



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
60-80% of healthcare IT budgets go to maintaining legacy systems. Big-bang EHR replacements fail 70%+ of the time. The strangler fig pattern — wrapping your legacy system with a FHIR API layer and incrementally replacing components — is the lowest-risk modernization strategy. Here are 4 strategies ranked by risk, real modernization metrics (30TB migrated, 30-40% cost reduction), and the regulatory deadlines (USCDI v3, HTI-4) that make modernization mandatory for non-FHIR systems.
The VA’s EHR modernization program is the cautionary tale nobody in healthcare IT can ignore. Billions spent. Years of delays. A GAO report (2026) calling for “critical actions needed to support accelerated system deployments.” Sites going live after 3-year resets.
That’s what big-bang EHR modernization looks like at enterprise scale.
Meanwhile, 500 million health records have been exchanged through TEFCA as of February 2026 — up from roughly 10 million in January 2025. Interoperability isn’t a future requirement. It’s happening now. And legacy EHR systems that can’t expose FHIR R4 APIs are being left behind.
If you’re a CIO or VP IT at a mid-market health system running a 5-10 year old EHR, you already know modernization is coming. The question is which strategy minimizes risk while getting you to a modern architecture.
I. How Do You Know Your EHR Needs Modernization?
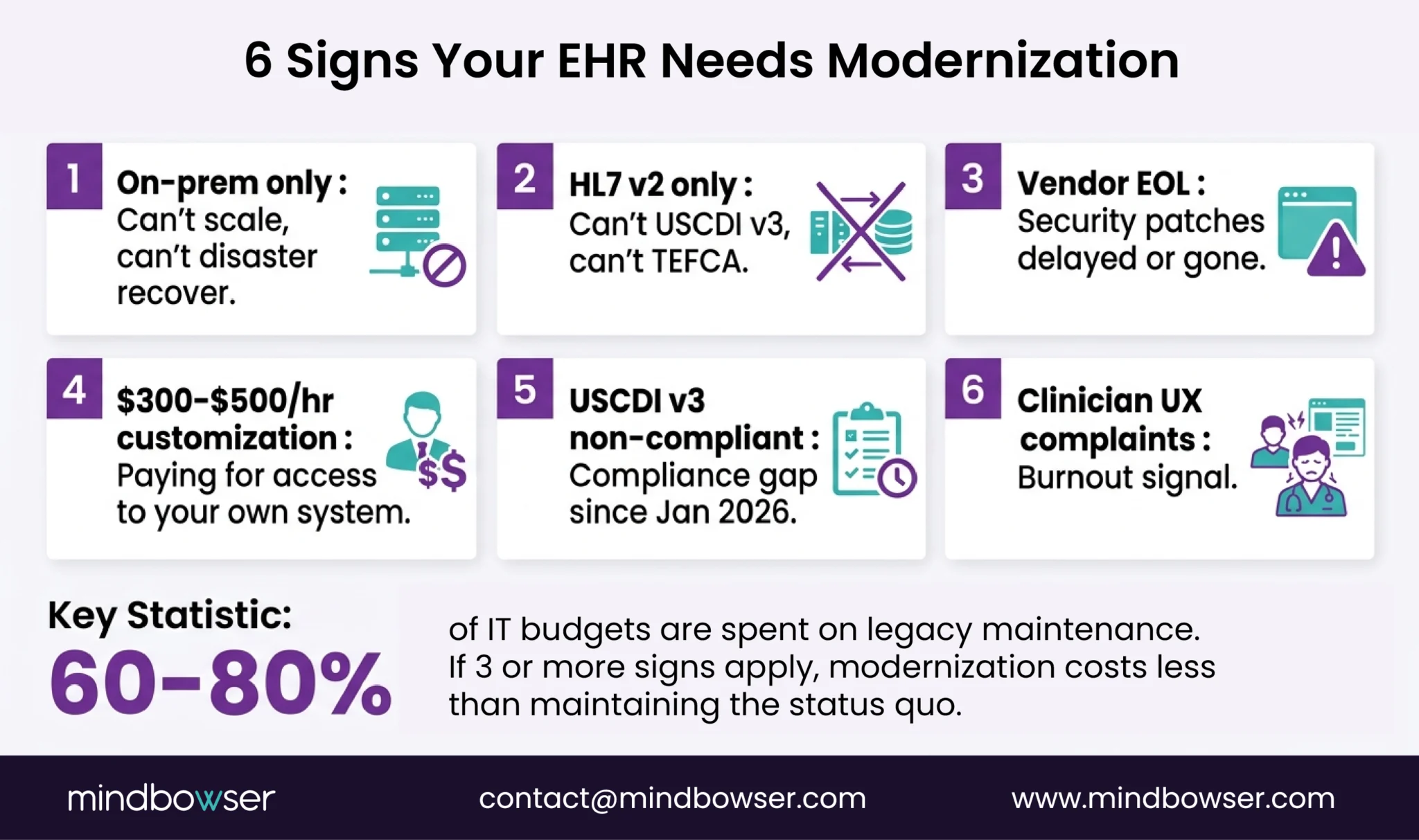
Six signs. If 3 or more describe your situation, modernization isn’t a strategic initiative — it’s an operational necessity.
- On-premise only, no cloud option. Your EHR runs on servers in your data center (or a closet). No cloud deployment path. Scaling means buying hardware. Disaster recovery means a second data center.
- HL7 v2 only, no FHIR APIs. Your system sends ADT messages and ORU results, but can’t expose patient data via FHIR R4 APIs. In 2026, that means you can’t participate in TEFCA, can’t connect modern applications, and can’t meet USCDI v3 requirements.
- Vendor no longer supports your version. End-of-life or extended support. Security patches are delayed or unavailable. You’re running on a platform the vendor has stopped investing in.
- Customization requires vendor professional services at $300-$500/hour. Every template change, workflow modification, or report request goes through the vendor’s professional services team at enterprise rates. You’re paying for access to modify your own system.
- USCDI v3 compliance is not possible on current platform. USCDI v3 became mandatory January 2026. It requires 16 data classes, ~94 data elements, FHIR US Core 6.1.0, and SMART v2. If your platform can’t support this, modernization is a compliance event, not a choice.
- Clinicians complain about speed and UX. Slow load times. Excessive clicks for simple tasks. Mobile access either non-existent or barely functional. These complaints are burnout signals. The EHR-burnout link is settled science.
The budget signal: Industry benchmarks place legacy system maintenance at 60-80% of total healthcare IT spend estimates 40% of IT budgets go to technical debt. If most of your IT budget is keeping the old system alive, you’re paying maintenance costs that exceed the cost of modernization.
II. What Are the 4 EHR Modernization Strategies?
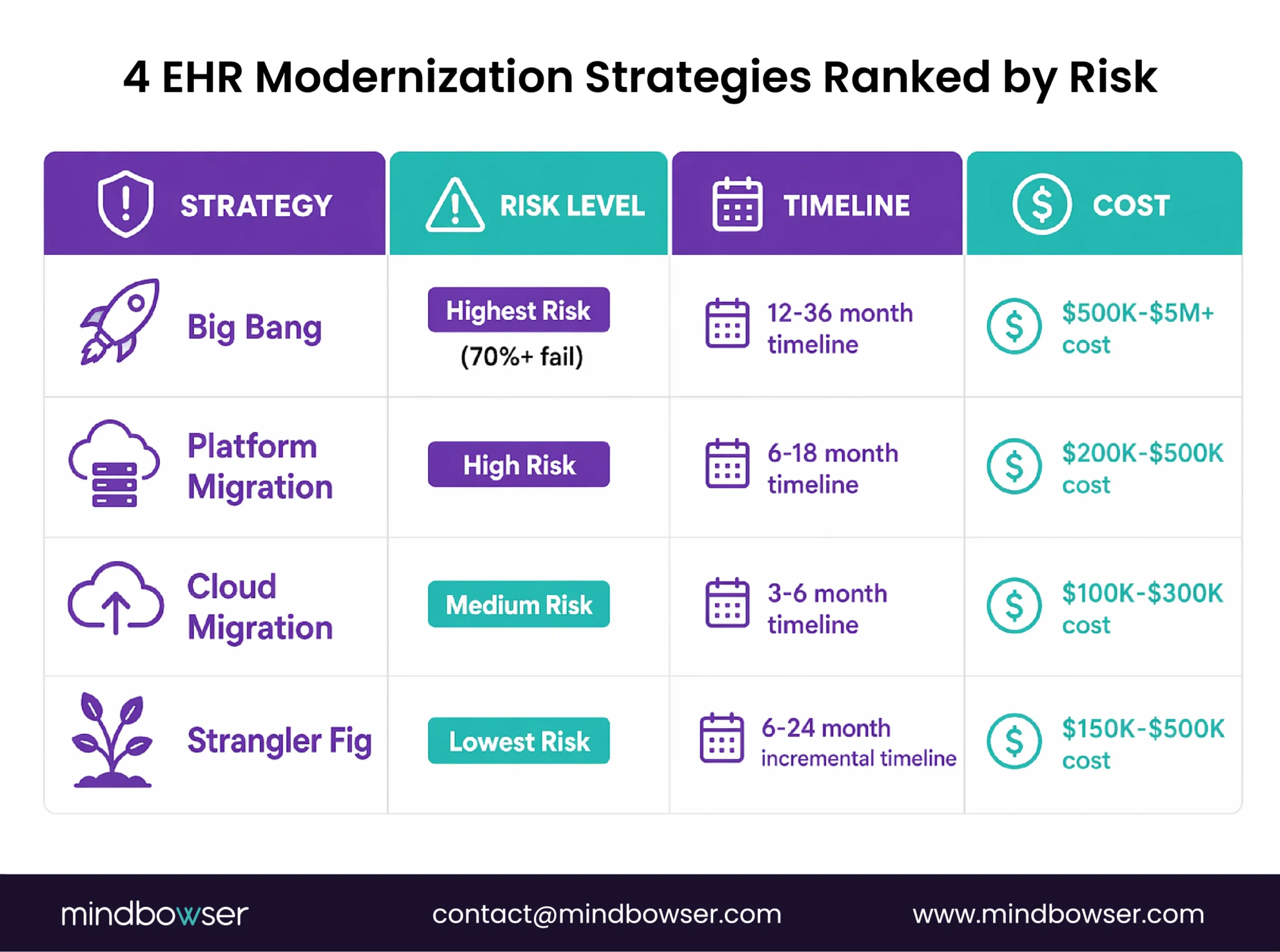
Four approaches, ranked from highest risk to lowest.
A. Strategy 1: Big Bang Replacement
Replace everything at once. New system, new data model, new workflows. Hard cutover.
- When it works: Legacy system is truly dead (vendor gone, no support, security risks unmanageable)
- Why it usually fails: 70%+ of big-bang modernization projects fail or exceed budgets. Clinical continuity during the cutover is the biggest risk. If something breaks, patients are affected.
- The VA is the poster child for this risk.
B. Strategy 2: Headless Platform Migration
Move from legacy to a modern headless EHR platform (Medplum, Canvas, Oystehr). Rebuild the frontend and clinical logic on the new platform. Migrate data.
- When it works: You want a modern FHIR-native architecture AND are willing to rebuild clinical workflows
- Risk: Medium — you’re rebuilding, not just moving. But the platform handles infrastructure, so you’re rebuilding on a solid foundation.
- See our headless EHR comparison for platform selection guidance.
C. Strategy 3: Cloud Migration
Same application, new infrastructure. Move from on-premise to AWS/Azure/GCP. The clinical software doesn’t change. The hosting, database layer, networking, and cost structure do.
- When it works: Your application is viable, but your infrastructure is the bottleneck (cost, scaling, reliability)
- Our proof: We migrated a multi-specialty healthcare platform from Azure to AWS — 30TB of data, 180 production databases, 30-40% infrastructure cost reduction, latency improved from 120ms to 80ms, zero clinical downtime. Full migration details.
Cloud migration is “enough” when your application architecture is sound but your infrastructure isn’t. If the application itself is the problem (outdated data model, no FHIR support, poor UX), cloud migration just moves the problem to a different data center.
D. Strategy 4: Strangler Fig (Recommended)
The lowest-risk strategy for most legacy EHR systems. We recommend this as the default approach unless there’s a specific reason to choose otherwise.
Build a Custom EHR
III. How Does the Strangler Fig Pattern Work for EHR?
The strangler fig is a tree that grows around an existing tree, eventually replacing it. The software pattern does the same: gradually replace legacy components while keeping the system running.
4 steps, zero downtime:
A. Step 1: Wrap Legacy with a FHIR API Layer
Build a FHIR R4 API layer on top of your legacy EHR. The legacy system continues running. The API layer translates legacy data formats (HL7 v2, proprietary databases) into FHIR resources.
- Legacy system: unchanged
- New applications: connect through FHIR APIs, not directly to the legacy database
- USCDI v3 compliance: achieved at the API layer, even if the legacy system doesn’t natively support it
- This is “Type 5: FHIR API Wrap” from our data migration guide. Timeline: 2-4 months. Cost: $50K-$150K.
B. Step 2: Build New Modules on Modern Stack
With the FHIR API layer in place, build new clinical modules on a modern architecture – Medplum, custom React frontend, or a headless platform. These new modules read from and write to the FHIR API layer.
- New scheduling module replaces legacy scheduling
- New clinical documentation module with AI-native capabilities
- New patient portal with mobile access
- Each module is independent. If one has issues, the legacy system is still running.
C. Step 3: Route Traffic to New Modules
As new modules reach production quality, route users to them. The legacy system handles everything the new modules don’t cover yet. Over time, more and more functionality moves to the modern stack.
- Gradual user migration (department by department, or feature by feature)
- A/B testing possible: some users on the new system, some on legacy system
- Clinical continuity is maintained throughout – patients never experience a “switchover” moment
D. Step 4: Decommission Legacy Components
When all critical functionality has been migrated to the modern stack, the legacy system moves to read-only (for historical data access and audit trails), then full decommission.
- Keep legacy in read-only for a minimum of 90 days (longer for compliance)
- Migrate remaining historical data to the FHIR data store
- Decommission legacy infrastructure
Why strangler fig works for clinical systems: The #1 risk in EHR modernization is clinical continuity. Patients don’t stop getting treated during a system upgrade. The strangler fig ensures the old system runs until the new one proves itself in production. No hard cutover. No “go-live weekend” where everything has to work. Incremental risk instead of concentrated risk.
Evaluating modernization strategies for your legacy EHR? Tell us about your current system, and we’ll map the approach — strangler fig, cloud migration, platform migration, or a combination.
IV. When Is Cloud Migration Enough vs Full Modernization?
This is the decision most CIOs struggle with. The answer depends on where your technical debt lives.
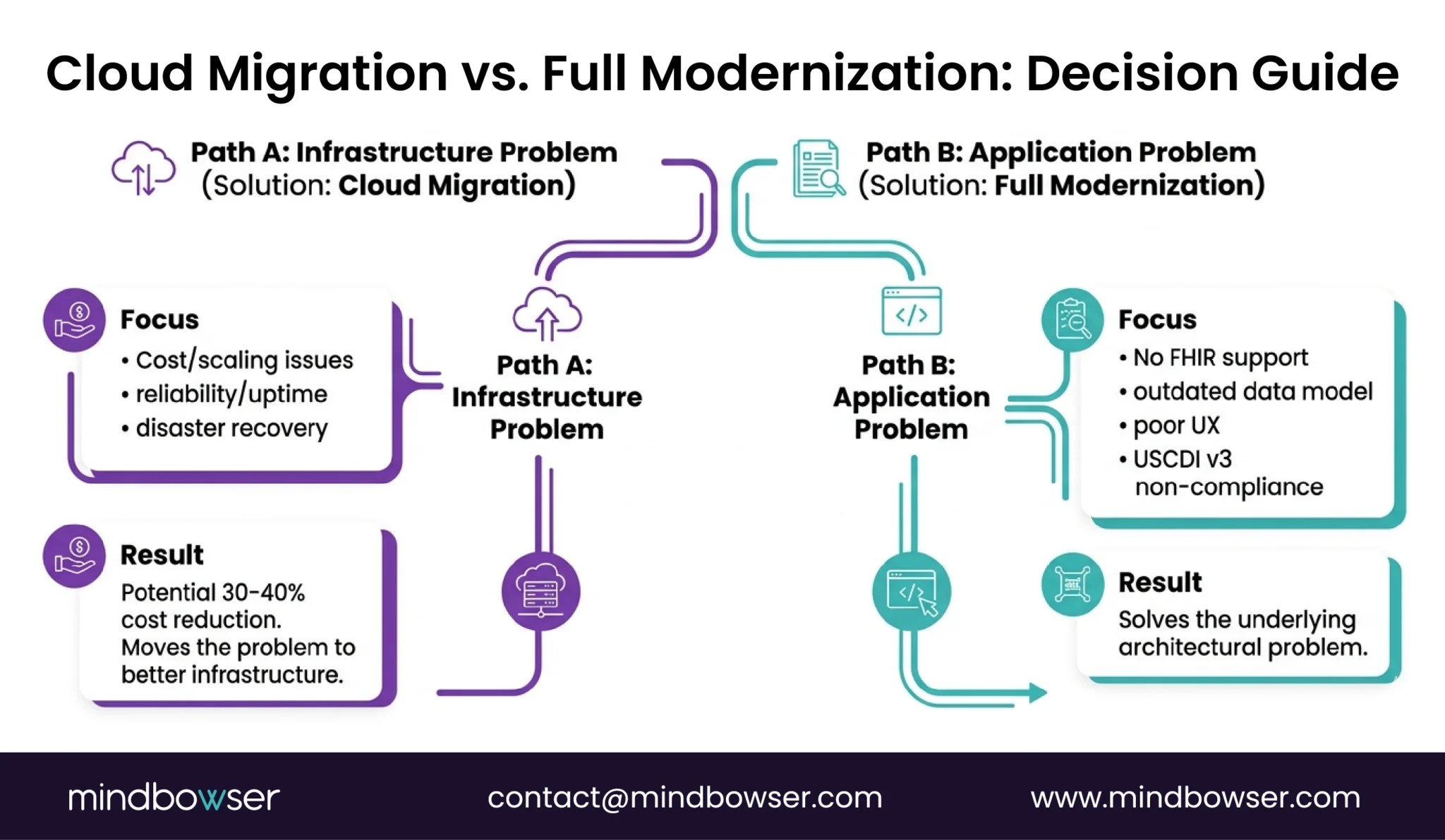
- Our cloud migration in numbers: A multi-specialty healthcare platform needed to move from Azure to AWS. The application was sound — the infrastructure was the bottleneck.
- 30TB of data across 180 production databases
- Latency: 120ms -> 80ms (33% improvement)
- Cost: 30-40% infrastructure reduction through Reserved Instances, EC2 Spot, and S3 Intelligent-Tiering
- Downtime: Zero
The platform kept running throughout. That’s the cloud migration promise — better infrastructure, same application, no clinical disruption.
V. What Regulatory Deadlines Are Forcing Modernization?
Three deadlines that turn modernization from “should do” into “must do.”
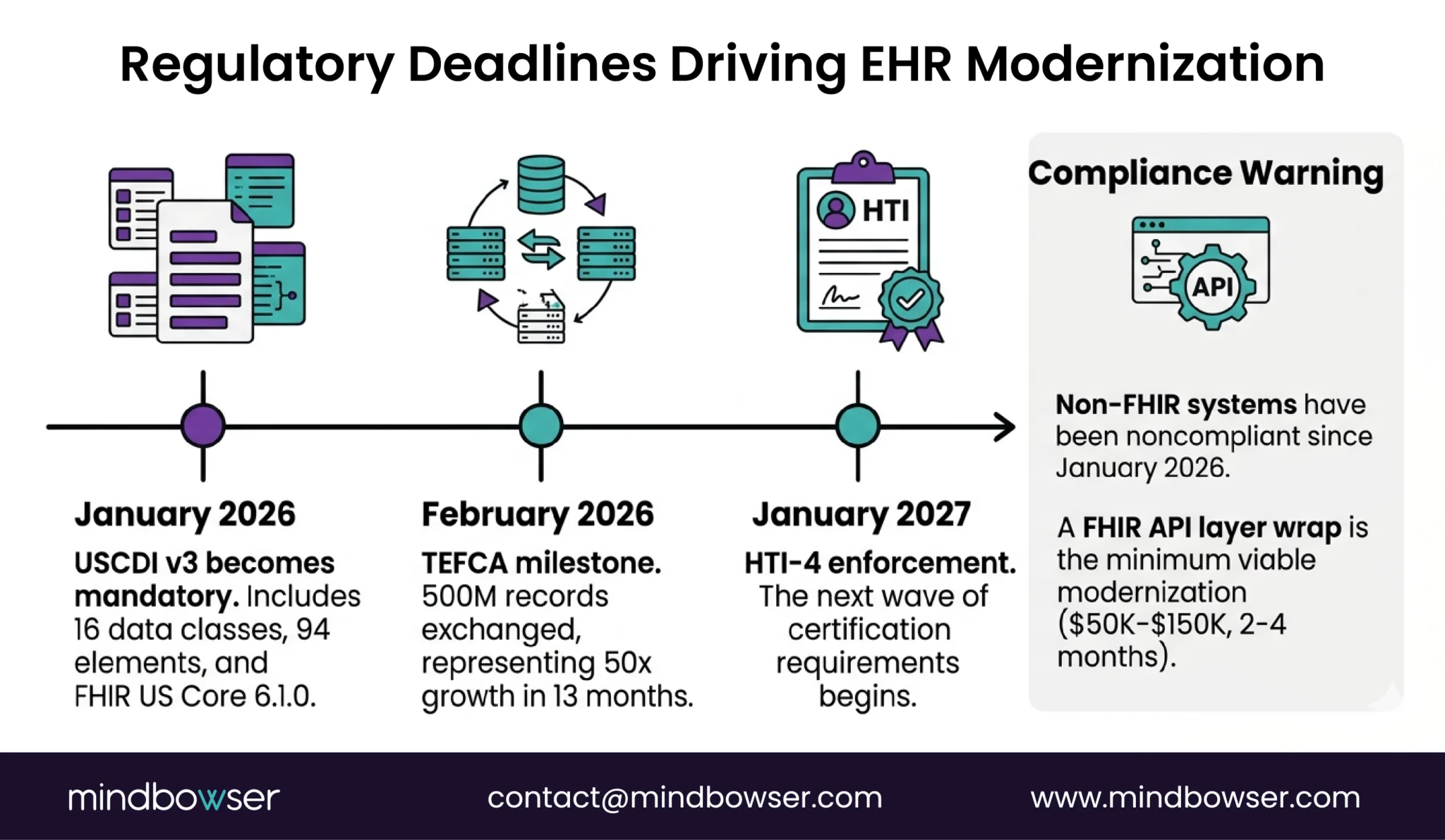
A. USCDI v3 – Mandatory since January 1, 2026
- 16 data classes, ~94 data elements
- FHIR US Core 6.1.0 required
- If your legacy EHR can’t expose FHIR R4 APIs with v3 data elements, you’re non-compliant
B. HTI-4 – Enforcement begins January 2027
- Next wave of ONC certification requirements
- Medplum is already pursuing HTI-4 certification
- Legacy systems not on the HTI-4 path face increasing certification gaps
C. TEFCA – Interoperability at scale
- 500 million health records exchanged through TEFCA as of February 2026
- Up from 10 million in January 2025 — 50x growth in 13 months
- Systems that can’t participate in TEFCA are excluded from the national interoperability network
- If you can’t exchange data via FHIR, you’re not just behind on compliance. You’re disconnected from the healthcare data ecosystem.
The practical implication: If your legacy EHR doesn’t support FHIR R4 APIs, the strangler fig Step 1 (FHIR API layer wrap) becomes your minimum viable modernization. $50K-$150K and 2-4 months buys you USCDI v3 compliance and TEFCA participation without replacing the underlying system. It’s the fastest path from “non-compliant” to “compliant” while you plan the longer modernization.
Where Does This Leave You?
EHR modernization isn’t optional for non-FHIR systems. The regulatory deadlines are here. The interoperability network is growing 50x per year. And maintaining legacy costs more than modernizing.
Three things worth remembering:
- 60-80% of your IT budget on maintenance is the signal. If most of your spend is keeping the old system alive, the math favors modernization. A strangler fig approach at $150K-$500K is bounded. Legacy maintenance at 60-80% of budget is indefinite.
- Strangler fig over big bang. Every time. Big-bang replacements fail 70%+ of the time. The strangler fig wraps your legacy with FHIR, builds new modules incrementally, and decommissions the old system only after the new one has proven itself in production. Zero downtime. Incremental risk. Clinical continuity maintained.
- USCDI v3 makes Step 1 mandatory for non-FHIR systems. If your legacy EHR doesn’t support FHIR R4 APIs, the minimum viable modernization is a FHIR API layer wrap ($50K-$150K, 2-4 months). That’s not the full modernization — it’s the compliance bridge that buys you time to plan the rest.
Running a legacy EHR that needs modernization? Tell us about your current architecture and we’ll map the strategy — strangler fig, cloud migration, platform migration, or a combination based on where your technical debt lives.
When 3+ of these apply: (1) On-premise only with no cloud path, (2) HL7 v2 only with no FHIR APIs, (3) vendor no longer supports your version, (4) customization costs $300-$500/hr through the vendor, (5) can’t meet USCDI v3 requirements, (6) clinicians complain about speed and UX. The budget signal is definitive: if 60-80% of your IT spend is maintaining the legacy system, modernization costs less than continuing. USCDI v3 (mandatory since January 2026) makes modernization a compliance requirement for any system without FHIR R4 APIs.
By strategy: – FHIR API layer wrap (strangler fig Step 1): $50K-$150K, 2-4 months — minimum viable modernization for compliance – Cloud migration (same app, new infra): $100K-$300K, 3-6 months — our client saw 30-40% ongoing cost reduction – Strangler fig full modernization: $150K-$500K, 6-24 months incremental — lowest risk, recommended approach – Headless platform migration: $200K-$500K, 6-18 months — rebuild on Medplum/Canvas/Oystehr – Big bang replacement: $500K-$5M+, 12-36 months — highest risk, 70%+ failure rate Compare to: 60-80% of IT budget annually on legacy maintenance. A bounded modernization investment often pays for itself by reducing the ongoing maintenance bleed. See our full cost guide.
The strangler fig pattern incrementally replaces a legacy EHR while keeping it running. 4 steps: (1) Wrap the legacy system with a FHIR R4 API layer — legacy continues running, new apps connect through FHIR. (2) Build new clinical modules on a modern stack (Medplum, custom React, etc.) that read/write through the FHIR API. (3) Route users to new modules as they’re ready — department by department or feature by feature. (4) Decommission legacy components after the modern system has proven itself in production. The key advantage: zero downtime and zero “go-live weekend.” Clinical continuity is maintained throughout because the old system runs until the new one replaces each function. This is the recommended strategy for most legacy EHR modernizations.

