



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
The $50 billion Rural Health Transformation Fund flows through state procurement processes that most states are building from scratch. Every state has an approved plan, but the translation from plan narrative to RFPs to contracts happens between Q3 2026 and Q1 2027. For hospitals, health systems, and vendors positioned to capture funded work, the decision point is not the federal program. It is the state’s specific allocation across statutory elements and the stakeholder engagement process each state runs. This guide covers how the money actually flows, which technology categories are eligible, how to get your facility or capability into the state’s funded activities, what typical RFP structures look like, and where most grant recipients misread the spending mechanics.
Spending $10 billion per year is harder than it sounds, especially when the money has to flow through 50 separate state procurement processes that did not exist 18 months ago.
That is the actual operational reality of the Rural Health Transformation Program in 2026. Congress authorized $50 billion under Section 71401 of Public Law 119-21. CMS awarded all 50 states on December 29, 2025. State health agencies hired program directors and initiative leads through Q1 2026. State workplans finalized between March and June 2026. RFPs start posting between July 2026 and Q1 2027. Implementation contracts get awarded through Q2 2027. Money starts flowing to facilities and vendors after contract execution.
For hospitals, health systems, and technology vendors positioned to capture RHTP-funded work, the federal program is not the decision point. The state’s specific allocation across seven statutory elements, the activities named in the state’s approved plan, and the stakeholder engagement process each state runs during Q1-Q3 2026 are the decision points.
This guide is written for grant recipients at the state and facility level who need to translate “our state got $X million” into specific technology spending decisions that qualify for RHTP funding and survive state procurement scrutiny.
For the program-level overview, see our Rural Health Transformation Program complete guide. This piece is the practitioner playbook for what happens after the awards.
What Is the Rural Health Transformation Fund?
The Rural Health Transformation Fund is the $50 billion pool authorized by Section 71401 of Public Law 119-21 for distribution to all 50 states over five fiscal years (FY2026 through FY2030), $10 billion per year. CMS administers the federal program. States administer their individual allocations through state health agencies, Medicaid offices, or cross-agency coordinating bodies.
Three mechanics distinguish the Rural Health Transformation Fund from prior rural health funding streams.
- Scale: Prior federal rural health programs (HRSA Flex, SHIP, Rural Health Clinic support) operate at $350-400 million per year combined. RHTP allocates 25 times that annually to states.
- State discretion: Each state determines its own spending priorities within the seven statutory elements defined by the legislation. Activities funded in Vermont look different from activities funded in Texas, reflecting the actual needs and infrastructure of each state’s rural population.
- Implementation requirement: The statutory scoring favored states that demonstrated operational capability to execute, not just need. States that scored higher on operational readiness now carry the implementation expectation downstream to vendors and facilities that participate in state procurement.
The fund will end September 30, 2030 absent Congressional reauthorization. That boundary condition shapes sustainability planning, which states must document in Year 4 of the program (FY2029).
How Does the $50B Connect to Medicaid Cuts?
Sophisticated readers of RHTP content encounter a recurring framing in policy analysis: the fund exists partly to soften the impact of Medicaid reductions enacted in the same legislative package. The numbers matter. KFF’s November 2025 analysis calculated that the reconciliation law that created RHTP also reduces federal Medicaid spending by approximately $911 billion over ten years, with approximately $137 billion of that reduction falling on rural areas specifically. The $50 billion RHTP allocation offsets about 36% of the rural Medicaid cut across the same decade. On net, rural healthcare loses roughly $87 billion, meaning RHTP is positioned as partial offset, not net new capacity funding.
The operational framing matters more than the political one. Rural hospitals are disproportionately Medicaid-dependent. Commercial payer mix in rural service areas is lower. A reduction in Medicaid reimbursement hits rural facilities harder than urban facilities. The institutional data is what makes this concrete. The UNC Cecil G. Sheps Center rural hospital closures tracker shows 153 rural hospital closures and conversions since 2010, including 85 complete closures and 68 converted closures. CHQPR (Center for Healthcare Quality and Payment Reform) estimates 760 rural hospitals are currently at risk of closing, with 314 at immediate risk within three years, and reports 23 rural hospital closures in 2025 alone. AHA’s April 2025 financial analysis documented that Medicare reimbursed only 83 cents for every dollar hospitals spent caring for patients in 2023 and that general inflation rose 14.1% against a 5.1% Medicare inpatient payment increase from 2022 to 2024. RHTP arrives into a system where the financial baseline is already distressed and getting worse.
The practical implication for grant recipients: the money is real, the spending categories are broad, and the policy debate does not change what you can fund under the statutory elements. A Critical Access Hospital in Kentucky does not need to resolve the political framing to pursue RHTP-funded technology modernization. The procurement window opens regardless.
What does matter: states with larger Medicaid-impact exposure may prioritize RHTP spending toward activities that directly offset revenue pressure (value-based payment infrastructure, RCM modernization, population health platforms) rather than toward infrastructure that primarily serves long-term capacity building. Grant recipients should read their state’s plan carefully to identify which framing their state adopted. The Center on Budget and Policy Priorities (CBPP) analysis of the reconciliation package argued that “Rural Health Fund Will Do Little to Offset Harm to Rural Providers” given the net reduction after subtracting RHTP from the Medicaid cut. That argument is worth engaging with, whether or not a particular hospital’s leadership agrees with CBPP’s framing, the operational question of which RHTP spending categories produce the most durable revenue stabilization is the same regardless of political lens.
Which Technology Categories Are Eligible?
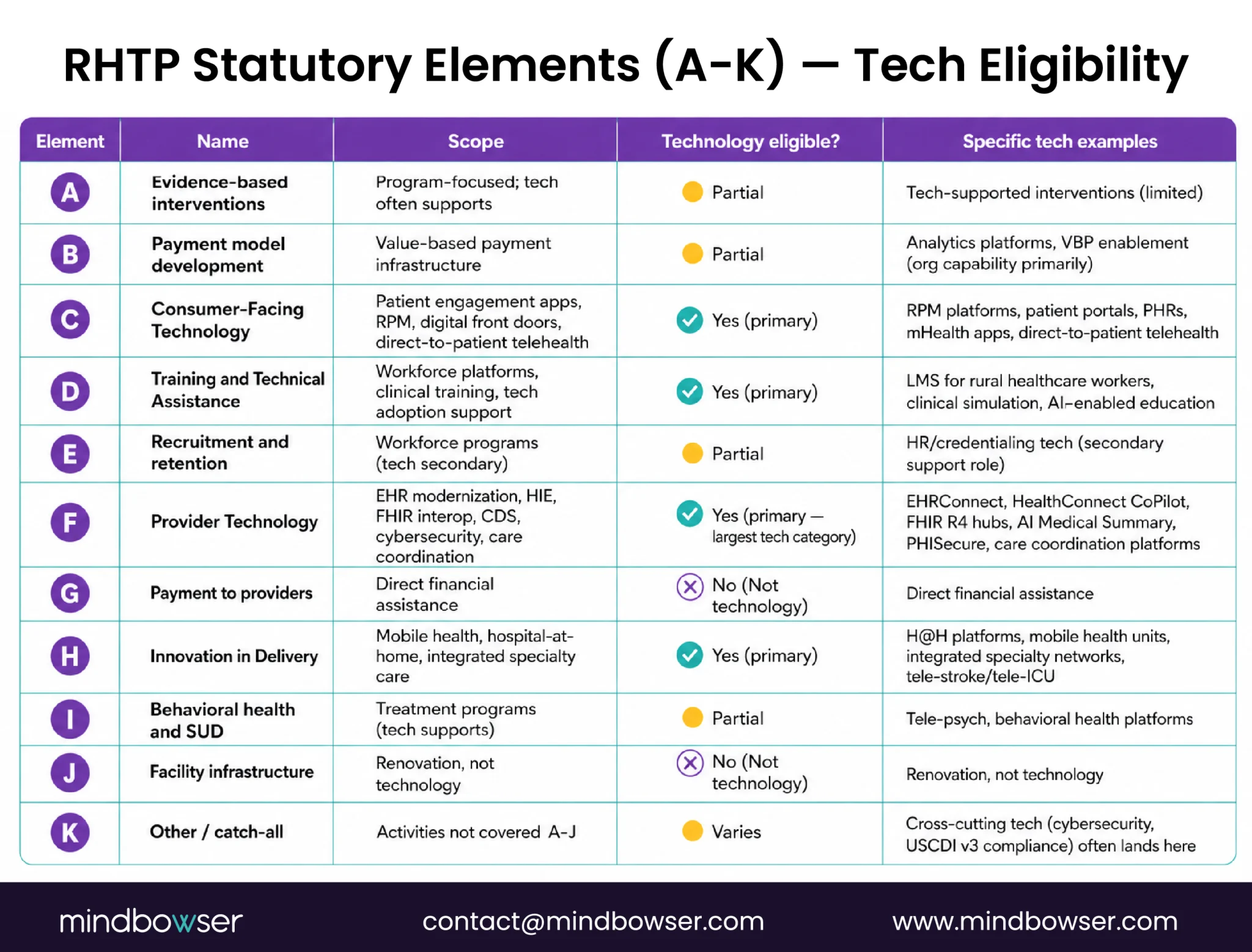
The seven statutory use-of-funds elements (A through K, with some letters skipped in the original legislation) define what qualifies for RHTP spending. Technology touches four of them directly.
- Element C: Consumer-Facing Technology: Patient engagement applications, remote patient monitoring devices and platforms, digital front doors, telehealth platforms offered directly to patients. Most state plans include RPM expansion as an Element C activity.
- Element D: Training and Technical Assistance: Workforce development platforms, clinical training programs, technology adoption support. Virtual training platforms, LMS for rural healthcare workers, and AI-enabled clinical education tools fall under Element D.
- Element F: Provider Technology: EHR modernization, health information exchange (HIE) capacity, FHIR-based interoperability, clinical decision support, cybersecurity infrastructure, care coordination platforms. This is the largest technology category in most state plans.
- Element H: Innovation in Delivery: Mobile health units, hospital-at-home programs, integrated specialty care networks, new care delivery models. State plans that fund hospital-at-home technology typically cite Element H.
What falls outside the four technology-direct elements:
- Element A (evidence-based interventions) is primarily program-focused rather than technology-focused, though it often includes technology-supported interventions
- Element B (payment model development) includes technology to support value-based payment but usually funds organizational and analytical capability rather than platforms
- Element E (recruitment and retention) funds workforce programs; technology is a secondary component
- Element G (payment to providers) is direct financial assistance rather than technology infrastructure
- Element I (behavioral health and substance use disorder) funds treatment programs; technology supports but does not lead
- Element J (facility and physical infrastructure) funds renovation, not technology
- Element K (other) is the catch-all for activities not covered A-J
Cross-category spending is common: A care coordination platform might serve Element C (consumer-facing), Element F (provider technology), and Element H (innovation in delivery) simultaneously. State plans often list the same activity under multiple elements for flexibility.
What Are States Actually Funding (Not Promising)?
Reading 50 state plans reveals a pattern that matters for grant recipients: the rhetoric of what states plan to fund and the actual dollar allocations frequently diverge. States list aspirational activities to score well on application narrative, then concentrate actual spending in a narrower set of proven categories during implementation.
What shows up as actual funding across most state plans (high-confidence spending categories):
- HIE and FHIR onboarding infrastructure: Initiative VI equivalents in most states. Massachusetts funds $83M over five years on Technology Interoperability alone. Similar allocations appear in 35+ other state plans.
- RPM expansion infrastructure: Named as funded activity in Massachusetts, Kansas, Maryland, South Carolina, and 20+ other state plans
- Clinical AI deployment: Explicitly funded in Maine (Rural AI Hub), Utah (clinical AI agents), Massachusetts (AAEM), Texas (AI-automated fax processing), West Virginia, Tennessee
- Telehealth infrastructure and hub-and-spoke: Arizona, Arkansas, Maine, Florida, Utah, and most state plans with rural broadband gaps
- EHR modernization (typically subsidizing small facilities joining larger instances): Oklahoma, New Mexico, several other state plans
- Cybersecurity managed services: Maine, Utah, Massachusetts partnership with MeHI/MassCyberCenter, and growing adoption across state plans
What shows up in narratives but rarely as funded line items:
- Moonshot-style AI initiatives without specific operational plans
- Proprietary platform commitments that lock states into single vendors (CMS scoring penalizes vendor lock-in)
- Aspirational “innovation” categories without measurable outcomes
- Activities that duplicate existing federal programs (Flex, SHIP) without clear coordination
The pattern matters for vendors and grant recipients: states funded the categories where existing infrastructure, vendor capacity, and measurable outcomes exist. States deferred or sidelined the categories where the execution path was unclear. Technology that sits in the first list has a meaningfully higher probability of being funded than technology in the second list.
How Do You Get Your Facility Into the State’s Funded Activities?
RHTP funding does not flow to every rural facility automatically. It flows through state procurement processes that select specific recipients or contracts for specific activities. Getting your facility (or your capability) into the funded activities requires active engagement during a narrow window.
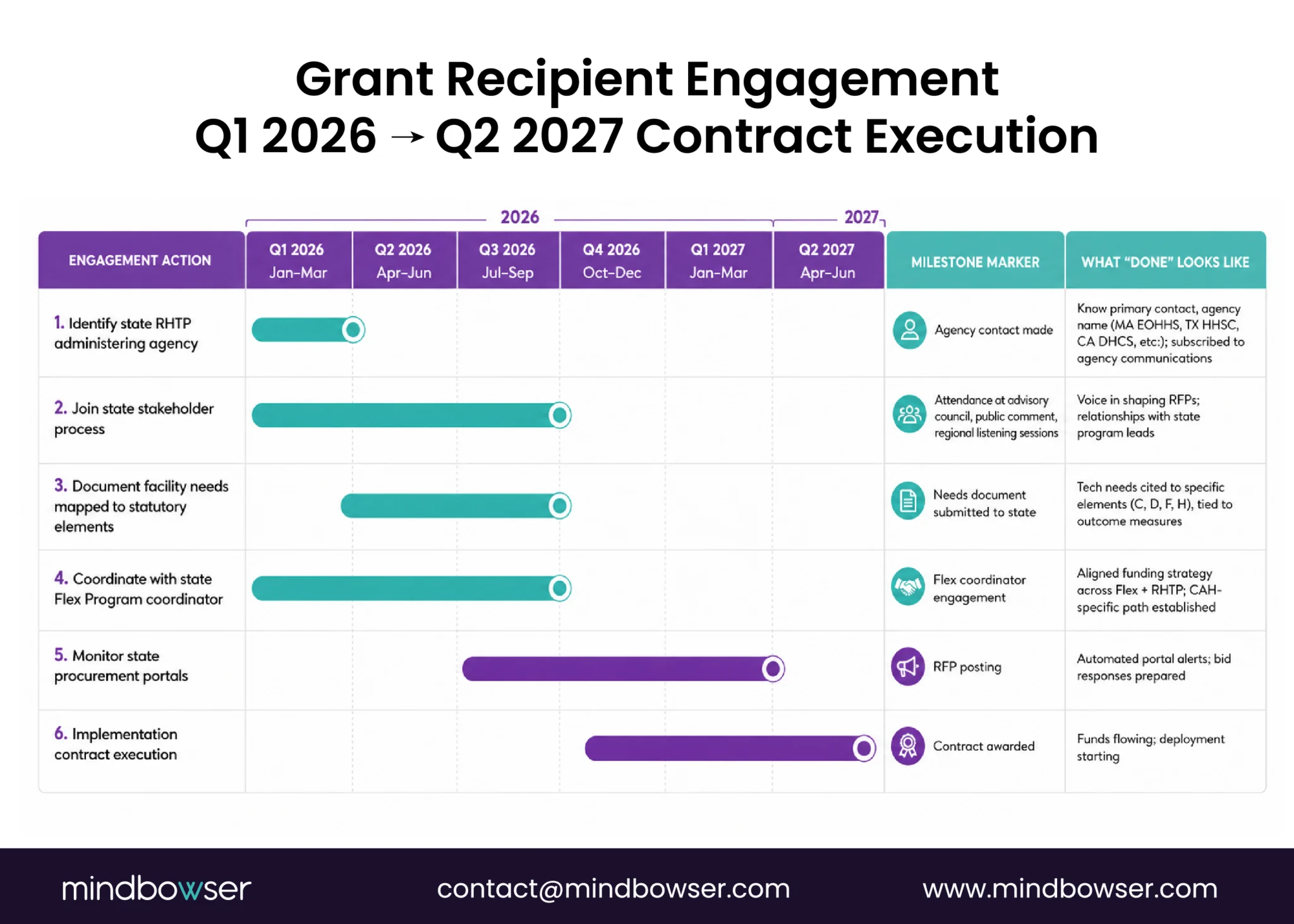
The engagement timeline:
- Q1-Q3 2026 (now through August): State program directors and initiative leads set up governance, finalize workplans, and run stakeholder engagement sessions. This is the window when facility needs get incorporated into planned RFPs. Missing this window means your specific situation is not reflected in the RFPs that post later.
- Q3-Q4 2026: States post initial RFPs. Vendor selection begins. Contract structures finalize.
- Q4 2026-Q2 2027: Implementation contracts execute. Initial funds flow to selected vendors and facilities.
- Beyond Q2 2027: Additional RFP cycles, cohort expansions, and follow-on contracts. Smaller windows of opportunity but still meaningful.
Four engagement actions that matter:
- Identify your state’s RHTP administering agency: Typically the state Medicaid agency, state health department, or a cross-agency coordinating body (e.g., Massachusetts Executive Office of Health and Human Services). State websites have published program pages with contact information.
- Join the state’s stakeholder process: Every state RHTP governance structure includes stakeholder engagement mechanisms: advisory councils, public comment periods, regional listening sessions. Attendance is typically open to hospital administrators, health system representatives, vendors, and community organizations.
- Document your facility’s needs in a format that maps to RHTP statutory elements: Generic capital wishlists do not survive procurement review. Specific technology needs mapped to specific statutory elements (Element C, D, F, H as applicable) and tied to outcome measures are the shape RHTP RFPs will take.
- Engage your state’s Flex Program coordinator. State Flex coordinators are typically involved in RHTP governance and bring longitudinal CAH relationships. If your facility is a CAH, the Flex coordinator is often the most direct path into the RHTP conversation.
Planning to use RHTP funding for healthcare technology modernization?
What Procurement Looks Like in Practice
State procurement structures vary, but common patterns emerge across the state plans we have read.
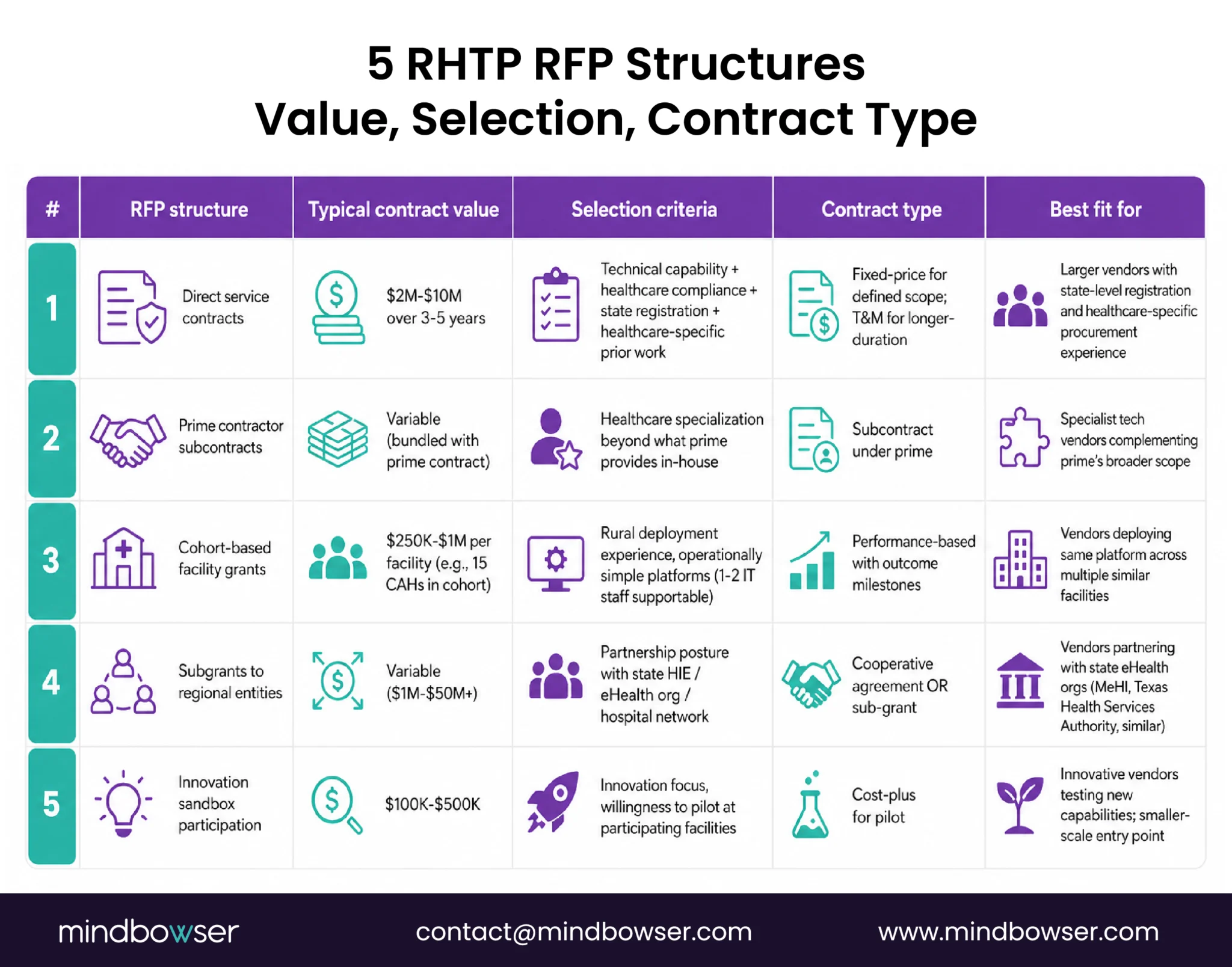
Typical RFP structures:
- Direct service contracts: State contracts directly with vendors for specific technology deliverables (e.g., Rural MA Connect platform build). Contract values typically $2M-$10M over 3-5 years.
- Prime contractor subcontracts: Large consulting firms or systems integrators prime the contract with the state, then subcontract to technology vendors for specific build components. Common for initiatives with multiple technology and non-technology activities bundled.
- Cohort-based facility grants: State selects cohorts of facilities (e.g., 15 CAHs) that receive RHTP-funded technology deployments administered by a prime vendor or consortium. Individual facility allocations typically $250K-$1M.
- Subgrants to regional entities: State grants funds to state eHealth organizations (e.g., MeHI), rural hospital networks, or population health collaboratives that administer technology deployments across member facilities.
- Innovation sandbox participation: State-run innovation programs (digital health sandboxes) where selected vendors receive modest funding ($100K-$500K) to pilot technology at participating facilities.
Vendor selection criteria common across state plans:
- Technical capability documented with prior builds
- Healthcare-specific compliance posture (HIPAA, HITRUST, state requirements)
- Rural deployment experience or explicit rural-aware architecture
- Implementation timeline that matches state fiscal year constraints
- Sustainability plan for operations beyond the RHTP funding window
- Partnership posture with existing state technology infrastructure (HIE, state Medicaid systems)
Contract types to expect:
- Fixed-price contracts for defined-scope technology deliverables
- Time-and-materials contracts for longer-duration implementation work
- Cost-plus contracts for research and pilot activities (less common)
- Performance-based contracts with outcome milestones (increasingly common as CMS emphasizes measurable results)
Where vendors lose procurements:
- Failure to demonstrate healthcare-specific prior work (generic software development credentials insufficient)
- Lack of rural deployment awareness (urban-scale platform pitches misfire)
- Missing state-specific requirements (each state has unique registrations, insurance, certifications)
- Weak sustainability plans (states penalize vendors that cannot articulate post-2030 operations)
HRSA Grants & RHTP Technology Implementation Guide: Structure grant-funded technology investments before procurement begins.
Where Most Grant Recipients Get the Spending Wrong
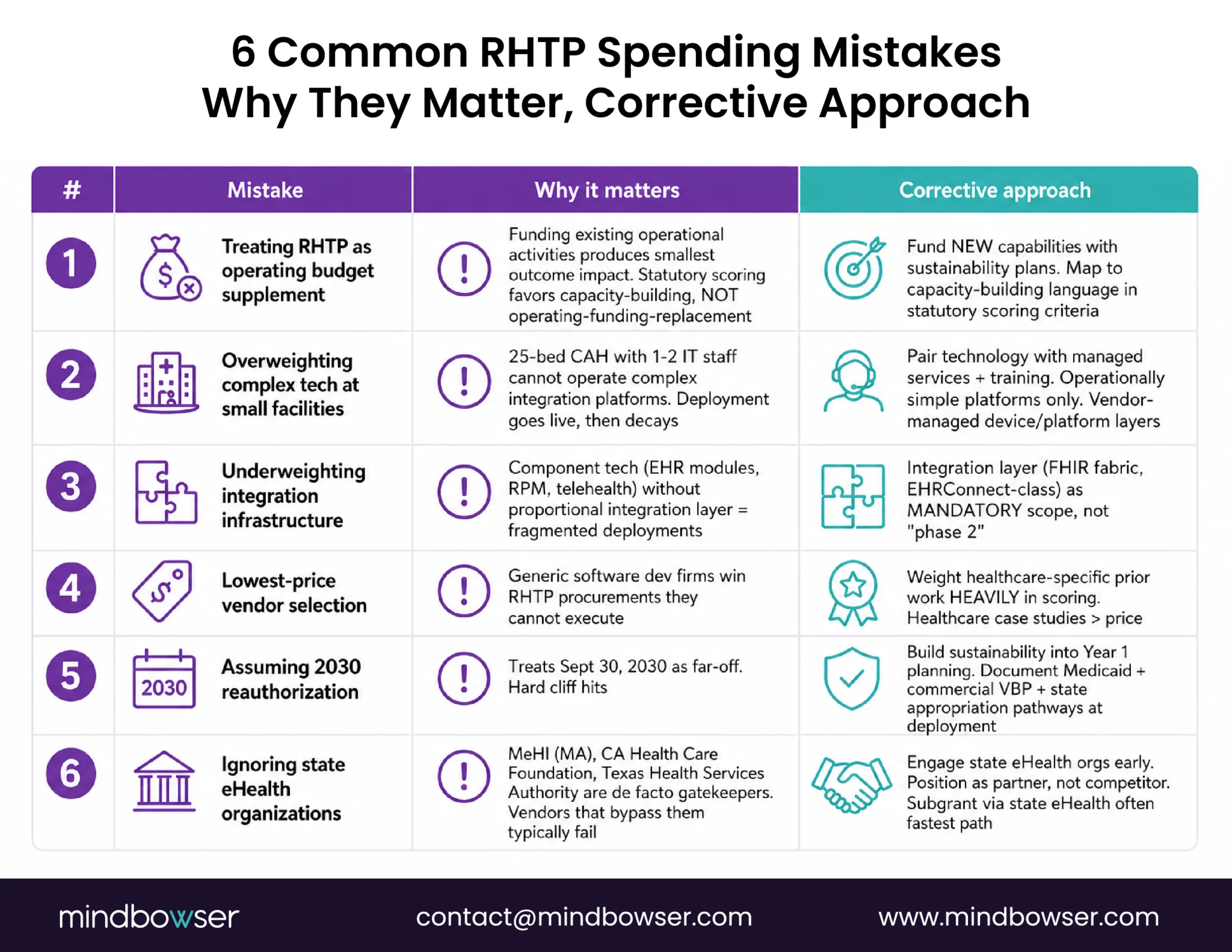
Six patterns we have seen or read about in state plans and stakeholder engagement sessions that undermine RHTP-funded outcomes:
- Mistake 1: Treating RHTP as an operating budget supplement rather than a capability build: States that funded existing operational activities with RHTP dollars produce the smallest outcome impact. States that funded new capabilities with sustainability plans produce the largest. The statutory scoring reinforces this: programs classified as capacity-building score higher than programs that replace existing funding.
- Mistake 2: Overweighting technology that requires deep IT capacity at small facilities: A 25-bed Critical Access Hospital with 1-2 IT staff cannot operate complex integration platforms without managed services. States that funded complex technology without also funding operational support produce deployments that go live and then decay. States that paired technology with managed services and training produce sustained operational impact.
- Mistake 3: Underweighting integration infrastructure: Every state plan includes technology components that require interoperability to function as a system. Plans that funded component technology (EHR modules, RPM platforms, telehealth) without proportional investment in the integration layer produce fragmented deployments.
- Mistake 4: Selecting vendors based on lowest proposal price without weighing healthcare-specific execution capability. Generic software development firms win RHTP procurements they cannot execute. States that weight healthcare-specific prior work heavily in scoring produce better outcomes. This pattern is driving increased RFP scoring emphasis on healthcare case studies.
- Mistake 5: Assuming RHTP funding renews after 2030: The legislation authorizes five years. Reauthorization would require future Congressional action. States that built sustainability into Year 1 planning protect their investments. States that treated 2030 as a far-off consideration face a hard cliff.
- Mistake 6: Ignoring state eHealth organizations as gatekeepers: Massachusetts eHealth Institute, California Health Care Foundation, Texas Health Services Authority, and similar organizations in other states are de facto gatekeepers for vendor participation in state procurements. Vendors that try to bypass them into direct state contracts typically fail.
The grant recipients (facilities and vendors) who avoid these six mistakes are a small share of the total pool. The ones who address them explicitly have the strongest position in Q4 2026-Q2 2027 procurement cycles.
How to Structure Technology Investments to Qualify for RHTP
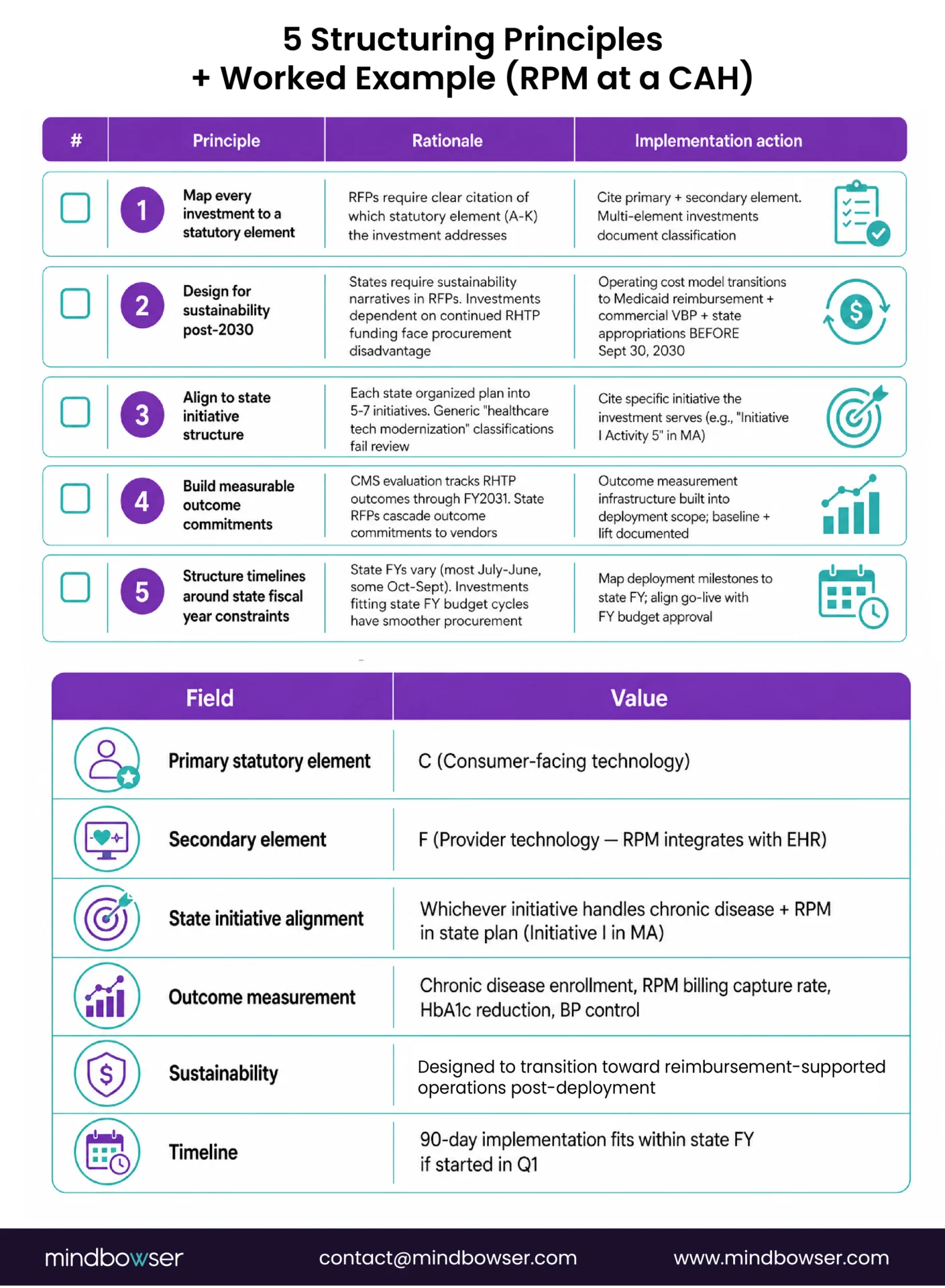
For facilities and vendors planning technology investments that need to qualify for RHTP funding, five structuring principles matter.
- Principle 1: Map every investment to a statutory element: RFPs will require clear citation of which statutory element (A-K) the investment addresses. Investments that cannot be cleanly classified do not survive procurement review. Multi-element investments should note primary and secondary element classifications.
- Principle 2: Design for sustainability post-2030: States will require sustainability narratives in RFPs. Investments that depend on continued RHTP funding for operations after September 30, 2030 face procurement disadvantage. Design operating cost models that transition to Medicaid reimbursement, commercial payer billing, or state appropriations before 2030.
- Principle 3: Align to state initiative structure: Each state organized its plan into 5-7 initiatives (Massachusetts has seven; other states vary). Investments must cite the specific initiative they serve. Generic “healthcare technology modernization” classifications will not survive review.
- Principle 4: Build measurable outcome commitments:. CMS evaluation will track RHTP outcomes through FY2031. State RFPs will cascade outcome commitments to vendors and facilities. Investments without clear outcome measurement infrastructure will struggle in procurement and evaluation.
- Principle 5: Structure implementation timelines around state fiscal year constraints: State fiscal years vary (most run July-June, some October-September). Investments that fit state FY budget cycles have smoother procurement paths than investments that require mid-year appropriations.
Tactical structuring example (RPM infrastructure at a CAH):
- Primary statutory element: C (consumer-facing technology)
- Secondary element: F (provider technology, because RPM integrates with EHR)
- State initiative alignment: Whichever initiative handles chronic disease management and RPM in the state plan (Initiative I in Massachusetts)
- Outcome measurement: Chronic disease management enrollment, RPM billing capture rate, clinical outcome metrics (HbA1c reduction, BP control)
- Sustainability: Medicare RPM CPT billing (99453-99458) covers operations; no dependency on RHTP after deployment
- Timeline: 90-day implementation fits within state FY if started in Q1
Investments structured this way survive procurement review and survive evaluation. Investments that skip the structuring work fail procurement or produce poor outcomes that hurt the vendor’s position in later cycles.
Sustainability After 2030: When the Funding Ends
RHTP funding ends September 30, 2030. States are required to submit sustainability planning documentation in Year 4 (FY2029) demonstrating how funded activities will continue without federal support.
Five sustainability pathways states are planning:
- Pathway 1: Medicaid reimbursement integration: Activities that can be billed through Medicaid transition from RHTP funding to Medicaid operational funding. Chronic care management (G0511 and successor codes), RPM (CPT 99453-99458), telehealth, and care coordination all have Medicaid billing mechanisms that can replace RHTP funding.
- Pathway 2: Commercial payer contracts: Value-based payment infrastructure, care management programs, and population health platforms can be sustained through commercial payer contracts if they produce measurable outcomes that commercial payers value.
- Pathway 3: State appropriations: States that demonstrate RHTP-funded activities produce state-level savings (reduced ED visits, improved outcomes, workforce retention) can make the case for state general fund appropriations after 2030.
- Pathway 4: Federal successor programs: If RHTP demonstrates measurable impact, Congress may reauthorize or create successor programs. This is not guaranteed and cannot be assumed in sustainability planning.
- Pathway 5: Private foundation and philanthropic support: Some RHTP-funded activities align with foundation priorities (rural health equity, chronic disease management, workforce development). Foundation support can bridge funding gaps but rarely replaces federal scale.
What sustainability planning looks like in practice:
- Year 1 (FY2026): Sustainability narrative in RFPs and contracts. Vendors commit to transition paths.
- Year 2 (FY2027): Implementation. Operational data collection begins.
- Year 3 (FY2028): Mid-point evaluation. Outcome data informs sustainability pathway selection.
- Year 4 (FY2029): State sustainability plan submission to CMS. Billing code integration, payer contract negotiations, state appropriation advocacy.
- Year 5 (FY2030): Transition execution. RHTP-funded activities bridge to sustainable funding sources.
- For facilities and vendors, sustainability planning should start at Year 1, not Year 4. Investments structured with sustainability in mind from the beginning require less rework when the 2030 cliff approaches.
How Mindbowser Helps Grant Recipients Operationalize Their RHTP Plans
Mindbowser builds custom healthcare technology that aligns to RHTP statutory elements and survives state procurement review. Our work focuses on the execution layer between state plan approval and operational technology deployment.
- HealthConnect CoPilot delivers Element F provider technology (FHIR-based care coordination, EHR integration, HIE connectivity) designed for the rural deployment constraints RHTP plans explicitly address.
- WearConnect supports Element C consumer-facing technology and Element H innovation in delivery through device-agnostic RPM infrastructure that works with cellular-first connectivity rural patients require.
- AI Medical Summary reduces documentation burden by automating structured clinical note generation, coding support, and follow-up summaries. Efficiency gains should be measured during implementation rather than assumed in the RHTP application.
- PHISecure covers cybersecurity infrastructure that appears in most state RHTP plans as a cross-cutting requirement under Elements D, F, and K.
Our engagement model:
- 12-16 week MVP builds that fit within state fiscal year procurement cycles
- Scope structuring aligned to statutory elements from contract inception
- Sustainability planning built into implementation, not added in Year 4
- Operational handoff designed for 1-2 person IT teams at CAHs and small hospitals
The Rural Health Transformation Fund is a $50 billion federal pool authorized by Section 71401 of Public Law 119-21 for distribution to all 50 states over FY2026 through FY2030, at $10 billion per year. CMS administers the federal program; states administer individual allocations. The fund ends September 30, 2030 absent Congressional reauthorization.
Direct federal applications closed in November 2025. CMS awarded all 50 states on December 29, 2025. Individual hospitals, health systems, and vendors cannot apply directly for the $10 billion per year. Engagement happens through state procurement: each state runs its own RFP cycles (most between Q3 2026 and Q1 2027) for the technology, workforce, and facility investments its approved plan requires. Vendors and facilities engage through four paths: bidding on state RFPs, subcontracting through prime consulting firms, partnering with state eHealth organizations, or joining rural hospital networks that share-service across state RHTP allocations.
Technology spending touches four of the seven statutory use-of-funds elements. Element C (consumer-facing technology) covers patient engagement, RPM, digital front doors, and direct-to-patient telehealth. Element D (training and technical assistance) covers workforce and technology adoption support. Element F (provider technology) covers EHR modernization, HIE capacity, FHIR interoperability, clinical decision support, cybersecurity, and care coordination platforms. Element H (innovation in delivery) covers mobile health, hospital-at-home, and integrated specialty care. Cross-category classification is common for investments that serve multiple elements.
The exact% varies by state. Massachusetts allocates approximately 37% of its $1 billion request to the two most technology-heavy initiatives (Population Health Advancement at $291 million and Technology Interoperability at $83 million). Other states run similar or higher technology allocations. The 50-state comparison PDF details breakdowns by state and initiative.
Most states post initial RFPs between Q3 2026 and Q1 2027. Technology-specific RFPs tend to cluster in Q4 2026 and Q1 2027. Implementation contracts execute through Q2 2027. Additional RFP cycles run through Year 2 (FY2027) and into Year 3 (FY2028). The largest procurement window is Q4 2026 through Q1 2027.
Both paths exist. Direct state contracts typically go to larger vendors with state-level registration and healthcare-specific procurement experience. Prime contractor subcontracts provide path for specialized technology vendors whose capability exceeds what primes provide in-house. State eHealth organization partnerships (MeHI in Massachusetts and similar) provide additional path for innovation-focused vendors. Rural hospital network partnerships provide path for facility-level deployments coordinated across multiple hospitals.
Sustainability planning is required in Year 4 (FY2029). States must document how RHTP-funded activities will continue without federal support. Five pathways exist: Medicaid reimbursement integration, commercial payer contracts, state appropriations, federal successor programs (not guaranteed), and private foundation support. Facilities and vendors should structure investments with sustainability in mind from Year 1, not Year 4.
No. The Rural Health Transformation Fund is a CMS program authorized under the One Big Beautiful Bill Act. HRSA administers separate rural health programs including the Flex Program, SHIP, and Rural Health Clinic support. State RHTP plans sometimes reference HRSA programs or build on HRSA-funded infrastructure, but the $50 billion is CMS funding, not HRSA funding. Search queries for “HRSA Rural Health Transformation Program” typically land on the CMS program because the terminology has consolidated informally. This page references the following primary federal sources. All citations link directly to the official Federal Register, CFR, or agency record.
