



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
- CMS allows concurrent enrollment in RPM (CPT 99457/99458) and CCM (CPT 99490/99439) for the same patient, same month. Combined revenue: $215-300 per patient per month.
- Add Behavioral Health Integration for qualifying patients: $350-400+. At 300 dual-enrolled patients, stacked billing generates $774K to $1.44M annually (CMS CY2026 PFS).
- Most health systems run these programs in separate departments and never stack them. The revenue sitting uncaptured in your existing patient panel is almost certainly six figures.
I ask every CFO I talk to the same question: are your RPM patients also enrolled in CCM?
The answer is almost always no. And the follow-up math is almost always painful.
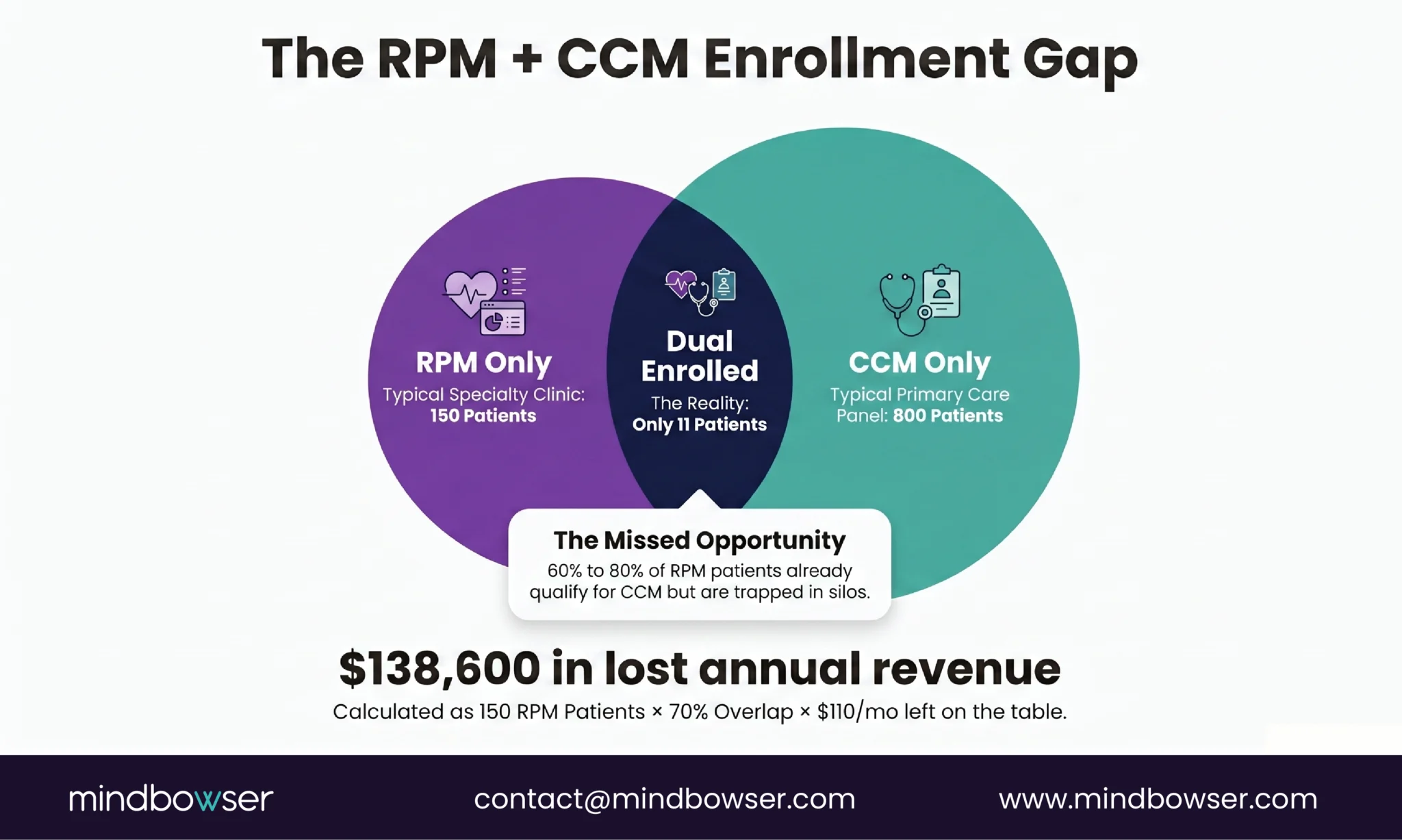
Last quarter, a 400-bed system walked me through their chronic care programs. They had 800 patients in CCM, generating solid revenue under 99490. They had 150 patients in RPM, generating revenue under 99457. I asked how many patients were enrolled in both. The answer: eleven. Eleven patients out of a combined panel of nearly 950. The billing team genuinely did not know concurrent enrollment was allowed.
That is not an unusual story. It is the default. RPM runs out of cardiology or pulmonology. CCM runs out of primary care. Different departments, different budgets, different care managers, different billing workflows. The programs operate in parallel on patients who qualify for both, and neither team captures the stacked revenue.
This piece is the math they should have run before launching either program.
Why Are Most Programs Billing RPM or CCM, Not Both?
Three structural reasons.
- Organizational silos. RPM typically lives in a specialty department (cardiology for heart failure, endocrinology for diabetes, pulmonology for COPD). CCM lives in primary care or population health. These departments have separate leadership, separate budgets, and separate EHR workflows. A patient seeing a cardiologist for heart failure RPM and a PCP for chronic care management is generating data in two systems, with nobody connecting the billing.
- The assumption gap. Many practices believe a patient can only participate in one Medicare chronic care program per month. This is wrong. CMS explicitly permits concurrent enrollment in RPM and CCM, provided the documented time for each program is tracked separately and not double-counted. The rules are clear. The awareness is not.
- Billing system limitations. Most practice management systems are configured to bill one chronic care program per patient. Adding a second program requires configuring separate time buckets, separate code submission workflows, and separate compliance documentation. The technical lift is modest, but nobody prioritizes it because nobody realizes the revenue impact.
The result: practices leave $110-130 per patient per month on the table for every RPM patient who qualifies for CCM but isn’t enrolled. At 200 RPM patients with a 70% CCM qualification rate, that is $18,480 to $21,840 per month in uncaptured revenue. Over a year: $221,760 to $262,080. From patients already in your system, already being monitored, already receiving care.
What Does CMS Actually Allow for Concurrent Billing?
The rules are more permissive than most billing teams realize, with specific mutual exclusions that matter.
What stacks (same patient, same month):
- RPM (99453-99458) + CCM (99490/99439/99491) = Yes
- RPM + BHI (99484 or 99492/99493) = Yes
- CCM + BHI = Yes
- RPM + CCM + BHI (triple stack) = Yes, for patients with chronic conditions + behavioral health diagnosis
- APCM + RPM = Yes (new in 2026)
- APCM + RTM = Yes
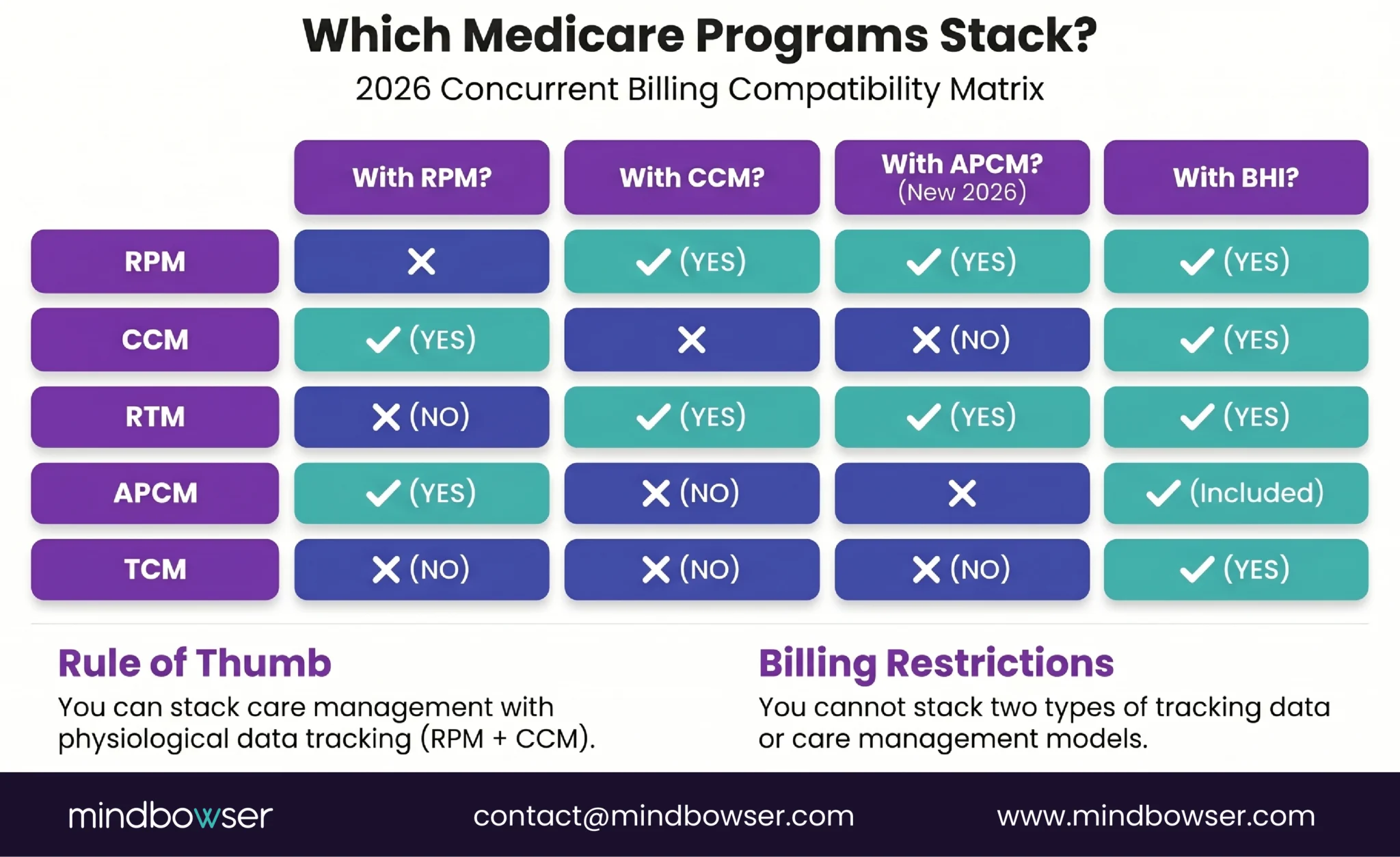
What does NOT stack (mutually exclusive):
- RPM + RTM in the same month = No. Pick one. RTM codes (98979-98985) and RPM codes (99457/99458) cannot be billed for the same patient in the same calendar month
- CCM + PCM = No. These are mutually exclusive care management programs
- CCM + APCM = No. APCM replaces CCM for patients enrolled in the new Advanced Primary Care Management model
- CCM + TCM in the same month = No (TCM is a 30-day post-discharge code)
The critical compliance rule: time must be documented separately for each program. RPM time covers: device data review, interactive communication about readings, alert threshold management, and device-related patient education. CCM time covers: care plan development and revision, care coordination with specialists, medication reconciliation, referral management, chronic disease education not related to devices.
A 30-minute care manager call that discusses both blood pressure readings (RPM) and a specialist referral (CCM) gets split: 15 minutes documented as RPM interactive time (99457), 15 minutes documented as CCM coordination time (99490). The total call is 30 minutes. The billing captures both programs. The documentation must clearly distinguish which minutes belong to which program.
What Is the Revenue Math Per Patient?
Let me walk through the numbers from single-program billing to full stack.
RPM only:
- 99454 (device supply): ~$55-64/month
- 99457 (first 20 min interactive): ~$50-58/month
- Total: $105-122/patient/month
CCM only:
- 99490 (first 20 min): ~$62-70/month
- 99439 (additional 20 min): ~$48-55/month
- Total: $110-125/patient/month
RPM + CCM stacked:
- 99454 + 99457 + 99490: $167-192/patient/month
- Add 99439 (additional CCM time) + 99458 (additional RPM time): $257-295/patient/month
RPM + CCM + BHI (triple stack):
- Add 99484 (BHI, 20 min): ~$50-58/month
- Total: $307-353/patient/month
- Or add 99492/99493 (CoCM): $350-400+/patient/month
Now scale it.
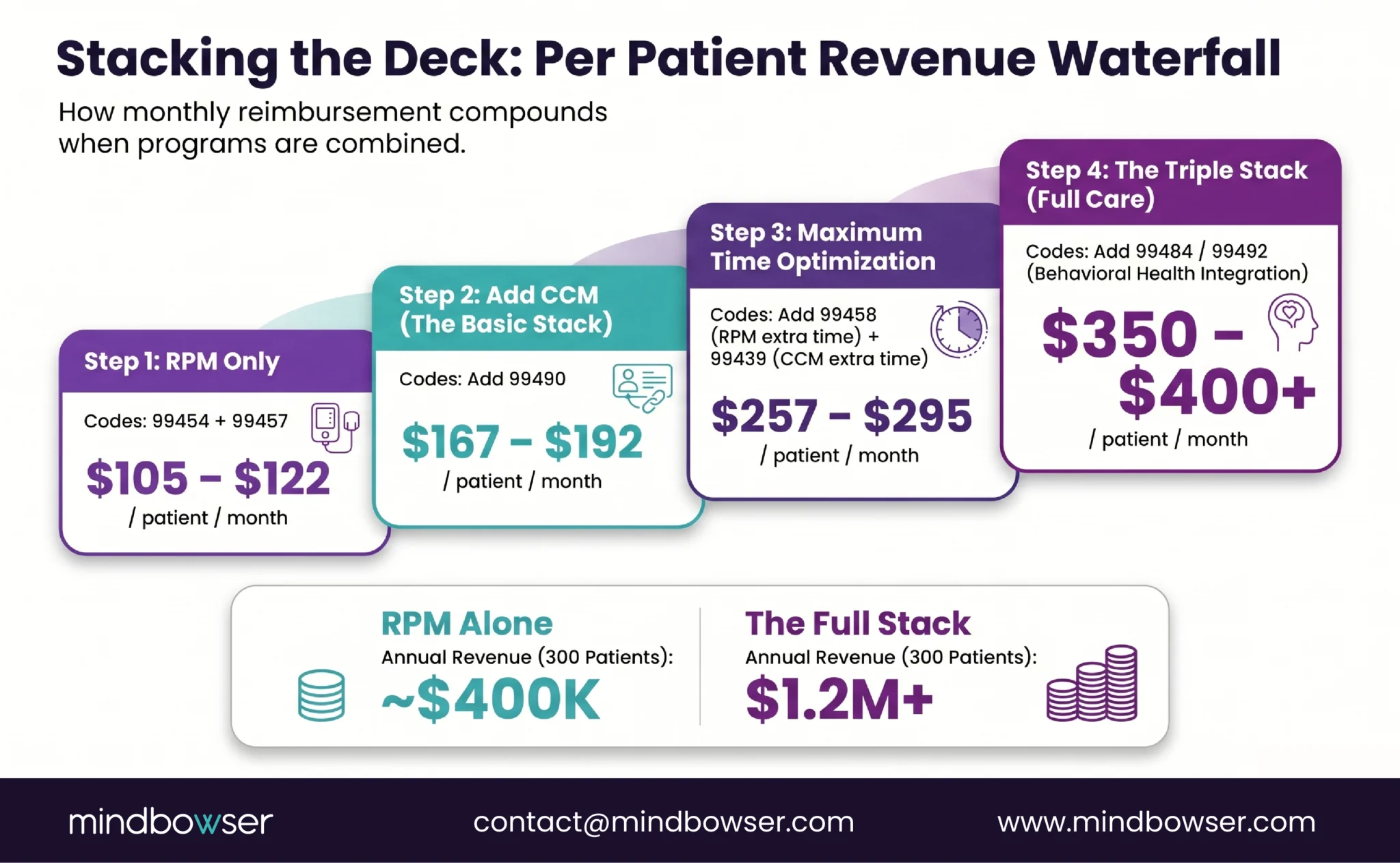
At 500 dual-enrolled patients on the full RPM + CCM stack, you are looking at $1.0 million to $1.84 million annually. From the same patients already in your chronic care panel.
The most common reaction when I present this table to a CFO: “Why hasn’t anyone shown me this before?” The answer is usually that the RPM team reports to the cardiology P&L and the CCM team reports to primary care. Nobody is modeling the combined revenue because nobody owns both programs.
Configure concurrent RPM and CCM billing in your platform
Which Patients Qualify for Both Programs?
The qualification overlap is larger than most programs realize.
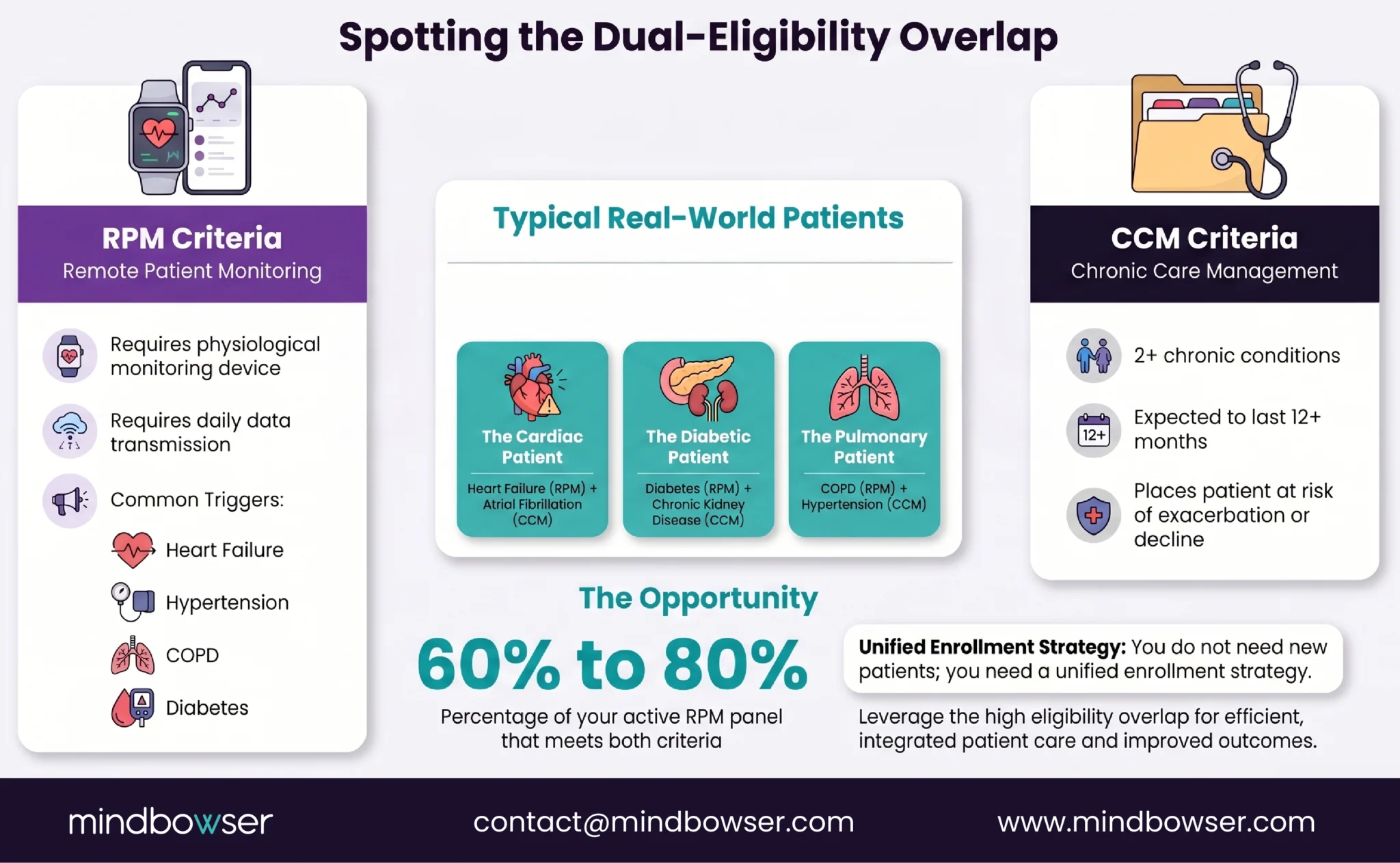
- RPM eligibility: patient must have a condition requiring physiological monitoring (chronic or acute), with a device that transmits data digitally to the practitioner’s monitoring system. Common qualifying conditions: heart failure, hypertension, COPD, diabetes, CKD, obesity.
- CCM eligibility: patient must have 2 or more chronic conditions expected to last at least 12 months, placing the patient at significant risk of death, acute exacerbation, or functional decline. Must have a comprehensive care plan established and maintained.
- The overlap: nearly every RPM patient qualifies for CCM. A heart failure patient on RPM has heart failure (chronic condition #1) and almost always has hypertension, diabetes, CKD, or atrial fibrillation (chronic condition #2+). A COPD patient on RPM typically has hypertension or diabetes as a comorbidity. A diabetes patient on RPM almost always has hypertension.
In my experience across client programs, 60-80% of RPM patients meet the CCM eligibility criteria. The overlap is not the exception. It is the rule.
How to identify the overlap in your panel:
- Pull your current RPM enrollment list
- Cross-reference each patient’s problem list for 2+ chronic conditions
- Verify that a care plan exists or can be established
- Check consent status (patient must consent to CCM separately)
- Run payer eligibility (Medicare FFS is the primary payer for both; commercial coverage varies)
Most practices find the match in a single afternoon. The limiting factor is never patient eligibility. It is operational readiness to manage dual enrollment.
How Do You Track Time Without Double-Counting?
This is the compliance question that stops most billing teams. The answer is simpler than they expect but requires discipline.
RPM-eligible time activities:
- Reviewing device data (BP trends, SpO2 readings, glucose patterns, weight changes)
- Interactive communication with the patient about their readings
- Modifying alert thresholds based on data trends
- Device troubleshooting and patient education on device use
- Documenting device-related clinical observations
CCM-eligible time activities:
- Care plan development, revision, and documentation
- Care coordination with specialists (sending referrals, receiving reports, reconciling recommendations)
- Medication reconciliation unrelated to device readings
- Chronic disease self-management education
- Coordinating community resources (pharmacy, home health, transportation)
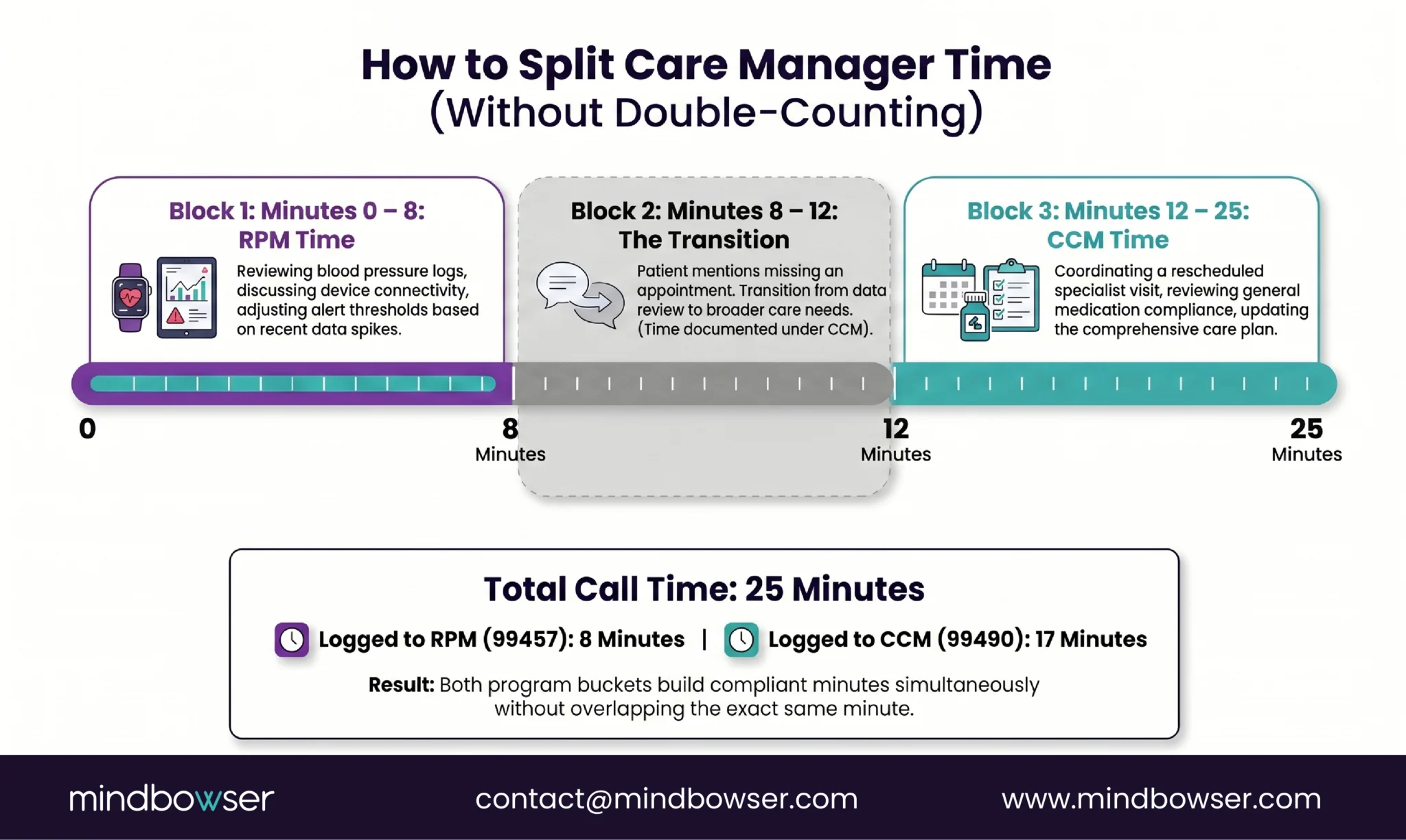
The gray area (and how to handle it): A care manager calls a patient for the monthly RPM check-in. The call starts with reviewing blood pressure readings from the past week (RPM time). The conversation shifts to the patient mentioning they missed their endocrinology appointment (CCM time). The care manager spends 5 minutes discussing readings and 10 minutes coordinating the rescheduled appointment.
Documentation: 5 minutes under 99457 (RPM interactive communication about device readings). 10 minutes under 99490 (CCM care coordination for specialist follow-up). Total call: 15 minutes. Both codes are documented with specific activities and timestamps.
The platform matters here. If your billing system tracks time in a single bucket, you cannot split it for concurrent billing. The system must support separate time documentation for RPM and CCM activities. This is a configuration requirement for any practice running stacked programs.
What Changes in 2026 Affect Stacking?
Three 2026 changes shift the stacking calculus.
- New RPM short-duration code (99445). Covers 2 to 15 days of device data transmission in 30 days, reimbursed at approximately $47, lower than 99454’s approximately $52, and mutually exclusive with 99454 in the same 30-day window. For patients who monitor inconsistently, this means more RPM-eligible months per year. More RPM-eligible months mean more months in which RPM + CCM stacking applies. At a practice level, this could increase dual-billable months by 15-25% for patients who previously fell below the 16-day threshold.
- APCM (Advanced Primary Care Management). New in 2026, APCM is an alternative to CCM with optional add-on codes that eliminate time tracking for BHI and CoCM services. The catch: APCM cannot be billed alongside CCM, PCM, or TCM. The strategic question for each patient: is APCM + RPM more revenue than CCM + RPM? The answer depends on whether the patient qualifies for BHI. If yes, APCM’s BHI add-on (no time tracking required) may simplify operations. If no, CCM + RPM likely generates more revenue.
- Conversion factor increase. CMS raised the Medicare conversion factor for the first time in five years. The increase is modest (roughly $1-2 more per code per encounter) but it compounds across a stacked program with multiple codes per patient per month.
The net effect: 2026 makes stacking both more accessible (short-duration RPM code) and more complex (APCM vs CCM decision). Programs that model the comparison per patient segment will capture more revenue than programs that default to one approach.
How Do You Operationalize Dual Enrollment?
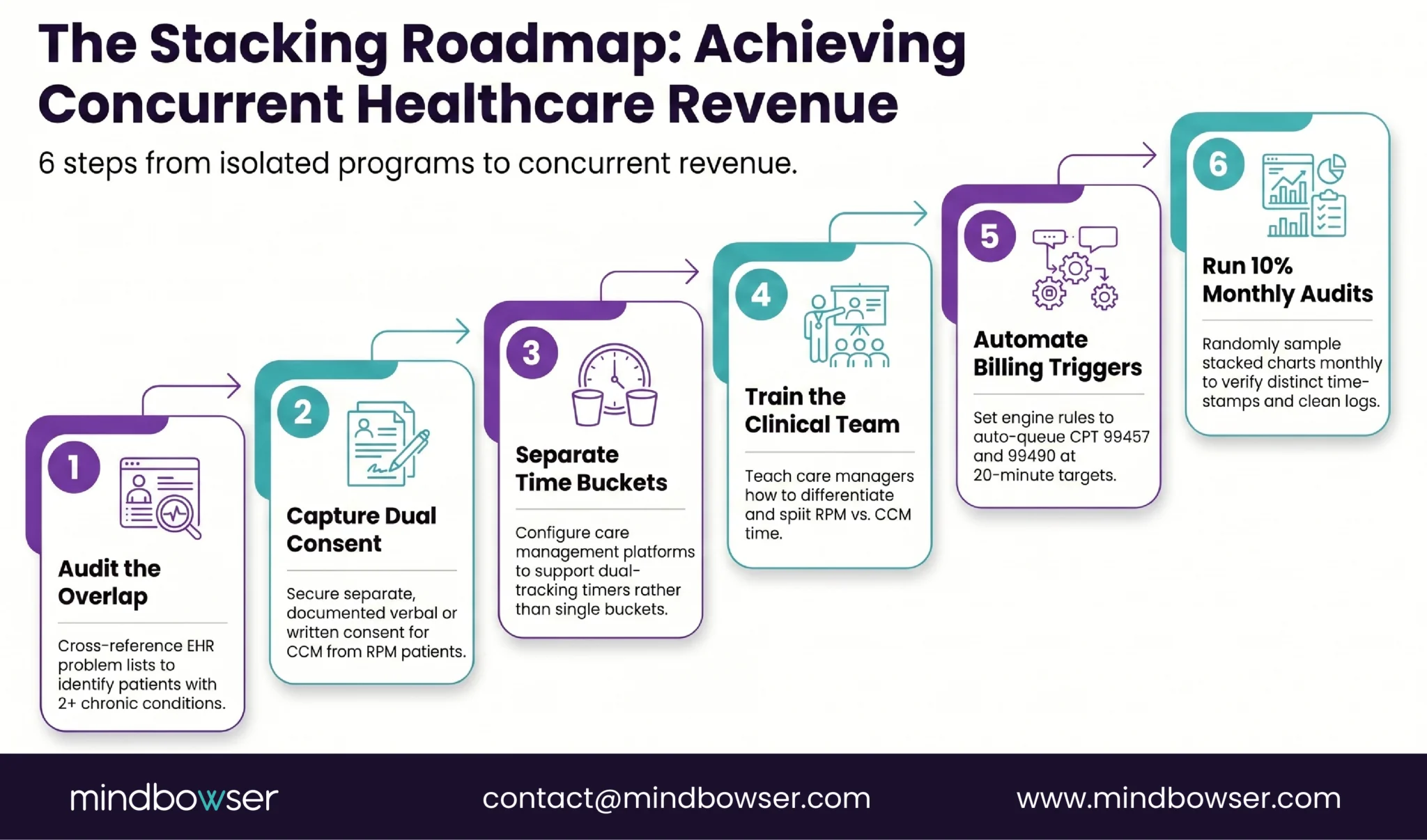
Six steps from “we should do this” to “we’re billing both programs.”
- Step 1: Identify the overlap population. Pull your current RPM enrollment list. Cross-reference each patient’s problem list against CCM eligibility (2+ chronic conditions, 12+ month duration). In our experience, 60-80% match. This analysis takes one afternoon.
- Step 2: Obtain consent. CCM requires separate patient consent (verbal or written, documented in the chart). If the patient is already consented for RPM, add a CCM consent conversation at the next scheduled interaction. One call, two consents.
- Step 3: Configure dual time tracking. Your RPM platform or billing system must support separate time buckets for RPM and CCM activities. If it doesn’t, configure it before enrolling dual patients. This is a platform requirement, not a clinical one. Most modern CCM/RPM platforms (ThoroughCare, ChartSpan, TimeDoc, HealthSnap) support concurrent program tracking.
- Step 4: Train care managers on time splitting. A 90-minute training session covering: which activities count as RPM time, which count as CCM time, how to document a mixed call, and how to use the dual-tracking interface. Include 3-4 scenario walkthroughs.
- Step 5: Set billing triggers. Configure automatic code submission when documented time thresholds are met. RPM 99457 triggers at 20 minutes of device-related interactive time. CCM 99490 triggers at 20 minutes of care coordination time. The system should queue both codes when both thresholds are met in the same month.
- Step 6: Monthly compliance audit. Sample 10% of dual-enrolled patient charts monthly. Verify: time is not double-counted, RPM activities are correctly categorized, CCM activities are correctly categorized, both consents are documented, care plan is current. This audit takes 2-3 hours per month for a 200-patient panel and prevents the audit risk that makes billing teams nervous about stacking.
The Revenue Is Already in Your Patient Panel
This is not a new patient acquisition play. The patients are already enrolled. The devices are already transmitting. The care managers are already making calls. What’s missing is the billing architecture to capture the concurrent value of work that’s already happening.
For a real-world example of RPM infrastructure built around patient monitoring and care-team workflows, see our health monitoring platform case study.
Two years ago I would have told clients to get one program running before adding another. Master RPM first, then layer in CCM. I have changed my position. If you are launching RPM, configure for dual enrollment from day one. The incremental cost of adding CCM billing to an RPM patient is near zero: the care manager is already on the phone, the patient already has the chronic conditions, the care plan can be built during the same enrollment process. The incremental revenue is $110-130 per patient per month. There is no operational scenario where it makes sense to delay.
Run the overlap analysis on your current RPM panel. If more than 50% of your RPM patients are not enrolled in CCM, you are leaving six figures on the table annually. At 300 dual-enrolled patients on the basic stack, that is over $600,000 per year. On the full stack with BHI: over $1.1 million.
The math is not ambiguous. The compliance rules are clear. The configuration is a one-time investment. The only thing standing between your current program and six-figure additional revenue is the decision to do it.
Yes. CMS explicitly allows concurrent enrollment in RPM (CPT 99457/99458) and CCM (CPT 99490/99439) for the same patient in the same month. The requirement is that documented clinical time for each program is tracked separately and not double-counted. RPM time covers device data review and interactive communication about readings. CCM time covers care plan management, care coordination, and chronic disease education unrelated to device data.
Basic stack (99457 + 99454 + 99490): $167-192 per patient per month. Full stack with additional time codes (99458 + 99439): $257-295 per month. Adding BHI for patients with behavioral health diagnoses: $307-400+ per month. At 300 dual-enrolled patients on the basic stack, annual revenue ranges from $601K to $691K. On the full stack with BHI: $1.1M to $1.44M annually.
No. RPM codes (99457/99458) and RTM codes (98979-98985) are mutually exclusive in the same calendar month for the same patient. Choose one per patient per month based on which code family generates more revenue and which monitoring requirements the patient meets. However, RTM can be billed concurrently with CCM, PCM, BHI, and the new APCM program.
Use separate time documentation buckets for each program. RPM activities include: device data review, alert threshold management, interactive communication about readings, device troubleshooting. CCM activities include: care plan development and revision, specialist coordination, medication reconciliation, referral management. For mixed calls, split the minutes by activity type and document each segment separately. Your platform must support dual time tracking; most modern CCM/RPM platforms (ThoroughCare, ChartSpan, TimeDoc) offer this capability.
Program stacking is enrolling a single patient in multiple concurrent Medicare chronic care programs (RPM, CCM, BHI, PCM, RTM) and billing each under its separate CPT code family with independently tracked clinical time. CMS permits stacking when programs are independently documented. The highest-revenue combination is RPM + CCM + BHI for patients with multiple chronic conditions and a behavioral health diagnosis, generating $350-400+ per patient per month.
Advanced Primary Care Management (APCM) is a new 2026 Medicare program that offers an alternative to CCM with optional add-on codes that eliminate the time-tracking requirement for BHI and CoCM services. APCM cannot be billed alongside CCM, PCM, or TCM in the same month. Choose one model per patient. RPM and RTM can still be billed concurrently with APCM. The strategic decision: APCM simplifies BHI billing operations but may generate less total revenue than CCM + BHI for some patient profiles.
RPM requires a condition needing physiological monitoring with a device transmitting daily data. CCM requires 2+ chronic conditions expected to last 12+ months with a comprehensive care plan. The overlap is 60-80% in practice because most RPM patients (heart failure, COPD, diabetes, hypertension) have multiple chronic comorbidities. Run your RPM panel against CCM eligibility criteria; the match rate is typically identified in a single afternoon.


