



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
- Most care coordination failures surface after go-live, not during planning, demos, or pilots.
- The root cause is rarely technology; it’s workflow misalignment, unclear ownership, and EHR handoffs that don’t reflect real clinical operations.
- Adoption drops when care teams are forced to work around tools rather than within existing care-delivery workflows.
- Fixing care coordination requires workflow-first redesign tied to roles, compliance, and operational accountability, not new features or another platform.
Why does care coordination seem stable during demos and pilots but start to unravel once it’s live inside real clinical operations?
For most mid-market health systems, care coordination doesn’t fail because the strategy was wrong or the technology was inadequate. On paper, the workflows are mapped. The roles are defined. The platform checks the right boxes. Leadership signs off, go-live happens, and early metrics look acceptable.
The breakdown starts later when real patients, real clinicians, and real operational constraints enter the system.
Care managers are forced to work outside the tool to complete their tasks. Ownership of handoffs becomes unclear across teams. EHR workflows don’t align with how care is delivered across settings. What looked like a clean process during implementation turns into fragmented workarounds that quietly erode adoption, data quality, and outcomes.
This is the hidden failure point in care coordination: the gap between designed workflows and lived clinical reality after implementation.
I. Why Care Coordination Breaks After Go-Live (Not During Planning)
Most care coordination initiatives don’t fail at the strategy stage. They fail after go-live, once workflows are exposed to real clinical volume, staffing variability, and EHR constraints.
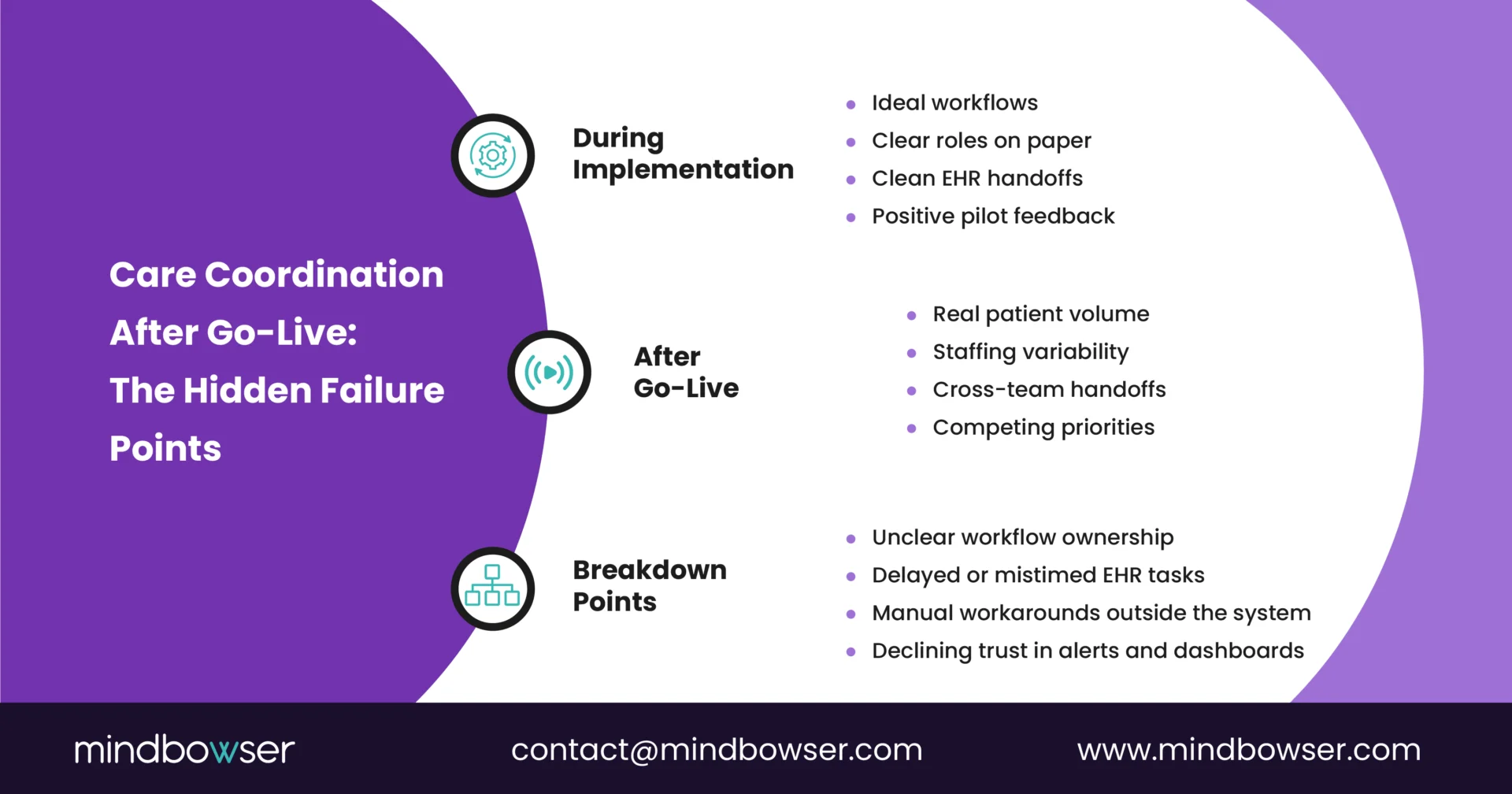
During planning and vendor selection, workflows are often designed in isolation:
- Ideal patient journeys
- Linear handoffs
- Clearly defined roles that assume consistent staffing and clean data
That version of care delivery rarely exists in production.
Once live, care teams coordinate across inpatient, outpatient, home health, and community settings, often within different EHR modules, task queues, and documentation standards.
Ownership of the next steps becomes ambiguous. Alerts and tasks pile up without clear accountability. Care managers adapt by building parallel processes outside the system just to keep patients moving.
The technology may be functioning as designed, but the workflow was designed for an operational model that doesn’t exist.
In practice, post-go-live breakdowns usually trace back to:
- Workflow ownership that was never operationalized beyond implementation
- EHR handoffs that don’t reflect real transitions of care
- Coordination tasks that add clicks without removing work elsewhere
Care coordination doesn’t collapse suddenly. It degrades quietly until adoption declines and leadership begins to question outcomes.
II. Where Workflow Ownership and Accountability Break Down
After go-live, care coordination workflows often exist, but no one truly owns them.
During implementation, responsibility is typically shared across IT, clinical leadership, population health, and vendors. Once the system is live, that shared ownership becomes ambiguous. When handoffs fail or tasks stall, it’s unclear who is accountable for fixing the workflow versus working around it.
This shows up quickly in day-to-day operations:
- Care managers receive tasks without clarity on clinical priority or escalation paths
- Multiple teams touch the same patient without a single source of truth for next actions.
- Exceptions (missed follow-ups, incomplete outreach, delayed transitions) have no defined owner
Without operational accountability, care teams default to informal coordination emails, spreadsheets, side conversations, and EHR notes that never feed back into the system.
From a leadership perspective, this creates a false signal. Dashboards may show activity, but they don’t reveal:
- Which handoffs are breaking
- Where delays are occurring
- Who is responsible when care plans stall
Care coordination workflows require explicit post-go-live ownership, not just during implementation but as part of ongoing clinical operations. Without that, even well-designed processes slowly fragment under real-world pressure.
Find Hidden Gaps and Improve Coordination Without Changing Your Systems
III. How EHR Handoffs and Integration Gaps Accelerate Breakdown
Care coordination workflows rarely fail in isolation. They fail at handoff points within the EHR where responsibility shifts, data flows, and timing are critical.
On paper, integrations look complete. Tasks are created. Notes syncalerts fire. But after go-live, teams discover that these handoffs don’t align with how care actually transitions across settings.
Common post-implementation issues include:
- Discharge events triggering tasks too late for timely outreach
- Care plans live in one module while daily work happens in another
- Referral or SDOH workflows that require duplicate documentation
- Alerts are firing without context, forcing care managers to hunt for information
These gaps push care teams into workaround behavior. Instead of trusting the system, they rely on memory, manual tracking, or parallel tools to ensure patients don’t fall through the cracks.
From an operational standpoint, the problem isn’t missing integrations; it’s misaligned ones. The EHR may technically support the workflow, but not in a way that matches real clinical timing, decision-making, or accountability.
Over time, this erodes confidence:
- Care managers stop engaging with assigned tasks
- Supervisors lose visibility into true workflow performance
- Leadership sees utilization, but not coordination effectiveness
When EHR handoffs aren’t designed around real transitions of care, care coordination becomes a documentation exercise rather than an operational process.
IV. The Silent Adoption Problem No One Sees in Dashboards
By the time leaders notice adoption issues in care coordination, the damage is already done.
After go-live, most teams don’t openly reject new workflows. They adapt quietly. Care managers still “use” the system, tasks still close, and reports still populate. On the surface, adoption looks stable.
In reality, the work has moved elsewhere.
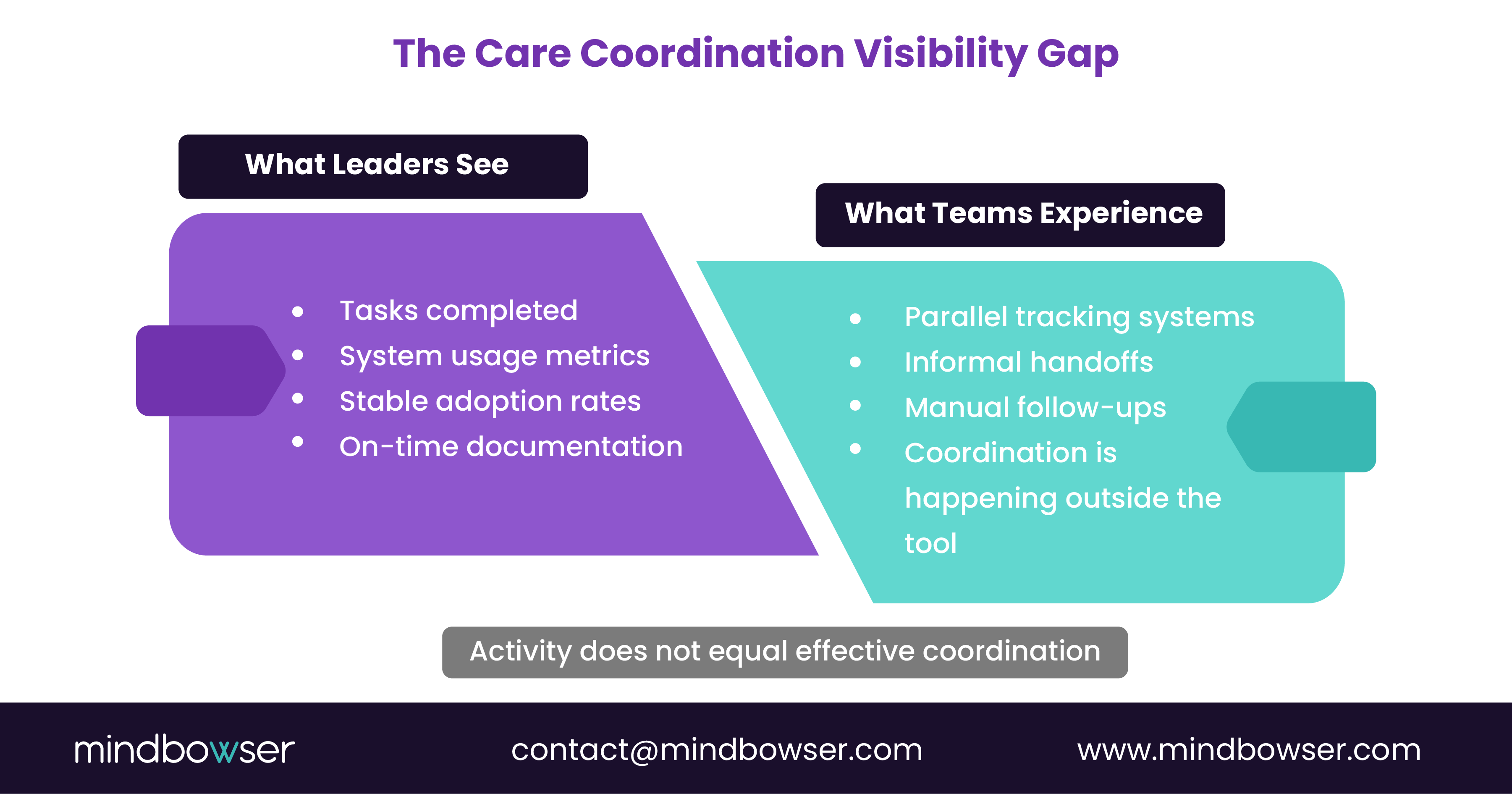
Care teams begin relying on:
- Personal tracking systems to manage follow-ups
- Informal communication to resolve handoffs
- Manual checks to compensate for unreliable alerts
The system becomes a place to document work after it’s completed, not where coordination actually happens.
This creates a dangerous blind spot for leadership. Standard dashboards rarely show:
- How often are workflows bypassed
- Where teams are duplicating effort
- Which steps are consistently ignored or delayed
Without visibility into these workarounds, organizations often respond by adding training or more features, neither of which addresses the root issue.
Adoption erodes not because teams resist change, but because the workflow increases cognitive and operational load instead of reducing it. When tools don’t fit into the flow of clinical work, care teams optimize for patient needs first and systems second.
V. What a Workflow-First Redesign Looks Like After Implementation
Fixing care coordination after go-live does not start with new features or platform changes. It starts with a clear look at how work is actually getting done today.
A workflow-first redesign focuses on aligning coordination tasks with real clinical roles, timing, and accountability rather than idealized process maps created during implementation.
In practice, this means:
- Redefining ownership for each coordination step, including exceptions and escalations
- Mapping workflows based on actual transitions of care, not system events alone
- Reducing cognitive load by removing steps that do not directly support patient movement or decision-making
- Embedding coordination tasks into the tools and screens that care teams already use daily
This approach often reveals that only a small set of workflow changes is needed to stabilize adoption. The impact comes from precision, not scale.
Successful post-implementation redesigns also treat care coordination as an operational process, not a configuration exercise. Workflows are reviewed, adjusted, and governed just like clinical protocols.
When coordination is designed around real-world execution, teams stop working around the system and start relying on it.
VI. What Healthcare Leaders Can Do to Prevent Repeat Breakdowns
Once care coordination workflows begin to erode, the instinct is often to stabilize the tool. The more effective move is to stabilize ownership, execution, and governance.
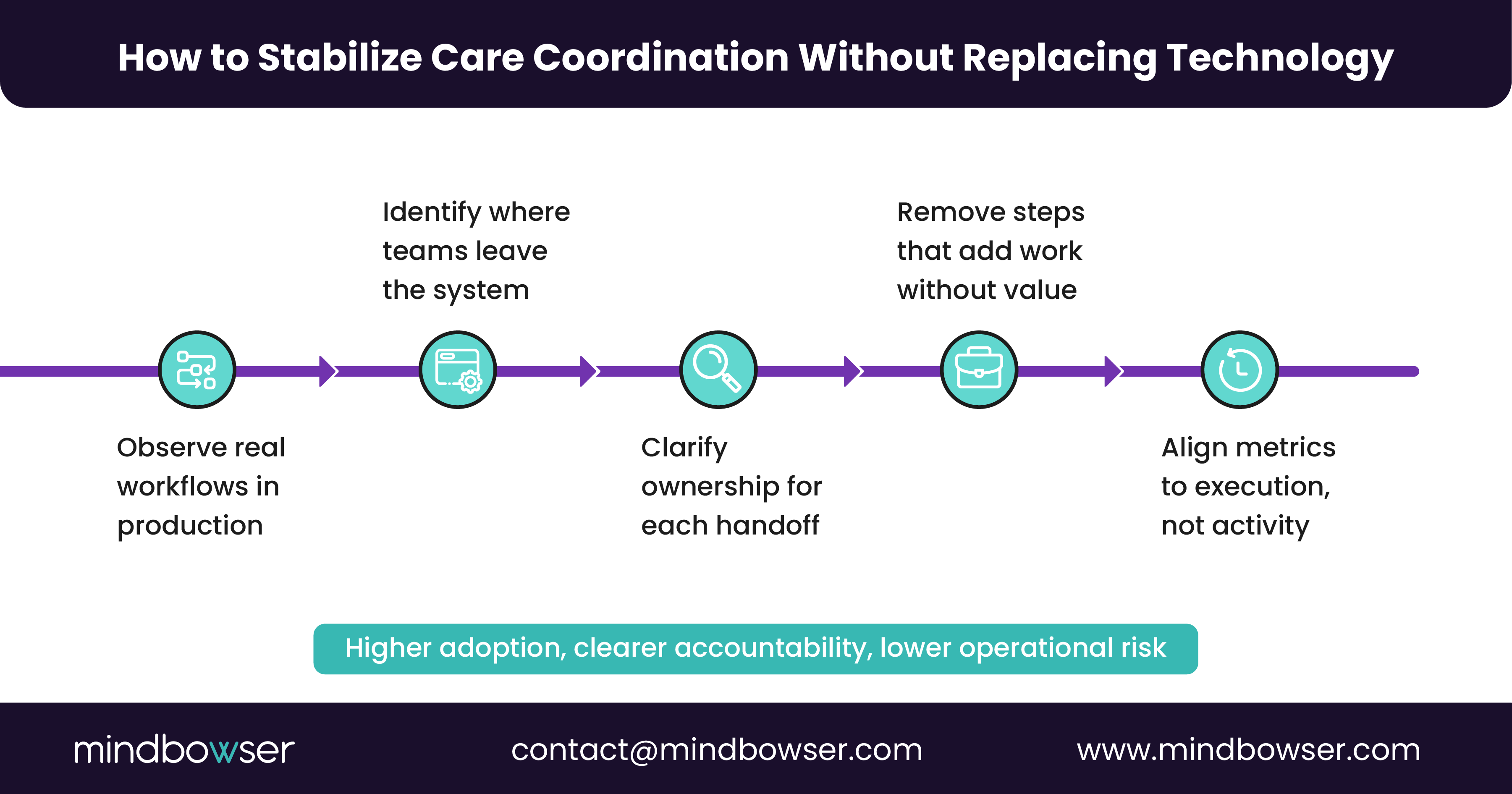
Healthcare leaders who prevent repeat breakdowns focus on a small set of operational actions.
First, they assign clear post-go-live ownership. This is not an implementation role. It is an ongoing operational responsibility tied to outcomes, not configuration. Someone must be accountable for how coordination actually functions across teams, settings, and handoffs.
Second, they review workflows in production, not in workshops. This involves observing how care managers, nurses, and coordinators utilize the system in actual patient care settings. The goal is to identify where steps are skipped, delayed, or bypassed, and the reasons why.
Third, they align metrics to execution, not activity. Task completion alone is not a proxy for effective coordination. Leaders track delays, exception rates, and handoff failures to identify where workflows break under real-world conditions.
Finally, they treat care coordination as a living operating model. As staffing, patient mix, and care delivery models change, workflows must be revisited. Governance ensures those changes occur deliberately rather than through silent workarounds.
Care coordination does not fail because teams stop caring. It fails when workflows stop matching reality, and no one owns the gap.
If you want to assess where your care coordination workflows are breaking after go-live and what to fix first, a workflow-first operational review can quickly surface the issues without disruption.
VII. How to Identify Care Coordination Breakdowns Before They Become Visible Failures
Most organizations only act once care coordination problems show up in outcomes or executive reports. By then, teams have already adapted in ways that are hard to unwind.
The goal is to surface breakdowns early, while they are still operational issues and not performance failures.
A. Signals to look for at the workflow level
These rarely appear in standard dashboards, but they show up quickly in day-to-day execution:
- Care managers maintain parallel tracking systems
- Frequent verbal or message-based follow-ups for “closed” tasks
- Inconsistent timing of outreach after key transitions
- Repeated clarification questions around who owns the next step
Each of these points refers to a workflow that no longer aligns with real-world operations.
B. Questions leaders should ask their teams
Instead of asking whether workflows are being followed, ask:
- Where do you have to leave the system to get your work done
- Which handoffs are hardest to trust
- What steps feel redundant or slow you down
- Where do patients most often get stuck
The answers usually highlight a small number of friction points with outsized impact.
C. What to fix first
Resist the urge to redesign everything. Focus on:
- High-volume transitions of care
- Steps with unclear ownership or escalation paths
- Tasks that require duplicate documentation
- Alerts that fire without actionable context
Targeted fixes in these areas often restore adoption faster than broad system changes.
Care coordination workflows do not break all at once. They fracture gradually under real-world pressure. Leaders who look beyond surface-level adoption metrics can intervene early and prevent small gaps from becoming systemic failures.
VIII. Compliance and Risk Considerations Leaders Often Overlook
When care coordination workflows break down after implementation, the impact is not limited to efficiency or adoption. It also introduces compliance and operational risks that are easy to miss until an audit or an adverse event surfaces them.
Fragmented workflows increase the likelihood of:
- Incomplete or inconsistent documentation across teams
- Care actions occurring outside auditable systems
- Gaps in follow-up that are difficult to trace back to ownership
- Inaccurate reporting driven by manual workarounds
From a compliance perspective, the issue is not whether a system is certified or HIPAA compliant. The risk arises from how coordination occurs when teams bypass workflows to get work done.
When care managers rely on external notes, spreadsheets, or informal communication, organizations lose:
- Clear audit trails for care activities
- Confidence in reported quality and performance metrics
- Visibility into access control and role-based responsibility
Over time, this creates exposure during audits, quality reviews, and payer evaluations, especially for programs tied to value-based care or population health outcomes.
A workflow-first approach reduces this risk by keeping coordination inside governed systems, with clear ownership and traceable actions. When workflows reflect real execution, compliance follows naturally rather than being enforced after the fact.
IX. The Real Failure Point in Care Coordination After Implementation
Care coordination rarely fails because teams choose the wrong platform. It fails when workflows designed during implementation are never recalibrated for real clinical operations after go-live.
For healthcare leaders, the signal to act is not declining adoption or missed metrics. It is the growing gap between how coordination is supposed to work and how work actually gets done day-to-day.
A focused, workflow-first assessment can help organizations:
- Identify where coordination breaks down after implementation
- Clarify ownership across teams and transitions of care
- Reduce reliance on manual workarounds that increase risk
- Restore adoption by aligning tools with real clinical execution
This does not require replacing systems or launching large transformation efforts. In most cases, small, targeted workflow changes deliver the fastest operational and compliance impact.
If your care coordination program is live but not delivering the outcomes leadership expected, the next step is not another feature rollout. It is a structured review of how coordination truly functions in production and what needs to change to support teams at scale.
In most organizations, early signs typically appear within 60 to 90 days after go-live. This is when initial training effects wear off, patient volume increases, and care teams begin operating under real staffing and time constraints. By the time issues appear in leadership reports, workflow workarounds are often already in place.
Yes. Most post-implementation breakdowns are workflow and ownership issues rather than platform limitations. In many cases, targeted redesign of handoffs, task timing, and accountability within the existing system delivers faster impact than switching vendors or adding new tools.
Dashboards typically track task completion and system usage, not whether coordination happened at the right time or by the right role. When teams complete documentation after the fact or outside the system, activity metrics remain high while real coordination quality declines.
Post-implementation workflow gaps often lead to missed follow-ups, delayed interventions, and inconsistent documentation. Over time, this undermines the quality of reporting, care gap closure, and performance under value-based contracts, even when patient volume and engagement appear stable.
Ownership should shift from implementation teams to an operational leader accountable for day-to-day execution and outcomes. This role sits at the intersection of clinical operations, population health, and IT, and is responsible for reviewing production workflows and addressing breakdowns as care delivery evolves.


