



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
Physicians spend 2x more time on EHR documentation than seeing patients (AMA, 2024). For solo practices, DrChrono and Kareo/Tebra lead on cost and workflow fit. For small groups, athenaOne and ModMed. Off-the-shelf EHRs hit a ceiling on specialty workflows, data portability, and built-in AI. A custom EHR on Medplum delivers in 60, 120 days and typically pays back inside 18, 24 months. Includes five questions to ask before signing any EHR contract.
The average physician spends 2 hours on EHR work for every 1 hour with patients. That’s not a workflow inefficiency. It’s a design problem baked into most off-the-shelf systems.
I’ve spent the last decade working with independent practices, rural hospitals, and specialty clinics. The question I hear most isn’t “which EHR is best?” It’s “why does picking an EHR feel like choosing between compromises?”
The answer: most commercial EHRs were designed for large health systems, not the economics or workflows of a private practice. They charge enterprise prices, demand enterprise implementation timelines, and leave specialists waiting months for features that don’t fit their workflow.
Here’s what matters when you’re evaluating EHRs as an independent practice owner:
- Billing and clinical modules actually talk to each other. When they don’t (and in many EHRs, they’re still separate products built by different teams), you end up exporting Excel sheets and building Airtables just to understand your own financials.
- Specialty customization costs what it says it costs. Not $50K in hidden “configuration” fees after you’ve already signed the contract.
- Your data is portable when you leave. Not locked into proprietary formats or locked behind per-API-call fees.
- AI is baked in, not bolted on. Most EMRs add AI to an old system like remodeling a 1970s house. You end up with a kitchen from 2025 and plumbing from 1995.
- FHIR APIs actually exist. By 2026, every EHR should support FHIR R4 APIs aligned to the ONC’s USCDI v3 mandate. If your vendor is vague about this, they’re not ready for 2026.
If none of the off-the-shelf options fit your workflow, there’s another path. We’ll get to that. Let’s start with what’s actually available.
I. Why Do EHR Decisions Feel So Hard for Private Practices?
The burden of EHR work in medicine has become absurd. According to the American Medical Association, physicians now spend twice as much time on EHR documentation as they do seeing patients. For a solo practice, that means you’re either burning out fast or hiring a full-time documentation specialist just to keep up.
But here’s what most EHR comparison sites won’t tell you: that burden is not equally distributed across all EHRs. Some systems were built to minimize provider friction. Others were built to maximize billable events and data collection, for the vendor’s use.
In a private practice, you don’t have an IT department to absorb that friction. You don’t have a chief medical information officer to argue with your EHR vendor. You don’t have time to wait 18 months for an implementation or 6 months just to get the billing module talking to the clinical module.
What you have is a practice that needs to move fast, bill cleanly, and let you focus on patients instead of screens. When that’s not what your EHR is built for, that’s when the compromises start.
II. How Did We Evaluate These EHRs?
I looked at each system through the lens of what a private practice actually needs on day one:
- Billing and clinical integration. If your charge capture, coding, and invoicing don’t live in the same ecosystem, you’re building manual workflows. That’s not scalable.
- Specialty workflow flexibility. Can you customize the templates, the data model, and the automation rules to match your practice’s specific workflow? Or does the vendor force you into a template designed for dermatology when you’re a cardiology group?
- FHIR R4 API support. Starting in 2026, the ONC’s 21st Century Cures Act rule requires all EHRs to support FHIR R4 APIs aligned to USCDI v3 data classes (89 FR 1192). If your EHR doesn’t have this roadmap now, they’re not serious about staying compliant.
- Transparent pricing per provider. Not per organization, per click-through, or “contact sales.” Per provider per month, so you can budget.
- Realistic implementation timeline. Weeks or months, not 18-month Epic rollouts or vaporware promises from vendors who’ve never implemented their own product at a small practice.
- Human support that knows small practices. Not a ticketing system where you wait 72 hours for a response.
III. What’s the Best EHR for Solo and 1-3 Physician Practices?
These four consistently perform well for small independent practices: low implementation lift, transparent pricing, and billing that doesn’t require a separate vendor.
DrChrono | Best for: solo + concierge | ~$199/mo
iPad-native charting, built-in RCM, FHIR-enabled API. Black Book Research (2024) ranked DrChrono #1 for ambulatory small practice usability in primary care. Telehealth is built in, not an add-on. Limitation: support is inconsistent above 5 providers.
Kareo / Tebra | Best for: high billing complexity | ~$150/mo
Strongest billing engine in this tier. KLAS Research (2023) gave Tebra 78.4/100 for small-practice ambulatory, above the category average. Limitation: Clinical and billing modules are still partially siloed post-merger.
Practice Fusion | Best for: price-sensitive primary care | $149/mo
Cheapest full EHR in this tier. KLAS (2023) scored it 64.8/100 for usability. Not for anyone with complex specialty workflows.
SimplePractice | Best for: behavioral health | $29-99/mo
Practice management built specifically for therapy workflows. Strong HIPAA compliance. Not the right tool if you need lab integration or e-prescribing.
| System | Best for | Price/provider | FHIR R4 | Billing integrated |
|---|---|---|---|---|
| DrChrono | Concierge / mobile-first | $199/mo | Yes | Yes |
| Kareo / Tebra | High-billing complexity | $150/mo | Yes | Partial |
| Practice Fusion | Price-sensitive primary care | $149/mo | Yes | Basic |
| SimplePractice | Behavioral health | $29/mo | Limited | Yes |
Not Sure Which Fits Your Workflow?
IV. What’s the Best EHR for Small Group Practices (4-10 Physicians)?
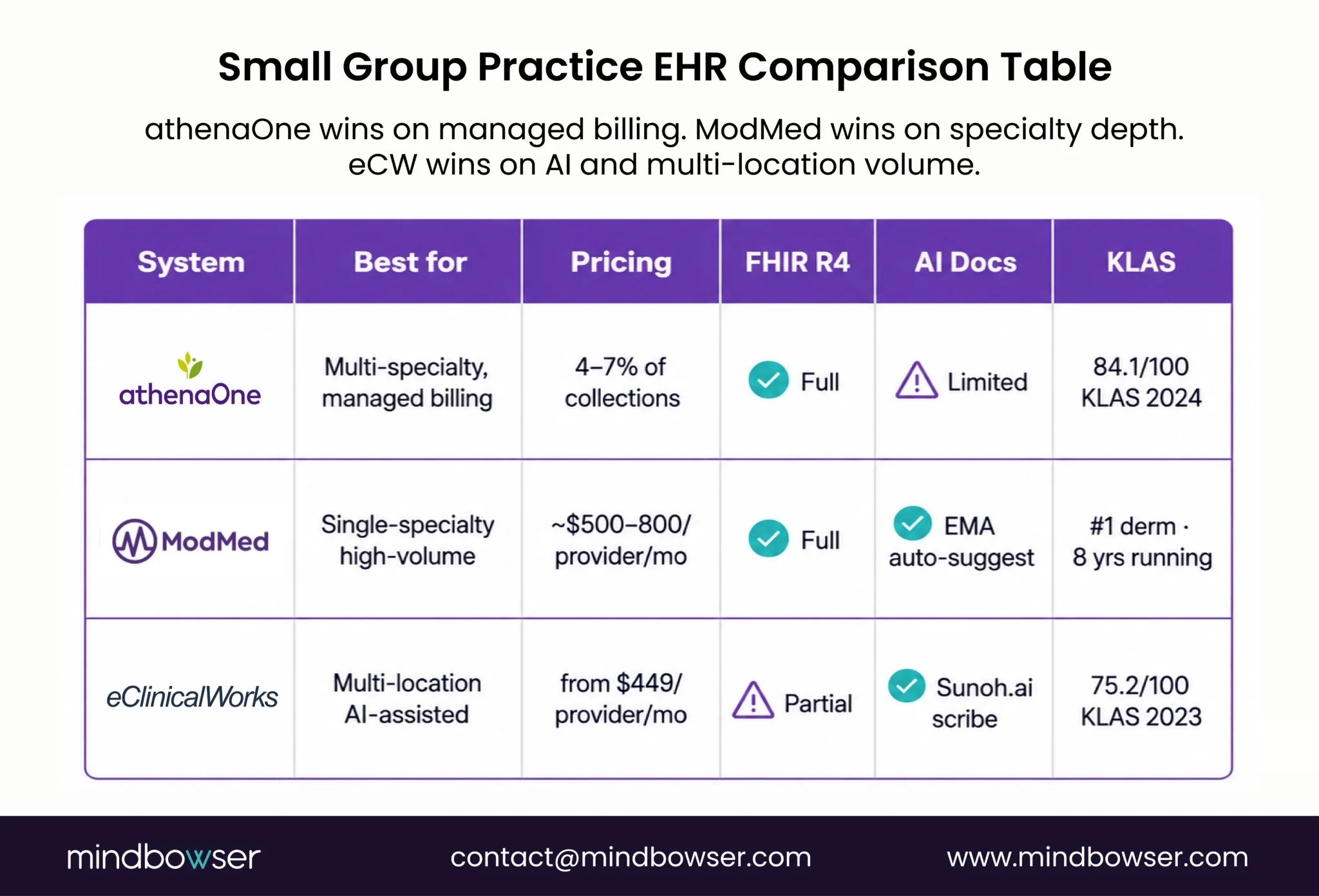
Athenahealth (athenaOne) | Best for: multi-specialty, managed billing | % of collections (4-7%)
KLAS Research (2024) ranked athenaOne #2 for small-to-mid ambulatory EHR, 84.1/100. Strong FHIR R4 API and app marketplace. Limitation: Percentage pricing works against you as revenue grows; clinical template customization is limited.
ModMed (Modernizing Medicine) | Best for: specialty practices | $500-800/mo
Purpose-built for high-throughput specialties. KLAS (2024) ranked ModMed #1 for dermatology EHR for the 8th consecutive year. Billing, coding, and templates are genuinely unified. Limitation: expensive, not for primary care.
eClinicalWorks (eCW) | Best for: multi-location AI-assisted | $449/mo
180,000 providers as of 2024. AI scribe (Sunoh.ai) reduces documentation time. KLAS (2023): 75.2/100. Limitation: legacy architecture, less open API ecosystem.
| System | Best for | Pricing | FHIR R4 | AI documentation |
|---|---|---|---|---|
| athenaOne | Multi-specialty, managed billing | % of collections | Yes | Limited |
| ModMed | Single-specialty high volume | Per-provider custom | Yes | Yes (EMA) |
| eClinicalWorks | Multi-location AI-assisted | $449+/mo | Partial | Yes (Sunoh.ai) |
V. Where Do Standard EHRs Fall Short for Specialty Practices?
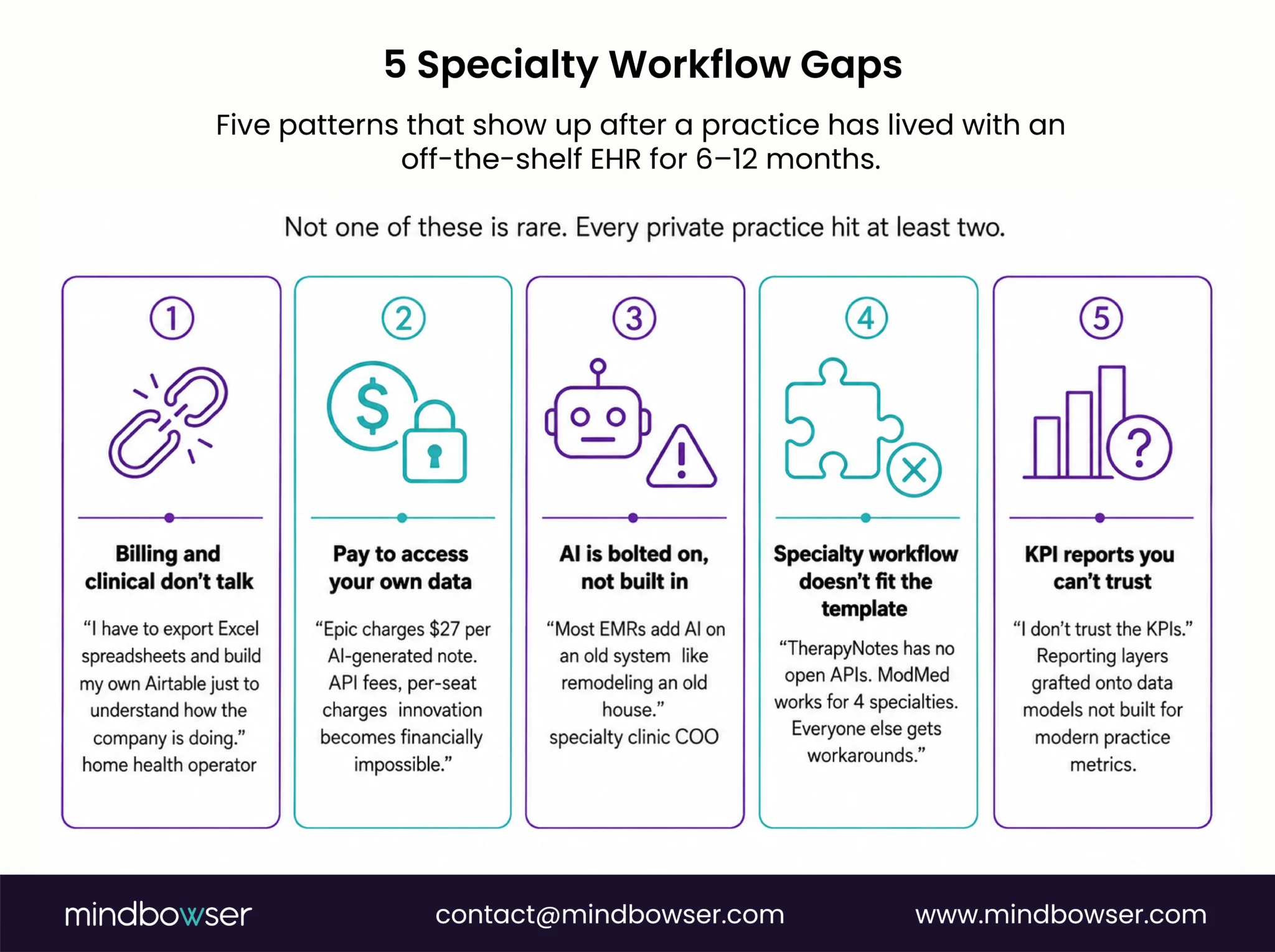
Here’s the pattern I see repeatedly. A practice picks one of the EHRs above, gets through implementation, and six months in, hits a wall that no amount of configuration fixes.
The billing and clinical modules still don’t talk to each other. “I have to export Excel spreadsheets and build my own Airtable just to make sense of how the company is doing.” That’s a direct quote from a home health operator who had been on a mid-market EHR for three years. Not a fringe case. A standard one.
The vendor charges for access to your own data. Integration fees, API call fees, and per-seat charges for every new tool you connect. Epic charges $27 per AI-generated note (cited in the AMA’s 2024 physician satisfaction report). For a specialty group trying to integrate its own AI tools, that makes innovation financially impossible.
AI is bolted on, not built in. “Most EMRs add AI on an old system like remodeling an old house, adding a kitchen, adding a bedroom.” That’s from a specialty clinic COO evaluating AI features from legacy vendors. The ambient scribe works. The underlying system was designed in 2003.
The specialty workflow doesn’t fit the template. TherapyNotes is a closed system with no open APIs, a direct limitation named by a mental health network CEO scaling to 13 clinics, who ended up choosing a custom build instead.
Custom reports are inaccurate. “I don’t trust the KPIs” is not a user error. It’s what happens when reporting layers are grafted onto data models that weren’t designed to surface the metrics a modern practice actually needs.
If any of those sound familiar, the issue isn’t which EHR you pick. It’s that the off-the-shelf category has a ceiling, and you may be hitting it.
VI. When Does Building Your Own EHR Make More Sense?
This isn’t the default recommendation. For most 1-5 physician practices, one of the systems above will do the job at a price that makes sense.
But there’s a real segment of private practice owners for whom custom EHR development is the sharper move. It’s not about budget. It’s about fit.
The pain: Your specialty workflow doesn’t map to any vendor’s template. Billing rules are specific enough that every off-the-shelf system needs expensive configuration that still doesn’t get you to 100%. You want AI in clinical workflows, not pay per-note for a vendor’s add-on.
What’s already built:
For a specialty private practice, we built a full AI-native EHR on Medplum in under 90 days: 70% reduction in provider documentation time, 60% drop in post-visit task delays, and 50% increase in patient interaction through an AI inbound assistant. That’s not a feature upgrade. It’s a different category of tool.
For BirthModel, we built a custom obstetric prediction module inside Epic via SMART on FHIR: 15% delivery rate improvement, 76% fewer coding denials.
We’ve also built a national-scale EHR for an entire country’s public health system at $131K. Custom doesn’t have to mean enterprise-only pricing.
Pre-built components on every build:
- PHISecure: HIPAA-compliant data handling layer. Production-ready. Learn more
- AI Medical Summary: Embedded ambient documentation, no third-party subscription. Learn more
If your practice needs a healthcare software development partner who understands the clinical layer as well as the engineering layer, that’s the distinction that matters.
| Factor | Off-the-shelf EHR | Custom EHR (Mindbowser) |
|---|---|---|
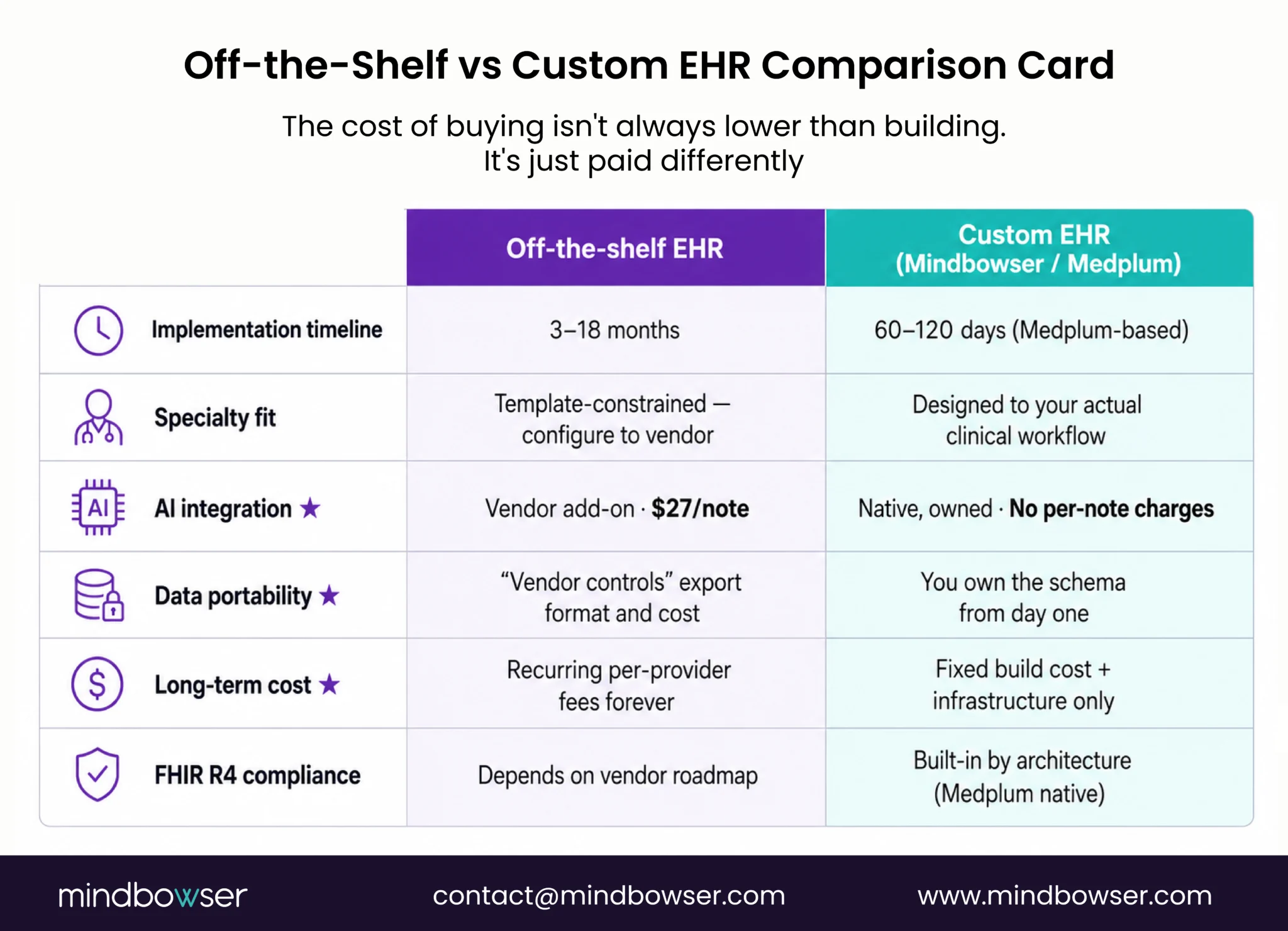
| Implementation timeline | 3-18 months | 60-120 days (Medplum-based) |
| Specialty fit | Template-constrained | Fully designed to workflow |
| AI integration | Vendor add-on (per-note fees) | Native, owned |
| Data portability | Vendor-controlled | You own the schema |
| Long-term cost | Recurring per-provider fees | Fixed build + hosting |
| FHIR R4 compliance | Depends on vendor | Built-in by architecture |
VII. What Should You Ask Before Signing an EHR Contract?
1. Does it support FHIR R4 APIs, and what does API access actually cost?
Under ONC’s HTI-1 rule (89 FR 1192), all certified EHRs must support FHIR R4 APIs aligned to USCDI v3. “Supports FHIR” and “gives you free API access” are different things. Ask: is API access in the base plan, or a separate fee?
2. Are billing and clinical modules the same product or separate acquisitions?
Ask to see the data flow from clinical encounter to submitted claim, end-to-end, live, in the demo. Not a slide. The screen.
3. What does specialty customization cost, and who controls it?
“Highly configurable” usually means “our team builds it for you, for a fee.” Ask the actual cost to add a custom template, a custom data field, and a custom report. If the answer involves a statement of work, you don’t own the configuration. They do.
4. What’s your data ownership model when you leave?
What format does your data export in? How long does it take, and what does it cost? Any vendor who can’t answer this in 60 seconds is telling you how they think about lock-in.
5. What’s the AI roadmap, and who pays for it?
“We have AI” in 2026 can mean anything from a built-in ambient scribe to a third-party integration at $27 per note. Ask: Is AI documentation in the base price? Who owns the clinical data used to improve it?
Built for Healing
The best EHR for a private practice is not the one with the longest feature list. It is the one that reduces documentation burden, supports clean billing, protects your data, and fits the way your clinicians actually work. For many solo and small-group practices, a proven off-the-shelf EHR is enough. But when specialty workflows, AI, interoperability, or data ownership become central to growth, custom EHR development becomes less of a technology decision and more of a healing decision: giving physicians time back, giving staff fewer workarounds, and giving patients a smoother care experience.
DrChrono and SimplePractice score highest in their categories. DrChrono has the lowest learning curve for primary care or concierge medicine. SimplePractice wins for behavioral health.
Budget $150-$500/month per provider for commercial EHR. Add implementation costs ($5K-$50K) and specialty module fees. Custom EHR development starts higher ($60K-$200K) but eliminates recurring fees and gives you full data ownership.
Rarely, and for good reason. Cost, complexity, and minimum viable implementation size all make it wrong for independent practice.
KLAS Research (2024): athenaOne, eClinicalWorks, and Kareo/Tebra lead adoption among independent practices. ModMed dominates in dermatology and ophthalmology. TherapyNotes leads in behavioral health, though its closed API architecture is driving multi-site practices toward custom builds.
More often than expected. A Medplum-based build delivers in 60-120 days. If your current EHR costs $600/month per provider plus workaround staff time, a custom build often pays for itself in 18-24 months.


