



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
- CDC 2024 data recorded 649 maternal deaths in the United States, a rate of 17.9 per 100,000 live births. Hypertension-related disorders account for approximately 7.4% of pregnancy-related deaths.
- More than half of those deaths occur in the postpartum period. A 2025 systematic review of 18 studies found remote blood pressure monitoring during pregnancy reduces hospital admissions without increasing adverse outcomes (IJG&O, 2025). RPM for gestational diabetes achieves glycemic control faster (3.3 vs 4.1 weeks), with lower preeclampsia rates and lower neonatal hypoglycemia in the AJOG study.
- UHC still covers pregnancy hypertension for RPM in 2026. The monitoring protocol is straightforward. The gap between OB visits is where deterioration happens undetected.
Six hundred forty-nine women died of maternal causes in the United States in 2024, and hypertension-related disorders accounted for roughly 7.4% of those deaths. The maternal mortality rate, 17.9 per 100,000 live births, has barely moved.
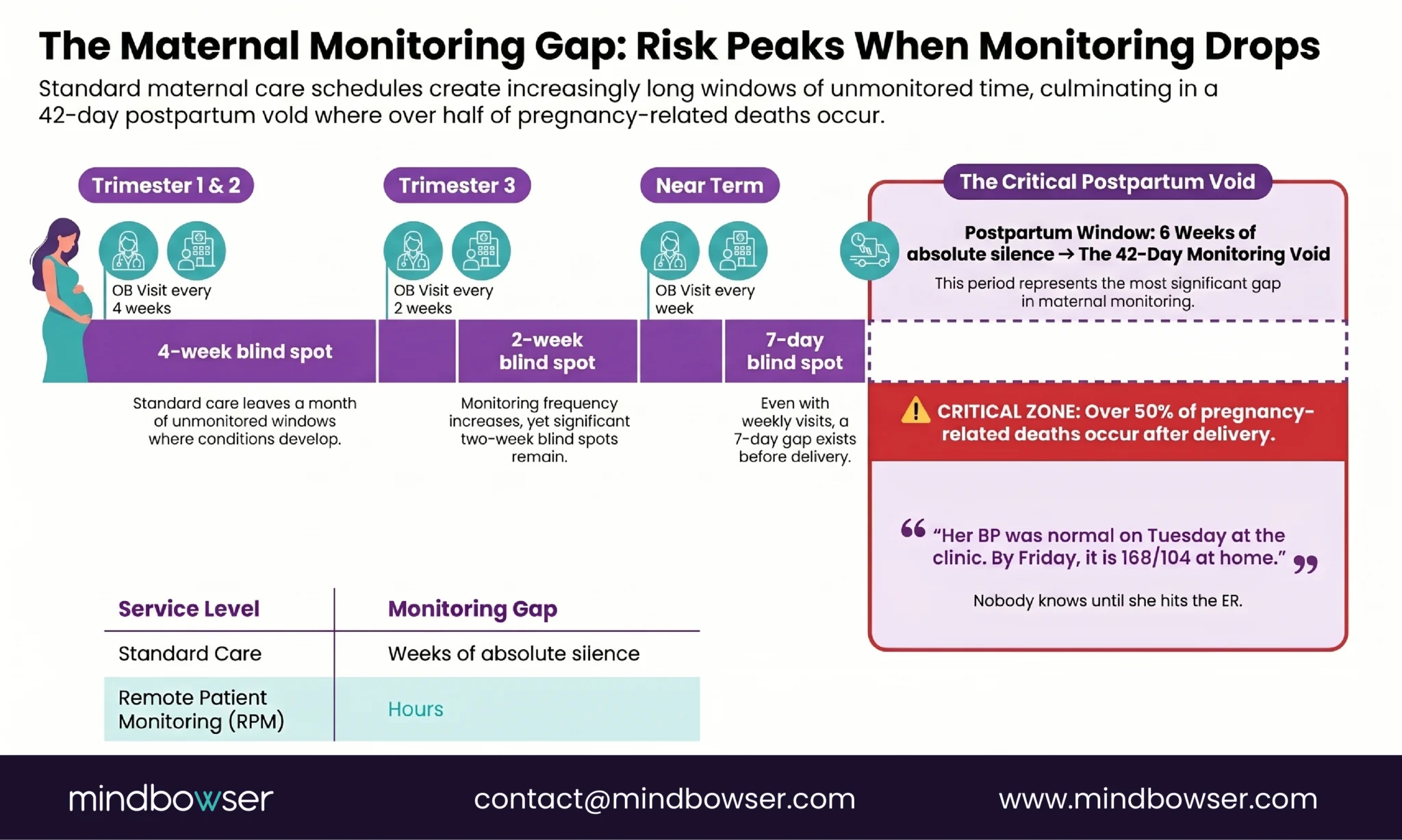
I keep coming back to a specific clinical reality when I think about these numbers. A pregnant patient sees her OB every four weeks in the first and second trimesters, every two weeks in the third trimester, and weekly near term. Her blood pressure is normal on Tuesday at the OB visit. By Friday, she has a headache, her feet are swollen, and her BP is 168/104. But nobody knows until the next visit, or until she shows up in the emergency department.
That three-day gap is where preeclampsia develops undetected. It is not a failure of clinical care. The care at each visit is appropriate. It is a failure of monitoring frequency. A condition that can kill within days is checked every 14 to 28 days.
Remote monitoring closes that gap. A cellular blood pressure cuff transmitting twice daily readings to the OB team means the Friday spike is caught on Friday, not at the next Tuesday appointment. The technology is a $200 device. The clinical protocol is well-established. The barrier was never technological.
Why Does Maternal Health Need Remote Monitoring?
The numbers establish the urgency.
The CDC reports 649 maternal deaths in 2024, a rate of 17.9 per 100,000 live births. This rate has not significantly improved from 18.6 in 2023. The United States has the highest maternal mortality rate among developed nations.
Hypertensive disorders of pregnancy (preeclampsia, eclampsia, chronic hypertension in pregnancy, gestational hypertension) account for approximately 7.4% of the nearly 800 pregnancy-related deaths that occur each year. Preeclampsia alone affects 5-8% of all pregnancies.
The detail that should change how we think about monitoring: more than 50% of pregnancy-related deaths occur during the postpartum period (AHA). After the delivery. After the patient has left the hospital. After the clinical team has shifted attention to the newborn. The mother is at her highest mortality risk at the exact moment when clinical monitoring is at its lowest intensity.
The standard postpartum follow-up is one visit at six weeks after delivery. Six weeks. A patient who had preeclampsia during pregnancy, whose BP was managed aggressively until delivery, goes home and has one clinical touchpoint over the next 42 days. During which her risk of hypertensive crisis, stroke, and death is at its peak.
Remote monitoring is not a convenience for maternal health. It is a safety intervention.
What Does Preeclampsia Remote Monitoring Look Like?
Preeclampsia monitoring is the simplest and most impactful application of RPM in maternal health.
The protocol:
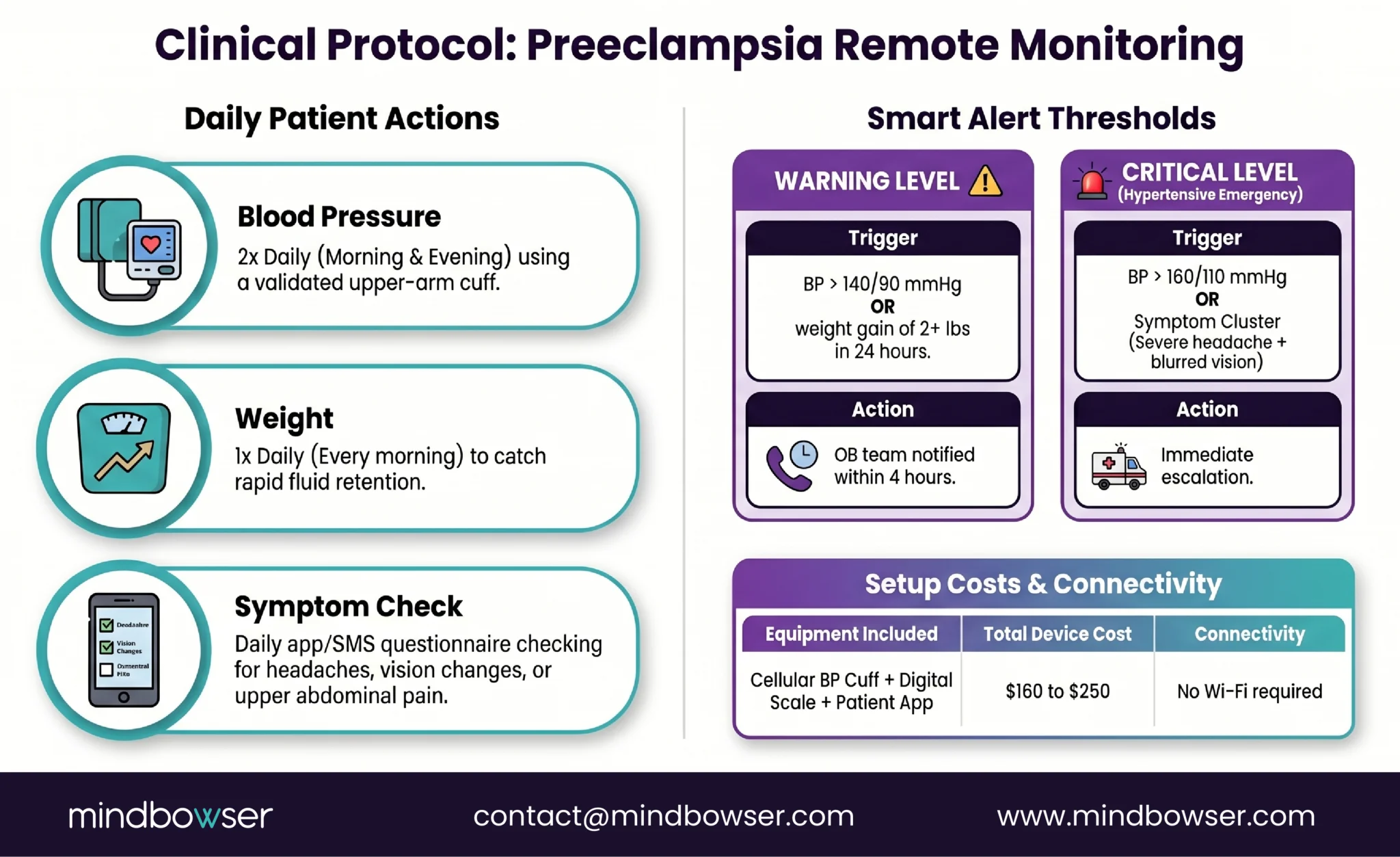
- Blood pressure: twice daily (morning and evening). The patient takes a reading using a validated upper-arm cuff, and the data transmits to the OB team’s monitoring platform
- Weight: daily. Sudden weight gain (2+ pounds in 24 hours or 5+ pounds in a week) signals fluid retention, one of the earliest warning signs of preeclampsia worsening
- Symptom questionnaire: daily check for headache (especially frontal or occipital), visual changes (blurring, scotomata, photophobia), upper abdominal pain (right upper quadrant, indicating liver involvement), and facial or hand edema
Alert thresholds:
- BP above 140/90 mmHg: warning. OB team notified within 4 hours. May trigger additional monitoring or an interim appointment
- BP above 160/110 mmHg: critical. Immediate escalation to the on-call OB provider. This is a hypertensive emergency in pregnancy
- Sudden weight gain (2+ lbs in 24 hours): warning. Assess for edema progression and proteinuria at next contact
- Symptom cluster (headache + visual changes): critical. Same-day evaluation regardless of BP reading
- Devices: cellular BP cuff ($80-120) plus connected weight scale ($80-120) plus a symptom questionnaire delivered through a patient app or automated text/IVR. Total device cost per patient: $160-250. For patients without smartphones, cellular devices eliminate the technology barrier.
- The evidence: A 2025 systematic review analyzing 18 studies found that antenatal remote blood pressure monitoring reduces outpatient visits and hospital admissions for hypertension without increasing adverse maternal or fetal outcomes. No increase in cesarean deliveries, no increase in induction for hypertension, no increase in NICU admissions. The monitoring reduces healthcare utilization while maintaining safety.
- Postpartum continuation. This is the part most programs miss. More than 50% of pregnancy-related deaths occur postpartum. The AHA published 2024 data on cell-enabled remote blood pressure monitoring during the postpartum period at a safety-net hospital, demonstrating feasibility in an underserved population. Remote BP monitoring should continue for 6-12 weeks postpartum for any patient who had a hypertensive disorder during pregnancy.
What Does Gestational Diabetes Remote Monitoring Look Like?
The evidence for RPM in gestational diabetes is the strongest of any maternal RPM application.
The American Journal of Obstetrics and Gynecology published a study comparing RPM to traditional paper-based glucose monitoring in pregnant patients with diabetes. The results were not marginal.
RPM patients submitted more glucose values (177 vs 146 over the monitoring period). They achieved glycemic control in target range at a higher rate (79.2% vs 52.0%). They achieved target range sooner (median 3.3 weeks vs 4.1 weeks). And the downstream clinical outcomes reflected it: preeclampsia rates were lower (5.8% vs 15.0%, p=.0006), and neonatal hypoglycemia in the first 24 hours was lower (29.8% vs 51.7%, p<.0001).
Those are not small effect sizes. The preeclampsia rate dropped by nearly two-thirds. Neonatal hypoglycemia dropped by nearly half. From the same clinical team managing the same patient population, with the only variable being how glucose data reached the providers.
Monitoring protocol:
- Glucose: CGM (Dexcom G7 or Abbott Libre 3) provides continuous data with targets of fasting below 95 mg/dL, 1-hour postprandial below 140 mg/dL, and 2-hour postprandial below 120 mg/dL. For patients not on CGM: 4x daily finger sticks (fasting + post-meal at each main meal) transmitted through a cellular or BLE glucose meter
- Blood pressure: twice daily. Gestational diabetes patients have elevated preeclampsia risk (the AJOG study confirmed this correlation). BP monitoring is not optional for GDM patients
- Weight: weekly (less frequent than preeclampsia monitoring because the primary concern is glucose, not fluid retention)
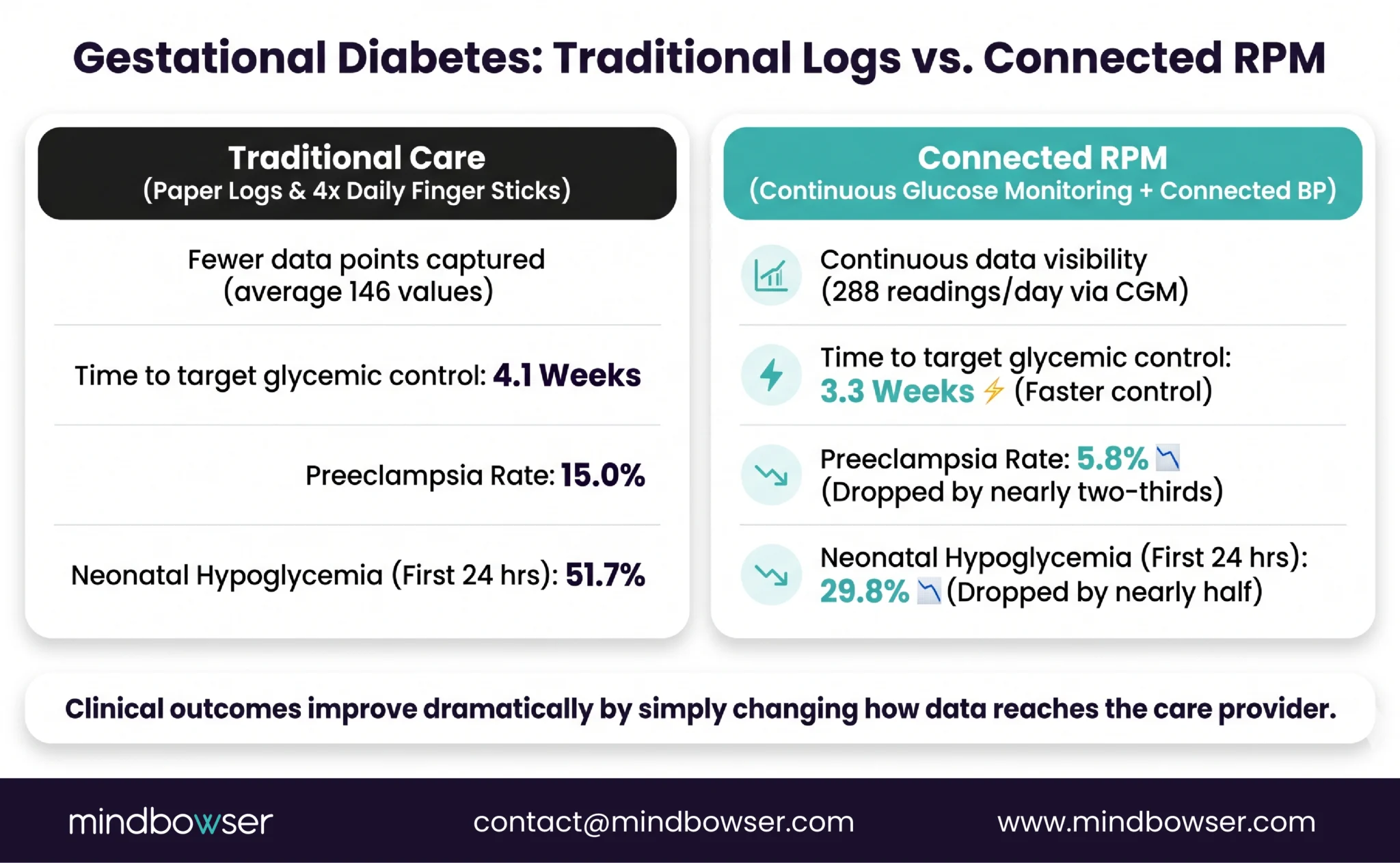
CGM advantage in pregnancy: four daily finger sticks capture four data points. CGM captures 288 per day (Dexcom G7). Postprandial glucose spikes that resolve within 90 minutes are invisible to finger sticks taken at the 1-hour or 2-hour mark. CGM catches them. The ADA published expert perspectives on CGM clinical evidence in pregnant patients in 2025, supporting expanded CGM use in pregnancy.
Build a Combined Preeclampsia + Gestational Diabetes Monitoring Platform for Your OB Department
What Is the Payer Coverage for Maternal RPM?
The payer coverage for maternal RPM is more favorable than for any other RPM condition in 2026.
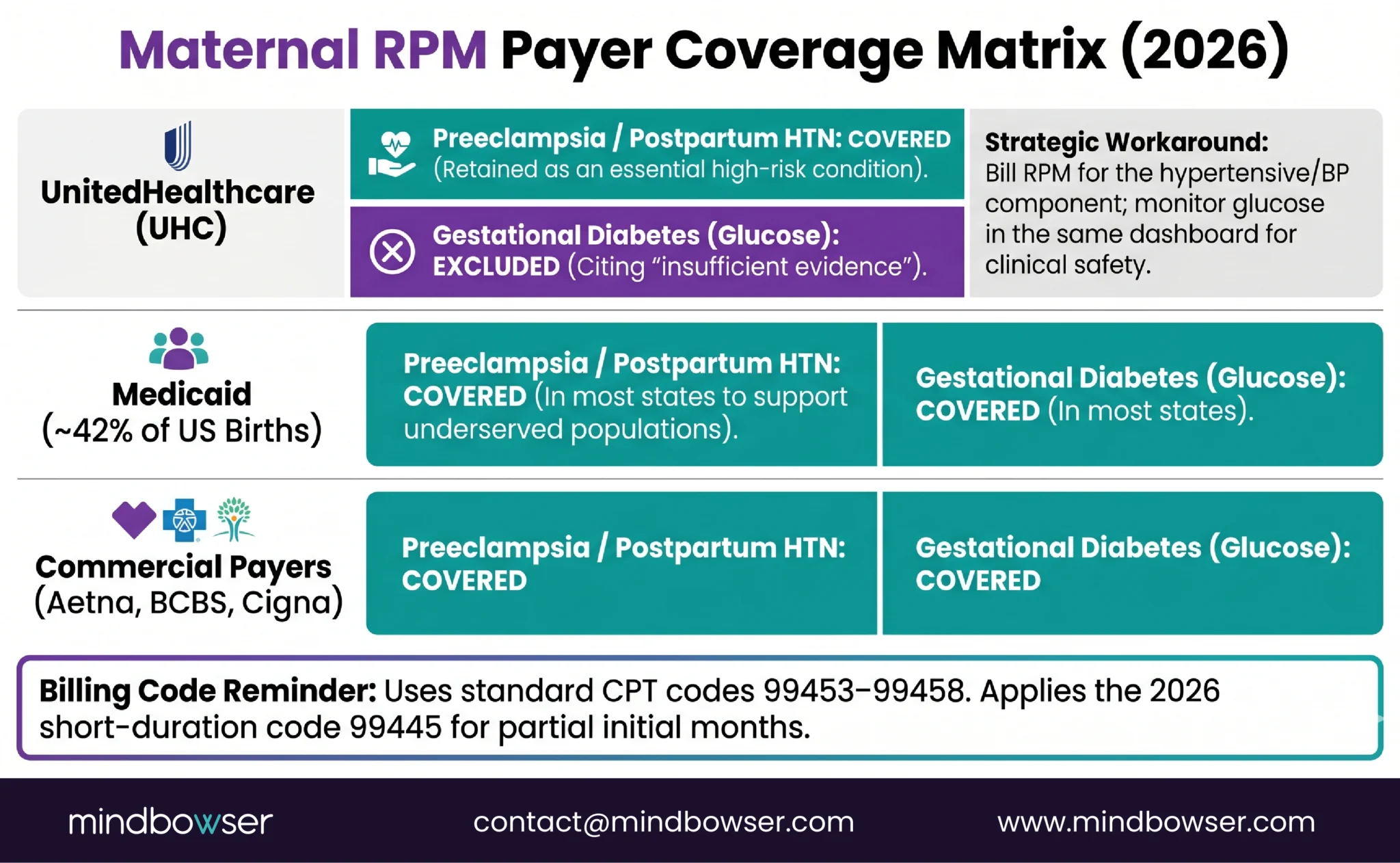
- UnitedHealthcare. “Hypertensive disorders during pregnancy” is one of only two conditions UHC covers for RPM (the other is heart failure). While UHC excluded chronic hypertension, diabetes, and COPD, pregnancy hypertension was retained. For maternal health programs, this is the green-light RPM use case under the most restrictive major payer.
- Medicaid. This is the payer that matters most. Medicaid covers approximately 42% of births in the United States. Most state Medicaid programs cover RPM for pregnancy. For health systems serving Medicaid populations (safety-net hospitals, FQHCs), maternal RPM is reimbursable for the largest portion of their obstetric patients.
- Commercial payers (Aetna, BCBS, Cigna). Generally covers pregnancy RPM. Verify specific plan coverage, but the category is broadly supported.
- Medicare. Largely irrelevant for maternal RPM (very few pregnant patients are on Medicare).
- The gestational diabetes caveat. UHC explicitly excludes gestational diabetes from RPM coverage, citing “insufficient evidence.” This is despite the AJOG data showing preeclampsia rates dropping from 15.0% to 5.8% with RPM. The exclusion is specific to RPM billing for GDM glucose monitoring under UHC plans. BP monitoring for a patient who has BOTH gestational diabetes AND pregnancy hypertension is still covered under the hypertensive disorder designation. The billing approach: bill RPM for the hypertensive monitoring (covered), manage glucose monitoring within the same program (clinical benefit without separate RPM billing for the glucose component).
- Billing codes: same CPT 99453-99458 as all RPM. No pregnancy-specific codes. The 2026 short-duration code 99445 applies, lowering the monitoring minimum for newly enrolled patients who may not hit 16 days in their first month.
What Are the Implementation Challenges?
A 2025 PMC study surveying obstetricians about their RPM experiences identified real-world barriers that differ from chronic disease RPM challenges.
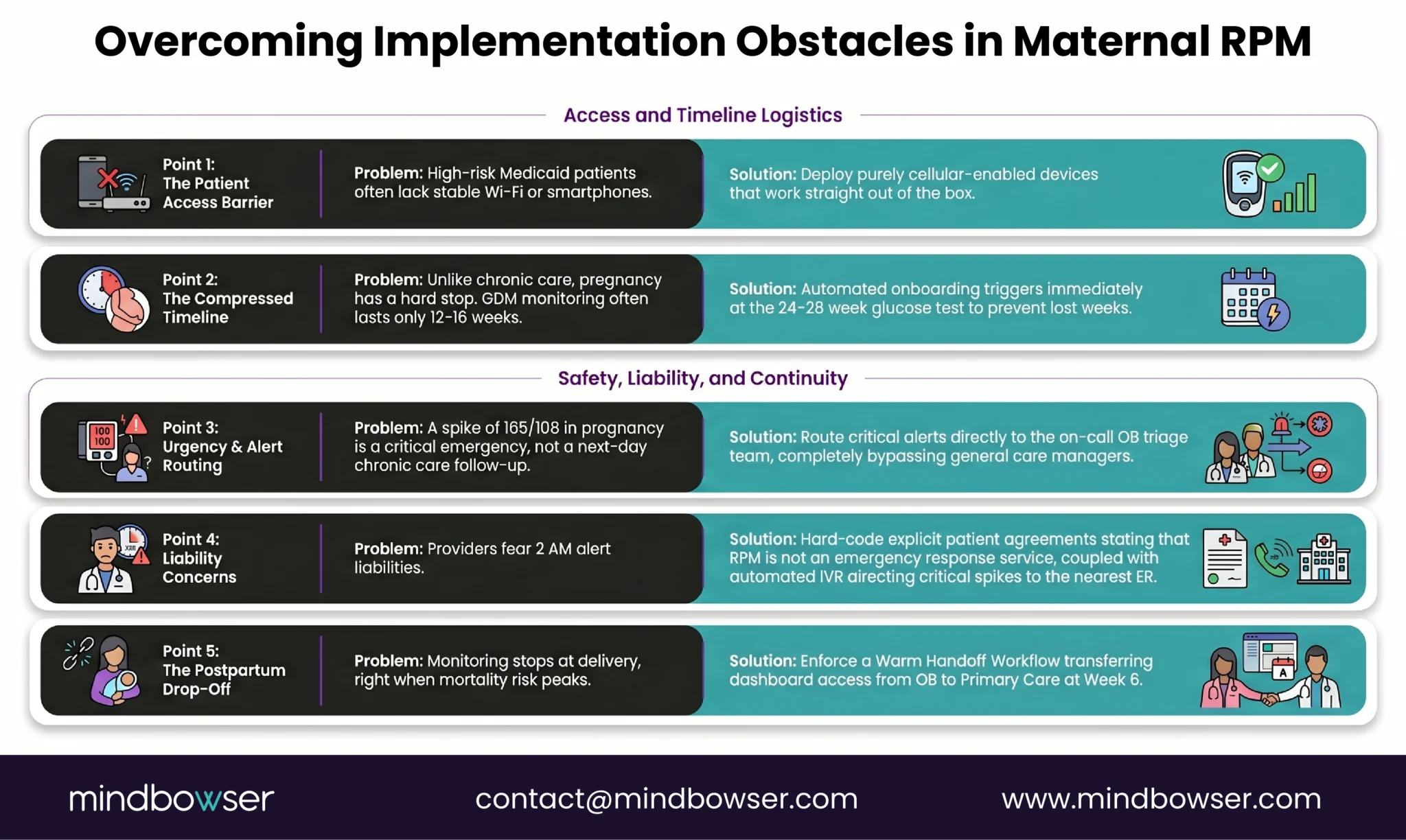
- Patient access. Many high-risk maternal patients, particularly those on Medicaid, lack smartphones or stable internet access. Cellular devices are not a preference for this population; they are a requirement. The AHA’s safety-net hospital study specifically used cell-enabled devices to address this barrier.
- Compressed timeline. Chronic RPM programs have months or years to establish workflows. Pregnancy RPM has 6-9 months from enrollment to delivery, and gestational diabetes typically isn’t diagnosed until the glucose tolerance test at 24-28 weeks, leaving only 12-16 weeks of monitoring. Every week of enrollment delay is a week of lost monitoring.
- Workflow integration. OB practices operate differently from chronic care management programs. RPM alerts need to reach the OB provider or on-call team, not a chronic care manager. Escalation pathways must account for OB-specific urgency: a BP of 165/108 in a pregnant patient requires faster response (minutes to hours) than the same reading in a chronic hypertension patient (hours to next day). The alert routing must know the patient is pregnant.
- Postpartum handoff. When the patient delivers, who continues the monitoring? The OB team typically manages for 6 weeks postpartum, then transitions to the PCP. This handoff is where monitoring most commonly drops off, which is precisely when maternal mortality risk is highest. The platform must support the handoff: OB team view for weeks 1-6, PCP view from week 6 onward, with no gap in between.
- Liability concerns. Obstetricians report uncertainty about liability when a patient transmits a concerning BP reading at 2 AM. The RPM program’s escalation protocol must define who receives the alert, what the expected response time is, and how after-hours coverage works. Ambiguity in the escalation pathway is a liability risk.
How Do You Build a Maternal RPM Platform?
Off-the-shelf RPM platforms (SmartMeter, Tenovi, Babyscripts) offer pregnancy monitoring modules that handle basic BP and weight data collection for single-condition preeclampsia monitoring.
Custom build adds value when the program needs:
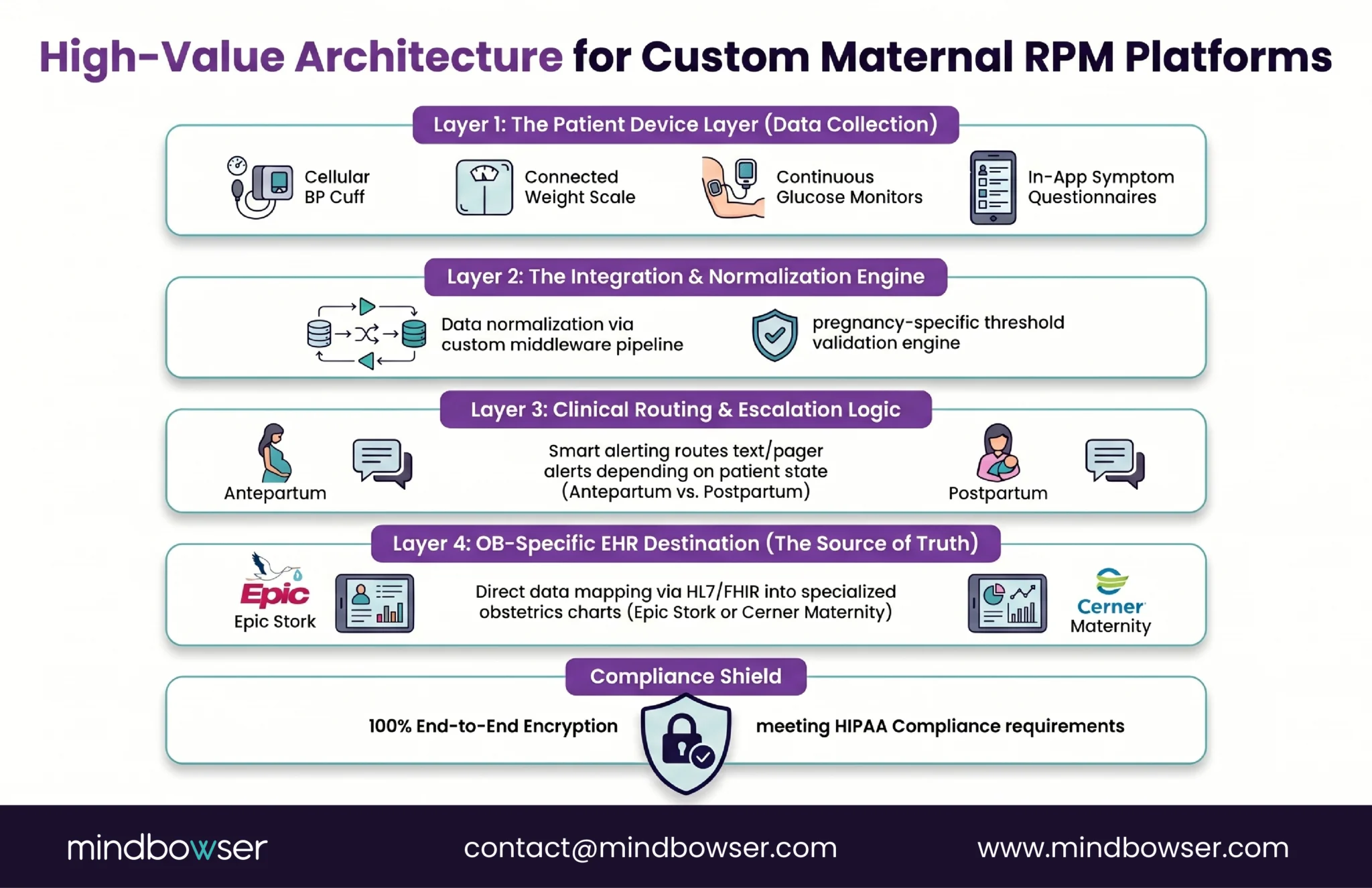
- Combined preeclampsia + gestational diabetes monitoring. A patient with both conditions needs BP data plus continuous glucose data flowing into one clinical view with pregnancy-specific thresholds (glucose targets are different in pregnancy than in Type 2 diabetes). Most off-the-shelf platforms handle BP OR glucose, not both in a unified pregnancy-specific view.
- Postpartum transition workflows. The monitoring doesn’t end at delivery. The platform must support the shift from antepartum monitoring (OB team, pregnancy thresholds) to postpartum monitoring (potentially different team, different thresholds, different escalation). This transition logic is rarely built into generic RPM platforms.
- OB-specific EHR integration. Epic Stork, Cerner Maternity, and other OB-specific modules have different data flows than general medicine EHR modules. RPM vital signs landing in the wrong section of the OB chart (general vitals instead of the antepartum record) creates clinical confusion. ConnectHealth handles EHR mapping, but OB-specific routing requires configuration.
- CGM integration for gestational diabetes. The Dexcom/Abbott CGM data pipeline described in our diabetes RPM guide applies directly. Continuous glucose data flowing through the same platform as BP data, with pregnancy-specific glucose targets and OB-specific alert routing.
Because maternal RPM data includes BP, glucose, weight, symptoms, and postpartum handoff details, the platform should follow RPM-specific HIPAA controls for device data, cloud storage, access controls, audit logs, and EHR transfer.
The platform architecture we built for a digital health client (CGM + BP + weight + activity data in a unified view) is directly applicable. Replace the wellness context with pregnancy clinical thresholds, add OB-specific escalation pathways, and the multi-device normalization pipeline is the same.
What About Postpartum Monitoring?
This section exists because postpartum monitoring is where most maternal RPM programs end, and where most maternal deaths occur.
More than 50% of pregnancy-related deaths happen after delivery. The American Heart Association published 2024 data on cell-enabled remote blood pressure monitoring during the postpartum period at a safety-net hospital. The study demonstrated that postpartum remote BP monitoring is feasible even in underserved populations when cellular devices are used (no smartphone required).
Postpartum monitoring protocol:
- Continue BP monitoring twice daily for 6-12 weeks after delivery for any patient who had a hypertensive disorder during pregnancy
- Continue weight monitoring to detect late-onset edema (postpartum preeclampsia can develop up to 6 weeks after delivery)
- Continue symptom monitoring (headache, visual changes) for the same period
- Alert thresholds remain the same as antepartum: BP above 140/90 (warning), above 160/110 (critical, immediate escalation)
The handoff protocol:
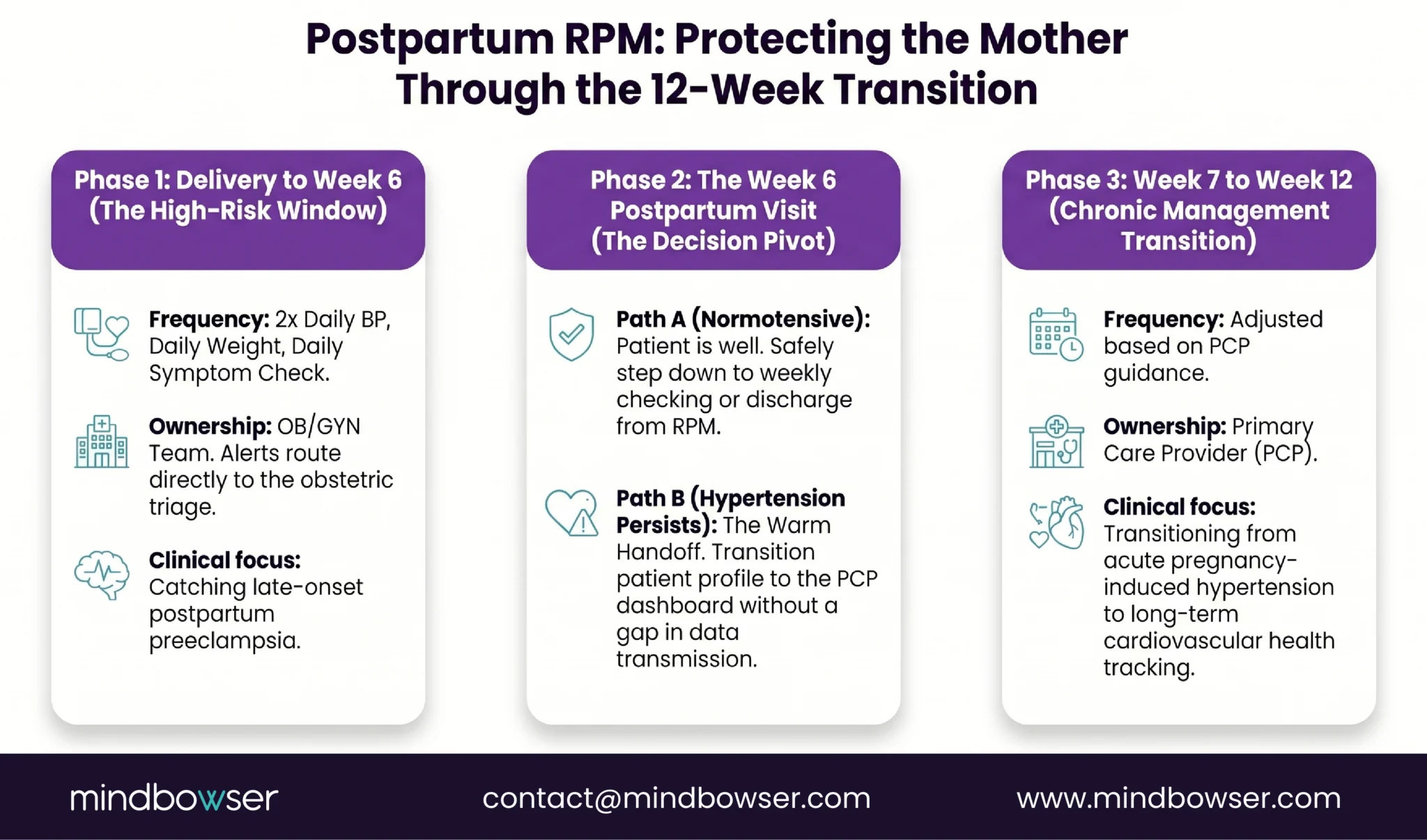
- Weeks 1-6 postpartum: OB team manages monitoring. Alerts route to the postpartum OB provider
- Week 6: postpartum visit. If BP is controlled and symptoms are absent, consider step-down to weekly monitoring or transition to the PCP for ongoing hypertension management
- If BP remains elevated at 6 weeks: transition to the PCP with RPM continuing under chronic hypertension management. See our blood pressure RPM guide for the chronic hypertension protocol
- The critical rule: no gap between OB monitoring and PCP monitoring. The transition must be warm (both teams have access to the patient’s data during the handoff), not cold (OB stops, gap, PCP starts)
For patients who continue into long-term chronic care after the OB handoff, the care plan can also connect to chronic care management workflows.
The Monitoring Gap Is Where Maternal Deaths Happen
Preeclampsia monitoring is simple. A blood pressure cuff, a weight scale, and a symptom questionnaire. The technology cost per patient is under $250. The monitoring protocol is established. The clinical evidence is clear.
The gap between OB visits is where deterioration develops undetected. A condition that can progress from warning signs to hypertensive crisis within 72 hours is checked every 14-28 days during pregnancy and once at 6 weeks postpartum. Remote monitoring fills that gap with daily readings flowing to the clinical team.
I initially thought maternal RPM was a niche application. Then I spent time with the numbers. Six hundred forty-nine deaths in 2024. Hypertensive disorders as a leading preventable cause. More than half of those deaths occurring postpartum, during a period when the standard of care provides almost no monitoring. A $200 cellular BP cuff transmitting twice daily to an OB team could have changed the trajectory for some of those patients.
That is not a niche. That is urgent.
UHC covers pregnancy hypertension for RPM. Medicaid covers it for 42% of births. The AJOG study shows that gestational diabetes RPM drops preeclampsia rates by two-thirds. The 2025 systematic review of 18 studies shows remote BP monitoring reduces hospitalizations without increasing adverse outcomes. The clinical case, the financial case, and the moral case all point in the same direction.
Preeclampsia and gestational hypertension are the primary RPM conditions in pregnancy, with the simplest protocol (BP twice daily, weight daily, symptom questionnaire). Gestational diabetes qualifies for RPM through glucose monitoring (CGM or cellular glucose meter). Chronic hypertension in pregnancy qualifies. Postpartum hypertension qualifies for continued monitoring for 6-12 weeks after delivery. UHC specifically covers “hypertensive disorders during pregnancy” for RPM in 2026.
Yes, across all major payers. UHC covers pregnancy hypertension for RPM (one of only two conditions they still cover). Medicaid, which covers approximately 42% of US births, covers pregnancy RPM in most states. Aetna, BCBS, and Cigna generally cover pregnancy RPM. The exception: UHC excludes gestational diabetes glucose monitoring from RPM coverage (citing insufficient evidence), though BP monitoring for a GDM patient with co-existing hypertension is still covered under the hypertensive disorder designation.
Three devices: a validated upper-arm blood pressure cuff (cellular preferred for patients without smartphones, $80-120), a connected weight scale ($80-120), and a symptom questionnaire delivered through a patient app or automated text/IVR. Total device cost per patient: $160-250. For postpartum monitoring, the same BP cuff continues. CGM (Dexcom G7 or Abbott Libre 3) is added for patients with gestational diabetes, bringing total cost to $225-350.
Yes. The AJOG study showed RPM patients with gestational diabetes achieved glycemic control faster (3.3 vs 4.1 weeks), had higher rates of control in target range (79.2% vs 52.0%), lower preeclampsia rates (5.8% vs 15.0%), and lower neonatal hypoglycemia (29.8% vs 51.7%) compared to traditional paper-based monitoring. CGM captures 288 glucose readings per day versus 4 from finger sticks, detecting postprandial spikes that finger sticks miss.
Yes. More than 50% of pregnancy-related deaths occur in the postpartum period. For any patient who had a hypertensive disorder during pregnancy, blood pressure monitoring should continue twice daily for 6-12 weeks postpartum. Postpartum preeclampsia can develop up to 6 weeks after delivery. The AHA published data on cell-enabled postpartum BP monitoring at a safety-net hospital demonstrating feasibility. The critical gap: the standard of care provides one postpartum visit at 6 weeks. RPM fills the 42-day monitoring void.
BP above 140/90 mmHg triggers a warning alert with OB team notification within 4 hours (may prompt additional monitoring or interim appointment). BP above 160/110 mmHg triggers a critical alert with immediate escalation to the on-call OB provider, as this constitutes a hypertensive emergency in pregnancy requiring urgent intervention. These thresholds are tighter than chronic hypertension thresholds because the clinical risk is higher and the timeline for intervention is shorter during pregnancy.


