



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
- Heart failure is the leading cause of 30-day readmissions in patients 65 and older and one of the original conditions in CMS’s Hospital Readmissions Reduction Program, where penalties run up to 3% of total Medicare reimbursement.
- RPM programs are now showing 38 to 50% readmission reductions across published studies (AJMC, 2024).
- Wearable ECG patches detect post-discharge arrhythmias in 27% of cardiac surgery patients that traditional Holter monitors miss (Vivalink, 2025). UnitedHealthcare still covers heart failure for RPM in 2026, one of only two conditions they kept.
- The business case and clinical case point in the same direction. This is the one RPM program where “should we do this?” is the wrong question. The question is how fast you can get it running.
Every hospital in America with a cardiac service line is paying the HRRP penalty, or spending significant resources trying not to, and the programs that are actually moving readmission rates have one thing in common: they monitor patients after they leave the building.
I’ve been involved in cardiac monitoring programs for years, and the pattern is consistent. The patient is stable at discharge. Medications are optimized. Education is delivered. The transition of care checklist is complete. Then the patient goes home, gains four pounds of fluid over five days because nobody is watching the scale, and shows up in the ER on day 12.
That sequence plays out thousands of times a day across the US. It is a monitoring gap, not a care gap. The care was appropriate. The follow-up was scheduled. But nobody had eyes on the daily weight between discharge and the first outpatient visit.
Why Is Heart Failure the Highest-Stakes RPM Condition?
Three forces converge on heart failure that don’t converge on any other RPM condition.
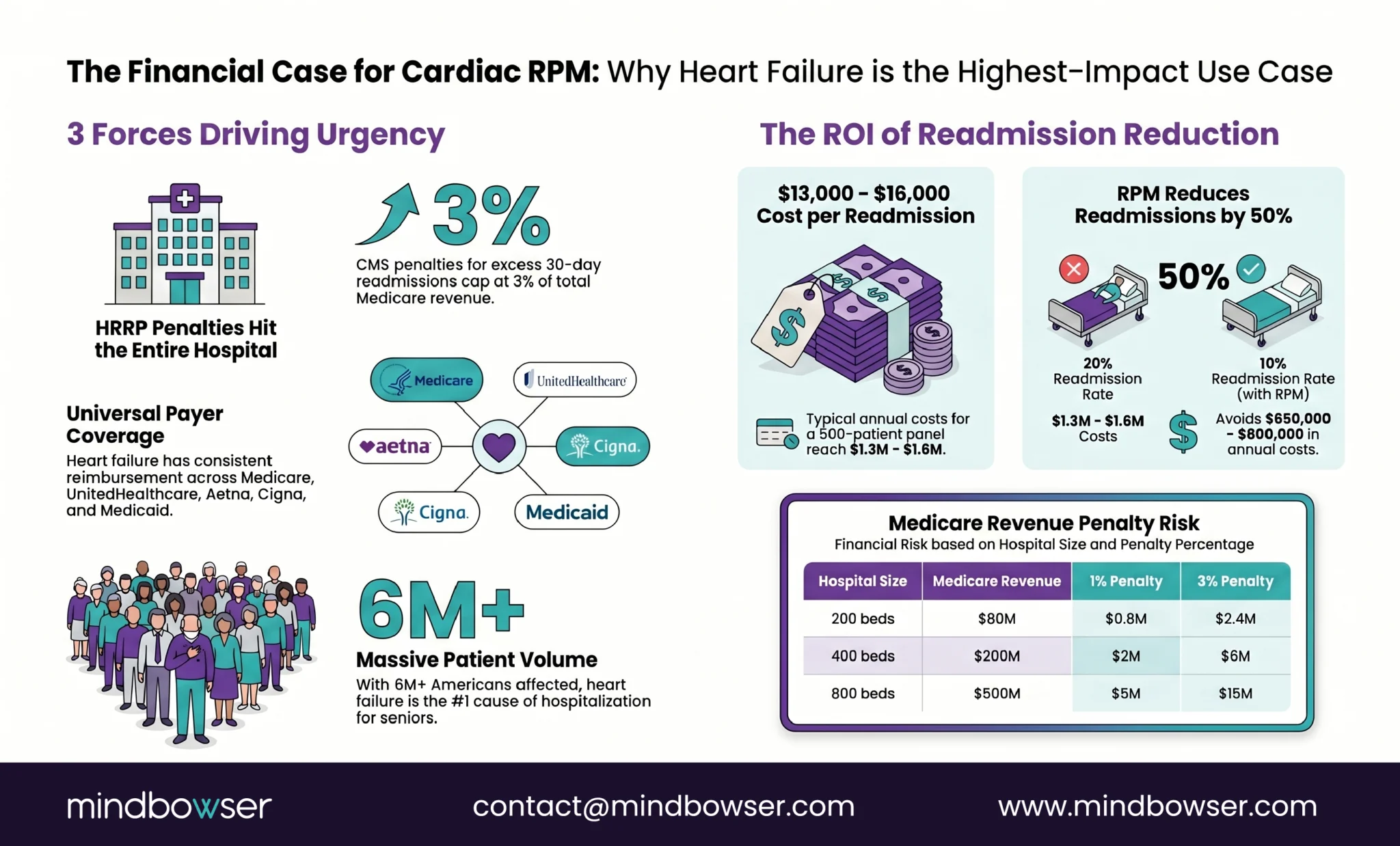
First: the readmission penalty. CMS’s Hospital Readmissions Reduction Program penalizes hospitals with higher-than-expected 30-day readmission rates for heart failure. The penalty is capped at 3% of total Medicare reimbursement. Not 3% of cardiology revenue. Three percent of all Medicare payments to the hospital. For a 400-bed hospital with $200 million in Medicare revenue, that is up to $6 million at stake. The FY 2026 performance period uses data from July 2021 through June 2024, and CMS has proposed shortening the lookback from three years to two, meaning more recent performance weighs more heavily.
Second: every payer covers it. Heart failure is one of only two conditions UnitedHealthcare still covers for RPM in 2026 (the other is hypertensive disorders during pregnancy). Medicare FFS covers it. Aetna, BCBS, Cigna, state Medicaid programs, all cover it. There is no payer mix scenario where heart failure RPM doesn’t have reimbursement support. That is unique among RPM conditions right now.
Third: the patient volume is enormous. Over 6 million Americans live with heart failure. Roughly 1 million new cases are diagnosed annually. Heart failure is the most common cause of hospitalization in adults over 65. Every health system with an inpatient service has these patients.
When I talk to quality officers at hospitals, the HRRP penalty is the conversation starter. But the real cost is downstream: each heart failure readmission costs $13,000 to $16,000 on average. A 500-patient heart failure panel with a 20% readmission rate generates roughly $1.3 to $1.6 million in readmission costs annually. Cut that rate in half (which published programs are doing) and you’re looking at $650,000 to $800,000 in avoided costs. That is before the HRRP penalty savings.
What Does the Readmission Reduction Evidence Show?
The evidence for heart failure RPM reducing readmissions is the strongest of any RPM application. Multiple study designs, multiple populations, consistent results.
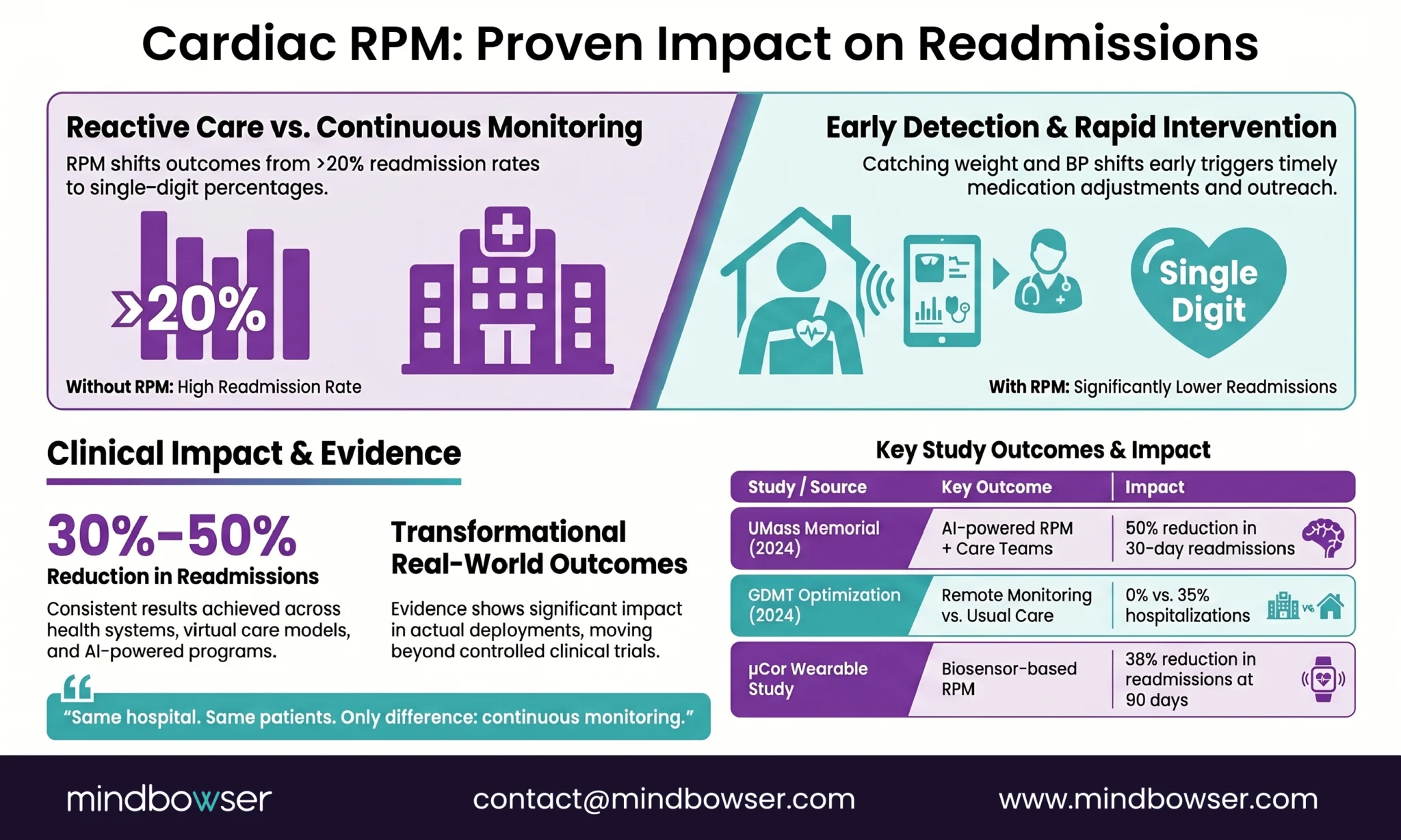
An AI-powered remote monitoring program at UMass Memorial Health (published in AJMC, 2024) cut 30-day heart failure readmissions by 50%. The program combined AI-driven monitoring with human care teams. Fifty percent. In a real health system, not a clinical trial with ideal conditions.
A virtual home health heart failure program evaluated in JMIR Cardio (2025) reported a 30-day readmission rate of 10.2%, compared to the historical benchmark of approximately 20%. The program used daily weight, blood pressure, and symptom monitoring with care manager follow-up.
A study on guideline-directed medical therapy optimization with remote monitoring found the remote monitoring group had a hazard ratio of 0.19 for hospital readmission compared to usual care. Zero heart failure hospitalizations in the remote monitoring cohort versus a 35% rate in the traditionally managed group. That is not a marginal improvement. That is a category change.
A wearable biosensor study (μCor, 522 patients) showed a 38% relative reduction in hospital readmissions at 90 days for the intervention group, with quality-of-life improvements that were statistically significant.
At BRI 2026, Jody Underwood and Tamika Rolle from St. Joseph’s presented their heart failure and hypertension RPM program results. The number that stopped the room: patients NOT enrolled in RPM continued readmission rates above 20%. Enrolled patients dropped to single digits. Same hospital. Same patient population. Same clinical team. The only variable was whether someone was watching the daily readings.
I should note that the CHAMPION, GUIDE-HF, and MONITOR-HF randomized controlled trials have consistently demonstrated that remote hemodynamic monitoring (CardioMEMS implantable sensor) significantly reduces heart failure hospitalizations. These are implantable device studies, not wearable RPM, but they validate the core principle: continuous monitoring catches decompensation before it becomes an emergency.
What Does a Heart Failure RPM Device Stack Look Like?
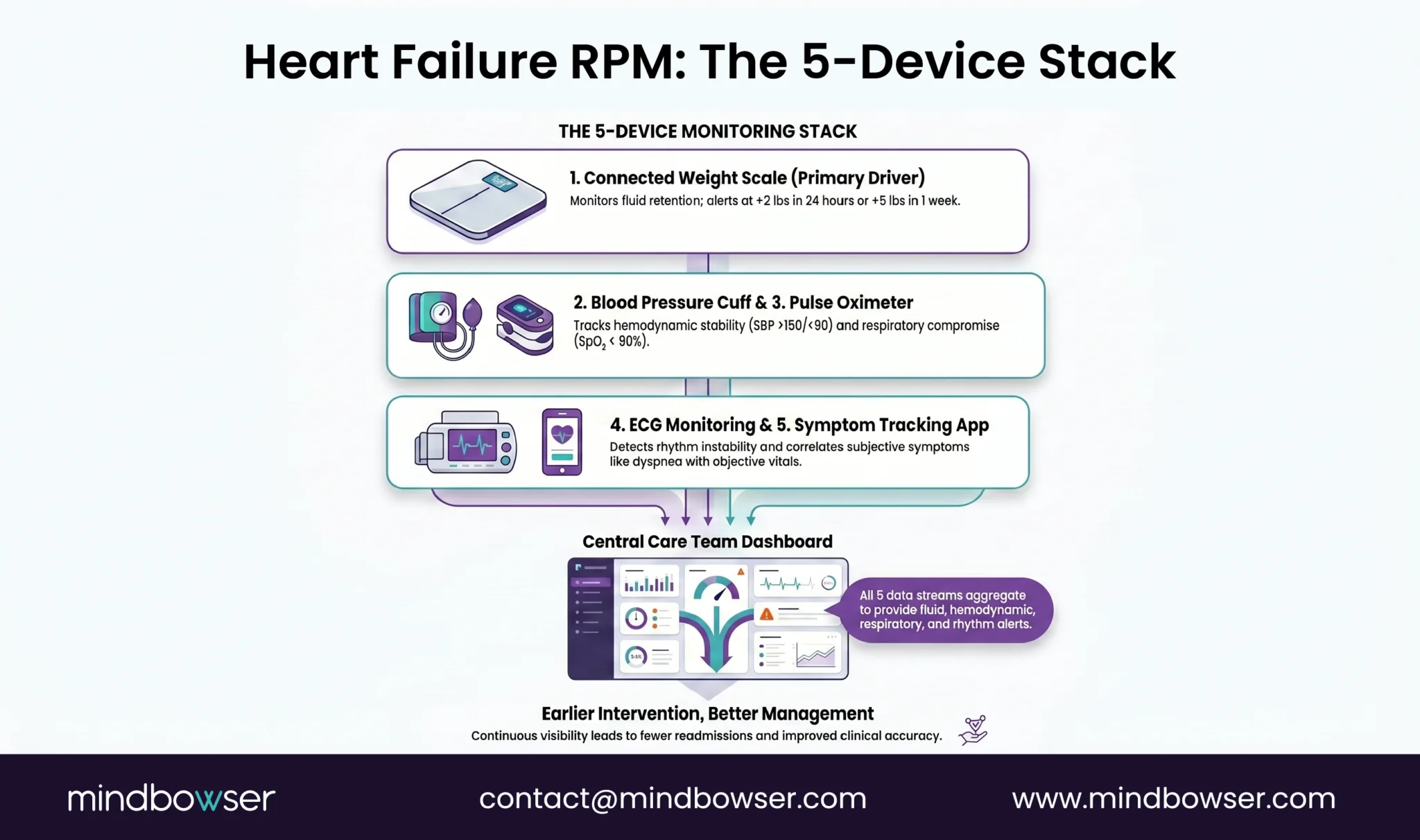
Heart failure monitoring is the simplest multi-device RPM protocol. Five data streams, each with clear clinical logic.
Daily weight (connected scale). This is the single most important metric. A weight gain of 2 or more pounds in 24 hours, or 5 or more pounds in a week, signals fluid retention and early decompensation. The patient steps on the scale every morning. The reading transmits automatically. If the number jumps, the care manager calls. This one device, used consistently, catches the majority of preventable readmissions.
Twice-daily blood pressure (cuff). Tracks hemodynamic stability and medication response. Heart failure patients on ACE inhibitors, ARBs, or beta-blockers need BP monitoring for both hypertension and hypotension. Alert thresholds: SBP above 150 or below 90.
SpO2 (pulse oximeter). Detects respiratory compromise. A drop in oxygen saturation signals pulmonary congestion, which often accompanies fluid retention. Alert threshold: SpO2 below 90%.
ECG monitoring (patch or single-lead device). Heart failure patients have a high prevalence of concurrent arrhythmias (atrial fibrillation in particular). An ECG patch worn for 7 to 14 days post-discharge catches rhythm changes that standard monitoring misses.
Symptom questionnaire (app-based). Daily check for dyspnea (shortness of breath at rest or with exertion), peripheral edema (ankle swelling), fatigue levels, orthopnea (needing extra pillows to sleep), and paroxysmal nocturnal dyspnea (waking up gasping). These subjective symptoms correlate with objective vital sign changes and catch decompensation patterns the devices alone may miss.
For specific device models, connectivity options, and costs, see our complete remote patient monitoring devices list.
How Is Arrhythmia Monitoring Different from Heart Failure RPM?
Search “cardiac remote patient monitoring” and 7 of the top 10 results are about implanted cardiac device telemetry: pacemakers, ICDs, CRT devices transmitting data to Medtronic CareLink or Abbott Merlin. That is a different clinical program with different technology, different billing, and different goals.
Let me clarify the distinction because it matters for program design.
- Heart failure RPM uses external devices (scales, BP cuffs, pulse oximeters, symptom apps) to monitor daily vitals in patients living at home. The goal is catching decompensation early enough to prevent a readmission. Billing: CPT 99453-99458.
- Implanted cardiac device monitoring uses telemetry from pacemakers, ICDs, and CRT devices that transmit rhythm data to manufacturer platforms (Medtronic CareLink, Abbott Merlin, Boston Scientific Latitude). The goal is detecting device malfunctions, arrhythmias, and lead issues. Billing: CPT 93294-93299 (separate code family).
- Wearable arrhythmia monitoring uses external ECG patches (Zio, BioTelemetry MCOT, Hexoskin) worn for 7 to 30 days to detect arrhythmias. Typically prescribed after a cardiac event, post-surgery, or for symptomatic patients without a diagnosis. A PMC study from 2025 found that wearable ECG patches outperform traditional Holter monitors in long-term arrhythmia detection, with overall accuracy of 97%.
The finding I keep coming back to: a Brigham and Women’s Hospital study found that while 42% of cardiac surgery patients experienced atrial fibrillation during hospitalization, an additional 27% had new AFib episodes after discharge that were only detected by wearable ECG patches worn at home. Twenty-seven percent. More than one in four patients. Those episodes are invisible without post-discharge monitoring.
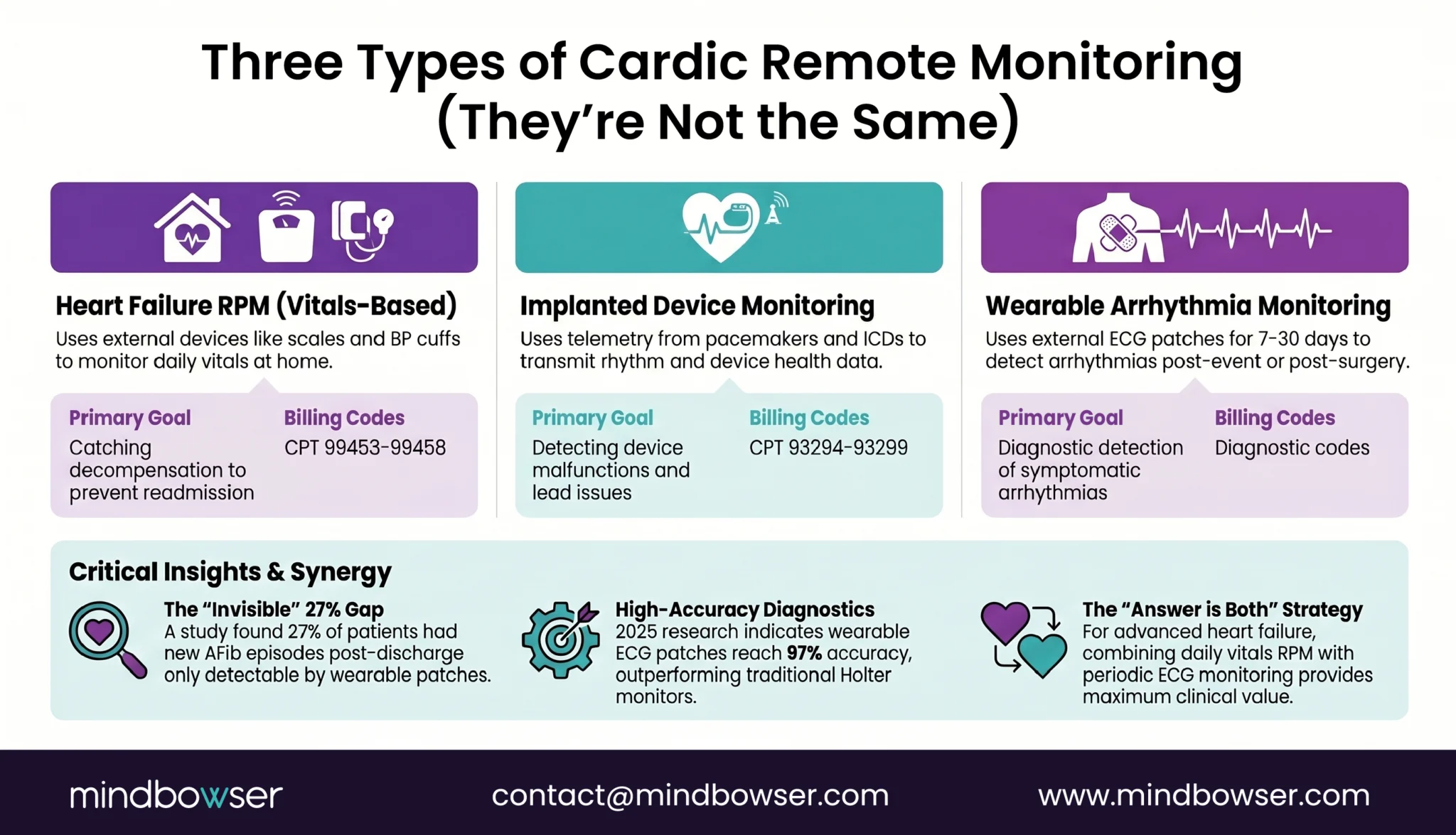
For programs that serve heart failure patients with concurrent arrhythmia risk (which is the majority of advanced heart failure patients), the answer is both: daily vitals RPM plus periodic ECG patch monitoring. Different devices, different billing codes, complementary clinical value.
What About Post-MI and Cardiac Rehab Monitoring?
Post-MI patients represent a third cardiac RPM population with different needs than heart failure or arrhythmia monitoring.
In the first 30 days after a myocardial infarction, patients face elevated risk of arrhythmia, recurrent ischemia, and decompensation. The monitoring needs are: ECG (rhythm surveillance), blood pressure (medication titration, particularly anti-hypertensives and beta-blockers), and activity tracking (graduated exercise tolerance).
Cardiac rehabilitation is where the opportunity gets interesting. Traditional cardiac rehab requires in-person attendance at a facility 2 to 3 times per week for 12 weeks. The completion rate is historically below 30%. Thirty percent. Seven in ten patients who are prescribed cardiac rehab don’t finish it. The reasons are predictable: transportation, work schedules, distance to facility, patient motivation.
Remote monitoring enables hybrid cardiac rehab: in-clinic sessions for the structured exercise and education components, plus remote monitoring on off-days to track exercise adherence, heart rate response, and recovery. The patient exercises at home wearing a heart rate monitor. The data flows to the rehab team. If the heart rate response is abnormal during a home exercise session, the team intervenes.
We built a cardiac rehab RPM platform for exactly this model: cardiac rehabilitation with Bluetooth heart rate monitoring. The platform monitors exercise sessions remotely, tracking heart rate zones and recovery patterns. The clinical team sees real-time data during the patient’s home exercise. It is the difference between hoping the patient exercised appropriately and knowing.
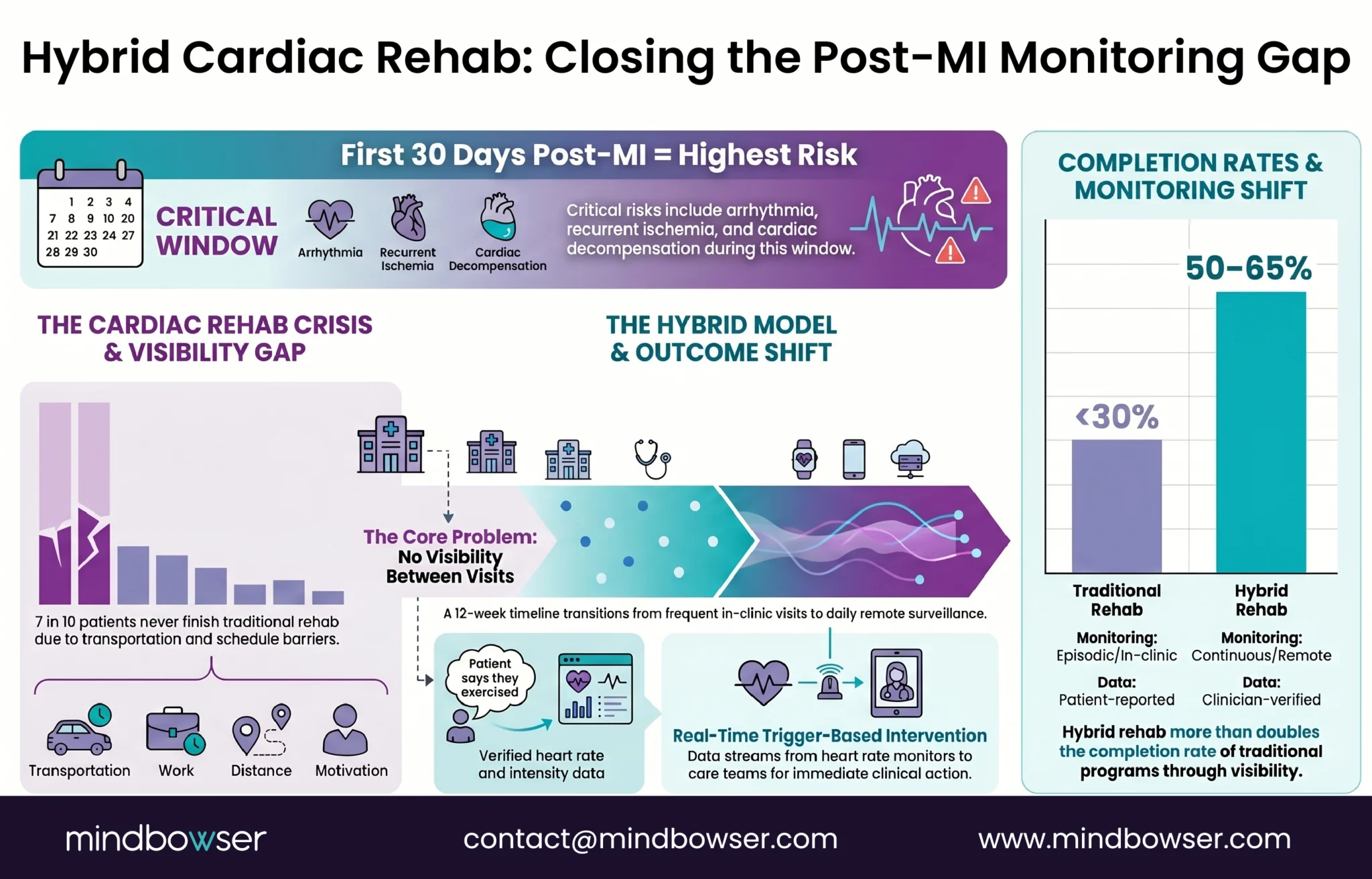
Actually, let me correct something. When I say “hoping,” I don’t mean cardiac rehab teams are careless. They care deeply. But between in-clinic visits, they have zero visibility into what the patient is doing. A patient who says “I walked 30 minutes” and a patient who actually walked 30 minutes at the right intensity look identical without monitoring data. Remote monitoring closes that gap.
Discuss Cardiac RPM Platform Architecture for Multi-condition Patients
How Does CMS Reimburse Cardiac RPM in 2026?
Cardiac RPM bills through the standard RPM codes (99453-99458), the same as every other condition. What makes cardiac RPM financially distinct is the HRRP penalty offset.
RPM billing: 99453 (setup, ~$19-21), 99454 (device supply, ~$55-64/month), 99457 (interactive communication, ~$50-58/month), 99458 (additional time, ~$42-48). Revenue per patient: $105-122/month RPM only, $167-184 with concurrent CCM.
HRRP penalty offset. This is where the ROI calculation is different from diabetes or COPD RPM. For cardiac RPM, the revenue isn’t just billing; it’s penalty avoidance.
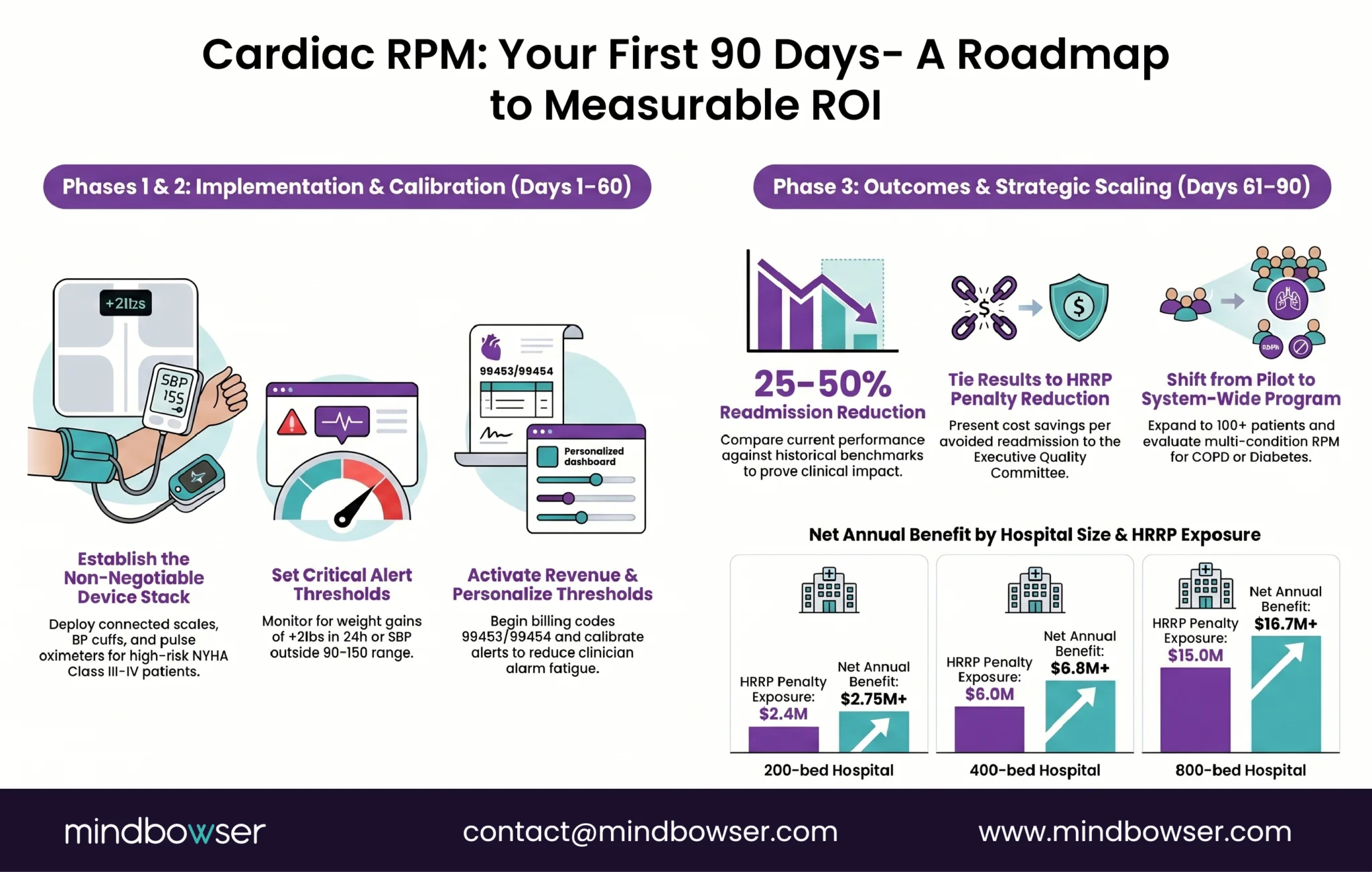
| Hospital Size | Medicare Revenue | Max HRRP Penalty (3%) | RPM Program Cost (200 pts) | Readmission Cost Avoided (50% reduction) | Net Annual Benefit |
|---|---|---|---|---|---|
| 200-bed | $80M | $2.4M | ~$300K | ~$650K | $2.75M+ |
| 400-bed | $200M | $6.0M | ~$500K | ~$1.3M | $6.8M+ |
| 800-bed | $500M | $15.0M | ~$800K | ~$2.5M | $16.7M+ |
The math assumes you’re currently at or near the penalty threshold. If you’re already well below national averages, the HRRP offset is smaller but the readmission cost avoidance still holds.
UHC coverage. Heart failure RPM remains billable under UnitedHealthcare in 2026. This is the one RPM condition where you don’t need to worry about the UHC rollback when doing payer mix analysis.
Arrhythmia monitoring (separate billing). If you’re also running wearable ECG monitoring for arrhythmia detection, those bill under CPT 93241-93248 (external ECG monitoring codes), not under RPM codes. Both can run concurrently on the same patient.
Should You Build Custom or Buy Off-the-Shelf?
Heart failure RPM has the most mature vendor market of any RPM condition. Several platforms do it well.
Health Recovery Solutions (HRS) is the market leader. KLAS #1 for RPM in 2020, 2021, 2022, and 2023. Frederick Health case study: 83% reduction in 30-day readmissions, $5.1 million in cost savings. HRS acquired Rimidi in March 2026 to add chronic disease management (diabetes, cardiometabolic) to their RPM platform. For single-condition heart failure RPM with a proven vendor, HRS is the benchmark.
Vector Remote Care specializes in cardiac implanted electronic device (CIED) monitoring plus heart failure RPM. If your program needs both implanted device telemetry and external vitals monitoring, Vector combines them.
Cardiac RMS is a focused cardiac remote monitoring vendor with strong presence in cardiology practices.
Where custom build adds value for cardiac RPM specifically:
HRRP-specific analytics. The standard RPM dashboard shows patient vitals. A custom dashboard built for the quality committee shows: current readmission rate, trending vs target, HRRP penalty risk score, patient-level risk stratification. That is different data for a different audience.
Multi-condition cardiac patients. A heart failure patient who also has diabetes (CGM data), COPD (SpO2 trending), and CKD (weight/fluid management) needs unified monitoring. Off-the-shelf platforms handle HF well in isolation. Custom platforms handle the multi-condition patient.
Hybrid cardiac rehab. The RecoveryPlus model (remote exercise monitoring with Bluetooth heart rate) is not a feature of standard HF RPM platforms. Cardiac rehab monitoring is a custom build.
EHR-native integration. Daily weight trends, BP patterns, and rhythm data embedded inside Epic or Cerner as FHIR Observations, visible during the cardiologist’s clinic visit without switching tabs. ConnectHealth handles this pipeline.
What Should Your First 90 Days Look Like?
Cardiac RPM has the clearest ROI timeline of any RPM condition because the outcome metric (30-day readmission rate) produces measurable data within the first billing cycle.
Phase 1: Foundation (Days 1-30)
- Deploy three devices: connected scale (daily weight is non-negotiable for HF), BP cuff (twice daily), pulse oximeter (once daily)
- Enroll first 50 patients: target recently discharged HF patients, NYHA Class III-IV, highest readmission risk
- Set alert thresholds: weight gain >2 lbs in 24 hours or >5 lbs in 7 days (critical), SBP >150 or <90 (elevated), SpO2 <90% (critical)
- Train care team: 4 hours on alert triage, escalation pathways, and documentation for 99457 billing
- Begin daily monitoring workflow
Phase 2: Calibration (Days 31-60)
- Add ECG monitoring for patients with concurrent arrhythmia risk (AFib, VT history)
- Refine weight alert thresholds: some patients have baseline weight fluctuation of 1-2 lbs that triggers false alarms. Patient-specific calibration after 30 days of data
- Activate RPM billing (99453, 99454, 99457). First revenue cycle
- Identify concurrent CCM candidates: most HF patients have comorbidities qualifying for 99490
Phase 3: Outcomes (Days 61-90)
- Measure 30-day readmission rate for enrolled patients vs historical rate. The UMass study saw 50% reduction. Your first-quarter target: 25-30% reduction (conservative, still meaningful)
- Present data to quality committee with HRRP penalty context
- Scale to 100+ patients based on Phase 1-2 learning
- Decision point: add hybrid cardiac rehab component? Add multi-condition monitoring for HF patients with diabetes/COPD?
The speed advantage of cardiac RPM: unlike COPD (6+ months for outcomes) or diabetes (90-day A1C lag), heart failure readmission data is available within 30 days of each patient discharge. You can demonstrate program value to the quality committee in the first quarter.
The One RPM Program Every Hospital Should Be Running
Heart failure RPM occupies a unique position in 2026. It is the only condition where every payer covers it (including UHC), a CMS penalty exists for poor outcomes (HRRP, up to 3% of Medicare reimbursement), readmission reduction evidence exceeds 50% in multiple studies, and the device protocol is well-established (scale, BP cuff, pulse ox, ECG, symptom app).
No other RPM condition checks all four boxes simultaneously. COPD has the clinical need but thinner evidence. Diabetes has the patient volume but lost UHC coverage. Hypertension has the strongest evidence but also lost UHC coverage. Heart failure has everything.
Five years ago I thought cardiac RPM was primarily for academic medical centers with dedicated heart failure clinics, specialized nurse coordinators, and enterprise IT infrastructure. After watching community hospitals run basic daily weight and BP monitoring programs and cut readmissions in half, I stopped thinking that. The technology isn’t complex. A scale and a BP cuff and someone watching the numbers is more effective than most pharmaceutical interventions at preventing readmissions.
If your quality team is presenting HRRP data next quarter and needs a plan, reach out. The 90-day path from pilot to outcome data is shorter than most people expect. And the first data point, a readmission rate comparison for your enrolled vs non-enrolled patients at 30 days, makes the case for scaling better than any business plan.
The standard heart failure RPM stack includes five devices: a connected weight scale (daily, most important for detecting fluid retention), a blood pressure cuff (twice daily), a pulse oximeter (daily SpO2), an ECG monitor or patch (for concurrent arrhythmia surveillance), and a symptom questionnaire app (daily self-reported dyspnea, edema, fatigue). Most programs start with three devices (scale, BP cuff, pulse ox) and add ECG monitoring for high-risk patients.
Published studies show reductions of 38 to 50%. An AI-powered program at UMass Memorial (AJMC, 2024) achieved a 50% reduction in 30-day readmissions. A JMIR Cardio study (2025) reported 10.2% readmission versus 20% historical. A wearable biosensor study (522 patients) showed 38% relative reduction at 90 days. BRI 2026 conference data from St. Joseph’s showed enrolled patients dropping to single-digit readmission rates versus 20%+ for non-enrolled patients.
Yes. Medicare FFS covers heart failure RPM through CPT 99453-99458. Heart failure has been a covered RPM condition since the program’s inception. The 2026 short-duration code 99445 adds billing flexibility for 2-15 day monitoring periods. Concurrent CCM billing (99490) is available for HF patients with comorbidities. Arrhythmia monitoring with external ECG patches bills separately under CPT 93241-93248.
Yes. Heart failure is one of only two conditions UnitedHealthcare continues to cover for RPM (the other is hypertensive disorders during pregnancy). This makes heart failure RPM the safest RPM investment regardless of payer mix. While UHC excluded chronic hypertension, diabetes, and COPD from RPM coverage, heart failure was retained.
The Hospital Readmissions Reduction Program penalizes hospitals with higher-than-expected 30-day readmission rates for heart failure (among other conditions). The penalty is capped at 3% of total Medicare reimbursement, not just cardiology revenue. For a 400-bed hospital with $200 million in Medicare revenue, the maximum penalty is $6 million. FY 2026 uses performance data from July 2021 through June 2024. CMS has proposed shortening the lookback period from three years to two.
Yes, with high accuracy. A 2025 PMC study found wearable ECG patches achieve 97% accuracy in arrhythmia detection, outperforming traditional Holter monitors for extended monitoring. Brigham and Women’s Hospital found that 27% of cardiac surgery patients had new atrial fibrillation episodes after discharge that were detected only by wearable ECG patches. Major devices include Zio (iRhythm, 14-day wear), BioTelemetry MCOT (30-day cellular), and AliveCor KardiaMobile (on-demand single-lead ECG). Apple Watch ECG is FDA-cleared for AFib detection but is not diagnostic-grade.
They are different clinical programs. Heart failure RPM uses external devices (scales, BP cuffs, pulse oximeters, symptom apps) to monitor daily vitals and detect decompensation. It bills under CPT 99453-99458. Cardiac device remote monitoring (also called CIED monitoring) uses telemetry from implanted pacemakers, ICDs, and CRT devices transmitted through manufacturer platforms (Medtronic CareLink, Abbott Merlin) to detect device malfunctions and arrhythmias. It bills under CPT 93294-93299. Both can run concurrently on the same patient with separate billing.


