



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 
























TL;DR
- Triggers that blow up CCM revenue: The fastest way to get denied is still the “big three” documentation gaps: time logs that don’t reconcile, missing consent or care plan, and notes that read like filler.
- Prevention that works before the claim leaves your shop: Implement pre-claim validation before billing, so claims can’t pass unless time, consent, and the active plan are present and linked. Build the packet as care is being taken, not after the letter arrives.
- ROI logic your CFO will respect: In one engagement, documentation automation reduced coding denials by 76% – a direct result of eliminating manual entry gaps before claims were filed.
- Accelerators that shrink compliance effort (without adding headcount): Mindbowser’s FHIR-native approach supports audit defense by design, and published outcomes include 50% less clinician documentation time with AI Medical Summary, plus 60% less physician review time in CCM workflows.
If CMS audited your CCM program tomorrow, could you prove every billed minute without scrambling?
That is the question hospital CFOs, compliance officers, and RCM leaders should be asking now. Not whether care was delivered, but whether time, consent, and interventions can be produced quickly, consistently, and without gaps under audit pressure.
Chronic Care Management has become a meaningful revenue stream. It has also become a high-scrutiny billing category.
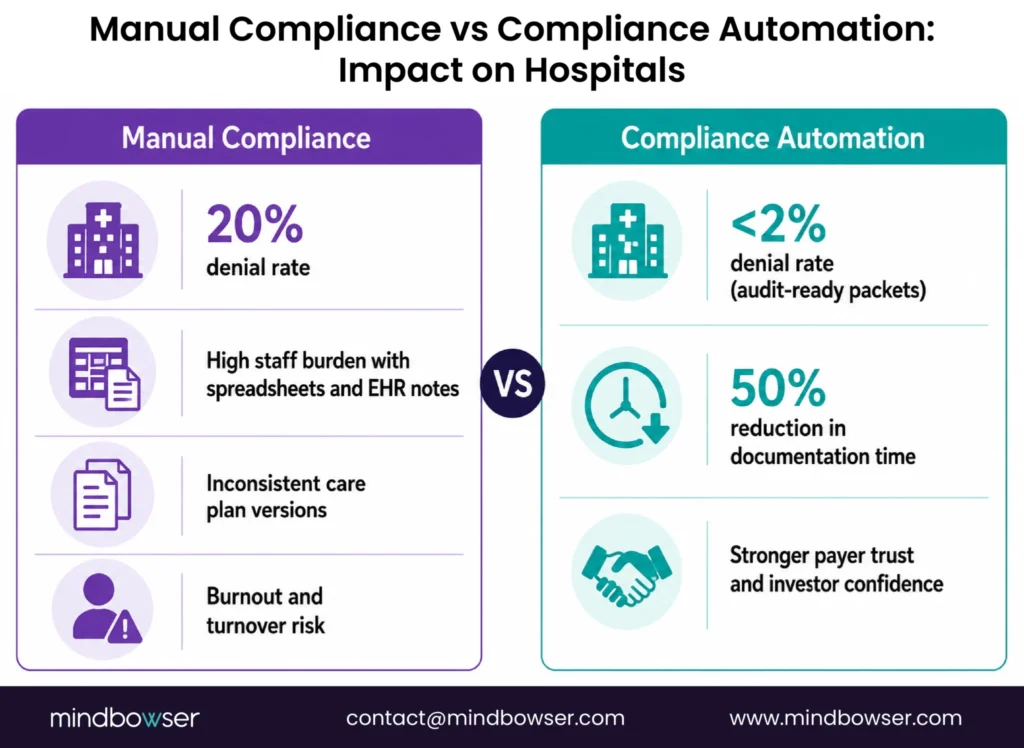
CCM is time-based, documentation-heavy, and unforgiving when proof is fragmented. Industry data shows denial rates exceeding 20% when documentation is incomplete, driven by the same repeat issues: mismatched time logs, missing consent or care plans, and vague intervention notes.
The shift since 2025 is not just more audits, but more deterministic audits. Payers are validating against structured expectations such as eligibility proof, CPT-aligned time thresholds, concurrency rules, and care plan accessibility. If these elements cannot be retrieved in a consistent format, the claim is treated as non-compliant regardless of care quality.
The old playbook waits for denials, then scrambles to reconstruct records. That approach no longer holds up as audits increase and lookback windows expand. Audit defense now starts before the claim is filed.
This playbook outlines how to move from reactive cleanup to proactive CCM audit defense, leveraging pre-claim validation, audit-ready documentation, and compliance-first, FHIR-native platforms to protect revenue before it is at risk.
I. The CCM Audit Landscape (What Auditors Are Testing First)
CCM audits are not fishing expeditions. They follow a narrow set of rules tied to time-based CPT billing and proof integrity, and CMS attention on CCM has intensified in 2025 as utilization and payouts grow.
For RCM and compliance leaders, the takeaway is simple. Audits are predictable. Losses are preventable.
Why CCM Draws Disproportionate Scrutiny
CCM reimbursement is not procedure-driven. It is minute-driven. Every dollar depends on whether staff can prove that the qualifying time was spent, consent was secured, and care activities met CPT intent.
Industry data shows CCM denial rates exceeding 20% when documentation is incomplete, a level that materially erodes margins in mid-market hospitals and scaled digital health programs. These denials rarely reflect poor care. They reflect missing or misaligned proof.
Organizations with lean compliance teams or fast-growing volumes are most exposed. Manual reconciliation does not scale. Small documentation gaps repeat across hundreds of patients. Auditors know this and test accordingly.
From a systems perspective, CCM has become one of the easiest programs for auditors to validate programmatically. Time-based billing, discrete CPT thresholds, and structured documentation requirements make it ideal for automated audit checks. This means organizations relying on manual reconciliation are inherently at a disadvantage.
The Three Triggers Behind Most CCM Denials
Across payer audits, the same failure points keep surfacing.
- Time mismatch across systems
When EHR timestamps, call logs, and billed totals do not reconcile, auditors assume an error or overstatement. Even minor discrepancies can invalidate a full month of CCM claims. - Missing consent or active care plan
CCM requires documented patient consent and an individualized, current care plan. If either is absent or outdated, the claim fails regardless of the care delivered. - Vague intervention documentation
Notes like “care coordination provided” do not meet audit standards. Auditors expect specific actions tied to CPT-defined activities, written clearly enough to stand on their own:
- Concurrency conflicts across CCM, RPM, RTM, and TCM when time is not clearly separated
- Missing initiating visits within required timelines
- Signature and supervision gaps where the billing practitioner linkage is unclear

The Real Cost of Getting This Wrong
Adverse findings cascade fast.
- Revenue clawbacks that reach back months
- Compliance overload as teams reconstruct records under deadlines
- Staff fatigue and payer skepticism, which slow future reimbursement
CCM audit risk is structural, not situational. Treating it as a once-in-a-while event leaves revenue exposed.
II. Preventive Strategies (Audit Defense Before the Claim Is Filed)
The safest CCM claim is the one that cannot be submitted unless it is compliant. High-performing programs do not rely on post-denial cleanup. They build guardrails that stop risk at the source.
A. Pre-Claim Validation Rules (Your First Line of Defense)
Pre-claim validation shifts audit defense upstream, where it belongs.
- Time reconciliation before billing
Every CCM minute must align across EHR activity, call logs, and billing totals. Automated reconciliation flags gaps immediately, before they become audit findings. This directly addresses the most common CCM denial trigger. - Consent verification as a hard stop
Claims should not move forward unless patient consent is present, dated, and linked to the active care plan. If consent is missing, the system should fail the claim. No exceptions. - Care plan completion checks
An individualized, current care plan is non-negotiable. Validation rules should confirm that the plan exists, reflects the patient’s chronic conditions, and is tied to the billed period. This reinforces both compliance and quality of care.
High-performing programs extend pre-claim validation into rules-based enforcement, including eligibility checks, initiating visit confirmation, concurrency matrix validation, and strict time-code mapping to prevent double counting across CCM, RPM, and related programs.
Bottom line: if a claim clears pre-claim validation, it is already audit-defensible.
B. Building an Audit-Ready Packet by Default
Winning audits is less about arguing and more about how fast and cleanly proof can be produced.
Leading programs align their documentation structure with Medicare Administrative Contractor (MAC) review logic, organizing packets in the exact sequence auditors expect: eligibility, consent, care plan, time logs, interventions, and signatures.
- Centralized documentation repository
Consent forms, care plans, time logs, and intervention notes should live in one secure system, not across inboxes and spreadsheets. Role-based access supports HIPAA and SOC 2 while keeping audits efficient. - Structured intervention notes tied to CPT intent
Documentation must describe what was done and why it qualifies. “Reviewed antihypertensive adherence and updated reminder cadence” holds up. “Care coordination provided” does not. - Standardized reviewer-ready summaries
Auditors expect clarity. A consistent packet layout that highlights total time, qualifying activities, and linked documentation reduces back-and-forth and speeds resolution.
C. Roles, Drills, and Escalation Paths
Compliance breaks down when it is owned by one team. Strong programs make it operational.
- Alignment between compliance and coding
Coding teams should review CCM documentation weekly, not quarterly. Early feedback prevents patterns from forming. - Quarterly mock audits
Tabletop exercises simulate payer requests and force teams to assemble packets under time pressure. Regular drilling programs prevent the majority of avoidable findings. - Clear escalation for red flags
When documentation looks weak, escalation should be fast and cross-functional. Compliance, clinical leadership, and legal must share accountability.
Preventive strategies turn CCM from an audit risk into a controlled process. Claims that pass these gates are easier to defend, faster to resolve, and far less likely to be clawed back.
High-performing CCM programs operationalize compliance through cadence: monthly denial-prevention drills, quarterly mock audits, and weekly compliance-coding alignment reviews that catch documentation drift early.
Every pre-claim validation check and audit packet item on one printable page. Pin it next to your billing desk. Run it before every claim submission. Hand it to your team lead. Aligned to OIG 2026 enforcement focus areas. What’s on the checklist-
- Section A: Pre-claim validation – eligibility, consent, care plan, time documentation, APCM, concurrency, signatures
- Section B: Audit packet assembly – 11-item checklist to build the full documentation packet in under 30 minutes per chart
- Section C: OIG 2026 focus areas – the 2 items auditors are specifically targeting this enforcement cycle
Get The Printable CCM + APCM Checklist To Validate Eligibility, Consent, Time, Care Plans, And Audit Packet Items In One Place.
Work with Mindbowser to build a custom compliance plan that fits your team and workflows.
III. Recovery and Continuous Improvement (When Findings Happen and How They Stop Repeating)
Even strong CCM programs will face findings. What separates resilient organizations from repeat offenders is how fast they diagnose the issue and how deliberately they close the loop. Recovery is not about damage control. It is about preventing the same gap from reappearing next quarter.
A. Responding to Adverse Findings Without Bleeding Revenue
When an audit finding lands, speed and structure matter.
- Root-cause analysis, not surface fixes
The first question is not “how do we appeal,” but “why did this pass pre-bill review?” Time mismatch, missing consent, or vague notes each require different remediation. Findings should directly inform workflow or template changes, not one-off corrections. - Targeted remediation plans
If multiple claims fail for the same reason, remediation must be systemic. That may mean retraining staff on intervention language, tightening time-capture rules, or enforcing consent checks earlier in the workflow. - Appeals backed by clean packets
Appeals succeed when documentation is complete, consistent, and easy to review. Organizations with standardized audit packets can respond within days instead of weeks, protecting cash flow and credibility.
B. Embedding Compliance as an Operating Discipline
Recovery only creates value if it changes future behavior.
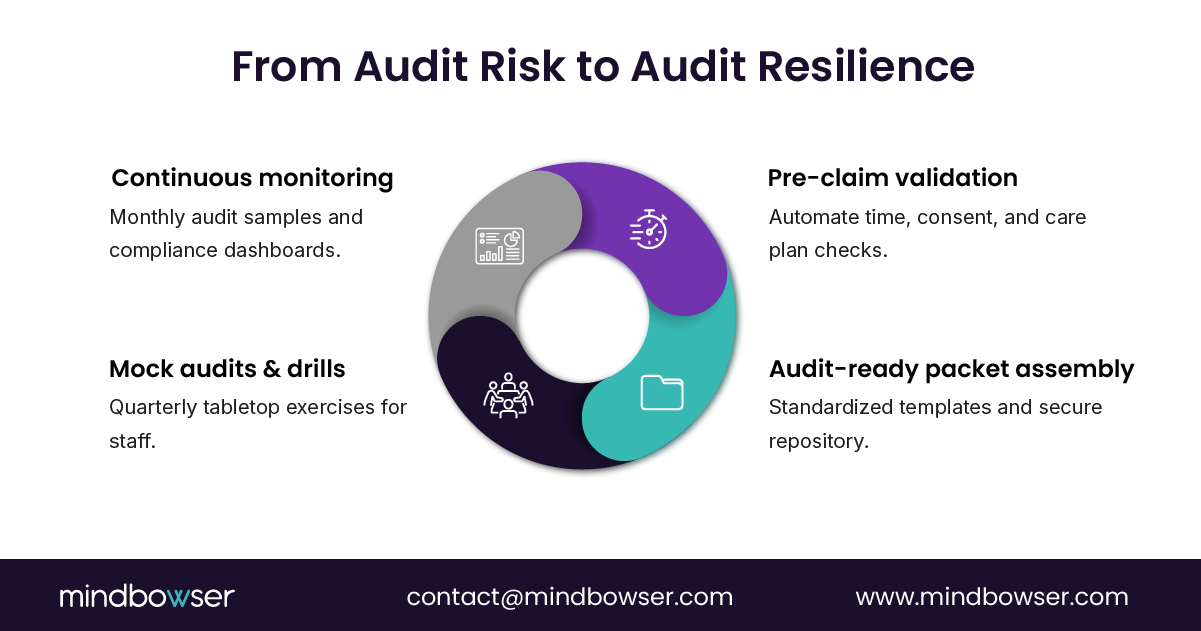
- Monthly internal audit sampling
Random claim sampling each month exposes gaps before payers do. Programs that audit themselves routinely catch issues while corrections are still cheap. - Technology-enabled monitoring
Compliance dashboards that track time thresholds, consent status, and care plan validity give leaders real-time visibility into risk. Alerts prevent small gaps from turning into systemic exposure. - KPIs that tie compliance to revenue integrity
Metrics like time-log accuracy and audit-ready packet completion should sit alongside AR days and denial rates. What gets measured gets protected.
Audits do not break CCM programs. Uncorrected patterns do. Continuous improvement turns each finding into a control point, reducing future exposure while stabilizing revenue.
Effective recovery frameworks also include formal overpayment protocols aligned with the CMS 60-day rule, ensuring identified overpayments are logged, reviewed, and returned within regulatory timelines.
IV. Why Manual CCM Compliance Breaks at Scale
Manual CCM compliance workflows fail for three structural reasons:
- Fragmented systems where time logs, consent, and care plans live separately
- Human dependency that introduces missed documentation and reconciliation errors
- Scaling limits where workflows break as patient volumes increase
Even strong clinical teams cannot maintain audit-ready documentation under manual workflows at scale. This is why denial rates increase as programs grow.
V. How Mindbowser Helps (Turning CCM Compliance Into a Revenue Control)
Most CCM audit failures are not caused by bad intent or poor care. They are caused by systems that allow non-compliant claims to slip through. Mindbowser’s approach flips that risk model by designing CCM platforms where audit defense is built into the workflow rather than layered on later.
A. Compliance-First, FHIR-Native CCM Platforms
Mindbowser builds custom chronic care management software where compliance gates sit upstream of billing, not downstream of denials.
- FHIR-native, API-first architecture
CCM workflows integrate directly with Epic, Cerner, athenahealth, and other major EHRs. Time, consent, care plans, and interventions are pulled from source systems and reconciled automatically, reducing manual errors that trigger audits. - Pre-claim validation baked into workflows
Claims cannot advance unless CPT time thresholds are met, consent is verified, and an active care plan is linked. This eliminates the most common audit triggers before revenue is ever posted. - One-click audit-ready packets
Consent, care plans, reconciled time logs, and structured intervention notes are assembled automatically into reviewer-ready packets. When auditors ask, teams respond with proof, not panic. - Security and regulatory alignment by design
Platforms are built to meet HIPAA, SOC 2, and 42 CFR Part 2 requirements, so scaling CCM volume does not increase compliance exposure.
B. Measurable Outcomes From Real Deployments
Compliance works best when it also reduces operational load.
- 50–60% reduction in documentation and review time
With Mindbowser’s AI Medical Summary, clinicians and reviewers cut documentation and review effort by up to 60%, reducing the risk of vague or incomplete intervention notes while freeing time for patient care. - Stronger outcomes with cleaner audit trails
In a CCM workflow automation engagement, a digital health client achieved a 60% reduction in post-visit follow-up time and 70% reduction in documentation time, with audit-ready records maintained across the full care cycle. - Faster audits, fewer findings
Teams using standardized packets and automated validation reduce back-and-forth during audits and prevent repeat findings through consistent proof quality.
In one CCM deployment, a healthcare organization reduced coding-related denials by 76% after implementing structured documentation, pre-claim validation, and audit-ready packet workflows.
C. Accelerators That Close the Biggest Compliance Gaps
Mindbowser’s accelerators target the exact failure points auditors test.
- AI Medical Summary
Converts complex histories and interactions into structured, CPT-aligned documentation, reducing ambiguity in intervention notes. - CarePlan AI
Captures patient goals and updates care plans in real time, ensuring plans remain current, individualized, and defensible. - HealthConnect CoPilot
Pulls structured data directly from EHRs into CCM workflows, strengthening the link between care delivery and billing proof while reducing manual entry errors.
Mindbowser does not just help teams pass audits. It reduces the likelihood of audit findings in the first place, lowers documentation burden, and protects CCM revenue at scale.
Beyond audit defense, compliance automation delivers measurable gains: up to 70% reduction in documentation time, improved patient engagement, and significantly lower denial rates by eliminating documentation gaps before submission.
VI. Compliance Automation as a Revenue Strategy
Compliance automation is no longer just defensive. It is a growth lever.
Hospitals that automate CCM compliance see:
- Lower denial rates and fewer clawbacks
- Higher staff efficiency and reduced burnout
- Faster audit response times
- Stronger payer relationships
Startups benefit through improved payer trust, scalable compliance, and stronger investor confidence.
VII. From Audit Risk to Revenue Control
CCM is no longer a low-risk add-on. It is a core revenue stream under active audit surveillance.
Time mismatches, missing consent, and vague documentation are not minor errors. They are predictable failure points that trigger denials, clawbacks, and repeat scrutiny.
The organizations that protect CCM revenue do one thing differently. They treat compliance as a front-line operating discipline, not a clean-up task after claims go out the door. Pre-claim validation, audit-ready packets built in real time, and routine drills change the math. Risk moves upstream. Revenue stabilizes.
Technology accelerates that shift. FHIR-native platforms with embedded validation and structured documentation reduce human error, lower staff burden, and make every claim defensible by default. Mindbowser’s work shows that when compliance is designed into workflows, CCM stops being an audit liability and becomes a controlled, scalable growth engine.
The most common triggers are time mismatches across systems, missing patient consent or care plans, and vague intervention notes. These issues account for the majority of CCM denials and clawbacks.
Prevention starts before billing. Pre-claim validation rules that enforce time reconciliation, consent verification, and care plan linkage stop non-compliant claims from being submitted in the first place.
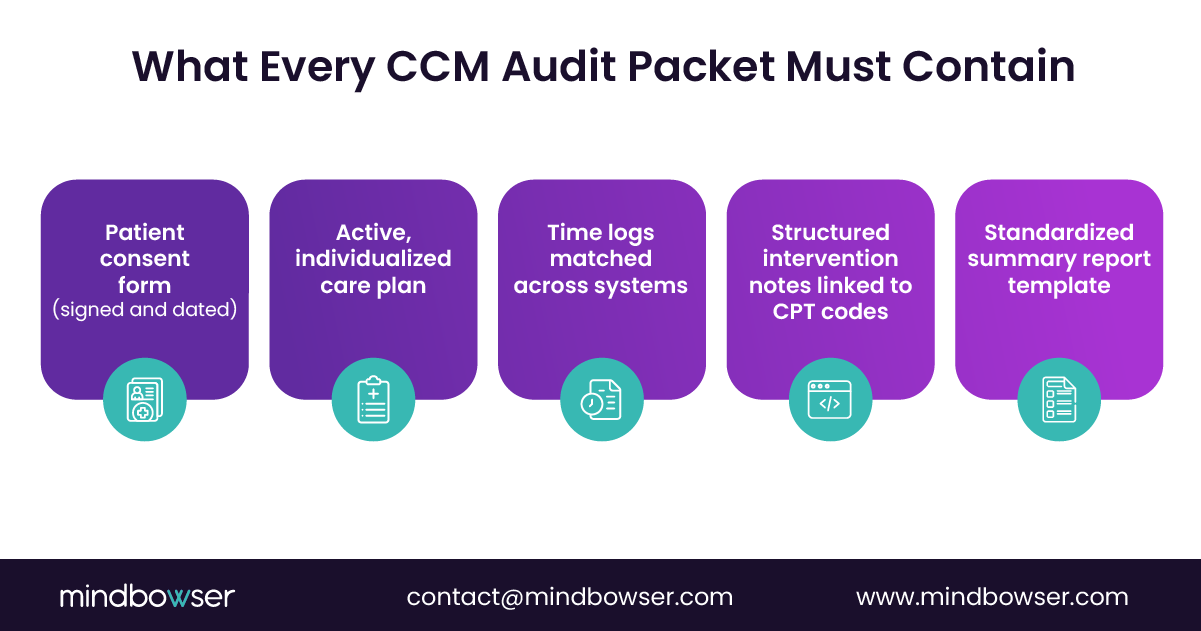
A defensible packet includes signed patient consent, an active individualized care plan, reconciled time logs, detailed CPT-aligned intervention notes, and a standardized summary report for reviewers.
At least quarterly. Mock audits expose weak points early and help teams respond quickly and consistently when real payer requests arrive.
Automation centralizes documentation, enforces compliance checks, and generates audit-ready packets on demand. AI-supported tools reduce documentation time while improving note quality, thereby lowering audit exposure.


