



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
- Core RPM billing codes: 99453, 99454, 99457, 99458
- RTM codes to know in 2026: 98975, 98976, 98977, 98979, 98980, 98981, 98984, 98985
- RPM and CCM can be billed together if time is documented separately and not double-counted
What Changed in 2026 for RPM and RTM Billing?
Remote patient monitoring (RPM) billing can create recurring monthly reimbursement when providers capture the right CPT codes, document time correctly, and meet payer requirements. For many programs, RPM revenue comes from device setup, monthly device supply, and treatment management time. CMS continues to recognize core RPM codes 99453, 99454, 99457, and 99458, while 2026 also brings important Remote Therapeutic Monitoring (RTM) updates, including codes 98979, 98984, and 98985 for therapy-related monitoring scenarios.
Many providers underbill RPM because they stop at device reimbursement and miss treatment-management codes, fail the 16-day rule, or do not separate RPM time from CCM or other care-management services. CMS allows RPM and RTM to be billed with CCM and other care-management services as long as the same time is not counted twice.
In this guide, we cover RPM CPT codes, RTM codes, reimbursement logic, concurrent RPM + CCM billing, payer considerations, documentation requirements, and the compliance steps needed to reduce denials.
How Much Revenue Can RPM Generate Per Patient?
RPM reimbursement usually comes from three buckets: onboarding, monthly device supply, and monthly treatment management. In a typical program, 99453 is billed once for setup and patient education, 99454 covers monthly device supply/data transmission, and 99457/99458 cover treatment-management time when documentation supports the required thresholds.
Example reimbursement model
- 99453: one-time setup and patient education
- 99454: monthly device supply and transmission
- 99457: first treatment-management time block
- 99458: each additional treatment-management time block
For finance and operations leaders, the bigger issue is not just eligibility — it is code capture. Many programs bill the device code but miss management time, which reduces total RPM yield per enrolled patient.
What are the CPT Codes for Remote Patient Monitoring in Healthcare?
The main RPM billing codes are 99453, 99454, 99457, and 99458. These codes cover device setup, patient onboarding, monthly device supply/data transmission, and treatment-management time. For 2026 planning, providers should also understand how RPM differs from RTM and where new RTM-related updates fit into therapy-driven monitoring workflows.
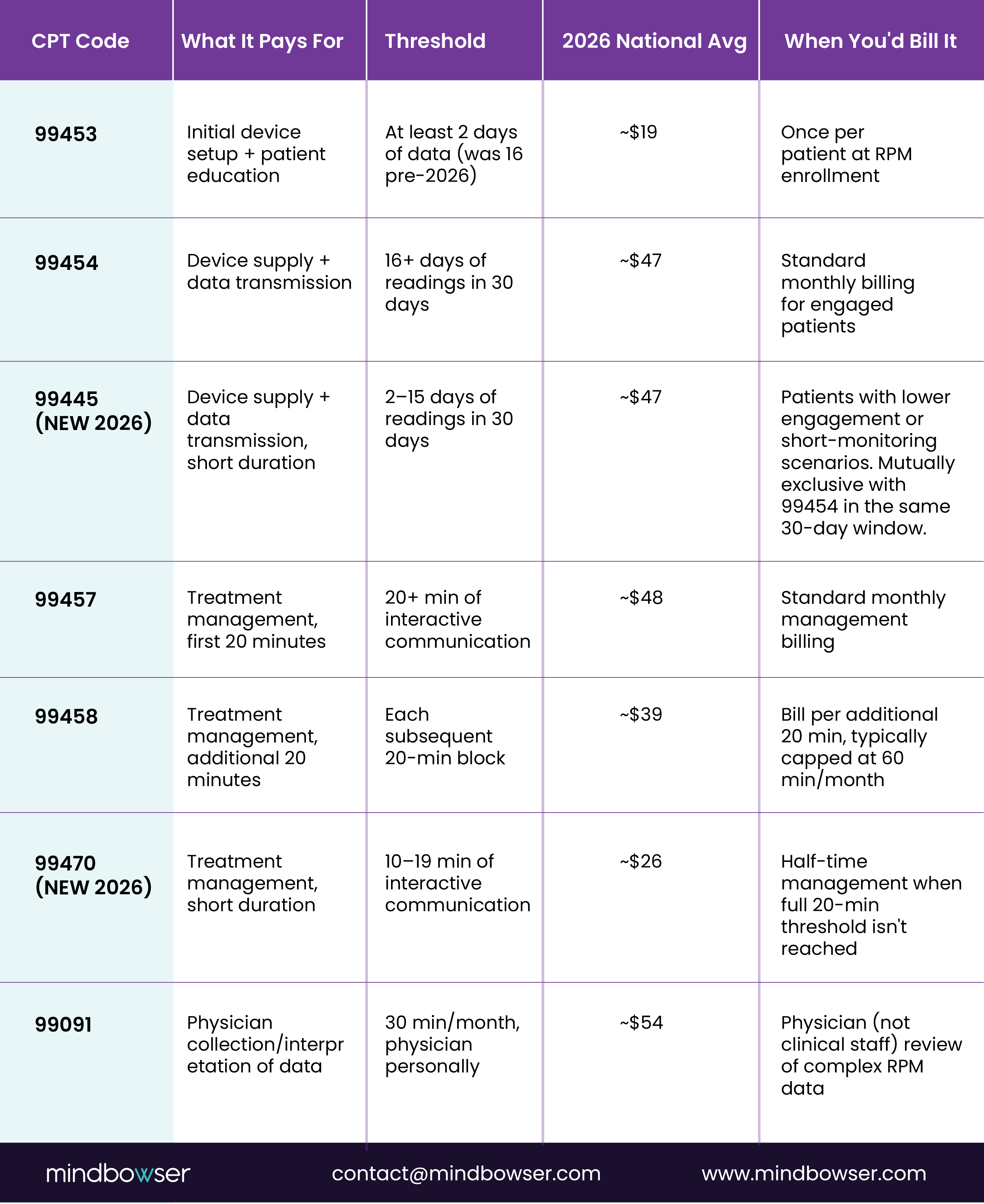
Critical 2026 mutual-exclusion rules: 99445 and 99454 cannot both be billed in the same 30-day window. 99457 and 99470 cannot both be billed in the same month. Pick the code that matches the actual data days (for device supply) or actual management minutes (for treatment management). 99453 setup is once-per-patient-per-episode and is not re-billable if a patient pauses and resumes RPM under the same condition. 99091 is physician-only and cannot be billed by clinical staff under “incident to.
2026 RPM Code Notes:
For RPM, providers should continue focusing on the core four codes: 99453, 99454, 99457, and 99458. Do not mix unrelated digital or interprofessional codes into the RPM workflow unless the service actually matches that code definition. Keep this page centered on true RPM billing first, then explain adjacent billing only where it changes reimbursement strategy.
Key RPM Billing Considerations
✔ 99453 is billed only once per patient at the initiation of RPM services.
✔ 99454 requires at least 16 days of patient readings within a month to qualify for reimbursement.
✔ 99457 can be billed once 20 minutes of provider-patient interaction are completed.
✔ 99458 is used for additional 20-minute increments, up to 60 minutes per month.
RPM vs RTM: When to Use Each
| Use case | RPM | RTM |
|---|---|---|
| Blood pressure, glucose, oxygen saturation | Yes | No |
| Respiratory therapy adherence | No | Yes |
| Musculoskeletal therapy response | No | Yes |
| Physiologic device monitoring | Yes | No |
| Therapy-focused monitoring | No | Yes |
Use RPM for physiologic monitoring and RTM for therapy adherence/response workflows. Do not treat them as interchangeable.
What are Medicare & Medicaid Guidelines for Remote Patient Monitoring Billing?
Medicare recognizes RPM as a reimbursable remote care model when providers meet code-specific requirements for setup, device use, data collection, and treatment management. CMS also continues to emphasize correct use, documentation accuracy, and fraud prevention in RPM billing. Medicaid and commercial payer rules can vary, so payer-by-payer verification is still necessary.
Medicare’s RPM Reimbursement Rules
✔ Covers Chronic & Acute Conditions – Primary care physicians, specialists, and nurse practitioners can bill for RPM services.
✔ FDA-Approved Devices Required – Remote monitoring must use FDA-approved medical devices for reimbursement eligibility.
✔ Minimum Communication Time – Medicare mandates at least 20 minutes of interactive communication per month between providers and patients.
✔ Strict Documentation Compliance – Providers must meet Medicare’s reporting and billing requirements to qualify for reimbursement.
Medicaid & Private Insurance RPM Billing
✔ Medicaid Coverage Varies by State – Some states offer full RPM reimbursement, while others limit coverage to chronic condition monitoring.
✔ Private Insurance Expanding Coverage – More insurers are reimbursing RPM, but billing rules differ by payer.
✔ Eligibility Verification is Essential – Providers must confirm reimbursement policies with each insurer to ensure compliance and proper claim processing.
How Do You Bill RPM Concurrently with CCM, BHI, and APCM?
Concurrent billing is the single biggest revenue lever in remote monitoring programs and the area where most billing teams under-capture. CMS allows more stacking than commonly assumed, with specific exclusions that matter.
What stacks (same patient, same 30-day period):
- RPM (99453-99470) + CCM (99490 / 99439 / 99491): yes
- RPM + BHI (99484, or 99492/99493 for CoCM): yes
- CCM + BHI: yes
- RPM + CCM + BHI (triple stack): yes, for patients with chronic conditions plus a behavioral health diagnosis
- APCM (G0556 / G0557 / G0558) + RPM: yes (new in 2026)
- APCM + RTM: yes
What does NOT stack (mutually exclusive):
- RPM + RTM management codes (99457/99458 vs 98980/98981): pick one per patient per month
- 99445 + 99454: pick one based on data days
- 99457 + 99470: pick one based on management minutes
- CCM + PCM (Principal Care Management): mutually exclusive care management programs
- CCM + APCM: APCM replaces CCM for patients enrolled in the new Advanced Primary Care Management model
- CCM + TCM (Transitional Care Management) in the same month: TCM is a 30-day post-discharge code
Worked example, CHF patient on RPM + CCM:
A 72-year-old patient with congestive heart failure and Type 2 diabetes is enrolled in RPM (BP cuff + scale, daily readings) and CCM (chronic condition care planning). In a typical month, the practice captures:
- 99453: month 1 only (~$19, one-time)
- 99454: 16+ days of readings, ~$47/month
- 99457: first 20 min of RPM management, ~$48/month
- 99458: additional 20 min of RPM management, ~$39/month
- 99490: first 20 min of CCM coordination, ~$62/month
- 99439: additional 20 min of CCM coordination, ~$48/month
Total monthly capture: $244/patient. At 200 dual-enrolled patients, that’s $48,800/month or $585,600/year from patients already in the chronic care panel. Add BHI (99484, ~$50) for patients with depression or anxiety and the per-patient figure climbs to ~$294. The full revenue model, including the APCM vs CCM tradeoff, is in our RPM + CCM stacking guide.
The compliance discipline that keeps the stack clean: time must be documented separately for each program. A 30-minute care manager call discussing both blood pressure trends (RPM) and a cardiology referral (CCM) splits 15/15 in the documentation. The total call time stays at 30 minutes. The billing captures both programs. Audits look for this separation.
2026 Payer Changes You Should Watch
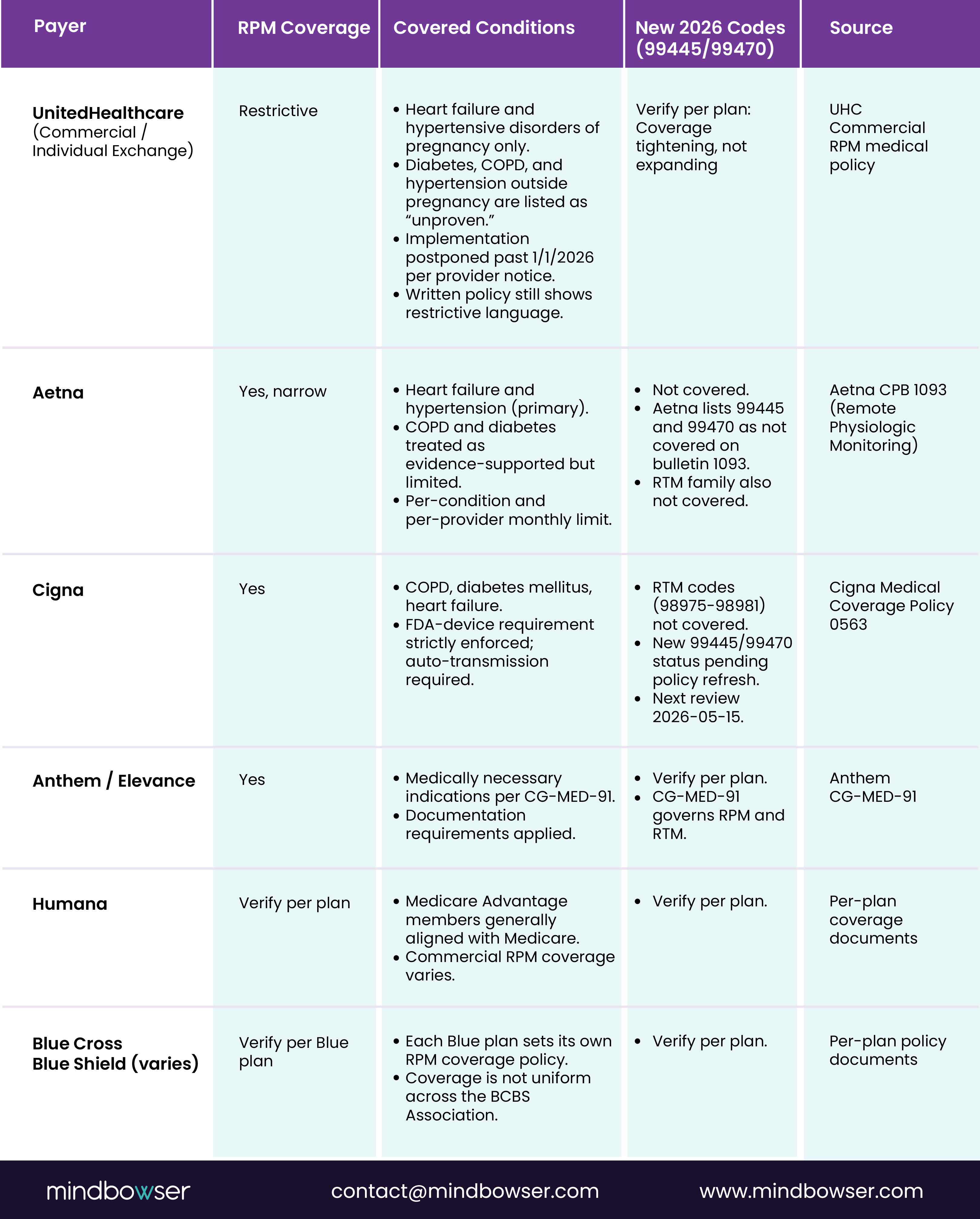
The 2026 commercial RPM coverage landscape is tightening, not expanding. Verified policy positions as of 2026-05:
Three patterns matter for revenue planning:
- UnitedHealthcare’s posted policy (HF + hypertensive disorders of pregnancy only) is the most restrictive shift in commercial RPM coverage to date. Implementation was postponed in early 2026 but the written policy direction signals where commercial coverage is heading. Programs concentrated in UHC commercial populations should model revenue against the restrictive scenario.
- Aetna does not cover the new 2026 codes (99445 and 99470) per bulletin 1093 as of this writing. The covered RPM family for Aetna is the original 99453, 99454, 99457, 99458 set.
- RTM coverage is the weakest area in commercial. Cigna and Aetna both exclude RTM codes broadly. Anthem covers per CG-MED-91 with documentation gates. RPM has stronger commercial footing than RTM.
Practical billing rules:
- Bill the new 2026 codes for Medicare immediately, full coverage confirmed.
- For commercial, verify per-plan policy bulletin before billing 99445, 99470, or any RTM code. A denied claim is recoverable; systematic miscoding across a panel is not.
- For RPM-heavy programs with significant commercial volume, model revenue against the conservative coverage scenario (HF + HTN only) for UHC, and verify state-by-state for BCBS.
Re-verify all payer positions if more than 30 days have passed since 2026-05-02. Payer policies update mid-year.
Practical billing rules:
- Bill the new 2026 codes for Medicare immediately, full coverage confirmed.
- For commercial, verify per-plan policy bulletin before billing 99445, 99470, or any RTM code. A denied claim is recoverable; systematic miscoding across a panel is not.
- For RPM-heavy programs with significant commercial volume, model revenue against the conservative coverage scenario (HF + HTN only) for UHC, and verify state-by-state for BCBS.
Billing Requirements & Compliance for Remote Patient Monitoring
Remote patient monitoring billing requires providers to meet specific Medicare and compliance guidelines. Key factors include patient eligibility, data collection criteria, and HIPAA-compliant security measures. Ensuring proper documentation and adherence to these rules is essential for successful RPM reimbursement.
1. Patient Eligibility
- Medicare requires an established provider-patient relationship before RPM billing.
- Prior visits or consultations must be documented to ensure eligibility.
2. Data Collection & Billing Criteria
- CPT 99454 requires providers to collect 16+ days of RPM data per month.
- CPT 99457 & 99458 require 20+ minutes of interactive patient communication monthly.
3. HIPAA & Data Security Compliance
- RPM must comply with HIPAA & HITECH Act regulations for data privacy.
- Encrypted platforms should be used for patient monitoring and documentation.
Related Read: Patient Monitoring: A Guide for Healthcare Providers
Optimize Your RPM Billing, Maximize Reimbursements, and Stay Compliant!
What are the Common Challenges in RPM Billing & How to Overcome Them?
Remote patient monitoring billing challenges include coding errors, documentation gaps, compliance issues, and reimbursement delays. Overcoming them requires accurate coding, streamlined documentation, and adherence to Medicare guidelines. Let’s learn this in detail:
1. Understanding CPT Codes & Billing Requirements
🧩 Challenge: Many providers struggle with selecting the correct CPT codes, leading to underbilling, claim denials, and revenue loss. Incorrect coding results in delays, audits, and compliance risks, making reimbursement difficult.
💡 Solution: Familiarize yourself with CPT 99453, 99454, 99457, and 99458, ensuring documentation meets Medicare’s time-tracking requirements. EHR-integrated billing tools automate compliance, reducing manual errors and improving claim approval rates.
2. Revenue Leakage From Underused Management Codes
🧩Challenge: Many organizations bill the monthly device code but do not consistently capture treatment-management time, which reduces total reimbursement opportunity.
💡Solution: Build workflows that track care-team time, prompt interactive communication, and surface add-on eligibility before claim submission. CMS billing guidance makes proper code use and documentation central to correct RPM reimbursement.
3. Medicare & Private Insurance Reimbursement Variability
Challenge: Medicare follows clear reimbursement guidelines, but Medicaid and private insurers have inconsistent policies across states and payers. This makes RPM billing unpredictable, leading to potential claim rejections.
💡 Solution: Providers should verify reimbursement policies for each payer before billing and implement billing software with real-time eligibility verification to avoid surprises, ensuring a streamlined reimbursement process.
4. Meeting Data Collection Requirements
🧩 Challenge: CPT 99454 mandates 16+ days of patient data per month, but ensuring patient compliance in consistently using RPM devices is difficult. Missed data collection results in billing ineligibility and revenue loss.
💡 Solution: Implement automated patient reminders via SMS, emails, or app notifications. Engage care teams to educate patients on device usage benefits, ensuring better participation and compliance.
5. Compliance with HIPAA & Security Standards
🧩 Challenge: Continuous RPM data transmission increases the risk of HIPAA and HITECH Act non-compliance, leading to security breaches, legal penalties, and patient trust issues.
💡 Solution: Use HIPAA-compliant RPM platforms with encrypted communication and secure cloud storage. Conduct regular security audits to detect vulnerabilities and maintain strict compliance with healthcare regulations.
6. Lack of Staff Training on RPM Billing & Documentation
🧩 Challenge: Many healthcare teams lack formal training in RPM billing workflows, leading to documentation errors, claim rejections, and revenue losses. Complex regulations make it hard for staff to stay updated.
💡 Solution: Conduct regular staff training on RPM billing requirements and compliance. Use RPM billing software to simplify workflows and consult revenue cycle management experts to reduce errors and optimize claims processing.
Related Read: Automated Remote Patient Monitoring: A Complete Guide for Healthcare Providers
How Mindbowser Can Help You Optimize Remote Patient Monitoring Billing & Reimbursement
Mindbowser provides end-to-end RPM solutions designed to streamline remote patient monitoring billing, maximize reimbursements, and ensure compliance with Medicare, Medicaid, and private insurance requirements. Our expertise in RPM automation, EHR integration, and AI-driven analytics helps healthcare providers scale their remote care services while minimizing billing complexities.
A provider organization wanted to improve RPM enrollment, reduce missed billing opportunities, and create cleaner handoffs between care teams, device workflows, and reimbursement operations. Mindbowser helped design a connected RPM workflow with EHR integration, patient data capture, and billing-support logic aligned to program documentation needs.
The result was a more structured RPM operating model with better visibility into code eligibility, monitoring adherence, and care-management activity.
Why Choose Mindbowser?
✔ Custom RPM Billing Automation – AI-powered automation minimizes claim denials and optimizes reimbursement workflows, ensuring faster and error-free billing.
✔ Seamless EHR Integration – RPM platforms integrate effortlessly with existing EHR systems, enabling real-time data synchronization and streamlined care coordination.
✔ HIPAA & Compliance Expertise – Our solutions meet HIPAA and HITECH standards, ensuring secure data transmission and regulatory compliance for remote monitoring.
✔ AI-Powered RPM Analytics – Advanced analytics automate data collection, providing actionable insights to improve patient monitoring and clinical decision-making.
Conclusion
Remote patient monitoring billing plays a crucial role in expanding remote care services while maintaining financial sustainability. A clear understanding of CPT codes, compliance regulations, and payer-specific reimbursement policies helps healthcare providers avoid claim denials and maximize revenue.
We simplify RPM implementation with automated billing solutions, seamless EHR integration, and AI-powered analytics, ensuring providers optimize reimbursements while focusing on patient care. Partnering with Mindbowser means less complexity, better compliance, and higher financial returns for your RPM program.
The 2026 RPM CPT family includes 99453 (setup, now requires 2+ days of data), 99454 (device supply 16+ days), 99445 (NEW: device supply 2-15 days), 99457 (management first 20 min), 99458 (management additional 20 min), 99470 (NEW: management 10-19 min), and 99091 (physician data interpretation, 30 min). RTM codes are 98975, 98976, 98977, 98980, 98981, plus 2026 additions 98984 and 98985, and the redesignated 98979.
No. 99445 and 99454 are mutually exclusive. Bill 99445 for 2-15 days of data transmission or 99454 for 16+ days of data, never both in the same 30-day window.
99457 covers the first 20 minutes of interactive RPM management time per month. 99470 (new in 2026) covers 10-19 minutes. The codes are mutually exclusive in the same month. Pick the one that matches the documented management time. 99458 (additional 20-minute increments) is only billable on top of 99457, not 99470.
No. The RPM management codes (99457/99458) and RTM management codes (98980/98981) cannot both be billed for the same patient in the same calendar month. If a patient is receiving both physiologic and therapeutic monitoring, the care team must decide which program owns billing for that month.
The choice is determined retrospectively at month-end based on actual days of data transmitted. You don’t pre-commit to one code and switch. At the close of the 30-day period, count the days of readings and bill the appropriate code (99445 for 2-15 days, 99454 for 16+ days).
Adoption is uneven across commercial payers as of early 2026. Aetna lists both as not covered on bulletin 1093. Cigna and other carriers have not yet refreshed their policies. Bill the new codes for Medicare immediately, and verify per-payer (UnitedHealthcare, Anthem, Aetna, Cigna, BCBS plans, Humana) before submitting commercial claims with 99445 or 99470.


