



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
Epic Payer Platform helps payers and providers work from the same clinical and financial picture. It supports real-time, bidirectional data exchange for prior authorization, claims, care gaps, referrals, and care management inside Epic workflows. The business case is strongest when organizations need to reduce manual record requests, speed payer decisions, improve risk documentation, and support value-based care. The catch? ROI depends on integration strategy, payer participation, workflow redesign, and a custom orchestration layer around Epic.
I. What Is Epic Payer Platform? (And Why It Matters Now)
A. Why payer-provider fragmentation is still a $15 billion problem
Payer-provider integration is no longer a back-office IT issue. It now sits directly in the path of access, revenue, clinician capacity, and patient trust.
Here is the daily reality for many health systems: a clinician orders care, the payer needs more information, the revenue cycle team chases records, the patient waits, and the care team absorbs the frustration. Not dramatic. Just expensive.
CMS has put a number behind the problem. Its Interoperability and Prior Authorization Final Rule is expected to produce about $15 billion in savings over ten years by improving data exchange and prior authorization workflows. CMS also notes that prior authorization can delay care when providers face varied payer requirements and long decision timelines.
What happens when every payer asks for the same clinical truth in a different format?
You get slow authorizations, repeated chart requests, avoidable denials, staff burnout, and incomplete care gap closure. For CIOs and CMIOs, the issue is not just technology. It is an operating design. For CFOs, it shows up as delayed cash, preventable write-offs, and expensive manual labor.
Epic Payer Platform matters because it attacks the waste where it starts: between payer rules and provider workflows.
B. What Epic Payer Platform actually does
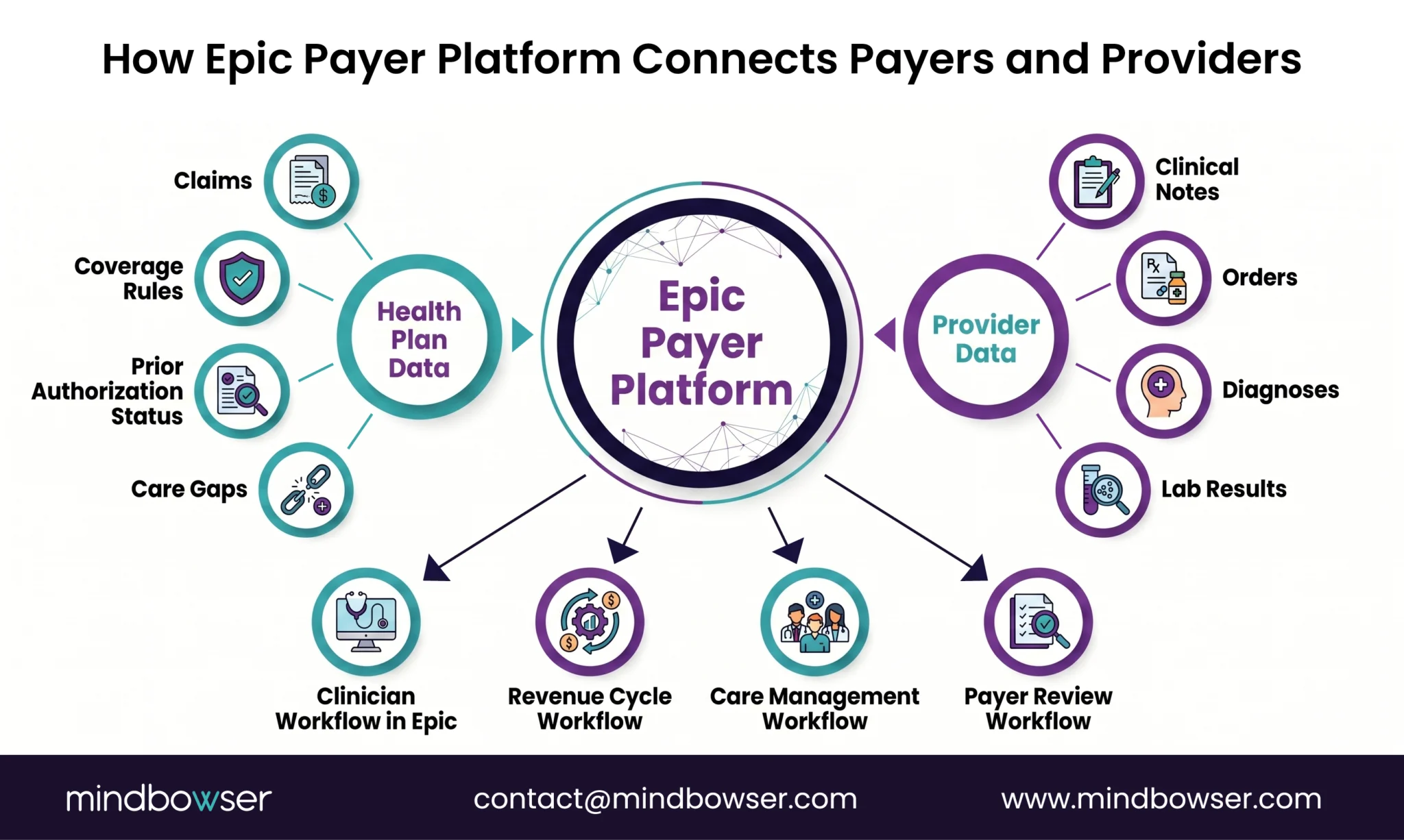
Epic describes its payer software as enabling payers and providers to exchange rich clinical data, reduce care friction, and improve the member experience. Its payer capabilities include provider collaboration, population health, prior authorization, portals, real-time prescription benefits, and healthcare intelligence.
In plain english, the Epic Payer Platform creates a real-time interoperability layer between health plans and provider organizations already integrated with Epic. Instead of pushing teams into fax queues, payer portals, spreadsheets, and phone calls, it brings payer-provider tasks into the EHR flow.
That matters in four areas.
First, prior authorization. Teams can automate requests, track approvals, and support faster decisions without forcing staff to leave the clinical workflow. Epic’s public payer materials highlight integrated prior authorization tools that reduce administrative burden and improve access to care.
Second, claims and denials. Providers can share clinical information with payers earlier, before claims are submitted, which helps reduce avoidable denial loops. Epic’s Payer Platform overview says bidirectional exchange can reduce costs and administrative complexity while improving the healthcare experience.
Third, care management. Payers can send care gaps, diagnoses, claims information, and member insights into provider workflows. That helps care teams act while the patient is still in front of them, not three weeks later when the moment has passed.
Fourth, value-based care execution. Better data exchange supports risk adjustment, HEDIS performance, referrals, utilization management, and population health work. This is where the Epic Payer Platform begins to shift from an “integration project” to performance infrastructure.
The platform is not magic. No platform is. But when payer data, clinical data, and workflow logic meet at the point of care, the organization stops paying people to reconcile systems that should have been talking to each other all along.
Epic Payer Platform is most valuable when it reduces manual chasing and turns payer-provider coordination into an embedded workflow.
II. How Epic Payer Platform Works (Architecture + Core Capabilities)
A. Bidirectional data exchange at scale
Epic Payer Platform works by moving payer and provider data in both directions, inside the systems teams already use. That is the core shift. Traditional payer-provider integration often sends data one way, late, and in batches. Epic Payer Platform is designed for a more active exchange: clinical data, claims context, authorization status, care management updates, and quality insights can move between payer and provider workflows with less manual handling.
Epic’s payer platform overview describes this as a bidirectional data exchange that helps payers and providers reduce costs and administrative complexity while improving the healthcare experience. It also states that tools for claims, prior authorizations, decision support, care management, referrals, and scheduling are delivered to clinicians within their current Epic workflows.
For a CIO, the architecture question is not only, Can Epic connect to the payer? The better question is, Can the organization trust the data, route it to the right workflow, and measure whether work actually disappeared?
That is where the integration layer matters. The platform can synchronize payer and provider systems, but leaders still need clear data rules, consent handling, audit trails, exception queues, and workflow ownership. Without that operating model, real-time exchange can create real-time noise.
B. Key workflows enabled
Epic Payer Platform supports the workflows that usually create the most friction across payer-provider operations.
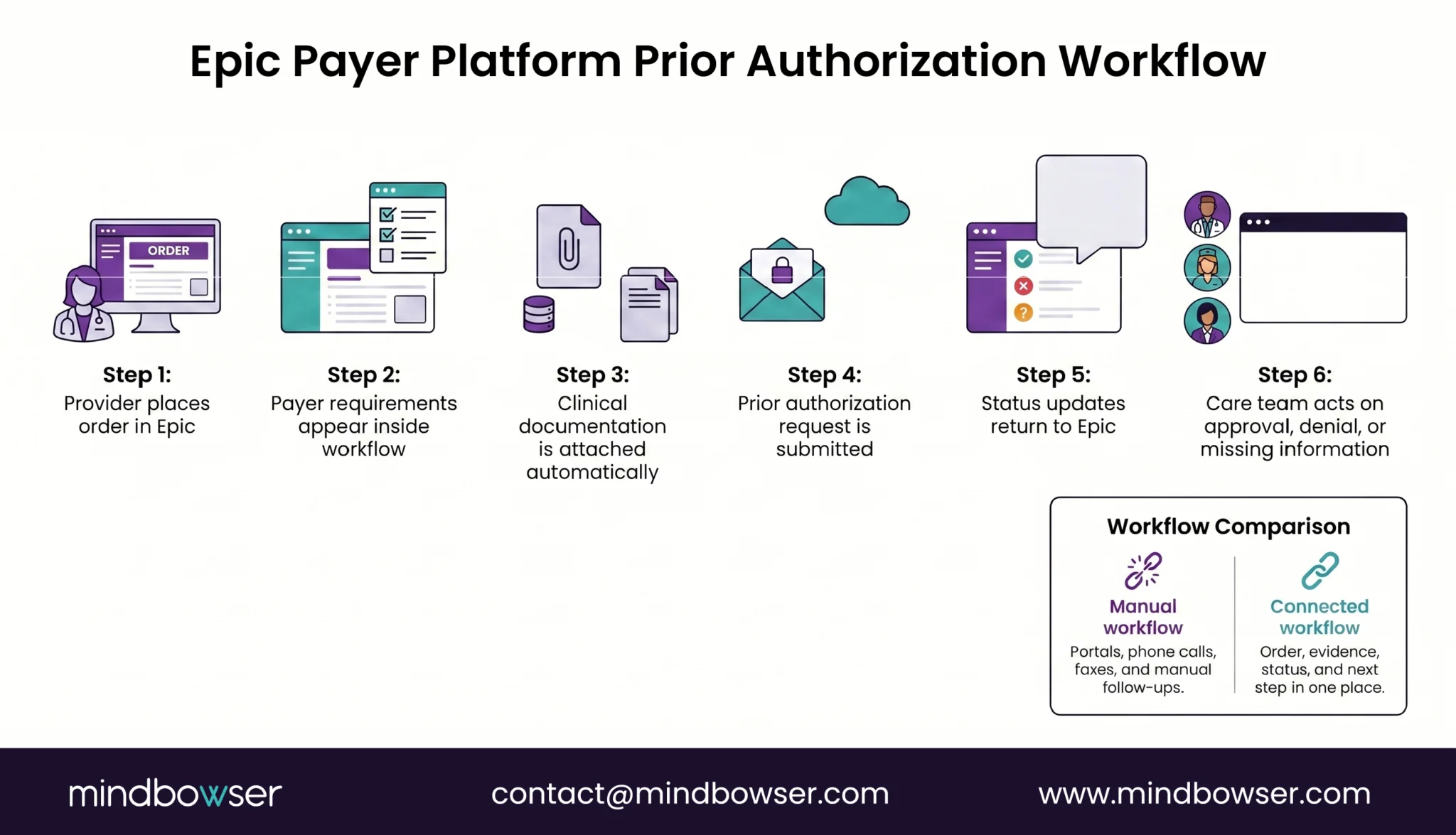
Prior authorization automation is the most visible use case. Instead of staff submitting requests through payer portals or fax-based processes, the work can happen closer to the clinical order. Epic notes that providers and health plans use the Payer Platform to fast-track prior authorization, claims, and quality reporting, with examples such as instant authorization completion and automated chart exchange.
Coverage checks help teams understand payer requirements earlier in the care journey. This reduces surprises after the patient leaves the visit.
Clinical data release to payers reduces manual chart requests. That matters for risk adjustment, quality reporting, denials, and additional documentation requests. When chart exchange is automated and governed, administrative teams stop acting like human APIs.
Care management collaboration brings payer-held insights into provider decision-making. Epic Share has described payer data as including information that providers may not easily access, such as care received at other organizations. That kind of context can help close gaps while the patient is still engaged.
The workflow pattern is simple: identify the payer need, gather the clinical context, route the task, document the action, and return the status. The value is not just speed. There are fewer dropped handoffs.
C. Embedded in clinician workflows
The strongest adoption argument for the Epic Payer Platform is workflow placement. Clinicians and staff do not need another portal that becomes one more tab, one more login, and one more reason to delay the task.
Epic’s payer platform overview states that payer-provider collaboration tools come to clinicians in their current Epic workflows, reducing dependence on faxes, portals, and extra clicks.
That matters because healthcare automation fails when it asks busy teams to do extra work in the name of efficiency. A prior authorization task that appears in the right EHR context, with the right documentation attached, has a much better chance of being completed correctly than a task buried in a payer portal queue.
The architecture only wins when the workflow wins.
For digital health leaders, this is the real design principle: don’t build integration for the interface alone. Build it for the moment of decision. The clinician needs clarity. The revenue cycle team needs status. The payer needs documentation. The patient needs care to move forward.
Epic Payer Platform works best when data exchange, workflow design, and governance operate as one system.
III. Who Uses the Epic Payer Platform? (Key Stakeholders)
A. Health systems & providers
Health systems use Epic Payer Platform to reduce the distance between clinical work and payer decisions. That distance is where administrative cost grows.
For CIOs, the priority is interoperability that does not create another disconnected system. For CMIOs, it is clinician adoption. For revenue cycle leaders, it is faster documentation exchange, fewer avoidable denials, and shorter reimbursement cycles.
What would change if prior authorization, payer record requests, and care gap data appeared inside the normal EHR workflow instead of outside it?
That is the provider-side value case. Epic says its payer collaboration tools can bring payer information and administrative tasks into Epic workflows, including claims, prior authorizations, decision support, care management, referrals, and scheduling. For providers, this means fewer manual handoffs and less portal-hopping.
The practical use cases are clear: reduce administrative burden, improve care coordination, and support faster reimbursement, not by asking staff to “work harder,” but by removing unnecessary chase work from the system.
B. Health plans & payers
Health plans use the Epic Payer Platform to gain a more complete clinical context from provider organizations. That context matters for medical management, risk adjustment, quality reporting, and member engagement.
Medical directors need more than claims. Population health leaders need more than retrospective reports. Quality teams need clinical evidence for measures such as HEDIS, and risk-adjustment teams need accurate documentation tied to actual patient conditions.
The payer benefit is a better signal. Clinical data helps payers understand what happened, what is missing, and where an intervention may prevent avoidable utilization.
A simple example: a payer sees a diabetic member with an open care gap. The provider sees the same patient in Epic. If the payer insight reaches the clinician at the visit, the team can act while the patient is present. If it arrives later in a spreadsheet, it becomes another task in another queue.
This works. Period.
C. Integrated delivery networks (IDNs)
IDNs sit in the middle of the payer-provider convergence story. They often own hospitals, ambulatory practices, employed physician groups, risk contracts, and sometimes health plans. That makes them a strong fit for the Epic Payer Platform, as they need a shared operating logic across care delivery and financial accountability.
For an IDN, the goal is not just data exchange. It is aligned execution for value-based care. That means care gaps, referrals, risk conditions, claims context, utilization signals, and care management tasks need to move across teams without forcing each department to rebuild the truth.
The best IDN use cases usually start where incentives already exist: Medicare Advantage, accountable care arrangements, Medicaid managed care, and employer-sponsored risk contracts. These models depend on earlier intervention, better documentation, and fewer preventable delays.
The platform helps, but governance decides the outcome. Who owns the workflow? Who approves data release rules? Who resolves mismatched payer-provider records? Those questions separate integration from performance.
D. Digital health ecosystems
Digital health teams use the Epic Payer Platform as a connection point for analytics, AI, population health, and care navigation tools that need reliable payer-provider data.
The opportunity is not to replace Epic. It is to build around Epic with the right orchestration layer. Product heads and digital health leaders can connect Epic workflows with external analytics platforms, claims systems, AI summarization tools, risk models, referral engines, and member engagement applications.
That said, digital health ecosystems must be careful. If the workflow depends on clinicians copying data between screens, adoption will suffer. If the integration sends too many alerts, trust will drop. If the data model does not reconcile payer and provider identities well, reporting will look precise but behave poorly.
Epic Payer Platform serves four groups best: providers who need workflow relief, payers who need clinical context, IDNs that carry risk, and digital health teams that need dependable integration paths.
IV. Key Features of Epic Payer Platform
A. Real-time clinical data exchange
The first major feature of Epic Payer Platform is automated clinical data exchange between providers and payers. This is where the platform removes one of healthcare’s most stubborn habits: asking humans to move records between systems that should already be connected.
In a traditional workflow, payer teams request records, provider staff pull charts, someone uploads files, someone checks status, and everyone waits. Epic Payer Platform changes that pattern by supporting clinical data release to payers through connected workflows.
For providers, this can reduce chart-chasing and staff rework. For payers, it improves access to clinical evidence needed for claims review, quality reporting, utilization management, and risk adjustment. For patients, it can mean fewer delays caused by missing documentation.
Would your team rather review care decisions or hunt for PDFs?
The ROI comes from replacing manual retrieval with governed exchange. That means policies still matter. Consent, auditability, minimum necessary access, and role-based controls cannot be afterthoughts. The data moves faster, so governance must be tighter.
B. Prior authorization automation
Prior authorization is often the clearest business case for the Epic Payer Platform because it affects access, revenue, and staff capacity simultaneously.
The platform allows prior authorization activity to happen closer to the point of care. Teams can submit, monitor, and respond to payer requirements without depending only on portals, phone calls, and manual follow-up. That matters because CMS has identified prior authorization as a workflow that can delay care and create administrative burden, which is why its interoperability rule requires certain payers to send prior authorization decisions within defined timeframes and give specific reasons for denials.
For executives, the value is not simply faster submission. It is better control. A strong prior authorization workflow should show:
What was requested.
What documentation supports it.
Who owns the next step.
Where the request is delayed.
How the outcome affects care and revenue.
When authorization status lives within the EHR workflow, operational leaders can manage the process rather than discover delays after patients call back angry. Fair warning: patients are not fond of administrative archaeology.
C. Care gap insights at point of care
Care gaps are only useful when they reach the right person at the right moment.
Epic Payer Platform can bring payer-held insights into provider workflows, including information that may not be obvious from the provider’s own records. This helps clinicians and care teams see open gaps during visits, outreach, care management reviews, or population health workflows.
The key phrase is “actionable at point of care.” A care gap report that arrives after the visit is a reminder. A care gap insight inside the visit is an intervention.
For example, a payer may identify a missing preventive screening, medication adherence issue, or risk condition based on claims and member activity. The provider may hold clinical notes, lab results, diagnoses, and the patient relationship. Together, the picture is stronger.
This is especially important for value-based care teams. Care gaps, risk conditions, referrals, and follow-up tasks must move from reporting to execution. A dashboard alone does not close a gap. A workflow does.
D. Quality reporting & risk adjustment
Quality and risk programs depend on an accurate clinical context. Claims alone rarely tell the full story, and clinical records alone may miss care delivered outside the system. Epic Payer Platform helps connect these views.
For HEDIS, Stars, Medicare Advantage, Medicaid managed care, and other value-based programs, payers and providers need evidence that is timely, complete, and tied to the patient’s actual care journey. Better data exchange can improve measure capture, documentation quality, and risk adjustment accuracy.
This is where CIOs and population health leaders should look beyond interface counts. The question is not, How many connections did we build? The question is, Did those connections improve measure performance, reduce manual review, and help teams act sooner?
The platform can support this work, but the organization still needs data stewardship. Measure logic, diagnosis validation, attribution, patient matching, and exception management all require careful design.
E. AI-driven workflow optimization (emerging)
AI is not the core of the Epic Payer Platform, but it is becoming part of the operating layer around payer-provider integration.
The emerging opportunity is to use AI to reduce documentation effort, summarize clinical context, score risk, and route work intelligently. For example, AI can help summarize chart history for prior authorization, flag missing evidence for a payer request, identify likely care gaps, or predict readmission risk for care management teams.
But healthcare leaders should be practical. AI cannot fix weak governance, poor data quality, or broken workflows. It can only make the existing operating model faster. If the process is messy, AI may scale the mess.
The better approach is to be sequenced: build reliable data exchange, define workflow ownership, add audit controls, then apply AI where it removes effort or improves decision-making.
Epic Payer Platform features deliver the most value when they move work from manual chase to governed action. Clinical exchange, authorization, care gaps, quality reporting, and AI all matter, but workflow design decides the return.
V. Real-World Impact (Success Stories & Outcomes)
A. Reduced administrative burden
The first measurable impact of Epic Payer Platform is less manual work. That sounds simple, but it changes the economics of payer-provider operations.
Epic Share reported that OSF HealthCare connected with Aetna through the Payer Platform to exchange medical records electronically, eliminating workflow inefficiencies and administrative burden associated with manual record exchange. The case also focused on reducing denials and accelerating payments, which is exactly where CFOs and revenue cycle teams feel payer friction first.
Another Epic Share example described NorthShore using Payer Platform with two large payers to send clinical documents electronically. The result: less time spent on administrative overhead, fewer payer medical record requests, and better care coordination for patients.
This is the executive point: record exchange is not clerical work when it blocks care and cash. It becomes a strategic constraint.
How many full-time hours does your organization spend proving what your EHR already knows?
When chart release, documentation exchange, and payer requests move from manual queues into governed digital workflows, teams get time back. That time can shift toward authorization exceptions, denial prevention, and patient follow-up instead of repetitive retrieval.
B. Improved care coordination
Epic Payer Platform also improves care coordination by enabling payer-held insights to reach provider teams earlier. That matters in value-based care, where the costliest issue is often not missing data. It is late data.
Blue Shield of California described Epic Payer Platform as part of its bidirectional data exchange strategy across eligible provider partners. The plan included more timely communication about care gaps, admission and discharge notifications, and overall health status, while allowing the payer to acquire relevant provider data and push insights back to support clinical decisions.
The workflow value is timing. A care gap inside a monthly report is an administrative task. A care gap during the visit is a clinical opportunity.
For CMIOs and population health leaders, this creates a practical bridge between claims intelligence and bedside action. The payer may be aware of out-of-network care, missed preventive screenings, or recent utilization. The provider may be aware of current symptoms, labs, medications, and patient preferences. When those signals meet, care teams can act with more confidence.
Better data does not replace clinical judgment. It gives judgment a cleaner operating field.
C. Faster decision-making
Payer-provider integration improves decision-making by giving teams immediate access to both clinical and financial context.
Epic’s Payer Platform overview states that the tools supporting claims, prior authorizations, decision support, care management, referrals, and scheduling come to clinicians within their current Epic workflows. That means the decision does not need to wait for a fax, a phone call, a portal login, or a separate data pull.
For healthcare leaders, the ROI comes from compression. Less waiting, fewer handoffs, faster status clarity.
Picture a high-cost imaging order. In a fragmented workflow, the team may place the order, discover payer requirements later, request documentation, wait for review, and reschedule the patient if approval lags. In a connected workflow, payer requirements and relevant documentation can surface earlier, which helps teams avoid delays before they become denials or patient complaints.
This matters for clinicians, too. They do not want another administrative guessing game. They need to know what is covered, what is needed, and what happens next.
faster decisions come from workflow clarity, not just faster data transport.
D. Example outcomes from implementations
The strongest examples point to three outcome categories: fewer unnecessary administrative steps, better execution of preventive care, and a stronger patient experience.
Independence Blue Cross announced the implementation of the Epic Payer Platform with Drexel Medicine, Jefferson Health, Main Line Health, and Penn Medicine to streamline data exchange, close care gaps, and improve outcomes for members. The organization also said it expected future use to support automated prior authorization requests and updates, improving efficiency and reducing delays.
Epic Share also reported a Geisinger preventive care outreach initiative that increased breast and colorectal cancer screening rates by 4% within 18 months, saved 88,000 staff hours, and translated to about $2.3 million in cost savings. That example is not positioned as a Payer Platform case, but it shows the broader operational value of timely, coordinated care gap workflows in Epic-enabled environments.
For executives, the pattern is clear. Real-world value appears when the platform changes work, not when it simply connects systems.
Reduced unnecessary admissions, improved preventive care metrics, and better patient experience all depend on the same chain: timely data, trusted workflow, clear ownership, and measurable action.
Epic Payer Platform creates ROI when payer-provider data exchange becomes part of daily operations, not a side process managed after the fact.
VI. Pros and Cons of Epic Payer Platform
A. Pros (Where it delivers ROI)
Epic Payer Platform delivers the strongest ROI when the organization has high payer friction, high Epic adoption, and a clear value-based care agenda.
The first benefit is real-time interoperability across the payer-provider relationship. Epic says its payer tools help payers and providers exchange rich clinical data, reduce friction in care, and improve the member experience. That exchange can support prior authorization, claims, care management, referrals, scheduling, and decision support inside existing Epic workflows.
The second benefit is adoption. A workflow that appears inside Epic has a better chance of being used than a separate payer portal. That matters because clinician and staff time is already under pressure. The 2024 CAQH Index reported a $90 billion annual cost for routine administrative tasks and a $20 billion savings opportunity if the industry moves from manual to electronic workflows.
The third benefit is value-based care execution. Epic Payer Platform can support care gap closure, risk adjustment, quality reporting, and payer-provider alignment. For leaders managing Medicare Advantage, Medicaid managed care, ACO, or employer-risk populations, this creates a more useful bridge between claims insight and clinical action.
The value chain is clear: fewer manual requests, faster decisions, cleaner documentation, better coordination, stronger financial performance.
B. Cons (Where organizations struggle)
The tradeoff is complexity.
Epic Payer Platform is not a plug-in that fixes payer-provider operations by itself. It requires Epic environment alignment, payer participation, governance, workflow redesign, and integration maturity. Without those pieces, teams may connect the systems but still keep the old workarounds.
The first struggle is the implementation scope. Health systems need to map which payers participate, which workflows come first, which data can be exchanged, and who owns exceptions. Prior authorization may be the obvious entry point, but chart release, risk adjustment, and quality reporting each carry different data rules and operational owners.
The second struggle is flexibility outside Epic-heavy environments. Organizations with mixed EHR footprints, external care networks, legacy payer systems, or non-Epic digital health tools may need a custom orchestration layer to route data and tasks correctly.
The third struggle is adoption. What happens if the integration is live, but clinicians still do not trust the alerts? You get a connected system with disconnected behavior.
CMS is also raising expectations. Its Interoperability and Prior Authorization Final Rule adds new data-sharing and prior authorization requirements for impacted payers, including API-driven improvements intended to reduce burden. That creates urgency, but it also raises the bar for auditability, data quality, and process design.
Epic Payer Platform is worth serious consideration, but only when leaders treat it as an operating model change, not just an Epic configuration project.
VII. Interoperability with Epic Modules & Ecosystem
A. Epic Tapestry (Payer Core System)
Epic Payer Platform becomes more powerful when it connects with the broader Epic ecosystem, especially Tapestry.
Epic Tapestry is Epic’s payer-focused system for health plan operations. In practical terms, it supports workflows such as claims processing, benefits configuration, utilization management, referrals, and member operations. When paired with the Epic Payer Platform, Tapestry can help payer teams bring operational context closer to provider workflows.
That matters because payer-provider integration is not only about moving clinical notes. It is about connecting coverage, benefits, utilization rules, authorization status, claims context, and care decisions in a way that enables both sides to act on them.
Can a provider make a better care decision when payer rules appear earlier in the workflow? Yes, but only if the data is timely, trusted, and clear enough for staff to use without interpretation gymnastics.
For CIOs, the priority is architecture discipline. Tapestry may support payer-side operations, but the organization still needs orchestration across provider Epic, payer systems, analytics tools, and external partners.
B. Epic CareEverywhere
CareEverywhere supports cross-organization health information exchange inside the Epic network. For payer-provider workflows, this matters because the patient’s care history often spans multiple organizations.
CareEverywhere helps widen the clinical view. A provider may see internal visits, labs, imaging, and notes. But the patient may also receive care elsewhere. When external clinical information is available, payer and provider teams can make better decisions about gaps, utilization, duplication, and follow-up needs.
For example, a payer may flag an avoidable pattern in emergency department use. CareEverywhere may help a provider see outside encounters that explain the pattern. Together, they create a fuller operational picture.
The tradeoff is governance. More data does not automatically mean better decisions. Teams need patient matching, consent rules, access controls, and clear guidance on what should enter the workflow.
C. Epic MyChart
Epic MyChart extends payer-provider integration into the patient experience.
When payer insights, care reminders, coverage guidance, or follow-up instructions are integrated into patient-facing workflows, MyChart can help reduce confusion and improve engagement. This is especially useful when a payer-provider workflow directly affects the patient, such as preventive screening, authorization status, referrals, benefits questions, or care management outreach.
The patient should not become the courier between payer and provider.
That sentence matters. When patients are asked to call the payer, call the clinic, upload records, check status, and repeat their story, the system has failed them. MyChart can help close part of that loop by giving patients clearer next steps and a single digital front door for parts of the journey.
For product leaders, the design challenge is tone and timing. Too many payer-related messages can feel like billing noise. The right message, at the right moment, can move care forward.
D. Epic Cogito & Caboodle
Cogito and Caboodle support analytics across the Epic environment. For the Epic Payer Platform, they matter because integration must eventually prove value.
Executives need to know whether payer-provider exchange actually reduced work, improved outcomes, and protected revenue. That requires reporting on more than interface uptime.
Useful measures include prior authorization turnaround time, denial rate, chart request volume, care gap closure rate, risk condition capture, avoidable admission trends, and staff hours redirected from manual tasks. Without analytics, leaders may know the platform is live but not whether it is working.
Caboodle can support structured data warehousing, while Cogito can help organizations report across clinical, financial, and operational activity. The strategic value comes from turning payer-provider exchange into a measurable performance management system.
A good dashboard answers three questions: Where is work stuck? Who owns it? What changed after integration?
E. FHIR-based interoperability
FHIR-based interoperability is now part of the regulatory and operational foundation for payer-provider exchange.
CMS has pushed the industry toward API-driven access, including requirements under its Interoperability and Prior Authorization Final Rule for impacted payers. The rule includes payer-to-payer, patient access, provider access, and prior authorization API policies intended to improve health information exchange and reduce administrative burden.
For the Epic Payer Platform, FHIR matters because it provides organizations with a more standardized way to exchange structured data across systems. But standards do not remove the need for strategy. Organizations still need to decide which workflows use APIs, which data elements are required, how exceptions are handled, and how the integration is monitored.
FHIR is the rail. Workflow is the train.
Epic Payer Platform delivers more value when it connects cleanly with Tapestry, Care Everywhere, MyChart, Cogito, Caboodle, and FHIR-based data exchange. The ecosystem matters, but architecture choices decide how much value reaches the front line.
VIII. Epic Payer Platform vs Traditional Payer-Provider Integration
A. Traditional model
Traditional payer-provider integration was built for transactions, not real-time decisions.
In the old model, data often moves through batch files, portals, fax queues, manual uploads, phone calls, and delayed eligibility or authorization checks. A payer asks for records. A provider searches the EHR. A staff member exports a chart. Another staff member uploads it somewhere else. Then both sides wait.
It works, technically. It just burns time.
The biggest weakness is limited visibility. Providers may not see payer requirements until after an order is placed. Patients may not see clinical evidence for days. Patients may not know whether care is approved until the process is already delayed.
What does that mean for an executive team? It means poor workflow control. Leaders can see denial rates, staff hours, or authorization delays after the damage is done, but they struggle to manage the work as it happens.
Traditional integration also creates a hidden adoption problem. When teams must leave the EHR to complete payer tasks, the workflow depends on memory, training, and manual discipline. That is fragile. Busy teams miss steps. Documentation gets delayed. Follow-up becomes a person, not a process.
B. Epic Payer Platform model
Epic Payer Platform shifts the model from delayed exchange to embedded coordination.
Instead of sending data late and asking staff to reconcile it, the Epic Payer Platform brings payer-provider workflows closer to the clinical and administrative moments when decisions are made. Prior authorization, care gap insights, clinical data exchange, quality reporting, and payer collaboration can be integrated into Epic workflows rather than sitting outside them.
The difference is not only speed. It is context.
A prior authorization task inside the EHR can include the order, documentation, payer requirement, status, and next step. A care gap insight can appear while the patient is still present. A clinical data request can be routed with audit controls instead of becoming another record chase.
For CIOs, this changes the technology conversation from “Did we connect the systems?” to “Did we remove work from the operating model?” For CMIOs, it changes adoption from training people on another portal to putting the right action in the right place. For CFOs, it creates a path to fewer avoidable denials, less rework, and faster reimbursement cycles.
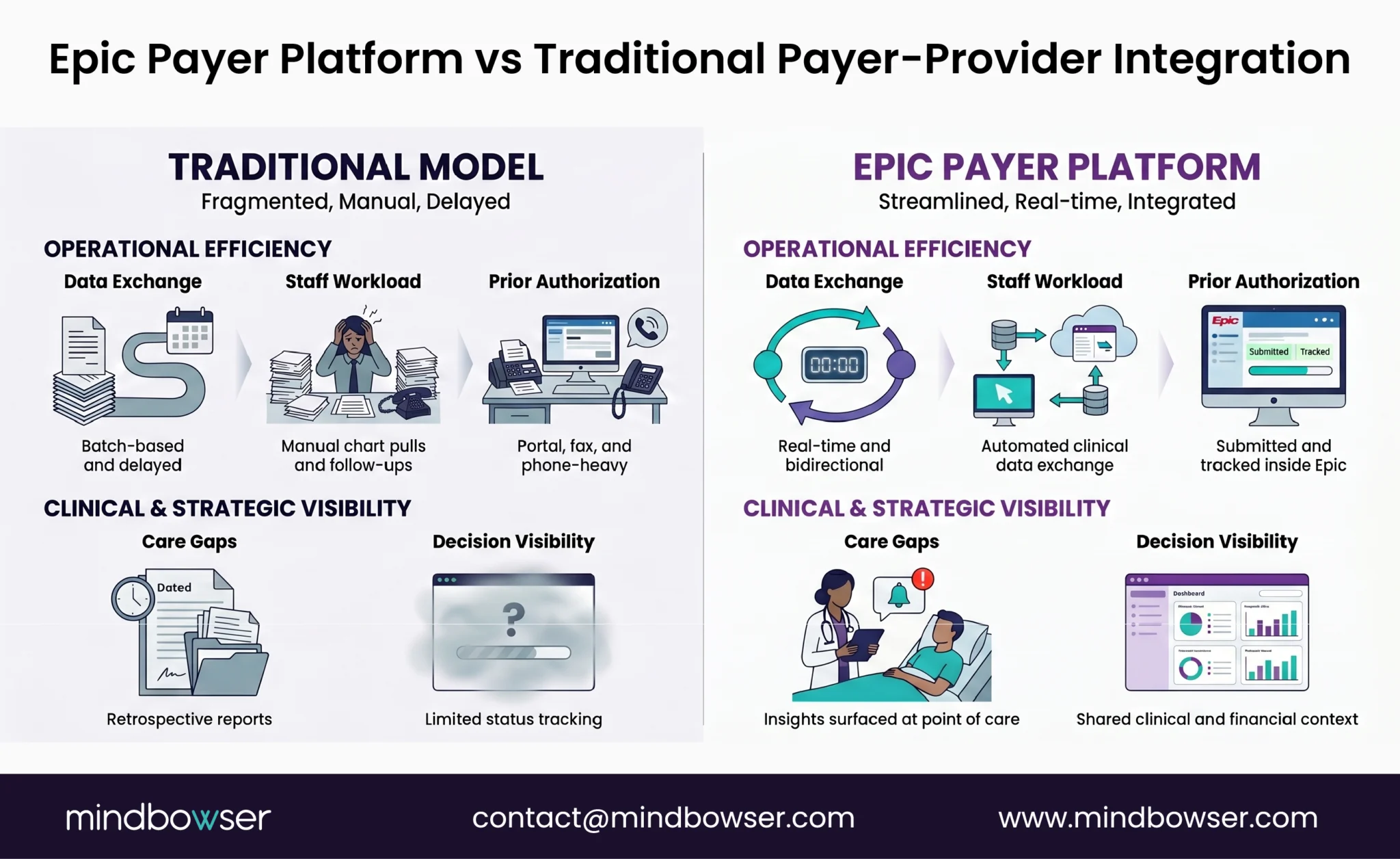
The clean comparison is simple:
Traditional model: batch exchange, manual work, limited visibility.
Epic Payer Platform model: real-time exchange, automated workflows, shared clinical and financial decisioning.
Traditional integration moves information; Epic Payer Platform is designed to move decisions. That is the difference leaders should measure.
IX. When Should You Invest in Epic Payer Platform?
A. Ideal scenarios
Epic Payer Platform makes the most sense when payer friction is already costing money, time, and patient trust.
The strongest trigger is a move toward value-based care. If your organization is taking more risk, managing Medicare Advantage lives, or trying to close quality gaps faster, you need payer and provider data to meet inside the workflow.
It also fits organizations with high prior authorization volume. When staff spend hours checking coverage, submitting documentation, tracking status, and chasing decisions, the business case becomes easier to defend.
A third fit is multi-payer complexity. If your teams manage different rules across many plans, Epic Payer Platform can reduce some of the noise by embedding payer-provider exchange into Epic workflows.
Ask this directly: are we solving a data problem, a workflow problem, or both?
If the answer is both, the platform deserves a serious look.
B. Red flags
Not every organization is ready.
If your care network is not Epic-dominant, the rollout may require heavier custom integration. If payer participation is limited, the ROI may arrive slowly. If internal teams lack governance around data sharing, consent, auditability, and workflow ownership, the platform can expose the gaps instead of fixing them.
The biggest red flag is treating the Epic Payer Platform as an IT installation. It is not. It changes how the revenue cycle, clinical operations, payer relations, population health, and compliance teams work together.
invest when the workflow pain is measurable, payer participation is real, and leadership is ready to redesign the operating model.
X. Implementation Challenges (What CIOs Must Plan For)
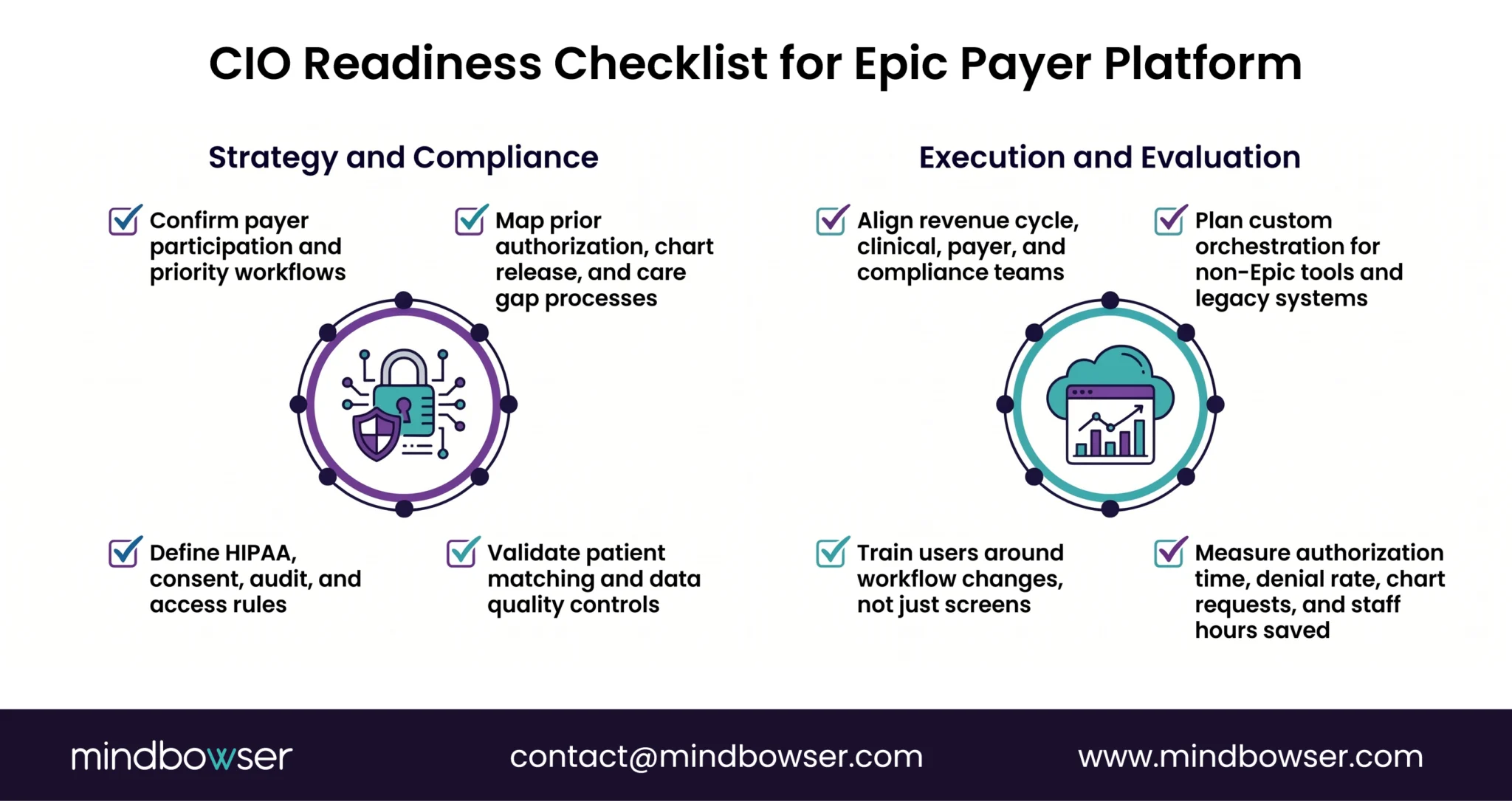
A. Data governance & compliance
Real-time exchange raises the bar for governance. CIOs must define what data can move, who can access it, how consent is handled, and how every action is audited.
HIPAA, role-based access, minimum necessary rules, and audit trails need to be designed before workflows go live. Faster exchange without control creates risk.
B. Workflow redesign
Epic Payer Platform works only when clinical and administrative teams agree on the new process.
Who owns a pending authorization? Who resolves missing documentation? Who closes the loop with the patient?
Those answers must be clear. Otherwise, the same manual work returns under a new interface.
C. Integration complexity
Legacy systems, payer platforms, HIEs, analytics tools, and external care partners can complicate implementation.
The hard part is not just connecting systems. It is mapping data, reconciling patient identity, routing exceptions, and keeping workflows reliable across teams.
D. Change management
Clinicians will not adopt a workflow they do not trust.
Training matters, but trust matters more. Leaders should start with high-value use cases, measure results, and remove noise from alerts. Adoption grows when teams see fewer clicks, fewer delays, and fewer follow-up calls.
Implementation success depends on governance, workflow design, integration discipline, and adoption.
Assess your Epic integration readiness
XI. How Mindbowser Builds Custom EHR with Epic Integration Capabilities
A. Why off-the-shelf Epic integration often falls short
Epic Payer Platform is powerful, but enterprise workflows rarely fit one standard pattern.
Most gaps appear in three places: custom workflows, data orchestration, and AI enablement. A health system may need payer data routed into a unique prior authorization queue. A payer may need clinical summaries shaped for a specific utilization review process. A digital health team may need to connect Epic data to analytics, care navigation, or risk models.
The platform creates the foundation. The customization layer creates the return.
B. Our approach (Practitioner POV)
Mindbowser builds around an interoperability-first architecture. That means FHIR APIs, real-time data pipelines, clear audit controls, and workflow logic designed around how care teams actually work.
Where should data go, who should act on it, and what should happen next?
Those questions guide the build. We create orchestration layers for prior authorization automation, care gap intelligence, claims context, care management workflows, and analytics-ready data exchange.
C. Accelerators we bring
Mindbowser brings accelerators that reduce build effort without forcing a generic product fit.
These include AI-driven clinical summarization, risk scoring, readmission prediction, and workflow automation engines. The goal is practical: reduce manual review, surface the right context, and help teams act faster.
D. Integration capabilities
Mindbowser supports integration across Epic Payer Platform, Epic Tapestry, CareEverywhere, external HIEs, claims systems, and population health platforms.
That matters when the real environment includes both Epic and non-Epic tools, payer platforms, data warehouses, and third-party applications. Integration must reflect the operating reality, not the clean diagram.
E. Outcomes we drive
The target outcomes are direct: faster time-to-value, reduced administrative cost, fewer workflow handoffs, better care coordination, and stronger support for value-based care.
Mindbowser helps teams turn Epic integration from a connection project into a working payer-provider operating model.
The Strategic Value of Epic Payer Platform
Epic Payer Platform is worth it when payer-provider coordination has become a measurable drag on care access, revenue, and staff capacity. It fits best in Epic-heavy environments moving toward value-based care, where prior authorization delays, manual chart requests, care gaps, and denial cycles create daily friction. The platform provides leaders with a stronger foundation for real-time exchange, but success depends on the integration strategy, workflow redesign, governance, and adoption. Epic Payer Platform is not just an interoperability investment. It is a way to turn payer-provider collaboration into a repeatable business capability.
Epic Payer Platform is a payer-provider integration layer that enables real-time data exchange inside Epic workflows. It helps support prior authorization, claims, care gaps, quality reporting, and care management.
It is best suited for health systems, IDNs, payers, and Epic-heavy organizations managing high prior authorization volume, value-based care contracts, or complex payer-provider workflows.
It reduces manual chart requests, payer portal use, fax-based workflows, and repeated documentation follow-ups. Teams can exchange clinical and payer data directly within connected workflows.
Yes. It supports care gap closure, risk adjustment, quality reporting, utilization management, and payer-provider collaboration, all of which are central to value-based care execution.
The main challenges are data governance, workflow redesign, payer participation, integration complexity, and clinician adoption. Strong planning is required to turn the platform into a measurable ROI.


