



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR:
Chronic care management billing in 2026 goes beyond counting minutes. With new APCM codes, the RHC and FQHC transition, and tighter compliance requirements, CIOs and Pop Health leaders must rethink workflows. This guide unpacks billing mechanics, data design, and ROI levers supported by case studies and solution accelerators.
- Denials remain the biggest threat. Up to 80% of CCM claims fail without automation, and even mature programs still see 25–30% denial rates when billing relies on manual workflows.
- The revenue is meaningful and recurring. CCM reimburses $42–$93 per patient per month, which makes small process failures add up to seven-figure losses.
- APCM changed what “compliance” means. Time tracking alone no longer protects revenue. In 2026, reimbursement depends on proving patient complexity, not just activity.
- Most organizations still under-collect. Without automated pre-adjudication and evidence assembly, providers often realize only 40–50% of their potential CCM revenue.
- Automation is now the line between growth and leakage. Systems that embed compliance into the workflow cut denials, defend audits, and turn CCM billing into a predictable margin contributor.
CCM billing has become the backbone of recurring hospital revenue. The 2026 CMS updates and APCM bundles changed how hospitals earn, track, and defend every dollar. Clean claims depend on complete documentation, verified consent, and time-stamped records. The right automation and FHIR-aligned data design can recover up to 3–5% of lost revenue. Even a 1% swing in denials can mean hundreds of thousands of dollars.
Chronic care management billing services help hospitals and digital health companies reduce administrative complexity, avoid denied claims, and maximize reimbursement. With new APCM codes, rising audit risks, and staffing shortages, outsourcing billing and leveraging automation ensures compliance, lowers costs, and drives measurable ROI.
Introduction
Chronic care management (CCM) billing has always been complex, but 2026 raises the stakes. New codes tied to the Advanced Primary Care Management (APCM) model, updated reimbursement for Rural Health Clinics and Federally Qualified Health Centers, and a sharper focus on audit readiness are reshaping how hospitals and physician groups approach care management.
For CIOs, population health leaders, and CTOs, the conversation has shifted. CCM billing is no longer just about compliance with CPT codes. It is about positioning organizations to capture sustainable revenue, protect against denials, and build workflows that meet the realities of staffing shortages and payer scrutiny.
That lesson still holds in 2026. Chronic Care Management billing is not just a compliance exercise. It is a systemic problem that resides at the intersection of data design, clinical workflows, and financial accountability.
The recent CMS updates to CCM, Complex CCM, and the new Advanced Primary Care Management (APCM) bundles changed the math for every care team. Hospitals and digital health operators now need to prove supervision, link each minute of service to a signed care plan, and store that evidence in a retrievable format.
This blog examines what matters most right now: the size of the CCM opportunity, the 2026 code landscape, the compliance checkpoints that cannot be overlooked, and the tools that can protect revenue while enhancing patient care.
For hospitals and digital health leaders, billing has become the single biggest burden in chronic care management. Each month, care teams must document the time spent, interventions provided, and updates to the care plan to meet CMS requirements.
Mid-market hospitals spend between $50,000 and $1 million annually on compliance and billing operations, with 60–80% preferring outsourced billing support.
This is why chronic care management billing services are becoming central to strategy—not just for compliance, but for scaling care and proving ROI.
I. Why CCM Billing Matters Now
A. Market Momentum
- The CCM and chronic disease management market is no longer a niche. In 2024, valuations ranged from $1.7 billion to $6.7 billion, depending on methodology.
- Projections indicate rapid expansion, with estimates placing the U.S. market between $6 billion and $30 billion by 2030.
- Growth is being fueled by three forces: the adoption of value-based care models, new CMS reimbursement opportunities, and the rise of enabling technology such as RPM platforms and integrated EHR workflows.
B. Policy Drivers
- The launch of APCM in 2025 is a watershed moment. These codes shift reimbursement from time-based measures to patient complexity, which could stabilize revenue for practices that manage highly complex patients.
- RHCs and FQHCs, which previously relied on G0511 as a blended code, can now bill using standard CPT codes. This eliminates a one-size-fits-all approach and opens the door to more accurate reimbursement.
- Policy alignment with patient complexity is also intended to drive measurable ROI, rewarding organizations that can demonstrate quality outcomes and patient engagement.
- Chronic care billing requires precise time tracking, care plan documentation, and eligibility verification. Missing even a single documentation element can invalidate the entire claim.
- Provider burnout from manual tracking and reporting continues to be a major barrier to scaling CCM programs.
C. Operational Pain Points
- Administrative overload remains a top complaint. Tracking time thresholds, documenting patient consent, and reconciling overlapping codes create burdens that often fall on already strained nursing and care coordination teams.
- Staffing shortages compound the issue. Many hospitals and practices struggle to meet the minimum 20 or 60 minutes required for billing CCM or complex CCM codes, especially when care teams are stretched thin.
- Denials tied to incomplete documentation are still frequent. Missing consent forms, gaps in supervision records, or conflicts with other billed codes remain common triggers for payer rejections.
II. How to Submit a CCM Claim — Step-by-Step (2026)
If you’ve made it this far on a CCM billing page, you probably don’t want another conceptual overview. You want to know exactly what a billing manager does, in what order, to submit a clean CCM claim that won’t get denied or recouped. The walkthrough below covers the five operational steps — eligibility verification, consent documentation, time tracking, code selection, and claim submission — with the specific fields, decisions, and audit-defensible artifacts each step produces.
The framework applies to any CCM CPT code (99490, 99439, 99487, 99489, 99491, 99437) and to APCM (G0556, G0557, G0558) with one exception flagged below.
Step 1 — Eligibility Verification
Before any minute is logged or any claim is generated, the patient has to clear four eligibility gates. Skip any one, and every claim that follows is exposed to denial or recoupment.
Gate 1 — Insurance. Patient must have Medicare Part B coverage. Traditional Medicare and most Medicare Advantage plans cover CCM; verify coverage before enrolling. Check for supplemental Medigap or Medicaid coverage that offsets the 20% Part B coinsurance — this affects enrollment willingness more than billing mechanics, but it’s a Day 1 conversation.
Gate 2 — Chronic conditions. Patient must have two or more chronic conditions documented in the EHR with ICD-10 codes. The conditions must be expected to last at least 12 months (or for the rest of the patient’s life), and they must place the patient at significant risk of death, acute exacerbation, decompensation, or functional decline. The qualifying-conditions list is broad — diabetes, hypertension, heart failure, COPD, depression, dementia, CKD, arthritis, cancer in active treatment, substance use disorder, and 60+ others.
Gate 3 — Initiating visit. Patient must have completed an Annual Wellness Visit (AWV), comprehensive E/M visit, or Transitional Care Management (TCM) visit before the first month of CCM billing. The initiating visit is billed separately and its time does NOT count toward CCM minutes. Document the visit date and link it to the CCM enrollment record.
Gate 4 — Practitioner uniqueness. Only one practitioner can bill CCM for a given patient in a given calendar month. Run an insurance check before billing to confirm no other provider has a CCM claim on file for that patient that month. Duplicate-practitioner billing is one of the fastest paths to denial.
Output of Step 1: A patient-eligibility record in the EHR confirming all four gates, with documentation pointers (insurance file, ICD-10 codes from problem list, initiating visit encounter ID, single-practitioner attestation).
Step 2 — Consent Documentation
CCM consent is the audit element most often missing from denied claims. The consent must be obtained, documented, and dated before any CCM time is logged.
What the consent must cover:
1. The patient is being enrolled in Chronic Care Management
2. The patient understands cost-sharing applies (standard Part B 20% coinsurance — about $13/month at 2026 rates)
3. The patient understands they can revoke consent at any time
4. The patient consents to electronic care plan storage and sharing across the care team
5. The patient acknowledges receipt of the practice’s 24/7 access protocol
How the consent is captured: Verbal consent is acceptable under current CMS rules and counts as long as it’s documented in the EHR with date, method (verbal), witness (the staff member who obtained it), and the practitioner of record. Written consent is preferred for audit defense — same content, signed by the patient. The EHR record of either form is what matters; a paper consent in a folder doesn’t satisfy the certified EHR storage requirement.
Output of Step 2: A structured consent record in the EHR with date, method, witness, and practitioner. Billing logic should block CCM time entry until this record exists.
Step 3 — Time Tracking
Every CCM CPT code (except APCM, which is complexity-based, not time-based) requires accurate time documentation. The 20-minute, 30-minute, and 60-minute thresholds in the CPT codes are floors — minutes accumulate across the calendar month, not per encounter.
What counts as billable CCM time:
– Phone calls with the patient or family related to chronic conditions
– Care plan creation, review, and update
– Medication reconciliation and pharmacy coordination
– Specialty referral coordination
– Lab review and follow-up communication tied to chronic conditions
– SDOH assessment and referral coordination
– Communication with other care team members about the patient’s chronic conditions
What does NOT count:
– Time during a face-to-face E/M visit (that’s billed separately)
– Time during the initiating visit
– Time on conditions outside the documented chronic problem list
– Idle wall-clock time when the staff member isn’t actively engaged
– Time on care for an acute condition unrelated to the chronic management
How to capture time: EHR-embedded timers tied to specific care plan tasks are the gold standard. Spreadsheet logs and paper sheets are common but lose to audit scrutiny because they can’t prove start/stop times match real activity. The practical rule: every billable minute should connect to a specific care plan element with a date, duration, and staff attribution.
Cumulative tracking matters. A 5-minute call on the 8th, an 8-minute med rec on the 14th, and an 11-minute follow-up on the 26th = 24 cumulative minutes for that month, which clears the 99490 threshold. The biller doesn’t need to find a single 20-minute encounter — they need to verify the total clears the threshold.
Output of Step 3: A monthly time log per patient, attributable to staff or provider, tied to specific care plan activities, with start/stop or duration entries.
Step 4 — Code Selection
Once eligibility, consent, and time are in place, code selection follows the decision tree. Five questions decide which code applies:
Q1 — Who delivered the care?
- Clinical staff under general supervision → staff-time CCM (99490 or 99487)
- Physician or QHP personally → physician-time CCM (99491)
- A mix → choose ONE lane for the month; mixing within a single month produces denials
Q2 — How many minutes documented (in the chosen lane)?
- Staff-time lane:
– 20-39 minutes → 99490 only
– 40-59 minutes → 99490 + 99439 (one add-on)
– 60+ minutes WITH moderate-or-high MDM documented → 99487 (complex)
– 60-89 minutes complex → 99487 only
– 90+ minutes complex → 99487 + 99489 add-ons (each additional 30 min) - Physician/QHP lane:
– 30-59 minutes → 99491 only
– 60+ minutes → 99491 + 99437 add-ons (each additional 30 min)
Q3 — Was the initiating visit complex enough to warrant G0506?
Optional add-on for the initiating visit when the billing provider personally performed extensive care planning. Bill once per patient.
Q4 — Is APCM (G0556-G0558) better suited?
APCM removes minute tracking entirely. If the patient panel skews high social complexity or behavioral health comorbidity, APCM (G0557 or G0558, plus G0568-G0570 if applicable) often nets more revenue than minute-based CCM. APCM and CCM cannot both be billed for the same patient in the same month.
Q5 — Concurrency check. Before claim finalization, verify:
- No 99495/99496 (TCM) claim with overlapping service dates
- Patient has either RPM or RTM active, not both, if any
- No other practitioner has billed CCM for this patient this month
- Standard CCM (99490) and complex CCM (99487) are NOT being billed for the same patient in the same month
Output of Step 4: The correct CPT or HCPCS code (or code combination) selected for the patient-month, with concurrency check completed.
Step 5 — Claim Submission
The mechanics of submission are claim-system-specific (Epic Resolute, Cerner Patient Accounting, Athena, or third-party clearinghouses), but the elements that have to be on every CCM claim are universal.
Required elements on the claim:
- Patient identifier and Medicare beneficiary ID
- Date of service (typically the last day of the calendar month for which CCM is being billed)
- CPT or HCPCS code(s) selected in Step 4
- Diagnosis pointers — at least two ICD-10 chronic condition codes from the patient’s documented problem list
- Place of service (typically POS 11 for office, POS 22 for hospital outpatient — match to where the supervising practitioner is based)
- Billing provider NPI and rendering provider NPI
- Modifier(s) if applicable (rare for CCM; check MAC-specific guidance)
Pre-submission validation:
Before submission, the system (or biller) should validate:
- Eligibility record from Step 1 is in place
- Consent record from Step 2 exists and is dated before the first day of the service month
- Time log from Step 3 supports the code threshold for the code in Step 4
- Concurrency checks from Step 4 all clear
- Care plan in CEHRT exists and was updated within the service month
Any one of these failing should block submission, not produce a denial after the fact. The cleanest CCM programs fail fast on the inputs — they don’t let bad claims reach the payer.
What happens after submission:
A clean CCM claim typically pays within 30-45 days for traditional Medicare; Medicare Advantage plans vary by payer (some are 14-21 days, some run longer). Denials, when they happen, usually trace back to one of the upstream gates — missing consent date, time log can’t be reconciled to care plan, eligibility lapse, or concurrency overlap. Treat each denial as a signal to improve the upstream workflow, not as routine cleanup work.
Output of Step 5: A submitted, validated CCM claim with full audit trail back through Steps 1-4. The same documentation pack should be retrievable in seconds during an OIG audit.
What this walkthrough doesn’t cover
A few CCM billing variants need their own treatment and aren’t covered above:
- APCM-only programs skip Step 3 (no minute tracking) and use a complexity-based decision tree instead. The APCM behavioral health add-on codes (G0568, G0569, G0570) layer on top.
- RHC and FQHC billing post-September 2025 follows the same five steps as any other practice (G0511 transition completed). The codes used are individual CCM CPT, not the old G0511 flat rate.
- Hospital-based outpatient CCM uses facility-rate CPT pricing and POS 22 instead of POS 11.
For the deeper code-selection logic, the 2026 CCM CPT codes guide covers each variant in detail.
III. 2026 Billing Landscape – CPT and APCM Codes
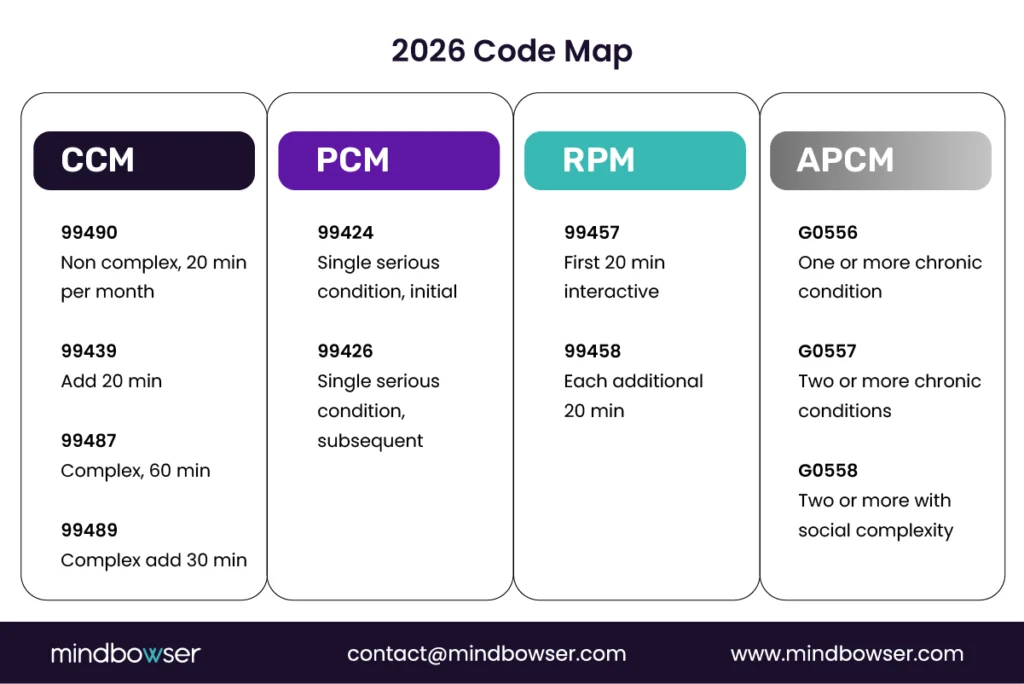
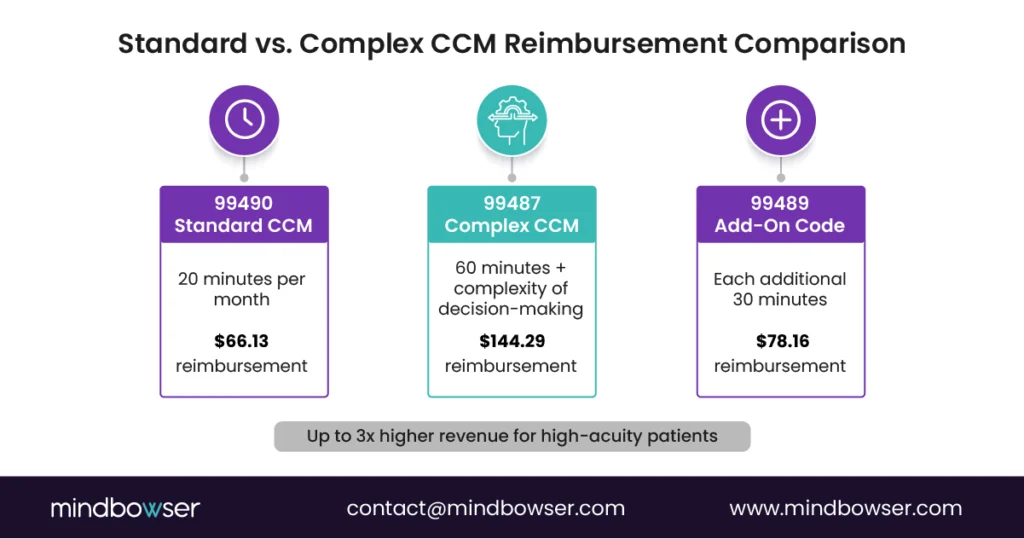
A. Standard CCM and Complex CCM Codes
Medicare’s CCM program continues to reward providers for structured, non-face-to-face care coordination. Payment amounts vary depending on time spent and complexity of care. All rates below reflect the CMS 2026 Physician Fee Schedule Final Rule (CMS-1832-F), effective January 1, 2026.
99490 — Non-complex CCM (20 minutes)
- $66.13 in non-facility settings
- $43.76 in facility settings
- Annualized: $794 to $525 per patient
99439 — Add-on for each additional 20 minutes
- $50.44 non-facility
- $30.73 facility
- Annualized: $605 to $369 per patient
99487 — Complex CCM (60 minutes)
- $144.29 non-facility
- $79.16 facility
- Annualized: $1,731 to $950 per patient
99489 — Add-on for each additional 30 minutes
- $78.16 non-facility
- $43.76 facility
- Annualized: $938 to $525 per patient
B. Physician and Qualified Health Professional Codes
Some providers prefer codes that specifically account for the time of physicians or advanced practice providers. These codes recognize higher levels of professional involvement.
99491 — 30 minutes of physician or qualified health professional time
- $89.18 non-facility
- $65.47 facility
- Annualized: $1,070 per patient (non-facility)
99437 — Add-on for each additional 30 minutes
- $63.13 non-facility
- $43.76 facility
- Annualized: $758 per patient (non-facility)
C. APCM Bundled Codes
The Advanced Primary Care Management codes represent a shift away from time-based billing toward patient complexity. For 2026, CMS increased APCM rates and expanded behavioral health integration support.
G0556 — Basic bundle for patients with zero or one chronic condition
- $16.37 per month
- $196 annualized
G0557 — Expanded bundle for patients with two or more conditions
- $53.78 per month
- $645 annualized
G0558 — Advanced bundle for patients with social complexity in addition to chronic conditions
- $117.24 per month
- $1,407 annualized
D. RHC and FQHC Billing After the G0511 Sunset
Historically, Rural Health Clinics and Federally Qualified Health Centers billed CCM services under G0511, a general care management code that bundled services into a flat rate. The G0511 transition completed on September 30, 2025. As of October 1, 2025, RHCs and FQHCs bill under individual CCM CPT codes, including 99490, 99439, 99487, and 99489, as well as APCM codes G0556, G0557, and G0558, the same way as other providers.
For RHCs and FQHCs that prepared early, this transition has created a 15–25% revenue uplift opportunity over the old flat G0511 rate because individual CPT billing rewards documented time and complexity. For RHCs and FQHCs still defaulting to G0511 in 2026, claims are denied automatically, making billing setup correction the highest-priority operational task.
The compliance bar is now the same as any other practice: consent in CEHRT, care plans in structured EHR data, time logs tied to care plan elements, and MDM evidence for complex CCM. The reimbursement upside is meaningful, but the documentation discipline required to capture it is real.
- CMS CY 2025 Physician Fee Schedule Final Rule, issued November 1, 2024, established the original G0511 transition window from January 1 through July 1, 2025. CMS Fact Sheet
- CMS Medicare Learning Network newsletter, June 5, 2025, extended the G0511 billing allowance through September 30, 2025. CMS MLN Newsletter
- Final sunset: September 30, 2025. Verified May 2, 2026, against multiple post-sunset industry references.
E. GPCM Codes: Enhanced Care Model Management Services (APCM Add-Ons)
The GPCM codes (GPCM1, GPCM2, and GPCM3) were introduced in the CY 2026 Medicare Physician Fee Schedule proposed rule as optional HCPCS G-codes designed to integrate Behavioral Health Integration (BHI) and Collaborative Care Model (CoCM) services into APCM without requiring time-based documentation. In the final rule, CMS finalized these codes under the designations G0568, G0569, and G0570, respectively. Both naming conventions appear in payer guidance and vendor documentation, so organizations should recognize either form.
These codes must be billed as add-on services when an APCM base code (G0556, G0557, or G0558) is reported by the same practitioner in the same calendar month. They cannot be billed independently. Unlike the CPT codes they are modeled after, no time tracking or minute documentation is required, which significantly reduces administrative burden and makes behavioral health integration more accessible for primary care practices.
i. GPCM1 (finalized as G0568): Initial Collaborative Care Model, First Calendar Month
- Mirrors CPT 99492 (initial psychiatric CoCM, first 70 minutes)
- Rate with 2.5% increase: approximately $166.58 per month
- Annualized: approximately $1,999
- Use case: First month in which a patient enrolled in APCM receives structured psychiatric collaborative care, including initial assessment, registry entry, and psychiatric consultant review
ii. GPCM2 (finalized as G0569): Subsequent Collaborative Care Model
- Mirrors CPT 99493 (subsequent month CoCM, 60 minutes)
- Rate with 2.5% increase: approximately $149.55 per month
- Annualized: approximately $1,794
- Use case: Ongoing monthly CoCM for patients already enrolled in APCM, covering caseload consultation, monitoring, and care plan updates in collaboration with a psychiatric consultant
iii. GPCM3 (finalized as G0570): General Behavioral Health Integration
- Mirrors CPT 99484 (20 or more minutes of BHI services per calendar month)
- Rate with 2.5% increase: approximately $58.43 per month
- Annualized: approximately $701
- Use case: Monthly BHI coordination for patients with behavioral or mental health conditions enrolled in APCM who do not require a full CoCM team; no psychiatric consultant required
Calculate your practice’s projected CCM revenue – CCM Revenue Calculator, Model your panel size, code mix, and denial rate to see annual net margin.
For A 1-Page Printable Reference With Every CPT Code, Rate, Time Threshold, And Denial Trigger
IV. Compliance and Audit Proof Billing
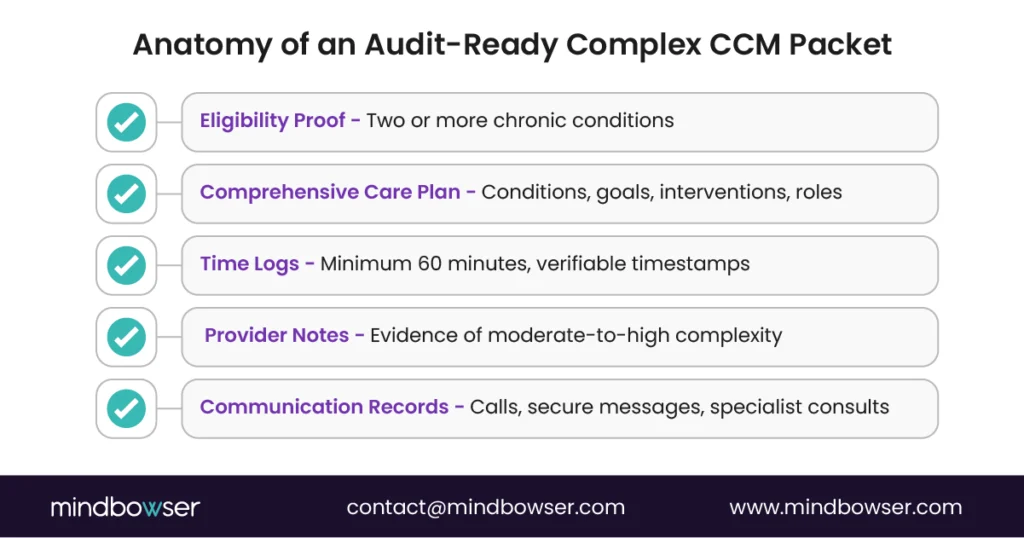
A. Supervision, Consent, and Documentation Rules
- Who can bill and how supervision works: Physicians, NPs, PAs, CNSs, and CNMs may bill CCM. Clinical staff can furnish services “incident to” the billing practitioner under general supervision, which means overall direction without being physically present. Document the supervising practitioner for each billed month.
- Patient eligibility: Patients must have two or more chronic conditions expected to last at least 12 months or until death, with risk of death, acute decompensation, or functional decline. Record the qualifying diagnoses in the chart.
- Initiating visit: Complete an initiating face-to-face visit for new patients or for patients not seen in the past 12 months. Bill it separately as an E/M visit, AWV, or IPPE. Do not count the initiating visit time toward CCM minutes.
- Consent: Obtain and document written or verbal consent before the first claim. The record should show patient cost sharing, that only one practitioner can bill CCM per month, and the patient’s right to stop at any time. Consent is only required once, unless the patient switches practitioners.
- Electronic care plan: Maintain a patient-centered electronic care plan with goals, interventions, monitoring, caregiver inputs, and periodic review. Make it available promptly across the care team and share a copy with the patient or caregiver when needed.
- 24 by 7 access and continuity: Ensure patients can reach clinical staff at any time and have a designated team member for routine appointments and secure messaging. Keep evidence of access pathways in policy and in the EHR.
- Concurrent billing rules: Do not report non-complex and complex CCM in the same month. Do not double-count time with other billed services. You may pair CCM with TCM, but follow the service period rules. You may bill CCM with RPM or RTM, but not both RPM and RTM in the same month. Keep a monthly conflict check.
B. Audit Artifacts Inside EHRs
- Minute log that survives an audit
- Who performed the work, what activity occurred, start and stop time, total minutes, and the supervising practitioner for the month.
- Store entries as read-only after the monthly close with a clear revision trail. Back the log with Provenance and AuditEvent, where available, to capture who, what, when, and from which system.
- Structured documentation aligned to CMS elements
- Care plan content, medication review, care transitions, and outreach attempts are tied to the month’s claim.
- Cross-reference each activity to the care plan and to patient communication records.
- Suggested EHR surfaces for teams
- Epic uses a SmartForm or flowsheet row for CCM activity type, minutes, and outcome; build a monthly report that rolls up by code.
- Cerner uses PowerForms and CareCompass tasks to capture work and minutes; it auto-attaches the care plan to the monthly summary.
- Athenahealth uses task queues and encounter documentation to track time and generate the monthly CCM summary note.
These are implementation patterns. Anchor each to the CMS required service elements and your organization’s policy manual.
- RHC and FQHC transition tracking: If you are moving from G0511 to individual CPT and APCM codes, keep a payer-specific control sheet and show the final month billed under G0511. CMS extended the G0511 deadline to September 30, 2025.
C. FHIR and HL7 Mapping for Billing Proof
- Core resources to prove the story.
- Condition for qualifying chronic diagnoses.
- CarePlan for goals, interventions, and review dates that match the billed month.
- Task for discrete CCM activities with performer, status, due date, and completion. Map a minutes field via extension or system metadata.
- Communication or CommunicationRequest for phone calls and secure messages tied to the care plan.
- Encounter for billable face-to-face touchpoints, including the initiating visit.
- Consent for documented patient consent to CCM.
- Provenance and AuditEvent to bind each entry to a user, time, and system for audit.
- How does this prevent denials?
- The Condition and CarePlan show eligibility and the care plan elements CMS expects.
- Task plus Provenance creates an immutable minute trail.
- Communication records resolve disputes about outreach.
- Consent satisfies the one-time consent requirement.
- Monthly close package. Generate a CCM monthly summary that references the above resources and lists total minutes, activities, conflicts checked, and the code billed. Keep a copy in the record and attach it to the claim if your clearinghouse supports documentation links.
Implementation note for Pop Health and CTO teams
- Build a pre-bill rules engine that checks consent on file, initiating visit date, minutes by staff type, overlapping services, and payer-specific edits before a claim is created.
- For RHC and FQHC, include a switch that selects G0511 through September 30, 2025, where your MAC guidance applies, then flips to CPT and APCM codes on October 1.
To understand how documentation gaps lead to denials and how to prevent them, see our CCM audit risk and protection guide.
V. ROI Sensitivity in CCM and APCM
A. The 2025 Medicare Conversion Factor Cut
In 2025, Medicare implemented a 2.83% reduction to the physician conversion factor. While the adjustment may seem small, it has a ripple effect across all professional services, including chronic care management. For hospitals and physician groups with thin margins, the reduction means less reimbursement per RVU. Pop Health leaders must account for this decrease when projecting revenue from CCM and APCM programs as part of broader revenue cycle management strategies.
A full breakdown of updated reimbursement rates is covered in our Medicare chronic care management payment guide.
B. ROI Waterfall: Variables That Drive Financial Outcomes
A structured view of the economics helps leadership teams make informed decisions. The following variables drive return on investment for CCM billing:
- Patient volume. The number of eligible patients enrolled is the largest driver of revenue. Even a modest increase in enrollment can offset lower reimbursement rates.
- Patient complexity. APCM codes pay more for patients with higher needs or social complexity. Patient mix can significantly impact total reimbursement.
- Payer mix. Commercial payers often mirror CMS policies, but at different rates. Tracking the proportion of Medicare, Medicaid, and commercial patients is critical for accurate projections.
- Staffing model. The cost of nurses, care coordinators, and technology support has a direct impact on ROI. Outsourcing versus in-house staffing will change the margin profile.
- Denial rates. Even well-designed programs lose revenue if documentation does not meet audit standards. Each percentage point reduction in denials increases realized revenue.
C. APCM versus CCM Economics
Organizations must decide when to use traditional CCM codes and when to shift to APCM. The choice depends on patient mix and workflow design.
- For lower complexity patients. Traditional CCM codes may offer more stable reimbursement since they are time-based. If staff can consistently meet the 20-minute requirement, CPT 99490 and its add-ons may yield better returns than G0556.
- For patients with multiple chronic conditions. APCM codes such as G0557 can outperform traditional CCM. Payments are tied to complexity rather than time, which reduces administrative burden and audit exposure.
- For patients with high social complexity. G0558 offers more than $100 per month, making it one of the most valuable billing options. Providers serving underserved or high-risk populations may see a higher ROI by moving quickly to APCM.
- Parallel billing with RPM. For patients using remote monitoring, organizations must carefully separate minutes. In some cases, combining CCM with RPM may outperform APCM. This requires strict rules in the billing engine and clear EHR documentation.
Every Chronic Care Management program has three levers that directly affect financial performance: enrollment, claim integrity, and denial prevention.
In a hospital generating $5 million annually from Chronic Care Management billing, a 1% increase in denial rates equals $50,000 in lost revenue.
ROI Sensitivity Table
This ROI view provides CFOs, Pop Health leaders, and CTOs with a clear lens into how coding choices, patient mix, and staffing structures impact outcomes.
Download the CCM Audit Readiness Checklist
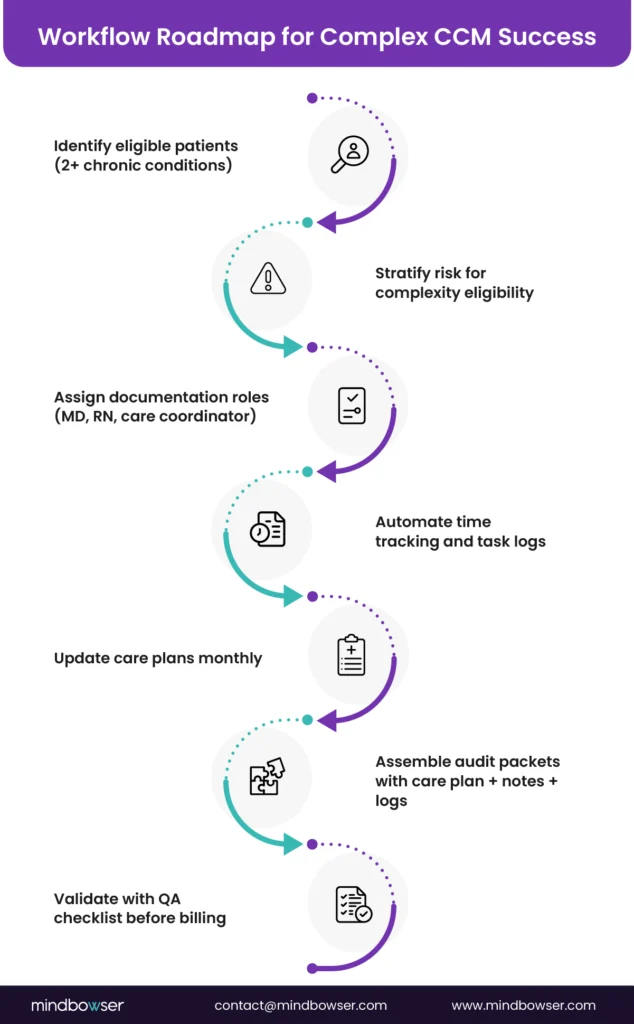
VI. Engineering CCM Billing Workflows
Scaling CCM requires more than coding knowledge—it demands a structured workflow. The roadmap below shows how high-performing programs operationalize complex CCM.
A. EHR Surfaces That Make Billing Reliable
- Minute logging at the point of work
Build a single place where staff record what was done, for whom, how many minutes, and the activity type. Use discrete fields for start time, stop time, activity code, and outcome. Lock entries after the monthly close and keep a revision trail. - Consent capture and verification
Store the original consent as a structured flag with date, modality, and the staff member who obtained it. Add a prebill check that blocks claims if consent is missing or expired. Show consent status in the care manager’s daily view. - Care plan versioning
Keep a living electronic care plan with goals, interventions, barriers, and target dates. Save a monthly snapshot so your “story of care” matches the billed month. Reference the snapshot in the billing note. - Outreach documentation that ties to the care plan
Log phone calls, secure messages, and education touchpoints with a direct link to the relevant goal or task. Categorize each touchpoint as billable or non-billable to prevent accidental time inflation. - Multi-specialist conflict detection
Surface a monthly banner that lists other known CCM billers for the patient, including the PCP and any specialists. Ask staff to confirm who the billing practitioner of record is. Record the attestation on the first contact of the month. - Monthly close packet
Auto-generate a summary that includes total minutes, activity breakdown, consent status, initiating visit date, conflict check result, and the code chosen. Store it as a read-only document and attach it to the claim if your clearinghouse supports documentation links. - Suggested placements by EHR
- Epic: SmartForm or flowsheet row for activity and minutes, plus a Reporting Workbench report that rolls up by patient and month.
- Cerner: PowerForm for activity capture, CareCompass tasks for work queueing, and a monthly MPages view that drives the close packet.
- athenahealth: Task queues for activity, a problem-oriented encounter note for the monthly summary, and a custom report for minutes.
- MEDITECH Expanse: PCS assessment for minutes and tasks, with a registry-style report for rollups.
- Healthie or Canvas: Build a care plan object with tasks, a visit timeline, and a monthly export that feeds claims.
B. Interoperability Gaps and How to Reduce Them
- Patient identity
Use a master patient index or a deterministic match to avoid duplicate charts. Minute logs tied to the wrong record cause denials and make audits difficult. - HL7 v2 and FHIR in the same program
Expect to run both. Use v2 for admissions, discharges, and results, and FHIR for care plan, task, and documentation elements. Map IDs across both so billing references are consistent. - Time tracking across systems
If staff work in a care management tool outside the EHR, post back a daily summary with minutes and activity types. Keep the system of record for minutes inside the EHR or a single approved adjunct system to avoid reconciliation wars. - Claims and attachments
Agree on a standard for monthly summaries that your clearinghouse can handle. If attachments are not supported, include a claim note that points to the internal document ID and keep it ready for payer requests. - Consent portability
When patients change practitioners, store a clear “consent released” state and the date. This prevents two organizations from billing the same month by mistake. - Data latency and retries
Queue events for minutes and tasks. Use idempotent writes so resubmits do not double-count time. Show staff a real-time counter that reflects posted minutes, not pending minutes.
C. Automation Patterns That Cut Denials
- Conflict checker
- Checks before claim creation
a. Consent on file for the current practitioner
b. Initiating visit within the required window
c. Minutes threshold met for the target code
d. Overlap with other monthly services such as complex CCM, PCM, or TCM
e. Known external biller on the same patient for the same month - Result handling
a. Hard stop for missing consent or initiating visit
b. Soft warning for potential duplicate biller with a space to document the outreach and resolution
- Checks before claim creation
- Add on triggers and safe downgrades
- If minutes for non-complex CCM exceed 20 plus 20, suggest 99439 as an add-on to 99490
- If complex CCM minutes are short of 60 at month close, downgrade to non-complex if allowed, with staff sign-off.
- Never auto-upcode without staff confirmation
- Payer edit packs
- Maintain a payer-specific rule set for place of service, supervising practitioner type, and documentation notes.
- Keep effective dates and versions so you can show what rule was applied at the time of billing.
- Flag payers that require claim-level notes for care plan availability or after-hours access
- RHC and FQHC code switch
- Maintain a facility-level toggle that applies the correct code set by date.
- Show staff which codes family will apply at the start of each month so they can target minutes and documentation correctly.
- RPM minute segregation
- Keep a separate counter for interactive RPM minutes that resets monthly.
- Do not let RPM interactive minutes flow into CCM minutes.
- If a touchpoint includes both CCM and RPM activities, staff must split the time and record two entries.
- Work queues that match revenue risk
- Priority 1 patients with high expected reimbursement or expiring minutes
- Priority 2 patients missing consent or initiating visit.
- Priority 3 patients at risk for concurrency conflicts with specialists
- Operational dashboards
- Enrollment funnel: eligible, consented, enrolled, active
- Minutes distribution: average minutes per patient, add-on utilization, complex CCM rate
- Denials: by reason, by payer, by location
- Staff productivity: average billable minutes per FTE, documentation completion time
- Monthly close playbook
- Freeze entries after a set hour on the first business day
- Run the conflict checker and present exceptions for resolution.
- Generate the close packet and store the hash or checksum of the document for integrity.
- Submit claims in a batch with a manifest that lists patient counts, codes, and expected amounts.
D. Example Rules in Plain Language
- Only one organization can bill CCM per patient per month: If you learn another group intends to bill, decide who will own the month and document the agreement.
- Do not mix complex and non-complex CCM in the same month: If staff members cross categories, choose the one that best fits the documentation and minutes, then remove the other entries.
- Do not double-count minutes: Education, coordination, or monitoring time can be recorded once and linked to the correct service.
- Every billed month must have a care plan snapshot: If the plan did not change, still save a snapshot and reference it in the note.
- Every add-on requires the base code: If the base code is missing, the add-on will be denied.
E. Build Order for CTO and Pop Health Teams
- Stand up minute logging and consent flags.
- Add the conflict checker with hard and soft stops.
- Produce the monthly close packet and lock the audit trail.
- Wire the payer edit pack and code switch for RHC and FQHC locations.
- Integrate RPM segregation and concurrency checks.
- Turn on dashboards and weekly exception reviews.
VII. Case Study POVs
A. Building Sustainable Engagement with Remote Monitoring
One health system serving elderly patients recognized that consistent engagement was its weakest link in chronic care management. Patients frequently missed daily checks and follow-ups, which left the organization vulnerable to both clinical risks and billing denials. To address this, the system deployed a remote monitoring portal that is integrated with Bluetooth-enabled blood pressure cuffs and heart rate monitors.
The result was a daily adherence routine tied directly to structured tasks for care managers. Patients could see reminders in a simple to-do list, while care teams accessed real-time dashboards of vitals and historical trends. Engagement reached nearly 90 percent across elderly users. Administrators cut reporting time in half because the system produced structured summaries aligned to billing requirements. This resulted in a higher throughput of valid claims without the need for additional staff.
B. Driving Readmission Reduction Through Behavioral Health Integration
A regional provider network faced rising costs and repeat admissions for patients with behavioral health needs. Traditional chronic care management models did not account for transportation, housing, or access to social services, which left patients without a coordinated path forward.
The organization created an integrated care platform that blended medical, behavioral, and social data. Using a central intelligence suite, care teams coordinated referrals, tracked appointments, and connected patients with community resources. Patients received reminders and surveys through mobile engagement tools.
The impact was measurable: readmissions dropped by more than half, and the system avoided hundreds of thousands of inpatient days. Medicaid plan costs fell significantly, validating that CCM billing paired with wraparound behavioral health support can deliver both financial and clinical outcomes.
C. Automating Billing and Financial Clearance with EHR Integration
Another provider group struggled with delays in obtaining financial assistance approvals for patients with chronic care needs. Manual data collection on demographics, insurance, and diagnoses created errors and slowed access to support. This not only delayed care but also created billing gaps and compliance risks.
By integrating directly with its Epic EHR, the group automated ingestion of demographics, coverage data, and medical information using HL7 and FHIR standards. The system triggered real-time updates when new patient events occurred and pulled precise data through FHIR calls for eligibility verification.
As a result, manual entry was reduced by 90%. Approvals were processed faster, patients gained access to needed assistance, and billing staff could trust that data matched the payer requirements. Compliance audits became smoother since structured logs showed every step of the eligibility process.
Book a CCM Billing Workflow Workshop to See How Custom RCM Software Can Automate Compliance, Cut Denials, and Boost ROI
VIII. Accelerator Tie Ins
A. Documentation and Care Plan Creation
- AI Medical Summary
This tool creates a structured summary from the patient record and recent encounters. It pulls diagnoses, medications, allergies, and recent tests into a concise view that a care manager can review in minutes.- What it solves: Missing or inconsistent problem lists and underdocumented comorbidities.
- How it helps billing: Faster care plan updates, cleaner eligibility proof, and fewer denials linked to incomplete histories.
- Implementation: Run the summary before monthly outreach. Post a dated copy to the chart and link it to the care plan snapshot for that month.
- CarePlan AI
This tool converts goals and barriers into a live care plan with due dates, tasks, and owner assignments. Reported improvements include higher patient understanding and fewer coordination delays.- What it solves: Care plans that are static, vague, or not aligned to monthly activities.
- How it helps billing: Each billable minute can be tied to an active task or goal. This creates a clear chain from activity to plan to claim.
- Implementation: Require a care plan refresh at the start of each billing month. Save a snapshot after the close so the billed code matches the plan in force.
B. EHR and Device Connectivity
- ConnectHealth
A connectivity layer that moves discrete data into Epic, Cerner, athenahealth and collects data from hundreds of wearables and home devices into a single stream.- What it solves: Siloed care management tools and manual rekeying.
- How it helps billing: Minutes, tasks, and consent flags land in the system of record, which reduces reconciliation disputes and supports audits.
- Implementation: Map patient identity and use a single source for minutes. Post back daily summaries so the EHR holds the authoritative monthly total.
C. Adherence and Monthly Minute Integrity
- MedAdhere AI
A reminder and follow-up engine for medications and self-care steps.- What it solves: Missed doses, missed education steps, and poor self-management.
- How it helps billing: Increases the chance that outreach is meaningful and tied to a specific plan task. Reduces no-value calls that do not support billable time.
- Implementation: Trigger reminders from the care plan. Record patient responses in the chart and link them to the month’s tasks.
- RPMCheck AI
A check in workflow for device-based programs.- What it solves: Inconsistent device use and unclear follow-up rules.
- How it helps billing: Keeps RPM and CCM streams separate. Staff know when to record RPM interactive time and when to log CCM coordination time.
- Implementation: Add a simple rule. If the contact addressed device setup or parameter coaching, log under RPM. If the contact coordinated services, updated goals, or handled non-device issues, log under CCM.
D. Patient Data Capture and Education
- AI-powered chat and call questionnaires.
Guided chat or voice calls collect vitals, symptoms, and barriers in a structured format.- What it solves: Unstructured notes that do not map to planned tasks or claims.
- How it helps billing: Produces discrete fields for symptoms, adherence, and social barriers that can be tied to tasks and minutes.
- Implementation: Use short pre-visit questionnaires. Post responses as structured observations and attach them to the care plan review.
- EduCare AI
Personalized education delivered through simple messages and quick calls.- What it solves: Low comprehension and repeated questions that consume staff time.
- How it helps billing: Education touches are documented with topic, time, and outcome. The record demonstrates why the outreach was necessary and what changes were made to the plan.
- Implementation: Assign content by diagnosis and reading level. Confirm understanding with a short quiz and record the score.
- HealthCheck AI
Automated reminders for labs, blood pressure logs, or follow-up visits.- What it solves: Missed data points that stall care plan progress.
- How it helps billing: Ensures required steps are completed within the month, allowing staff to complete tasks and meet time thresholds with less chasing.
- Implementation: Tie reminders to the plan’s due dates. If a patient misses a step, open a task and route it to the correct queue.
E. Risk Stratification and Outreach Targeting
- AI Patient Readmission Risk
A scoring model that highlights patients likely to be readmitted in 30 days.- What it solves: Flat outreach that treats all patients the same.
- How it helps billing: Directs staff toward patients who will benefit most from CCM outreach. Higher clinical yield often translates into clearer documentation and fewer denials.
- Implementation: Prioritize the top risk tier in weekly work queues. Require a care plan update and post-discharge follow-up within seven days for all flagged patients.
- AI Cardiovascular Risk Prediction
Risk scoring for patients with common comorbidities such as diabetes or hypertension.- What it solves: Late recognition of worsening risk.
- How it helps billing: Timely outreach tied to a documented risk change supports the medical necessity narrative for monthly claims.
- Implementation: Run scores nightly. When risk increases, open a task and schedule a call. Attach the score change to the monthly summary.
F. Putting it Together in the Billing Engine
- Trigger a pre-bill check that verifies consent, initiating visit date, completed plan tasks, minute totals by staff type, RPM segregation, and concurrency conflicts.
- Use add-on recommendations that appear when minutes cross thresholds. Always require staff confirmation to avoid upcoding.
- Generate a monthly close packet that pulls plan snapshots, tasks completed, communications, and total minutes. Save the packet as read-only and store a checksum for integrity.
- Track denial reasons by payer and accelerator. When an accelerator reduces a specific denial reason, document the before and after rates and share the playbook across teams.
IX. Buyer’s Checklist (Pop Health and CTO)
A. Program Design and Eligibility
- Confirm eligibility logic: Two or more chronic conditions documented, expected to last at least 12 months, and risk criteria recorded in the chart.
- Verify initiating visit process and cadence: Who performs it, how it is scheduled, how it is tracked, and how it is excluded from monthly CCM minutes.
- Standardize consent: Single source of truth, date and modality captured, renewal policy, and a prebill check that blocks claims if consent is missing.
B. Coding Strategy and Code Selection
- Define when to use non-complex CCM, complex CCM, or Principal Care Management.
- Establish APCM selection rules by patient complexity and social risk.
- Create RPM pairing guidance that prevents double-counting minutes and clarifies what work belongs to CCM vs RPM.
C. Documentation and Audit Artifacts
- Minute logs: Start and stop time, activity type, performer, and supervising practitioner with a locked monthly close.
- Care plan snapshots: Monthly version saved with goals, interventions, and outcomes that match the billed code.
- Conflict checks: One practitioner per month, no mixing complex and non-complex CCM in the same month, and documented outreach to resolve potential overlaps.
D. EHR and Interoperability
- Map Conditions, CarePlan, Tasks, Communication, Encounter, Consent, and audit events in your EHR or care management tool.
- Post daily summaries back to the EHR if staff work outside of it, so the EHR remains the system of record.
- Maintain a payer attachment strategy for monthly summaries and a fallback claim note when attachments are not supported.
E. RHC and FQHC Operations
- Maintain a facility switch that controls whether the system uses legacy care management billing or the current CPT and APCM structure.
- Train staff on new documentation standards that align with CPT and APCM so rural sites meet the same audit bar as larger systems.
- Keep a payer-specific control sheet that shows effective dates and any local MAC nuances.
F. Staffing and Productivity
- Define role-based targets for billable minutes and documentation completion.
- Run weekly reviews of “minutes close to threshold” and “patients with high expected reimbursement” to focus outreach.
- Track denials by reason and payer; close the loop with targeted coaching and rule updates.
X. Common Objections and Answers
A. “Implementation is Too Complex”
Answer: break the work into small, testable steps.
- Start with a minimum viable CCM stack. Minute logging, consent flag, monthly close packet, and a simple conflict check.
- Define acceptance tests.
- A care manager can record an activity with a start and stop time.
- A supervisor can see the total minutes by patient for the month.
- The system blocks a claim if consent is missing.
- A monthly close packet is produced with totals and a sign-off.
- Use a RACI chart. Assign who builds screens, who writes policy, who audits, and who owns change control.
- Run a pilot in one clinic. Ten providers, two care managers, ninety days. Stabilize, then roll out.
30, 60, 90-day Plan
- 30 days: build minute logging and consent flags, train two super users.
- 60 days: add conflict checker and payer edit rules, generate the close packet.
- 90 days: expand to RPM pairing, add dashboards, and publish the standard operating procedure.
B. “Audit Risk is Too High”
Answer: design records that tell the story in a clean, consistent way.
- Monthly close packet. Totals, activity breakdown, care plan snapshot, consent status, initiating visit date, conflict check, and the code billed. Lock it after submission.
- Structured fields. Activity type, goal or task, minutes, and outcome. Avoid free text for critical elements.
- Policy excerpts to include in your manual.
- Only one organization bills CCM per patient per month.
- Complex and non-complex CCM cannot be billed in the same month.
- RPM interactive minutes are recorded separately from CCM minutes.
- Internal audits. Sample five percent of claims monthly. Check documentation against policy. Track issues by type and fix the root cause.
What good looks like
- No missing consent in the sample.
- Care plan snapshot is present for every billed month.
- Variance between recorded minutes and billed code under two percent.
C. “ROI is Uncertain”
Answer: Use a simple model, measure weekly, and tune code selection rules.
- Create a working model. Inputs include the number of enrolled patients, the mix by complexity, average reimbursement per patient, denial rate, and staffing cost per patient per month.
- Run three scenarios. Low, base, and high. Update with real results every month.
- Track leading indicators. Enrollment rate, percent with consent on file, average minutes per patient, add-on utilization, and denial rate by reason.
- Tighten the rules. If many patients fall just short of thresholds, adjust outreach cadence and task design. If denials cluster on documentation, retrain staff and simplify the note template.
Finance checkpoints
- Break-even month is identified before going live.
- Unit economics per patient per month were reviewed at day 30 and day 60.
- Quarterly decision on APCM versus CCM mix by site.
D. “We Cannot Spare Clinicians or Nurses”
Answer: Redesign roles so licensed staff handle only what requires a license.
- Team structure. Use a registered nurse for assessment, goal setting, and escalations. Utilize medical assistants or health coaches for education, coordination, and follow-up calls.
- Escalation ladder. If a symptom screen is positive, route to a nurse within the same day. If a medication issue is reported, route to the prescribing clinician within two days.
- Templates that save time. Short, structured checklists linked to the care plan.
- Productivity targets. Average billable minutes per full-time care manager, average time to documentation close, and successful outreach rate.
E. “EHR Integration Will Delay Us”
Answer: Take a phased approach that protects the source of truth.
- Phase one. Work in the EHR or a connected tool and post a daily summary back to the EHR, ensuring the EHR maintains the official minutes and consent status.
- Phase two. Move to near real-time posting of activities and tasks.
- Data map. Patient identity, care plan ID, task types, activity codes, minutes, consent flag, and initiating visit date.
- Cutover rules. Decide which system is the system of record for minutes. Do not allow dual entry.
F. “Patients Will Not Enroll or Stay Engaged”
Answer: fix the offer, the script, and the follow-through.
- Enrollment script.
- Benefit statement in one sentence.
- What it costs the patient and what it covers.
- How to stop participation at any time.
- Consent at the right moment. Ask at discharge, during a telehealth visit, or during a medication refill touchpoint.
- Outreach cadence. First week after enrollment, then monthly, with a clear purpose tied to the care plan.
- Measure and tune. Reach rate, consent rate, active rate, and monthly churn. Test different times of day and channels.
G. “APCM Versus CCM is Confusing”
Answer: Use a decision tree that staff can follow.
- If time tracking is reliable and patients reach thresholds. Use traditional CCM codes.
- Suppose patient complexity and social risk are well documented. Use APCM for those patients.
- Suppose RPM is active and yields a strong interactive time. Consider CCM plus RPM rather than APCM for that segment.
- Governance. Review the mix monthly. Update the rule set and retrain staff when the payer environment changes.
H. “RHC and FQHC Sites Cannot Meet Documentation Standards”
Answer: standardize the workflow and give rural teams the same tools.
- Facility toggle. The system selects the correct code set based on location and date.
- One-page checklist. Eligibility, consent, care plan snapshot, minutes total, and conflict check.
- Short training sprints. One hour per week for four weeks. Show staff how to record minutes, update plans, and run the monthly close.
- Central review. A small central team reviews the first two months of claims from each site and provides coaching.
I. “Concurrency with Specialists Will Cause Denials”
Answer: Make ownership clear every month.
- Attribution record. One billing practitioner of record per month.
- Outreach protocol. If another group plans to bill, contact the group, agree on ownership for the month, and record the outcome in the chart.
- Patient communication. Explain who is responsible for coordinating this month and how to reach the team.
- Prebill check. The claim does not go out until ownership is confirmed.
J. “Minute Counting is Error Prone”
Answer: capture minutes at the point of work and lock them after close.
- Simple timer or start and stop fields—no guesswork at the end of the day.
- Activity types. Education, coordination, medication management, care plan review, and transitions.
- Read only after close. Changes require a supervisor and create an audit trail.
- Reconciliation report. Minutes by activity compared to billed codes. Outliers get reviewed before submission.
K. “Staff are Tired of New Documentation”
Answer: remove keystrokes and reward good behavior.
- Short forms. Two clicks to record a common activity, not ten.
- Auto fill. Pull the care plan goal into the activity note.
- Coaching, not punishment. Share weekly wins. Highlight denials avoided through good documentation.
- Feedback loop. Ask the staff what takes the most time. Fix one issue each sprint.
L. “We Fear Payer Policy Changes”
Answer: Version your rules and keep the history.
- Payer edit packs with effective dates. Staff can see what rule applies now and what changed last quarter.
- Change review. Once a month, confirm the rule set against payer bulletins.
- Playbook updates. When a rule changes, push a micro-lesson to staff and update the pre-bill checker.
XI. How Mindbowser Can Help
A. Compliance and Billing Automation
- Mindbowser builds custom chronic care management software that integrates directly with Epic, Cerner, Meditech, and Athena.
- Our solutions automate time tracking, add on code triggers, and payer-specific edits to reduce denials.
- Audit-ready logs and FHIR-native evidence design ensure compliance with CMS requirements.
B. Integration with RPM, Wearables, and Care Coordination
- Through ConnectHealth, we connect 300-plus devices and apps into the billing workflow.
- RPM minutes are automatically segregated from CCM time to prevent billing conflicts.
- This integration supports a seamless experience for patients while protecting revenue for providers.
C. ROI Focused Implementation
- We utilize ROI sensitivity modeling to help organizations forecast the revenue impact under various patient volumes and complexity levels.
- Our case work with behavioral health, telehealth, and financial assistance platforms shows how CCM billing can reduce readmissions and improve margins.
- By combining compliance and financial insights, we give leaders confidence that CCM and APCM programs will deliver measurable returns.
D. Outsourcing and Scale Support
- Mid-market hospitals and digital health startups often face staffing shortages.
- Mindbowser offers outsourced enrollment support, virtual nursing, and billing administration to extend internal teams.
- Our flexible model allows organizations to balance in-house control with outsourced scale.
E. Custom Billing-Logic Build — 76% Denial Reduction
A custom care platform built for a maternal-health program embedded billing logic directly into the clinical workflow rather than reconciling claims after submission. The clinical focus was obstetric, but the billing-automation pattern is identical to what CCM programs need: structured documentation captured at the point of care, claims rules validated before submission, and audit artifacts linked to every billed code.
Outcomes from the billing work:
– 76% reduction in coding denials
– ±12-minute prediction accuracy on care plan timing
– EHR-embedded billing capture at the point of clinical work, eliminating downstream reconciliation cycles
Why this matters for CCM: A 5% denial rate on a $5 million CCM program costs $250,000 a year. Cutting that to 1% recovers $200,000 — enough to fund two coordinators, an EHR upgrade, and still leave margin. The 76% reduction on the maternal-health build proves the lever isn’t theoretical: validate eligibility, consent, care plan, and time threshold before the claim is generated, not after.
Every concurrency check, every MDM documentation requirement, every initiating-visit reference — caught at the moment the staff would otherwise commit the error. Denial rate drops because the upstream conditions for denial are blocked before they reach the claims system.
The same pattern moved from maternal-health to CCM with no architectural change. The codes are different; the workflow design is the same.
Conclusion
Chronic care management billing in 2026 is a revenue and quality lever, not a paperwork exercise. Leaders who align code strategy, EHR evidence, and staffing can protect margins while improving patient outcomes. Use APCM where complexity is documented. Use traditional CCM where time thresholds are reliable or RPM pairing adds lift. Build a prebill rules engine, lock monthly close packets, and track denials by reason.
Start small—pilot one site for ninety days. Measure consent rate, minutes per patient, add-on utilization, and denial trends. Tune code selection monthly based on real data. The result is fewer write-offs, faster cycles, and a program that scales safely.
CCM billing continues to use CPT codes such as 99490, 99439, 99487, and 99489. APCM introduces new HCPCS codes G0556, G0557, and G0558 that align payment with patient complexity rather than time.
G0511 will sunset by September 2025. RHCs and FQHCs can now bill using the same CPT codes as physician practices, which improves alignment across care settings.
CCM and RPM can both be billed in the same month if services are documented separately. RPM minutes cannot be double-counted toward CCM thresholds. Accurate segregation of time is essential to avoid denials.
Providers should maintain accurate records of patient consent, time logs, care plan updates, and staff documentation. Audit trails must be accessible through the EHR and tied to FHIR objects such as Condition, CarePlan, Encounter, and Task.
APCM may be the better choice when patient populations have multiple chronic conditions or social complexity factors. CCM plus RPM may remain optimal for patients or organizations with lower complexity and an established RPM infrastructure.

