



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
- RPM is profitable for primary care practices with as few as 25 enrolled patients. At 200 patients, annual revenue reaches $144K-$204K with a 3-5x ROI and 2-3 month break-even (CMS CY2026 PFS).
- The 2026 CMS short-duration codes (2-day monitoring minimum, 10-minute treatment management threshold) lower the bar further.
- You do not need an enterprise IT department, a dedicated RPM coordinator, or a six-figure budget. You need a cellular BP cuff, a patient list, and a billing workflow. The math works at every practice size.
The most common objection I hear from independent practice physicians about RPM is not clinical. It is financial. “We’re five providers with 3,000 patients and no IT department. How do we afford this?”
I had that exact conversation with a managing physician in Ohio last quarter. Five providers, two MAs, one office manager, 2,800 patients, roughly 1,400 with at least one chronic condition. They had been reading about RPM for two years and assumed it was designed for health systems with dedicated IT teams and capital budgets.
We walked through the math on a napkin. Twenty-five hypertension patients on cellular BP cuffs. Platform subscription at $10 per patient per month. Existing MA doing 15-minute monthly check-ins that she was already doing by phone anyway, now documented as 99457 interactive time. Revenue per patient: roughly $105-120 per month. Twenty-five patients: $2,625-$3,000 per month. Annual: $31,500-$36,000. Startup cost for devices and platform: under $5,000.
The managing physician said: “Why did nobody show me this math two years ago?”
That is the conversation this piece is designed to have with every primary care practice that thinks RPM is out of reach.
Can a 5-Provider Practice Actually Afford RPM?
The short answer is yes, and the economics improve at every scale point.
RPM generates approximately $60-85 per enrolled patient per month from the core billing codes (99454 device supply + 99457 interactive communication). The range depends on payer mix, monitoring consistency, and whether the practice captures additional time codes (99458).
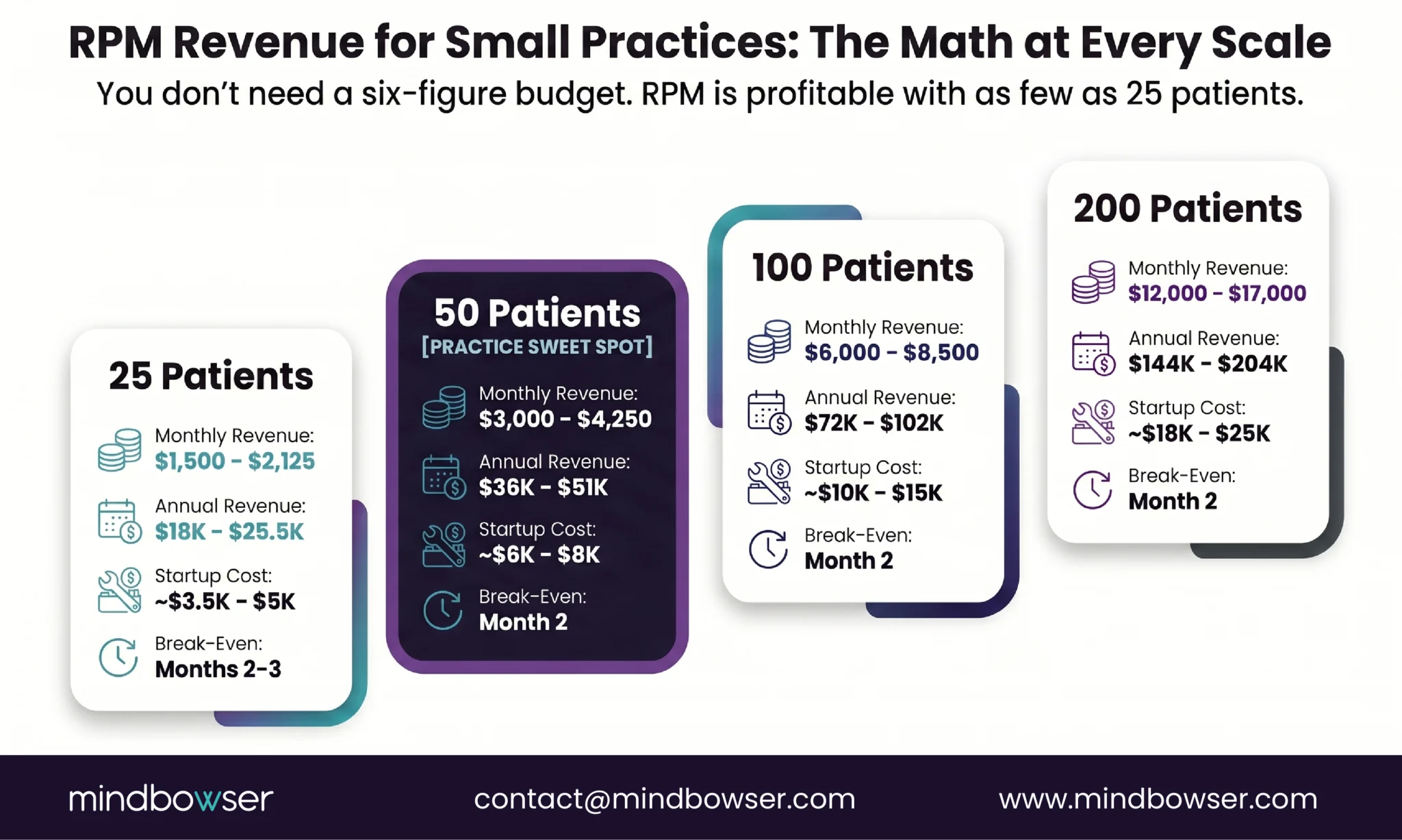
| Enrolled Patients | Monthly Revenue | Annual Revenue | Startup Cost (devices + platform) | Break-Even |
|---|---|---|---|---|
| 25 | $1,500-2,125 | $18,000-25,500 | ~$3,500-5,000 | Month 2-3 |
| 50 | $3,000-4,250 | $36,000-51,000 | ~$6,000-8,000 | Month 2 |
| 100 | $6,000-8,500 | $72,000-102,000 | ~$10,000-15,000 | Month 2 |
| 200 | $12,000-17,000 | $144,000-204,000 | ~$18,000-25,000 | Month 2 |
At 200 patients, published data shows a 4-7x return on technology and staffing investment. But the table above is what matters for a small practice: even at 25 patients, the program generates positive revenue from month two or three.
Now factor in the 2026 CMS changes. The new short-duration code 99445 covers 2 to 15 days of monitoring data per month at approximately $47, lower than 99454 and mutually exclusive with it. For small practices where patients are inconsistent with their monitoring, especially in the first few months, this means more patients generate billable events even when compliance is imperfect. The new 99470 code covers the first 10 minutes of treatment management, down from the previous 20-minute threshold under 99457. Ten minutes is achievable for every patient every month.
The startup cost reality for a 25-patient pilot: cellular BP cuffs at $80-120 per unit ($2,000-3,000 total), RPM platform subscription at $5-15 per patient per month ($125-375/month), and existing staff time (no new hire needed at this scale). Total first-month outlay: under $5,000. Revenue starts flowing in month two.
Which Patients Should You Monitor First?
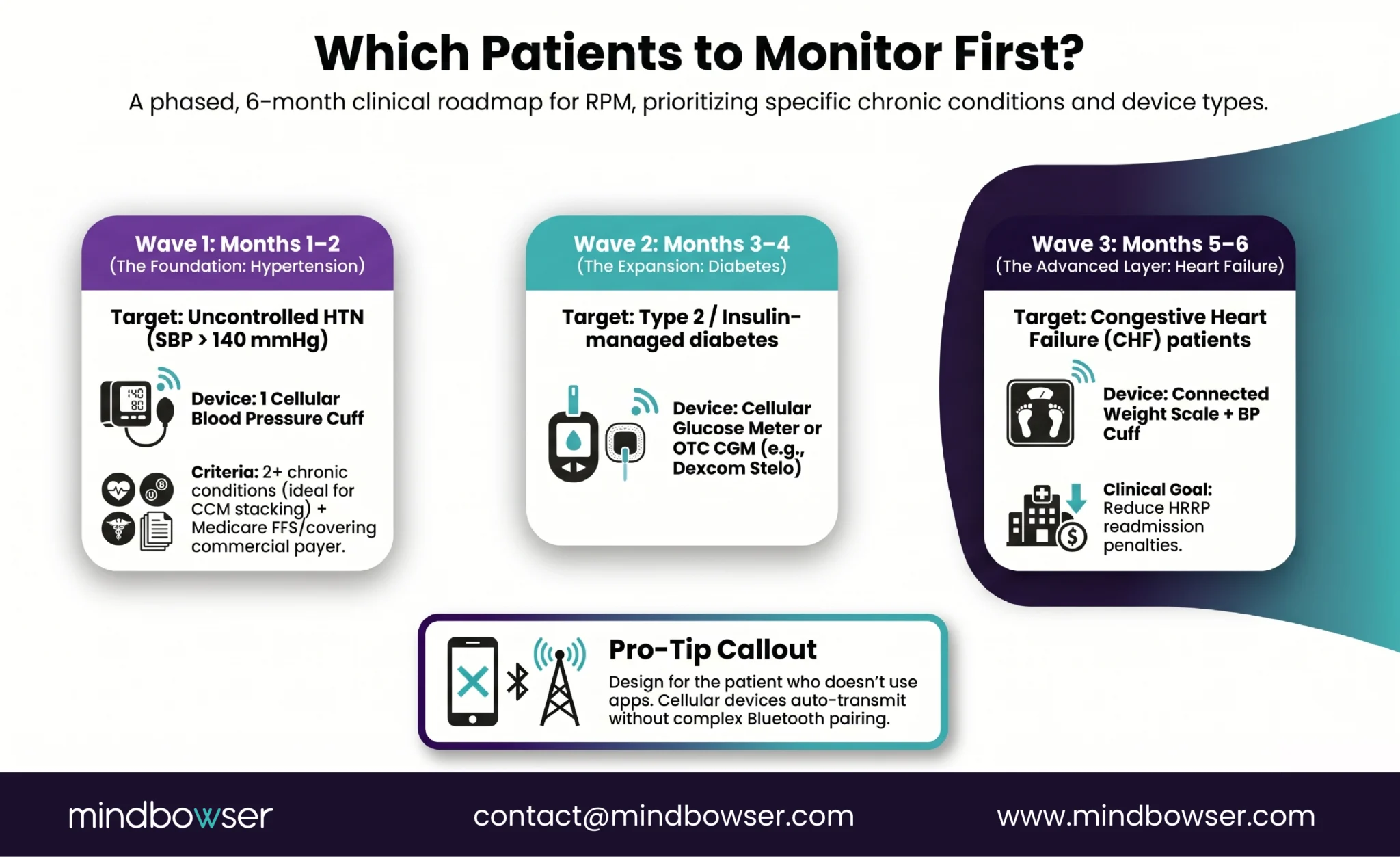
Start with hypertension. It is the largest chronic condition in any primary care panel, uses the simplest device protocol (one BP cuff), and produces the fastest measurable outcomes (blood pressure responds to medication changes within 1-2 weeks).
Your first 25 patients should meet all three criteria:
- Uncontrolled hypertension (SBP consistently above 140 mmHg)
- Two or more chronic conditions (qualifies for concurrent CCM billing, which we covered in our RPM + CCM stacking guide)
- Medicare FFS or a commercial payer that covers RPM (verify before enrolling; UHC excluded chronic hypertension in 2026)
Most 5-provider PCP practices have 200 or more patients meeting all three criteria sitting in their active panel right now. You are not searching for patients. You are selecting the first 25.
Second wave (month 3-4): add diabetes patients. A cellular blood glucose meter or, for insulin-managed patients, a CGM like Dexcom Stelo (OTC, no prescription needed). See our diabetes remote patient monitoring guide for the full CGM integration picture.
Third wave (month 5-6): add heart failure patients (connected scale + BP cuff). See our cardiac remote patient monitoring guide for the HRRP penalty context.
On patient engagement: RPM platform built for elderly care, achieved 90% engagement among elderly users. Their approach was design-first: large buttons, simplified workflows, proactive care manager outreach in the first 14 days. Primary care patients with chronic conditions skew older. Design for the patient who does not use apps, not the one who does.
What Does the Minimum Viable RPM Stack Look Like?
Three components. That is all.
- Device: one cellular BP cuff per patient. Cellular transmits the reading directly over the cell network. No patient phone required. No app to install. No Bluetooth to troubleshoot. The patient puts on the cuff, presses the button, and the reading appears on your dashboard. For a primary care practice without a help desk, cellular eliminates the #1 support burden (BLE pairing failures). Cost: $80-120 per unit. Omron, Tenovi, and BodyTrace all make cellular-connected cuffs.
- Platform: off-the-shelf RPM software. Prevounce, PrevounceTimeDoc, Rimidi, HealthArc, SmartClinix, and ChartSpan all serve the small-practice segment. Monthly subscription at $5-15 per patient. Features to require: alert dashboard, 99457 time tracking, billing code submission, and ideally EHR integration with your system (Epic, Athena, eClinicalWorks). Do not over-buy. You need a dashboard that shows which patients have out-of-range readings and a timer that tracks your interactive minutes.
- Staff: your existing MA or care coordinator. At 25-50 patients, RPM does not require a new hire. The MA who already calls patients about lab results and medication refills now also reviews BP readings and documents the interaction. Fifteen to twenty minutes per patient per month is the 99457 threshold. That is one call.
Total monthly operating cost at 50 patients: $250-750 (platform subscription) + $0 incremental staffing = $250-750. Revenue at 50 patients: $3,000-4,250. Net margin: $2,250-4,000 per month from an investment smaller than your monthly supply bill.
The EHR integration is not required to launch. RPM data should eventually flow into the patient chart, and most platforms offer standard integrations with Epic, Athena, and eClinicalWorks. But you can launch without it. The dashboard is sufficient for the first 90 days. Integrate the EHR after the program proves its revenue.
Discuss Which RPM Platform and Device Configuration Fits Your Practice
How Do the 2026 CMS Changes Help Small Practices?
The 2026 Physician Fee Schedule changes were, in my assessment, designed with practices like yours in mind.
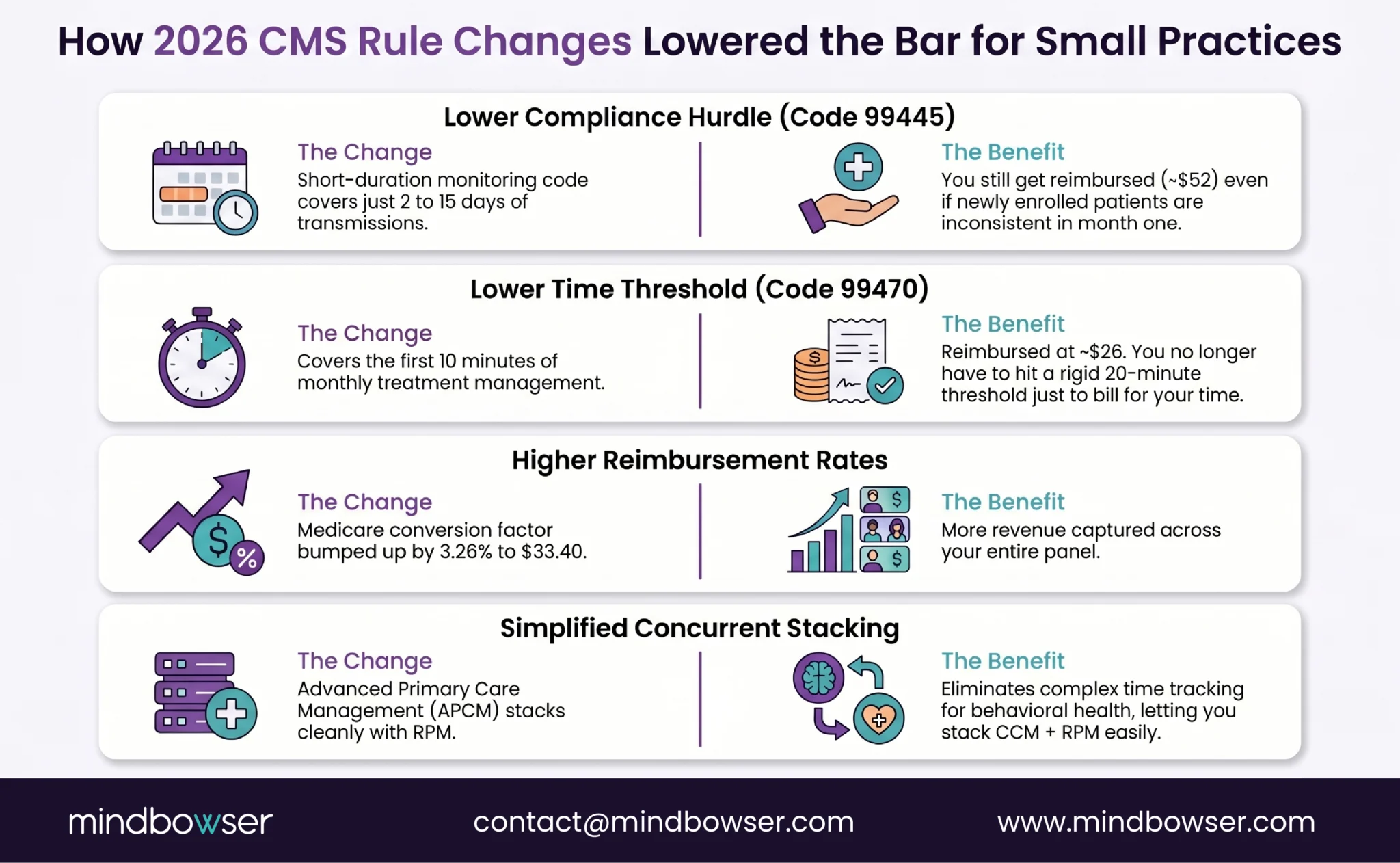
- Short-duration RPM code (99445). Previously, a patient had to transmit device data for at least 16 days within 30 days to bill 99454. Sixteen days is a high bar for newly enrolled patients who are still learning the device. The new 99445 code covers 2 to 15 days of data at approximately $47, lower than 99454 and mutually exclusive with it. For a primary care practice enrolling patients who are inconsistent in the first month, this is the difference between billable and non-billable.
- Lower time threshold (99470). The new code covers the first 10 minutes of treatment management services per month, reimbursed at approximately $26. The existing 99457 requires 20 minutes. For a small practice where every minute matters, 10 minutes of documented interaction is achievable for every patient every month. You bill 99470 when you hit 10 minutes and 99457 when you hit 20.
- Conversion factor increase. CMS raised the Medicare conversion factor to $33.40 (up from $32.35 in 2025), a 3.26% increase. Modest per code, meaningful across a patient panel.
- FQHC and RHC billing (expanded 2024). If your practice is a Federally Qualified Health Center or Rural Health Clinic, RPM is now fully billable under Medicare. This was not the case before the 2024 PFS expansion.
- APCM (new 2026). Advanced Primary Care Management is an alternative to CCM that eliminates time tracking for Behavioral Health Integration and Collaborative Care Model add-on services. For a small practice without dedicated billing staff, APCM simplifies concurrent program management. RPM stacks with APCM.
The net effect: every barrier that small practices cited in 2024 (monitoring threshold too high, time requirement too demanding, billing complexity too great) has been lowered by the 2026 rules.
Off-the-Shelf or Custom: What Makes Sense at Your Size?
For most primary care practices reading this, the answer is off-the-shelf. And I say that as someone whose company builds custom platforms.
- Under 100 patients: off-the-shelf. Prevounce, TimeDoc, Rimidi, HealthArc, or SmartClinix. Monthly subscription, no development cost, integrated billing, support included. The platform handles device data ingestion, alert routing, time tracking, and code submission. Your job is to enroll patients and make calls.
- 100-500 patients across multiple conditions: hybrid. The off-the-shelf platform handles the basics, but you start needing custom integrations: multi-condition monitoring (BP + glucose + weight flowing into one view), EHR integration that puts RPM data inside the physician’s workflow, and automated concurrent CCM/RPM billing. This is where a platform + custom integration layer makes sense.
- 500+ patients or RPM as a service line: custom build. At this scale, the platform is a revenue engine and the off-the-shelf subscription model becomes more expensive than owning the technology. ConnectHealth handles the device integration layer and the EHR pipeline. The platform is yours.
The honest answer for most small primary care practices launching in 2026: start off-the-shelf with a 25-50 patient pilot. Prove the revenue model. Graduate to hybrid or custom when the patient panel outgrows the platform, which usually happens around 200 patients or when multi-condition monitoring becomes the default.
If you need help selecting the right off-the-shelf platform, validating the billing workflow, or connecting RPM data into your EHR, Mindbowser can help with the integration layer while you keep the value of a fast, low-risk pilot.
For a detailed build-vs-buy analysis across all RPM use cases, see our RPM platforms vs build your own guide.
What Does the First 90 Days Look Like?
This is the part where I have to be honest about what works and what doesn’t based on the small practice launches I’ve been involved with.
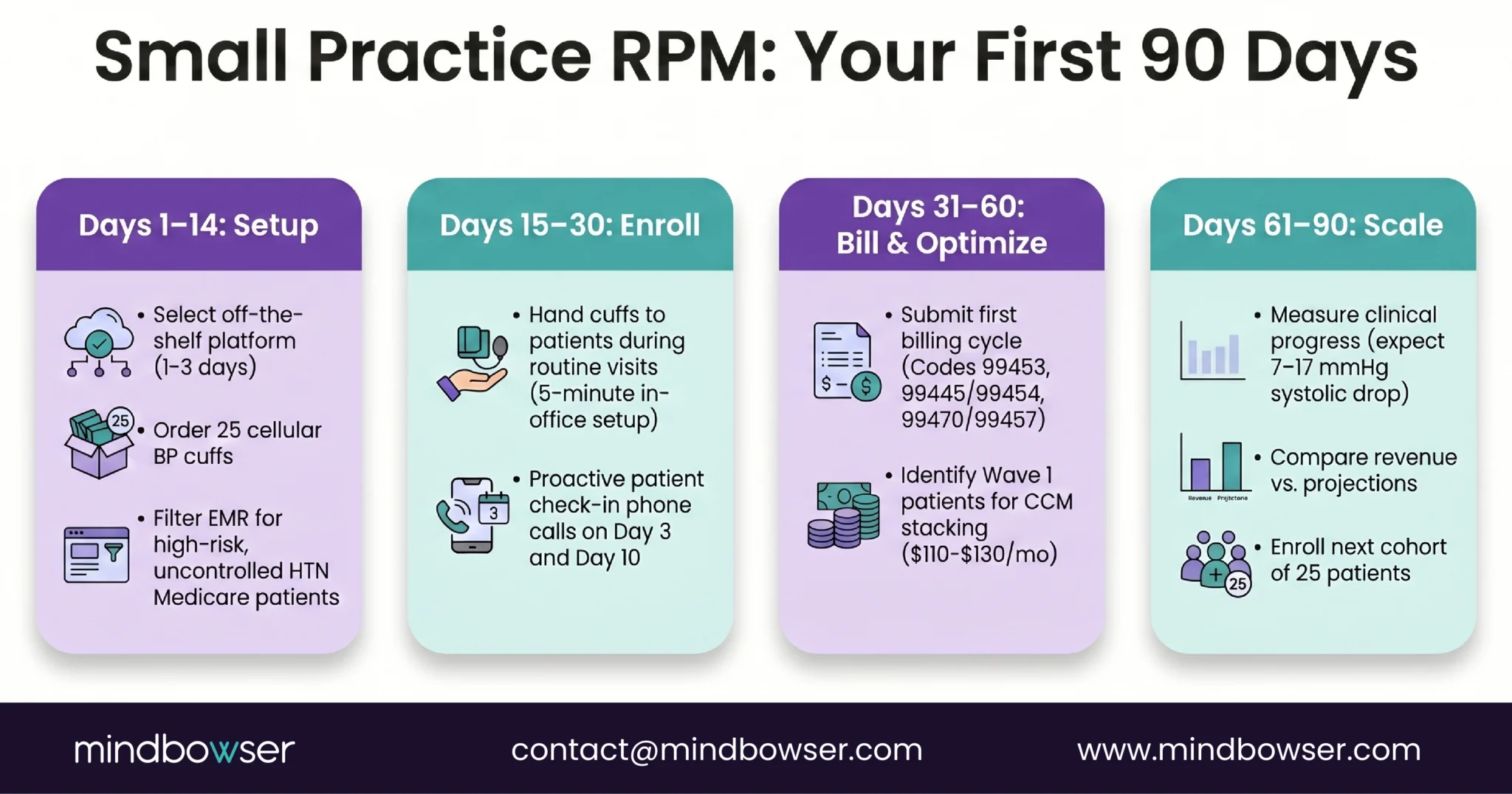
Days 1-14: Setup
- Select and sign up for an RPM platform (this takes 1-3 days, not weeks)
- Order 25 cellular BP cuffs (most vendors ship in 3-5 business days)
- Pull your EMR patient list: filter for uncontrolled HTN + 2+ chronic conditions + Medicare FFS
- Configure alert thresholds in the platform: SBP above 160 (critical), above 150 (elevated), below 90 (hypotension)
Days 15-30: Enroll
- Hand patients the cuff at their next scheduled visit. Five-minute setup: unwrap, pair (cellular does this automatically), take first reading, confirm it appears on your dashboard
- Obtain RPM consent (verbal or written, documented in chart)
- The first 14 days of each patient’s enrollment are critical for engagement. TodayHealth’s 90% engagement rate came from proactive outreach in those first two weeks. Call each patient on day 3 and day 10 to check on device use. This also counts toward your 99457 interactive time
Days 31-60: Bill and Refine
- Submit first billing cycle: 99453 (device setup, one-time) + 99454 or 99445 (device supply) + 99457 or 99470 (interactive time)
- Review alert accuracy: which alerts led to clinical action? Which are noise? Adjust thresholds
- Identify which patients also qualify for CCM (most will). Begin CCM consent conversations. Stacking adds $110-130/patient/month in revenue for zero additional device cost
- Begin enrolling the next 25 patients
Days 61-90: Measure
- Compare enrolled patients’ BP control vs non-enrolled. Published data shows 7-17 mmHg SBP improvement. You should see meaningful movement by day 60
- Calculate actual revenue vs projected. Most practices discover they’re slightly above projections because the MA is already spending the documented time
- Decision point: scale to 100? Add diabetes monitoring? Add a part-time RPM care coordinator (justified at 100+ patients)?
The key insight from every small practice RPM launch I’ve seen: this is not a technology project. It is a workflow addition. The MA who already calls patients about lab results now also reviews BP readings. The physician who already adjusts medications at visits now has 30-day trend data. The practice that already bills E&M now adds RPM codes. The technology is the smallest part of the change.
RPM Is the Next Revenue Line for Primary Care
Independent practices are facing margin compression from every direction. Payer reimbursements declining in real terms. Staffing costs rising. Administrative burden growing. The 2026 Private Practice Playbook from Doctors Management describes the pressure accurately: independent groups are fighting to survive margin erosion that large health systems absorb through volume.
RPM is one of the few new revenue lines that doesn’t require massive capital investment, generates positive cash flow within 2-3 months, improves measurable clinical outcomes (patients with BP readings getting reviewed weekly do better than patients waiting 90 days between appointments), stacks with CCM for additional revenue on the same patients, and scales incrementally from 25 to 500 patients as the practice builds capacity.
Three years ago I would have told a small practice to wait. The technology was clunkier, the billing thresholds were higher, the 16-day monitoring minimum was unrealistic for inconsistent patients, and the 20-minute interactive time threshold was hard for small teams. I would not give that advice now. The 2026 CMS changes were the tipping point. The minimum viable RPM program costs less than an MA’s monthly salary and generates 3 to 5 times that in revenue.
RPM can be profitable with as few as 25 enrolled patients. At 25 patients generating $60-85 per month each, monthly revenue is $1,500-2,125 against startup costs of $3,500-5,000 (devices + platform). Break-even occurs in month 2-3. At 100 patients, annual revenue reaches $72,000-102,000 with a 3-5x ROI on technology and staffing investment. The 2026 short-duration code (99445) and lower time threshold (99470) make even more patients billable.
For a 25-patient launch: cellular BP cuffs at $80-120 each ($2,000-3,000), RPM platform subscription at $5-15 per patient per month ($125-375/month), and existing staff time (no new hire needed). Total first-month investment: under $5,000. Monthly operating cost at 50 patients: $250-750 for the platform. Revenue at 50 patients: $3,000-4,250 per month. The program is cash-flow positive from month two.
Not at the pilot scale. At 25-50 patients, an existing medical assistant or care coordinator can handle RPM duties within their current role: 15-20 minutes per patient per month reviewing readings and making calls. This is often work the MA is already doing informally (calling patients about vital signs). RPM adds documentation structure and billing capture. A dedicated RPM coordinator becomes justified at 100-150+ patients, and at that point the program revenue more than covers the hire.
Start with hypertension (simplest protocol, largest patient pool, fastest measurable outcomes). Second wave: diabetes (blood glucose meter or CGM). Third wave: heart failure (connected scale plus BP cuff). Hypertension requires one device and produces measurable BP improvement within 2-4 weeks. Diabetes and heart failure require additional devices and more complex monitoring protocols. Most primary care RPM programs reach 80% of their revenue potential from hypertension and diabetes monitoring alone.
Three changes matter: (1) New code 99445 allows billing for 2-15 days of monitoring data per month (previously required 16 days under 99454), making inconsistent patients billable. (2) New code 99470 covers the first 10 minutes of treatment management (previously 20 minutes under 99457), a threshold achievable for every patient every month. (3) CMS raised the conversion factor by 3.26% to $33.40, increasing reimbursement per code. APCM also (Advanced Primary Care Management) simplifies concurrent behavioral health billing for practices without dedicated billing staff.
Yes. CMS allows concurrent RPM (99457/99458) and CCM (99490/99439) billing for the same patient in the same month, provided documented time is tracked separately. Most RPM patients in primary care (those with 2+ chronic conditions) also qualify for CCM. Stacking adds $110-130 per patient per month in additional revenue with minimal incremental work. See our detailed RPM + CCM stacking guide for the full revenue math and compliance walkthrough.


