



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
- Most RPM programs stall between 50 and 200 patients. The pilot worked. The outcomes data looked promising. Then enrollment plateaued, the care team hit capacity, the device logistics collapsed, and nobody could explain why the program wasn’t growing.
- The transition from pilot to enterprise is not a volume problem. It is an architecture problem: the platform, staffing model, alert management, and device logistics that work at 50 patients break at 500.
- At BRI 2026, Rachel Alfiero from MaineHealth presented their RPM scaling experience, and the pattern she described matches what we’ve seen across every program that hits the scaling wall.
We have shipped RPM platforms to organizations ranging from 25-patient pilots to programs managing thousands of concurrent patients. The technology that launches a pilot is almost never the technology that runs at enterprise scale. Not because the pilot technology is bad. Because the assumptions baked into a 50-patient program do not survive contact with 500 patients.
A pilot has one care manager who knows every patient by name. An enterprise program has a care team of 15 who manage patients by risk score. A pilot has 50 devices shipped from a closet. An enterprise program has a supply chain: procurement, shipping, patient setup, returns, replacement, and inventory tracking. A pilot has a care manager who reviews every alert. An enterprise program has AI triage or it has burnout.
Every RPM program that fails to scale fails at one of four points: platform architecture, staffing model, alert management, or device logistics. Usually two or three simultaneously.
Where Do RPM Programs Stall?
The pattern is consistent enough that we can describe it precisely.
- Phase 1 (0-50 patients): the pilot succeeds. A champion physician enrolls patients from their panel. One dedicated care manager handles all monitoring. Device setup happens in person at clinic visits. Alert thresholds are manually configured per patient. The care manager knows every patient’s name, baseline, and medication list. Outcomes are good. Leadership says “scale it.”
- Phase 2 (50-200 patients): the cracks appear. The original care manager is overwhelmed. A second care manager is hired, but they don’t know the patients as well. Device setup is still happening at clinic visits, but the volume of visits needed to enroll patients is competing with regular clinical operations. Alert volume has increased linearly with patient count, but the care team’s capacity has not. The platform starts showing limitations: reports that worked for 50 patients take too long to generate for 200. The physician champion is now spending time on program administration instead of clinical leadership.
- Phase 3 (200-500 patients): the wall. Enrollment slows or stops. The care team is at capacity. New patients cannot be onboarded because there’s nobody to do the initial device setup and threshold configuration. Alert fatigue is real (see our RPM alert fatigue guide for the full picture). Device logistics have become a full-time job that nobody was hired to do. The platform cannot handle concurrent data from 500 devices without performance issues. Leadership questions the ROI because the cost per patient has risen as operational complexity has increased.
At BRI 2026, Rachel Alfiero from MaineHealth presented their RPM scaling experience. Her timeline mapped precisely to this pattern. The insight she shared that resonated most: they refresh their RPM roadmap every six months, specifically because what works in the current phase will break in the next one. The technology, staffing, and workflows need to evolve every 6-12 months as the program doubles.
How Does Platform Architecture Need to Change at Scale?
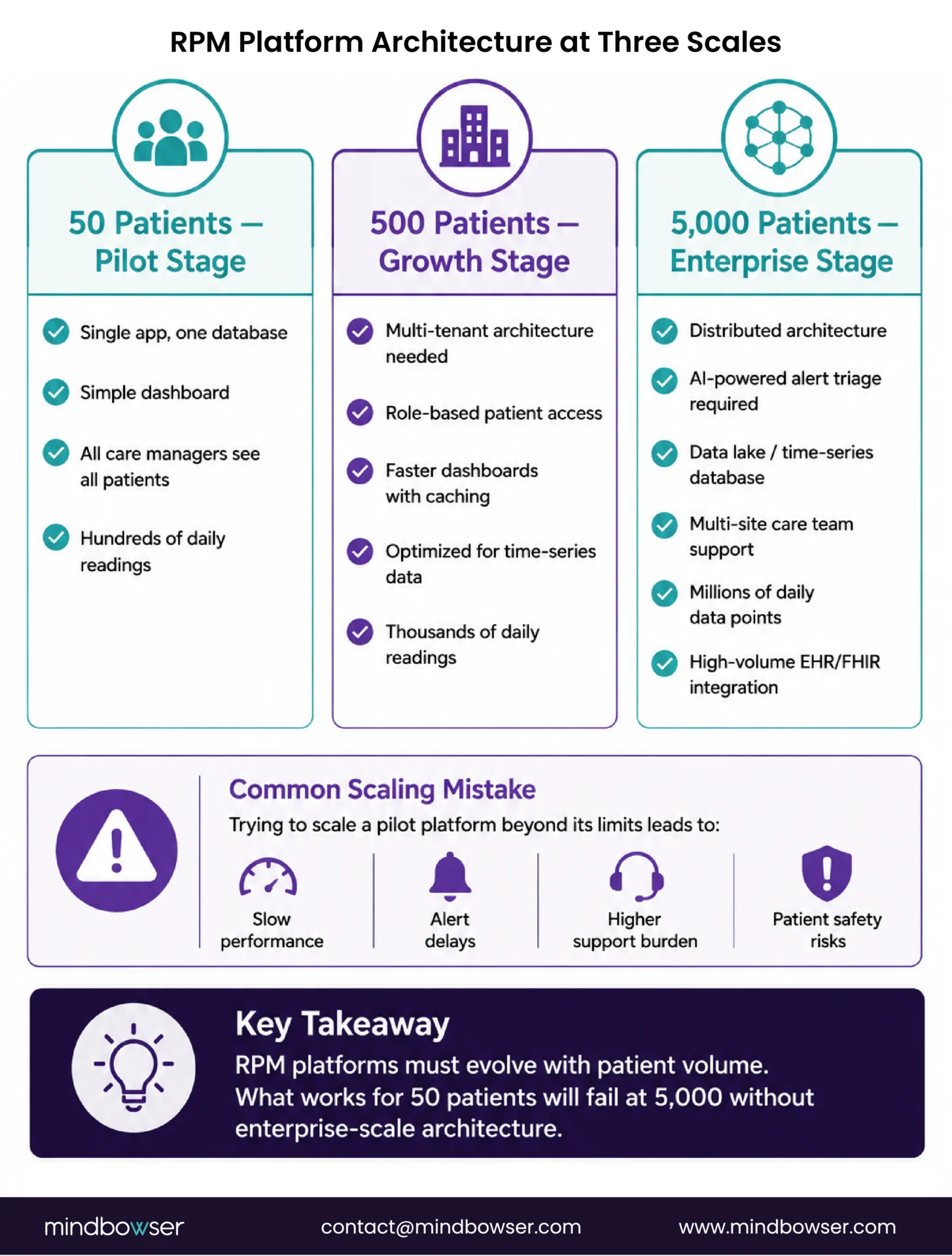
A 50-patient RPM platform and a 5,000-patient RPM platform share a name but almost nothing else architecturally.
- At 50 patients: single-instance application, one database, one dashboard. All care managers see all patients. Reports are generated in seconds. Device data ingestion is straightforward: 50 devices sending 1-3 readings per day is a few hundred data points.
- At 500 patients: multi-tenant architecture becomes necessary. Care managers need role-based panel assignments (you see your 80 patients, not all 500). Database queries must be optimized for time-series data at volume. Real-time dashboards need caching and incremental updates. Device data ingestion is 500-1,500 data points per day for intermittent monitoring, or 144,000+ per day if CGM patients are included (288 readings × 500 patients).
- At 5,000 patients: the platform must handle millions of daily data points. Alert triage is mandatory (AI-powered, as covered in our alert fatigue piece). The database is a time-series database or data lake, not a relational database optimized for transactional queries. Multi-site support means the platform serves different care teams across different geographies with different protocols. Analytics must run on aggregated data without blocking real-time dashboards. EHR integration must handle thousands of FHIR Observation writes per day without bottlenecks.
The common mistake: programs try to scale a pilot platform instead of migrating to an enterprise architecture. The pilot platform was chosen for speed to launch (which was correct). But attempting to run 500+ patients on infrastructure designed for 50 creates performance degradation, support burden, and eventually patient safety risks when alert delivery is delayed.
WearConnect scales the device integration layer across patient volumes. The normalization engine that handles 50 BLE devices handles 5,000 because the architecture was built for horizontal scaling from the start. HealthConnect CoPilot handles the EHR integration pipeline at volume.
What Staffing Model Works at Each Scale?
The staffing model is where most programs miscalculate, and the miscalculation kills growth faster than any technology limitation.
- At 50 patients: 1 care manager handles the full panel. They know every patient. They review every alert. They make every call. The ratio is 1:50, and it works because the care manager has built relationships with every patient.
- At 200 patients: 2-3 care managers, each with a panel of 65-80 patients. A program coordinator handles enrollment logistics, device shipping, and billing. The physicians spend 2-4 hours per week reviewing trend reports and signing off on care plan changes. The ratio shifts from “I know every patient” to “I manage a panel by risk priority.”
- At 500 patients: 5-7 care managers. A dedicated RPM program manager (not a care manager who also does admin). A device logistics coordinator (or outsourced logistics partner). A part-time data analyst running outcomes reports for the quality committee and payer negotiations. Care managers are now organized by condition or acuity tier, not just patient volume.
- At 1,000+ patients: care manager team of 12-15. Lead care manager per condition (cardiac, respiratory, diabetes). Program director (clinical operations). Device logistics team (2-3 people or outsourced). Quality/outcomes analyst. IT liaison for platform and EHR issues. Billing specialist for concurrent program coding (RPM + CCM + BHI). The program has become a department.
- At 5,000 patients: this is a service line. Multiple care teams across sites. Centralized command center model (similar to hospital-at-home command centers). Regional care managers with local patient panels. Centralized alert triage with AI + human escalation. Executive director reporting to the CMO or CNO. Analytics team. The operating model resembles a chronic care management company more than a clinical program.
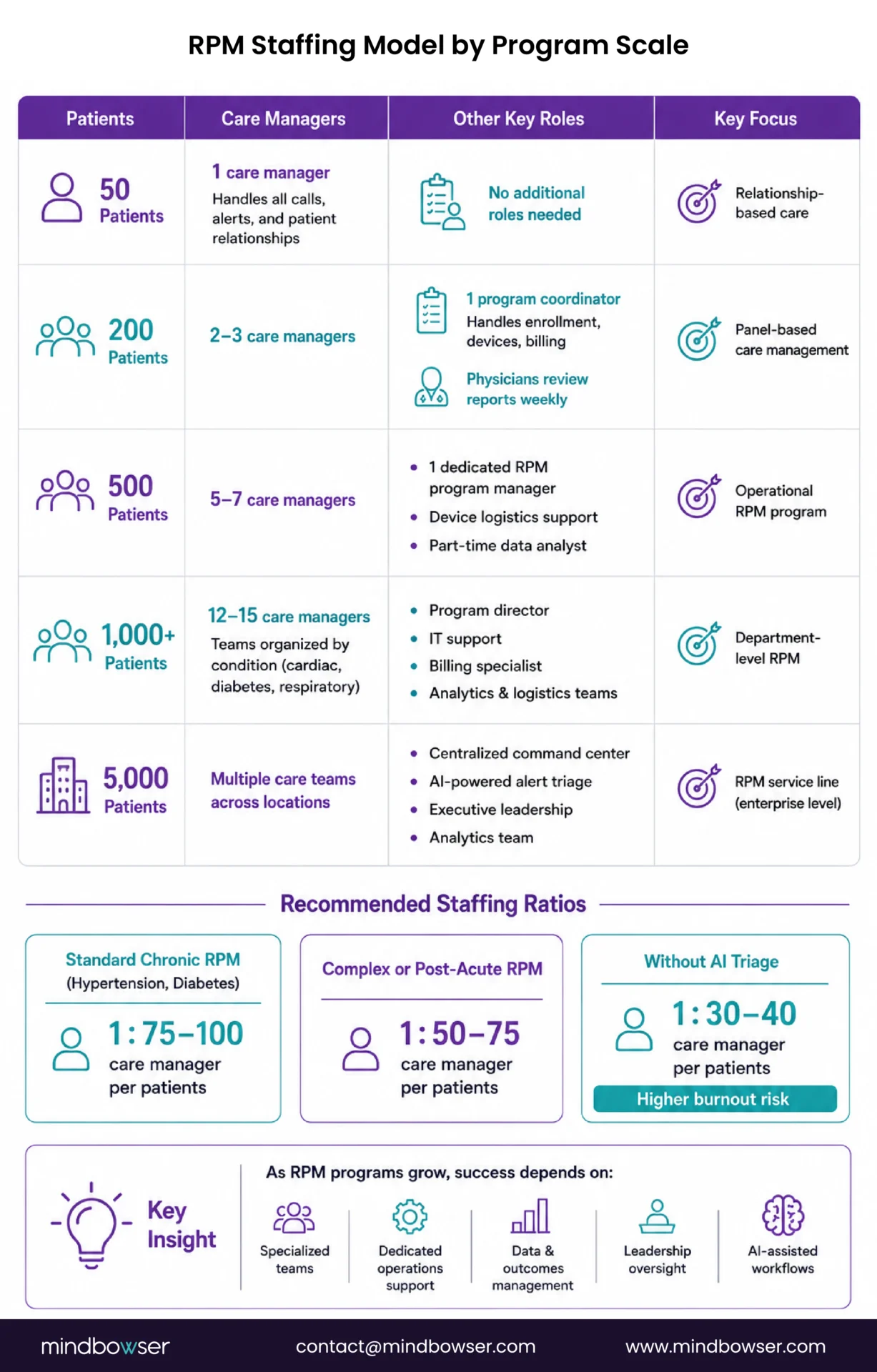
The staffing ratio that consistently works: 1 care manager per 75-100 patients for standard chronic RPM (hypertension, diabetes). 1 per 50-75 for complex multi-condition or post-acute patients. These ratios assume AI-powered alert triage is in place. Without AI triage, the ratio drops to 1 per 30-40 before burnout sets in.
Build a Roadmap to Scale Your RPM Program Beyond 200 Patients
How Do You Solve Device Logistics at Scale?
Device logistics is the operational problem nobody budgets for, and everybody hits by month six.
- At 50 patients: devices are stored in a closet. A care manager hands the patient a device at the clinic visit, shows them how to use it, and verifies that the reading appears on the dashboard. Returns come back at the next visit. This works. It is not scalable.
- At 200 patients: the closet is now a storage room. Devices need to be shipped to patients who cannot come to the clinic. Shipping means packaging, tracking numbers, delivery confirmation, and a setup call because nobody is there to demonstrate in person. Returns need prepaid shipping labels and a process for receiving, inspecting, wiping, and redeploying returned devices. The care manager who was handing out devices is now spending 30% of their time on logistics.
- At 500+ patients: device logistics is its own operation. Procurement cycles (ordering 100 devices at a time, not 10). Inventory management (which devices are deployed, which are in stock, which are returned pending inspection). Patient-facing setup guides (print or video). A shipping partner or in-house logistics coordinator. Battery replacement tracking (cellular devices have 6-18 month battery life). End-of-life device replacement. Lost or damaged device replacement protocol. For the cellular vs BLE tradeoff that drives device selection before you hit these logistics, see our RPM device comparison guide.
- At 1,000+ patients: outsource or automate. A dedicated logistics partner handles procurement, kitting (device + instructions + return label in one box), shipping, tracking, returns, and inventory. The clinical team should never touch device logistics at this scale. Every minute a care manager spends on shipping is a minute not spent on patient care.
The cost that surprises every program: device loss and replacement. Patients lose devices, break devices, and forget to return devices. At 50 patients, this is 2-3 devices per year. At 1,000 patients, it is 50-80 devices per year. Budget 5-8% annual device replacement rate into program economics.
When Does AI Alert Triage Become Mandatory?
At 200 patients. That is the threshold where static threshold alerts overwhelm a human care team regardless of staffing.
The math: 200 patients generating an average of 2 alerts per day (conservative for static threshold programs) is 400 alerts daily. At 90 seconds per alert review, that is 10 hours of triage per day. A care manager working 8 hours cannot triage all alerts AND make patient calls, document interactions, and update care plans. Something gives. Usually, it is an alert review quality.
AI triage (covered in detail in our RPM alert fatigue piece) converts 400 undifferentiated alerts into 30-40 actionable items by learning individual patient baselines and applying composite risk scoring. The care manager’s day shifts from “process 400 alerts, find the 20 that matter” to “review 35 pre-prioritized items, act on the ones that need intervention.”
RPMCheck AI provides this triage layer. At scale, it is not optional. It is the staffing multiplier that makes the care manager ratios in the previous section possible. Without AI triage, you need 1 care manager per 30-40 patients. With it, you need 1 per 75-100. At 1,000 patients, that is the difference between 25 care managers and 12. The salary savings alone justify the AI investment within the first quarter.
Rachel Alfiero’s BRI 2026 presentation on MaineHealth’s scaling experience specifically addressed this transition. The inflection point in their program was deploying intelligent triage. Before that, scaling was linear (more patients = proportionally more staff). After that, scaling became logarithmic (more patients, incrementally more staff).
What Does the Financial Model Look Like at Scale?
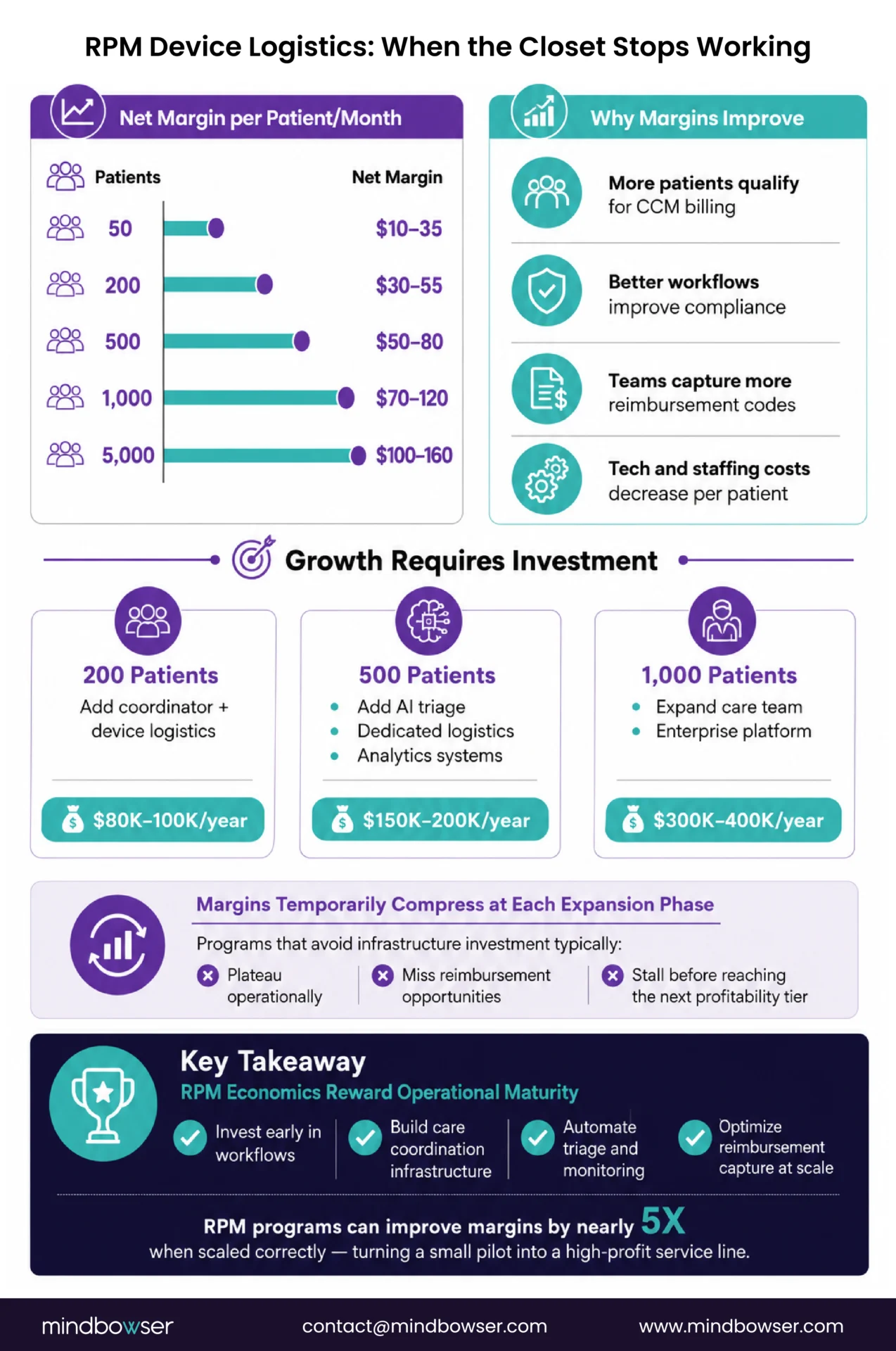
The economics of RPM programs improve with scale, but the improvement is not linear. There are cost step-functions at each growth phase.
| Scale | Revenue/Pt/Mo | Staff Cost/Pt/Mo | Tech Cost/Pt/Mo | Device Cost/Pt/Mo | Net Margin/Pt/Mo |
|---|---|---|---|---|---|
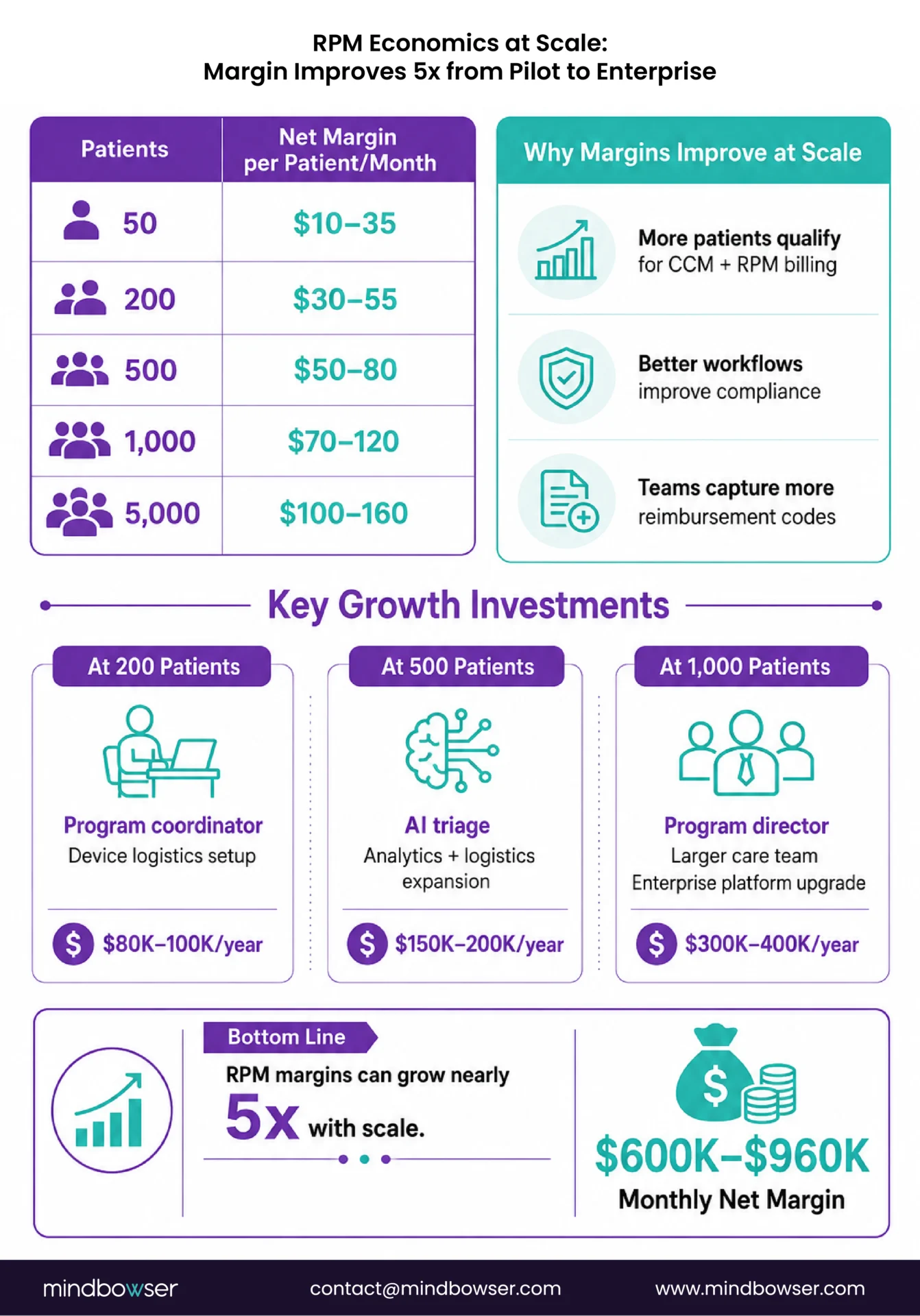
| 50 pts | $105-122 | $40-60 | $15-25 | $8-12 | $10-35 |
| 200 pts | $105-122 | $25-40 | $10-18 | $6-10 | $30-55 |
| 500 pts | $120-150* | $18-28 | $8-14 | $5-8 | $50-80 |
| 1,000 pts | $140-180* | $14-22 | $6-10 | $4-7 | $70-120 |
| 5,000 pts | $160-220* | $10-16 | $4-8 | $3-5 | $100-160 |
*Revenue increases at scale because: higher percentage of patients on concurrent CCM (stacking), more patients hitting the 16-day monitoring threshold (better compliance with established workflows), and additional time codes captured (99458) as care manager workflows become more efficient.
The margin improvement from 50 to 5,000 patients is roughly 5x. The program goes from a $10-35 per patient per month margin to $100-160. Run your own program’s numbers scale tier by scale tier in our RPM ROI calculator. That is the difference between a pilot that barely justifies its existence and a service line generating $600K-$960K in monthly net margin.
The cost step-functions to budget for:
- 200 patients: hire program coordinator + invest in device logistics (~$80K-100K/year)
- 500 patients: deploy AI triage + dedicated logistics + analytics (~$150K-200K/year)
- 1,000 patients: program director + expanded care team + enterprise platform migration (~$300K-400K/year)
Each step-function temporarily compresses margins before the next scale tier makes it back. Programs that try to avoid the step-function investment stall at the previous tier.
What Is the 12-Month Scaling Roadmap?
This roadmap assumes a program currently at 50-100 patients that has proven clinical outcomes and has leadership support to scale.
Months 1-3: Foundation for Scale
- Audit current platform: can it handle 500 patients without performance degradation? If not, plan the migration now
- Hire or assign a program coordinator (non-clinical, handles enrollment, logistics, billing)
- Implement AI-powered alert triage. Do this before scaling enrollment. Adding patients to a program with alert fatigue makes the problem worse, not better
- Standardize device setup: create kitting process, ship-to-patient workflow, video setup guide, day-3 follow-up call protocol
- Identify CCM stacking candidates across the current RPM panel (see our RPM + CCM stacking guide)
Months 4-6: Controlled Growth
- Scale enrollment to 200-300 patients. Add 30-50 patients per month, not 100 overnight. Controlled growth lets you catch operational problems before they compound
- Hire additional care managers to maintain 1:75-100 ratio (with AI triage in place)
- Establish device logistics process: procurement, inventory, shipping, returns. Track device utilization and loss rates
- Begin condition-based panel segmentation (cardiac care managers, respiratory, diabetes) instead of geographic or alphabetical assignment
Months 7-9: Operational Maturity
- Scale to 400-600 patients
- Deploy multi-site enrollment if the system spans locations
- Implement enterprise reporting: outcomes dashboards for the quality committee, financial performance for CFO, clinical metrics for the CMO
- Evaluate platform migration if pilot platform is hitting limits
- Alfiero’s MaineHealth principle: refresh the roadmap at month 6. What worked for 200 patients will not work for 600
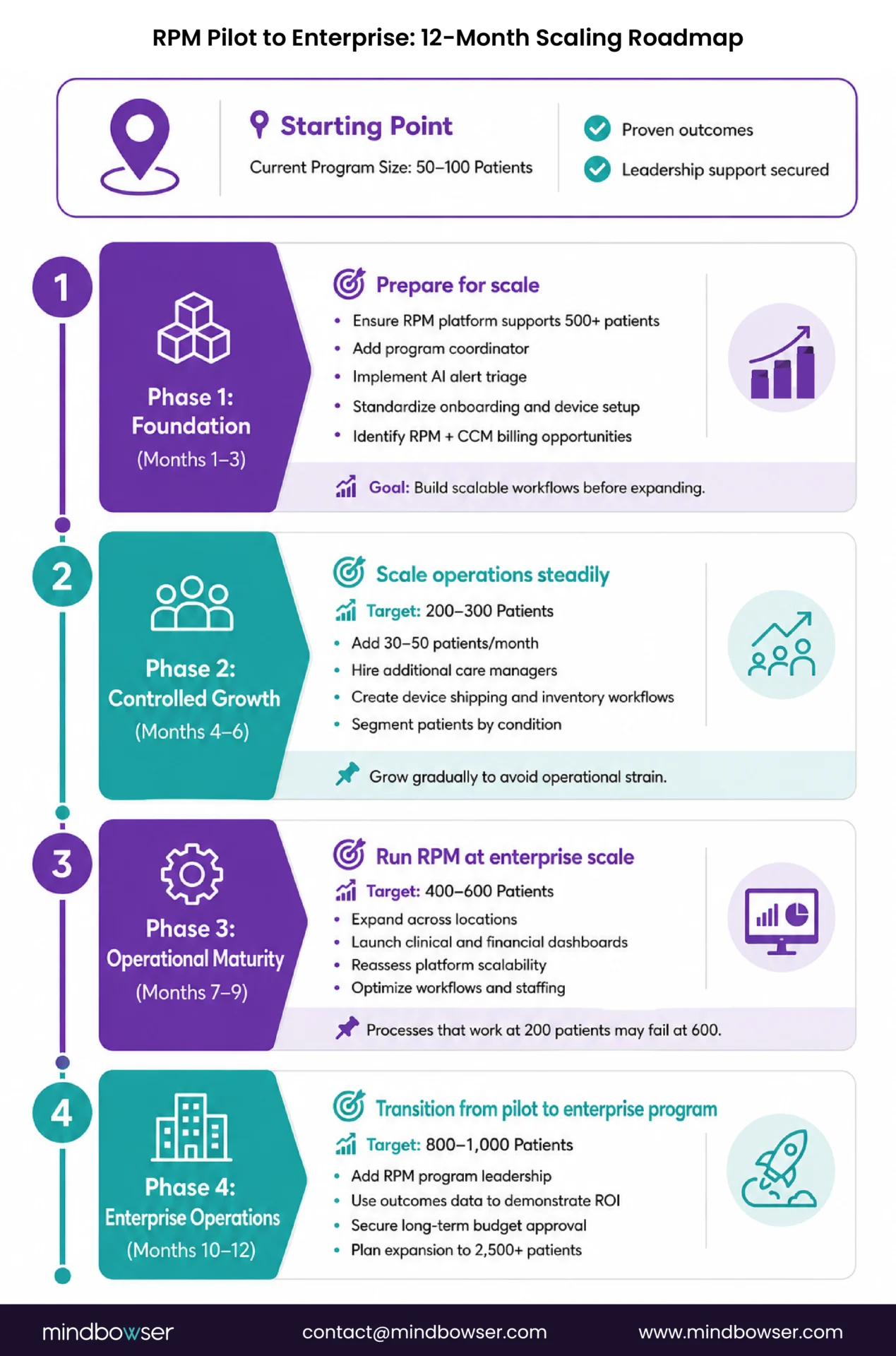
Months 10-12: Enterprise Operations
- Scale toward 800-1,000 patients
- Program director in place (if not already)
- Outcomes data should now show 6+ months of longitudinal results for the earliest enrolled patients
- Present outcomes + financial data to leadership for multi-year budget commitment
- Plan Phase 2 scaling: 1,000 to 2,500 to 5,000 over the following 12-18 months
The Architecture Decides Whether You Scale or Stall
Every RPM program that I have watched stall at 200 patients had the same root cause: the operational architecture designed for the pilot was asked to run at enterprise scale. The platform that worked at 50 patients choked at 500. The care manager who knew every patient by name burned out at 150. The device closet became a logistics nightmare at 200. The alert queue that was manageable at 75 became impossible at 300.
Scaling is not enrolling more patients. Scaling is rebuilding the operating model at each growth tier so that more patients improves the economics instead of degrading the experience.
Rachel Alfiero’s BRI 2026 insight applies to every program: refresh the roadmap every six months. The technology, staffing, and workflows that work today will break at twice the current patient count. Plan for the break before it happens, not after.
Actually, let me refine that. The programs that scale successfully don’t just plan for the break. They invest ahead of it. They hire the program coordinator at 150 patients, not at 300 when the care managers are already drowning. They deploy AI triage at 175 patients, not at 400 when alert fatigue has already caused a missed deterioration. They start the platform migration conversation at 200, not at 500 when the dashboard takes 30 seconds to load.
Investing one phase ahead is the single most predictive behavior of RPM programs that reach enterprise scale.
If your program is between 50 and 200 patients and you can feel the wall approaching, reach out. The scaling architecture is a solvable problem, and the conversation is shorter than you would expect because the pattern is consistent.
Most programs hit the scaling wall between 150 and 250 patients. The pilot worked at 50, but the staffing model, alert management, device logistics, and platform architecture designed for the pilot break at 3-5x the original volume. The stall is not a volume problem. It is an architecture problem: the operating model needs to evolve at each growth tier.
With AI-powered alert triage in place: 1 care manager per 75-100 patients for standard chronic conditions (hypertension, diabetes) and 1 per 50-75 for complex multi-condition or post-acute patients. Without AI triage, the ratio drops to 1 per 30-40 before burnout occurs. At 1,000 patients with AI triage, you need approximately 12-15 care managers. Without AI triage, you would need 25-33.
At 200 patients or earlier. Two hundred patients on static threshold alerts generate approximately 400 alerts per day, which exceeds the capacity of a care team to triage manually while also conducting patient interactions and documentation. AI triage should be deployed before scaling enrollment beyond the pilot phase, not after alert fatigue has already damaged the care team’s trust in the system.
At 50 patients, devices are handed out at clinic visits. At 200+, devices must be shipped, tracked, and returned. At 500+, device logistics becomes a dedicated operation: procurement cycles, inventory management, kitting (device + instructions + return label), shipping coordination, return processing, battery tracking, and end-of-life replacement. Budget 5-8% annual device replacement for loss and damage. At 1,000+ patients, most programs outsource logistics to a fulfillment partner.
Net margin per patient improves approximately 5x from pilot to enterprise. At 50 patients: $10-35/patient/month margin. At 500: $50-80. At 5,000: $100-160. The improvement comes from: lower per-patient staffing cost (AI triage enables higher care manager ratios), lower per-patient technology cost (platform cost amortized across more patients), higher revenue capture (more patients hitting billing thresholds, more concurrent CCM stacking), and lower per-patient device cost (volume procurement discounts).
Major architectural changes: multi-tenant design with role-based panel assignments, time-series database optimization for high-volume device data, cached real-time dashboards, AI-powered alert triage, multi-site support, streaming data ingestion (not batch), and EHR integration capable of handling thousands of FHIR Observation writes per day. Most pilot platforms cannot be retrofitted for this. The migration to enterprise architecture should be planned at 200 patients and executed before reaching 500.


