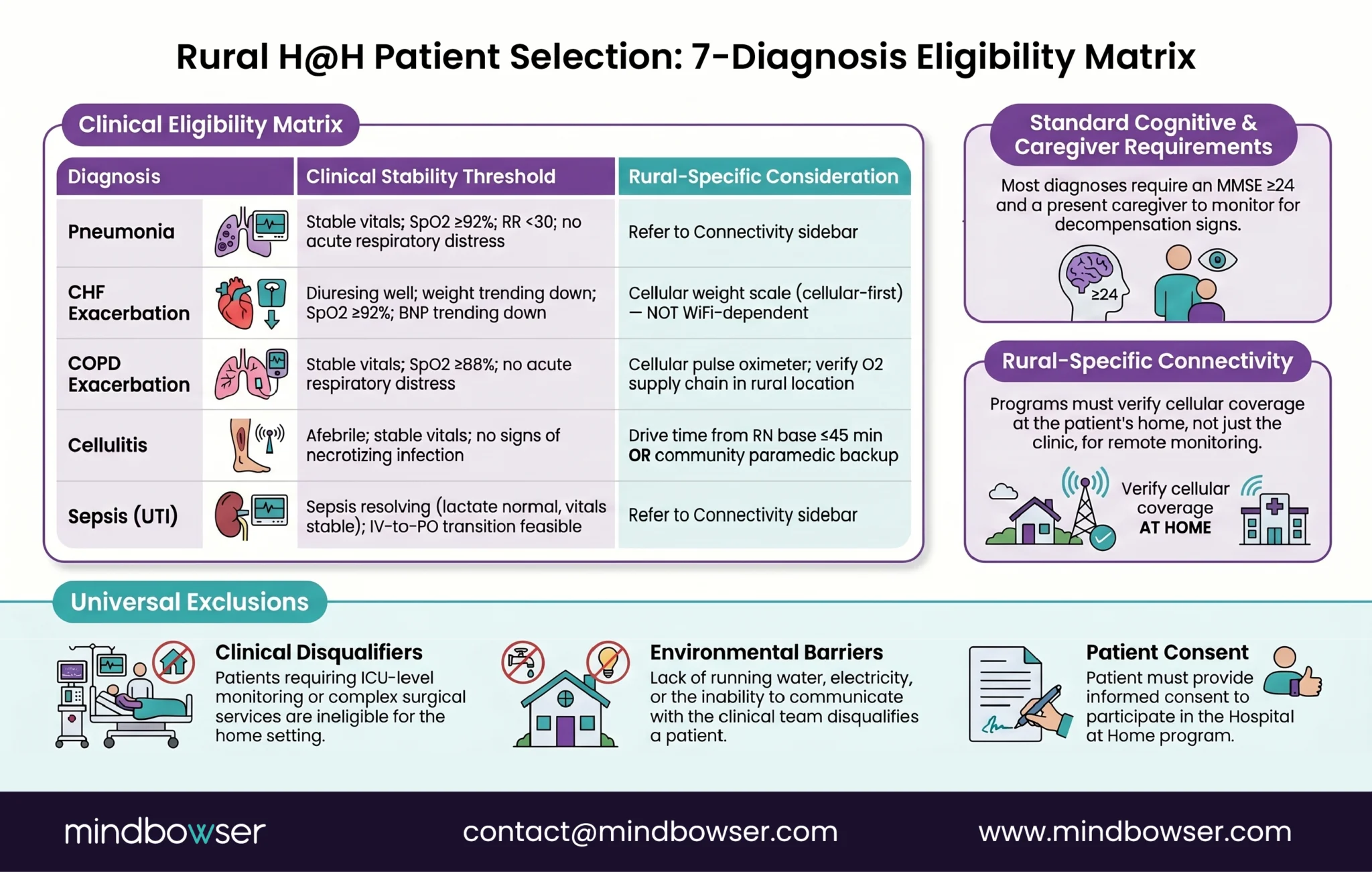
Clinical diagnosis list (starting categories based on CMS AHCAH data and Commonwealth Fund research):
- Community-acquired pneumonia without severe sepsis
- Cellulitis and skin/soft tissue infections
- Uncomplicated pyelonephritis
- Congestive heart failure exacerbation (stable, no recent ICU care)
- COPD exacerbation (moderate severity, no bilateral infiltrates)
- Selected urinary tract infections requiring IV antibiotics
- Post-operative monitoring for specific procedures (narrow list)
Clinical stability thresholds:
- Vital signs within defined ranges for 4-8 hours prior to H@H admission
- Oxygenation requirements met with portable supplemental oxygen
- Mental status intact and capable of participating in care
- No active delirium or acute cognitive decline
- No active psychiatric crisis
Cognitive and functional assessment:
- Patient capable of operating patient-facing app or has caregiver support
- Caregiver availability for 24-hour continuous presence or defined rotation schedule
- Patient willingness to participate in home-based care (not requesting hospital stay)
Home environment assessment:
- Safe home environment without active hazards
- Reliable power (or defined contingency for power loss)
- Sufficient space for medical equipment
- Home accessible for nursing visits (no active construction, etc.)
Rural-specific patient selection considerations:
- Higher median age: Rural H@H patients skew older (median 72 vs 67 urban). Cognitive assessment thresholds matter more.
- Caregiver availability variability: Rural communities have stronger extended family networks in some cases; lower caregiver availability in others (elderly spouse only, adult children geographically distant).
- Transfer distance if H@H fails: Long drive times to inpatient transfer create higher selection thresholds for stability.
- Dual-eligible prevalence: Higher proportion of Medicare + Medicaid dual-eligible patients requires state-specific Medicaid coordination.
Enrollment workflow integration points:
- ED-based screening: Patient presents to ED, meets admission criteria, screened for H@H eligibility before or during admission decision
- Inpatient-unit-based screening: Patient already admitted, identified as H@H-transition candidate during rounds
- Scheduled admission pathway: Patient scheduled for specific procedure or treatment identified as H@H-appropriate in advance
Clinical staff training on selection criteria is week 3-5 work during the 90-day launch. Ongoing case review during the first 30 days of operations calibrates the clinical team’s selection discipline.
Step 5: Logistics, Home Assessments, and Transportation
Logistics is where rural H@H economics differ most from urban H@H. A 15-minute urban home nursing visit becomes a 90-minute rural visit when the patient lives 40 miles from the hospital. The logistics layer has to account for these distances.
Logistics categories:
- Home nursing visit scheduling and routing
- Equipment delivery (RPM devices, IV poles, oxygen concentrators, monitoring hardware)
- Medication delivery including controlled substances with chain-of-custody documentation
- Lab specimen pickup coordination
- Emergency transportation for H@H transfer events
Home nursing visit routing:
Route optimization matters more at rural scale than urban scale. A nurse covering 6 patients in an urban 10-mile radius produces different economics than a nurse covering 6 patients in a rural 40-mile radius. Typical rural H@H programs structure routes in 4-6 patient clusters that a nurse can cover in a single 8-hour shift including drive time.
Equipment delivery:
Initial deployment delivery is scheduled for patient’s home within 2-4 hours of H@H admission. Home-based setup takes 60-90 minutes including RPM device pairing, IV pole assembly if needed, oxygen concentrator placement, and patient/caregiver orientation. Equipment retrieval happens within 24-48 hours of discharge.
Medication delivery and controlled substances:
Most H@H medications are delivered through hospital pharmacy or contracted specialty pharmacy. Controlled substances require specific DEA handling procedures. Rural H@H programs often partner with community pharmacies for same-day delivery capability.
Community paramedicine partnerships:
Community paramedicine is the highest-impact operational partnership for rural H@H. Community paramedics provide emergency response capability, home assessment, and in-home clinical interventions that extend the clinical team’s reach without adding employed clinical FTEs. Several state RHTP plans fund community paramedicine explicitly as a rural care coordination enabler.
Home health agency partnerships:
For H@H programs that do not operate their own employed home nursing staff, home health agency partnerships provide the home nursing capability. Contract terms define visit frequency, response time for urgent visits, and documentation integration with the H@H platform.
For the detailed RPM architecture including device logistics and cellular connectivity, see RPM for Rural Hospitals: Architecture, Cost, and 90-Day Launch Plan.
Step 6: Go-Live Operations and First 30 Days of Patient Care
Go-live is the operationally hardest phase of launch. Workflow gaps that did not surface during pilot appear at scale. Alert fatigue sets in if the AI triage layer is not calibrated. Home nursing visit delays produce documentation and clinical risk events.
Command center operationalization:
The command center monitors all active H@H patients on a real-time dashboard. Continuous vitals transmission from RPM devices produces 50,000-100,000 daily data points per patient. Staffing typically runs 1 RN per 10-15 active patients during high-coverage hours, 1 RN per 20-25 patients during overnight low-acuity hours. AI alert filtering reduces false alerts by 60-80 percent, which is what makes the staffing ratios feasible.
Quality measurement infrastructure:
CMS requires ongoing measurement of 30-day readmission rates, patient safety events, patient experience scores, and mortality rates. Measurement infrastructure must operate from day one. Waiting until day 60 to establish measurement creates both compliance risk and missing data that later prevents program improvement.
Clinician adoption support (weeks 1-2 post go-live):
Technology friction that did not surface in pilot surfaces at scale. Dedicated engineering or vendor support during weeks 1-2 enables rapid iteration. Common friction points: alert threshold calibration for specific physician preferences, documentation workflow variations, video rounding latency under peak load.
Financial and billing validation:
Claims submission for H@H encounters must match CMS billing requirements specifically. Denial rates during first 60 days typically exceed steady-state rates; dedicated billing attention during this window prevents chronic revenue leakage.
Scaling from 3-5 to 10-15 concurrent patients:
The pattern we see: facilities that scale too fast in the first 14 days overwhelm clinical and operational capacity and produce workflow failures. Facilities that scale deliberately (add 2-3 patients per week over weeks 2-6 post launch) stabilize operations and reach 10-15 concurrent patient capacity by day 30.
Common go-live surprises:
- Alert fatigue saturates clinical staff in week 1-2 (AI triage calibration mitigates)
- Home nursing visit delays cause documentation gaps (route optimization + schedule buffers mitigate)
- Patient/family app onboarding friction reduces enrollment speed (guided onboarding + support line mitigates)
- EHR integration gaps surface when real patients generate edge cases (rapid iteration with engineering team)
- Medication delivery logistics fail for controlled substances during after-hours (pharmacy coverage plan mitigates)
Where Rural H@H Launches Fail (and How to Avoid It)
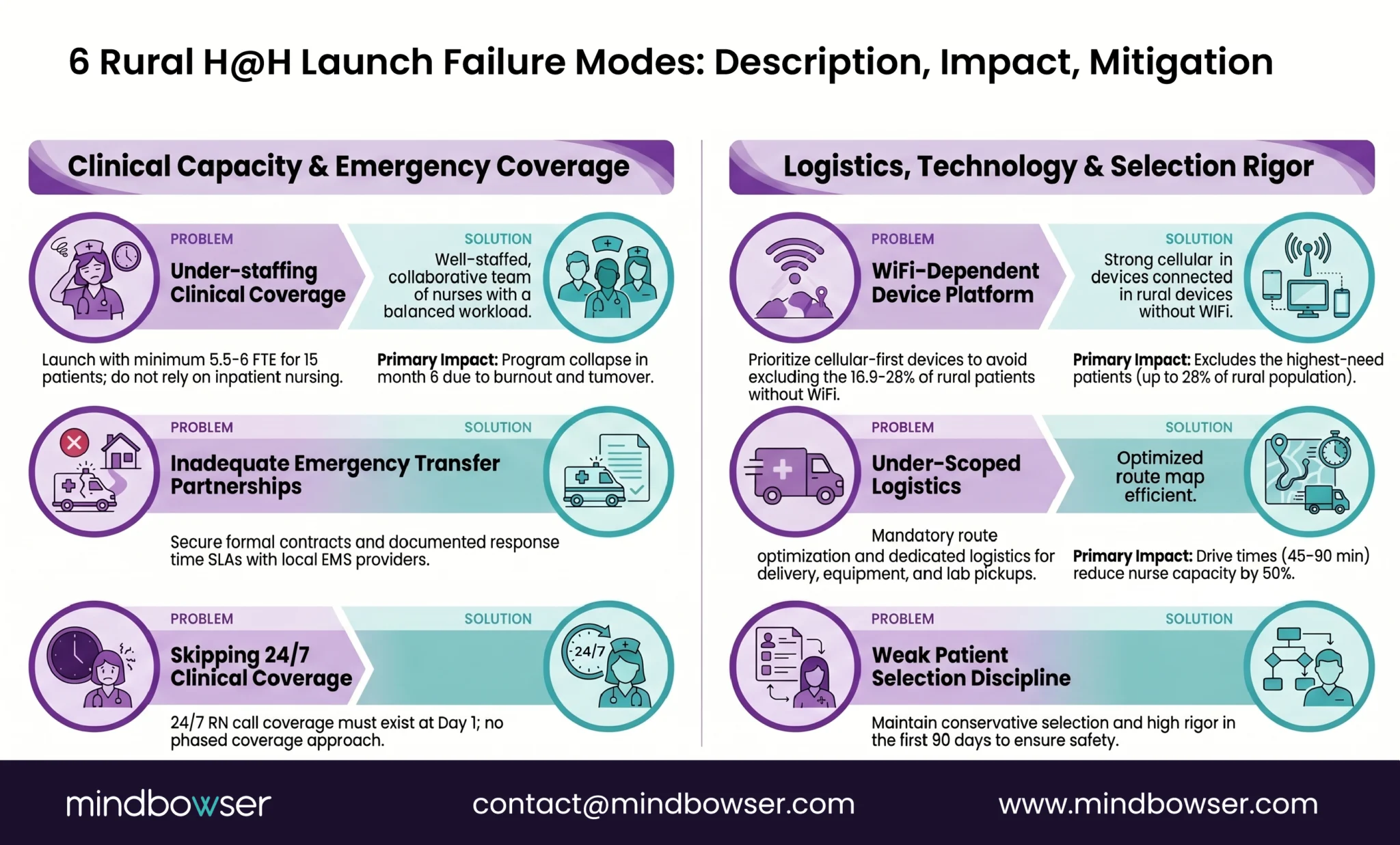
Six patterns we see in rural H@H launches that do not sustain operations past months two or three. Each is preventable with correct sequencing.
Failure 1: Under-staffing clinical coverage.
Clinical team starts H@H with existing staffing, assumes capacity is sufficient, and discovers in week 3-6 that nurses are working extended shifts to cover 24/7 command center plus home visits. Burnout follows. Staff turnover follows burnout. Program operational capacity collapses in month 2-3.
Mitigation: Staff the 24/7 command center and home visit routes before launch, not during. AI documentation and telehealth specialty consultation extend workforce capacity. Community paramedicine partnerships fill emergency response. Do not launch understaffed and plan to hire during operations.
Failure 2: Technology platform that excludes rural patients without broadband.
Platform requires home WiFi for RPM device connectivity. 23 percent of rural patients lack broadband. Program enrolls only the 77 percent with broadband, which reduces patient pool below sustainable volume. Program is accused (correctly) of selecting against the patients most in need.
Mitigation: Cellular-first RPM architecture from day one. Budget $15-25 per patient per month for cellular data plans. Do not accept a vendor platform that requires home WiFi.
Failure 3: Inadequate emergency transfer partnerships.
H@H patient decompensates at 2 AM. No established EMS transfer protocol. Ambulance service does not recognize patient as H@H enrollee. Clinical team cannot reach patient in time. Clinical event occurs. CMS notices.
Mitigation: Formal emergency response partnerships with local EMS agencies documented before launch. Include H@H-specific protocols for rapid transfer. Test the protocol during pilot phase with tabletop exercises.
Failure 4: Under-scoping the logistics layer.
Program launches with assumption that logistics (home visits, equipment delivery, medication delivery, lab pickups) can be managed ad-hoc. By week 3, delays have accumulated. Patients do not get medications on time. Home nursing visits are late. Documentation gaps create billing issues.
Mitigation: Explicit logistics staffing and workflow before launch. Route optimization technology, not manual scheduling. Defined SLAs with contracted partners (home health agencies, pharmacies, EMS).
Failure 5: Weak patient selection discipline.
Program is under volume pressure. Clinical staff enrolls patients who should remain inpatient. Patients decompensate. Clinical events occur. Staff confidence in program drops. Administrators question whether to continue.
Mitigation: Strict diagnosis list for first 60 days. Expand diagnosis list only after operational maturity demonstrated. Case review of every H@H admission during first 30 days. Clinical leadership reinforces selection discipline.
Failure 6: Skipping 24/7 clinical coverage setup.
Program plans to handle nights and weekends with on-call coverage. Overnight alerts go to on-call physician who is asleep. Alert response times exceed CMS waiver requirements. Compliance gap accumulates. CMS audit surfaces the issue.
Mitigation: 24/7 clinical command center coverage from go-live, staffed by RNs with defined physician escalation. Not on-call only. The command center is the regulatory compliance foundation, not an optional operational convenience.
How RHTP Funding Makes Rural H@H Economically Viable
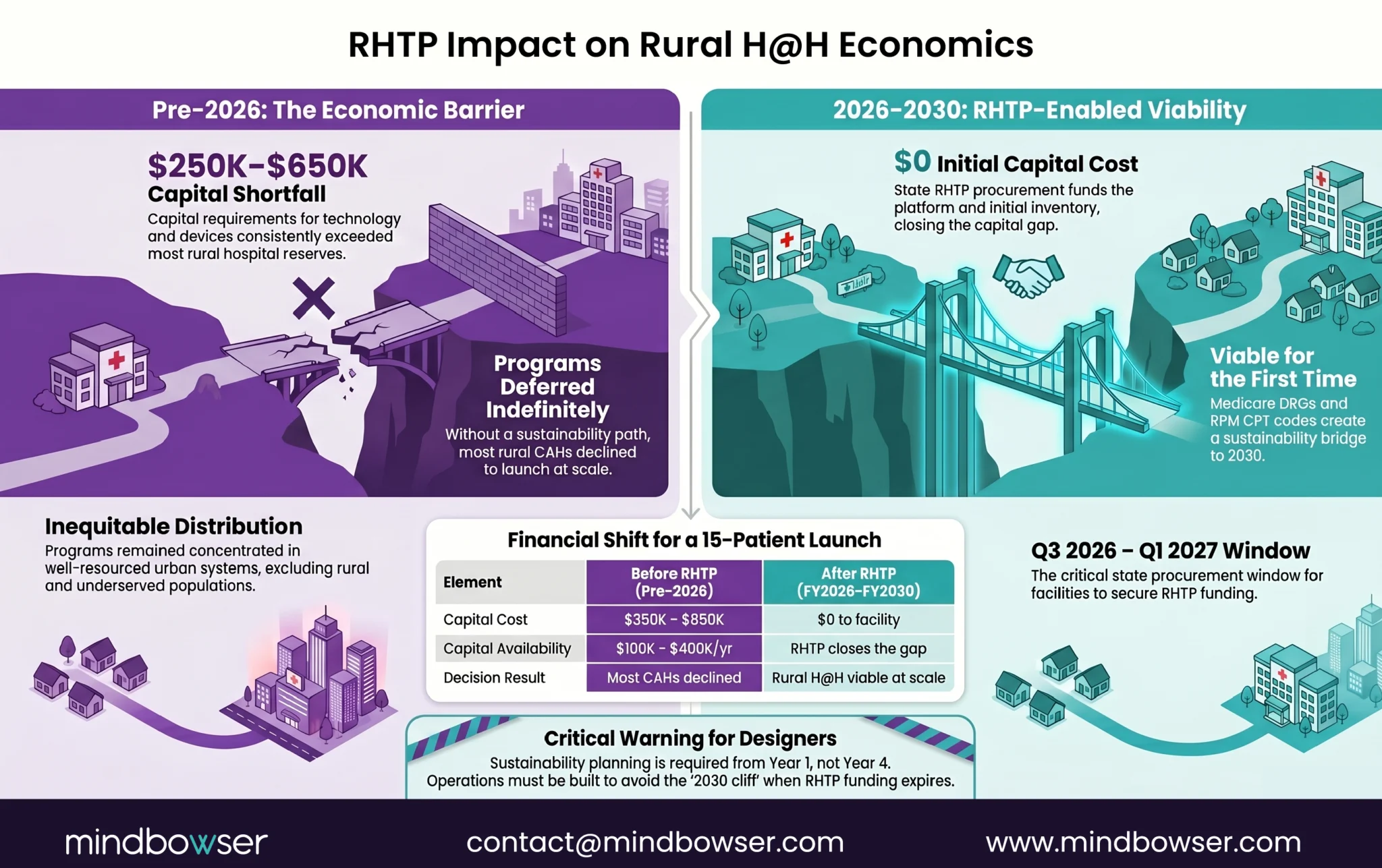
The financial model before RHTP explained why rural hospitals launched H@H at meaningfully lower rates than urban academic medical centers. The model after RHTP explains why the pattern is reversing.
Financial model before RHTP:
Rural H@H capital cost: $300K-$700K platform build or purchase plus $50K-$150K initial clinical setup costs. Total upfront: $350K-$850K per facility.
Rural H@H ongoing operating cost: $9K-$23K per month platform operations plus $80K-$180K annual clinical staffing for 15-patient concurrent capacity. Annual run rate: $180K-$400K.
Rural H@H revenue capture: Medicare cost-based reimbursement covers operating costs at 101 percent, so operating costs are covered by Medicare service revenue. Commercial payer revenue adds margin. Medicaid coverage varies by state (some states actively reimburse, others do not).
The capital gap is what killed rural H@H launches. A CAH operating at 1-3 percent margin generates insufficient cash flow to cover the upfront capital cost. Commercial financing is available but expensive at rural hospital credit profiles. HRSA Flex grants and state rural health grants are too small to close the gap.
Financial model after RHTP:
RHTP state procurement funds the capital cost directly or through state eHealth organization partnerships or through rural hospital network shared-services arrangements. Massachusetts’s RHTP plan lists Hospital-at-Home expansion as Activity 7 within Initiative I. Similar explicit H@H allocations appear in several other state plans including Arkansas, Maine, and additional state plans currently in review.
With RHTP funding closing the capital gap:
- Platform capital deployed without rural hospital capital exposure
- Clinical setup capital funded under RHTP Initiative D (training) and Element H (innovation)
- Operating cost covered by Medicare cost-based reimbursement plus commercial revenue post-launch
- Sustainability bridge to 2030 through Medicare billing maturity and state appropriations
The economic calculation shifts from “can we afford to launch H@H” to “can we position for state RHTP procurement.” Rural hospitals that engage their state RHTP program during Q1-Q3 2026 stakeholder processes have the positioning advantage. Rural hospitals that wait past this window miss the initial RFP cycles.
For the RHTP funding mechanics including engagement playbook and state-specific procurement timing, see our RHTP Funding Technology Guide.
How Mindbowser Helps Rural Hospitals Launch H@H
Mindbowser builds healthcare technology specifically for small and rural hospital operational constraints. Our accelerator stack maps to five of the seven H@H technology components, which is what compresses the technology deployment portion of the 90-day launch.
- HealthConnect CoPilot delivers care coordination and EHR integration across MEDITECH Expanse, Epic Community Connect, Athena, and eClinicalWorks. FHIR R4 native, USCDI v3 ready, operationally sustainable for 1-2 person rural IT teams.
- WearConnect handles cellular-first RPM across 14 device manufacturers through a single FHIR-compatible ingestion layer. The device-agnostic architecture handles rural broadband reality and prevents vendor lock-in as RPM markets evolve.
- AI SummaryAssist reduces clinical documentation time by 40-55 percent per encounter. For rural H@H programs where one physician covers multiple patient panels, this is the workforce capacity expansion that makes the program operationally feasible.
- PHISecure covers HIPAA compliance posture and managed security operations for rural hospitals without internal security teams.
Engagement model for rural H@H launch:
- 12-16 week technology deployment that fits within the 90-day launch window (technology is the longest workstream; clinical and regulatory work happens in parallel)
- Engagement paths: direct state contract (RHTP-funded), prime contractor subcontract, state eHealth organization partnership, rural hospital network shared-service deployment
- Operational handoff designed for 1-2 person rural IT teams to sustain
Conclusion
Rural Hospital-at-Home programs are no longer limited by geography alone. With the CMS waiver extended through 2030 and RHTP funding opening new procurement opportunities, rural hospitals now have a realistic path to launch and scale H@H programs in as little as 90 days. The difference comes down to execution. Hospitals that sequence staffing, technology, patient selection, logistics, and compliance correctly can expand care capacity without building new beds or stretching clinical teams beyond their limits. Rural H@H is not about copying urban models. It is about building a practical, sustainable care model designed for rural realities from day one.
Yes. Critical Access Hospitals are explicitly eligible for the CMS Acute Hospital Care at Home waiver. CAHs participate in H@H while maintaining cost-based Medicare reimbursement, which is a meaningful financial advantage over PPS hospitals. CAH-specific constraints (1-2 IT staff, limited broadband in service area, rural patient demographics) require technology platforms and operational models designed for these constraints. RHTP funding flowing in 2026-2030 makes CAH H@H launches financially feasible for the first time.
90 days if the facility meets four prerequisites (active CMS certification, minimum sustainable patient volume of 15-25 H@H-eligible admissions per month, clinical staffing capacity or contracted partnership, technology platform capability). CMS waiver application review takes 4-8 weeks, technology platform deployment takes 12-16 weeks, clinical protocol and staffing preparation runs in parallel. Rural hospitals using pre-built accelerators or RHTP-funded platforms launch faster than rural hospitals attempting proprietary builds.
Total launch cost runs $350K-$850K (platform capital plus clinical setup), plus $180K-$400K annual operating run rate for 15-patient concurrent capacity. Without RHTP funding, this capital cost exceeds what rural hospitals can typically fund from operating margin or commercial financing. With RHTP funding flowing through state procurement in 2026-2027, the capital cost is fundable through state contracts or state eHealth organization partnerships, removing the historical barrier to rural H@H launch.
The CMS Acute Hospital Care at Home waiver requires continuous or near-continuous patient monitoring, daily physician or APP evaluation (typically via video rounding), 24/7 patient communication access and emergency escalation, ability to transfer patient to brick-and-mortar facility within defined timeframes, documented informed consent with H@H-specific disclosures, and ongoing quality measurement covering 30-day readmission rates, patient safety events, patient experience, and mortality. The waiver is extended through September 2030. See our Hospital at Home CMS Waiver Guide for full detail.
A 15-patient rural H@H program typically staffs with 1 medical director (physician or APP, rounding 2x daily via video), 2-3 RNs covering command center and home visits across three shifts, 1 care coordinator, and 1 community paramedic or contracted home health nurse for emergency response. Rural workforce constraints are addressed through AI clinical documentation (reduces physician hours per patient), telehealth specialty consultation (eliminates need for on-staff specialists), and community paramedicine partnerships (emergency response without expanding employed EMS). 24/7 clinical command center coverage is a CMS waiver requirement and cannot be met with on-call coverage alone.
Medicaid coverage varies by state. Some states actively reimburse H@H admissions for Medicaid patients; others do not. The Center for Health Care Strategies (CHCS) maintains a dedicated resource on Medicaid H@H coverage by state. Several state RHTP plans include Medicaid H@H expansion as a funded activity, which would increase coverage in those states after 2026-2027 implementation. For rural hospitals with significant Medicaid patient populations, state Medicaid coordination is part of the H@H launch regulatory workstream.
The seven H@H technology components are: continuous RPM (cellular-first for rural), video rounding platform (bandwidth-adaptive), AI alert filtering (reduces false alerts 60-80 percent), EHR integration (FHIR R4 with MEDITECH/Epic/Athena), patient-facing app (onboarding optimized for elderly with minimal tech experience), care coordination dashboard (single view for 24/7 command center), and logistics dispatch (home nursing routing, medication delivery, equipment setup). Rural hospitals typically use vendor platforms, custom builds, or RHTP-funded shared platforms depending on facility circumstances. See our Hospital at Home Technology Platform Guide for the complete architecture. This page references the following primary federal sources. All citations link directly to the official Federal Register, CFR, or agency record.
