



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























III. Where the Data Lands: Flowsheets & EHR Targets
Integration is only successful if clinicians see the right data in the right place. In anesthesia monitoring, that place is the perioperative flowsheet. These are the rows that anesthesiologists trust to guide patient management, and they are the rows that auditors check when reviewing compliance.
A. Flowsheet Row Agreements
Every hospital has its own unique flow sheet configuration. Even within the same EHR vendor, two hospitals may label or arrange rows differently. That means the integration team must sit down with clinical leaders and agree on target rows before a single line of code is written.
- Epic example: The TOF ratio might be mapped to a row called “NMT TOF Ratio” in one site and “Train-of-Four %” in another.
- Cerner example: PTC could land in “Post Tetanic Count” or a site-customized “Residual Blockade.”
The safest approach is to maintain a single global code set for each metric and adjust the flowsheet row mapping only by site. This ensures that if you roll out integration across multiple hospitals, the source system and transformation logic remain stable while only the row IDs change.
B. Delivery Paths for Integration
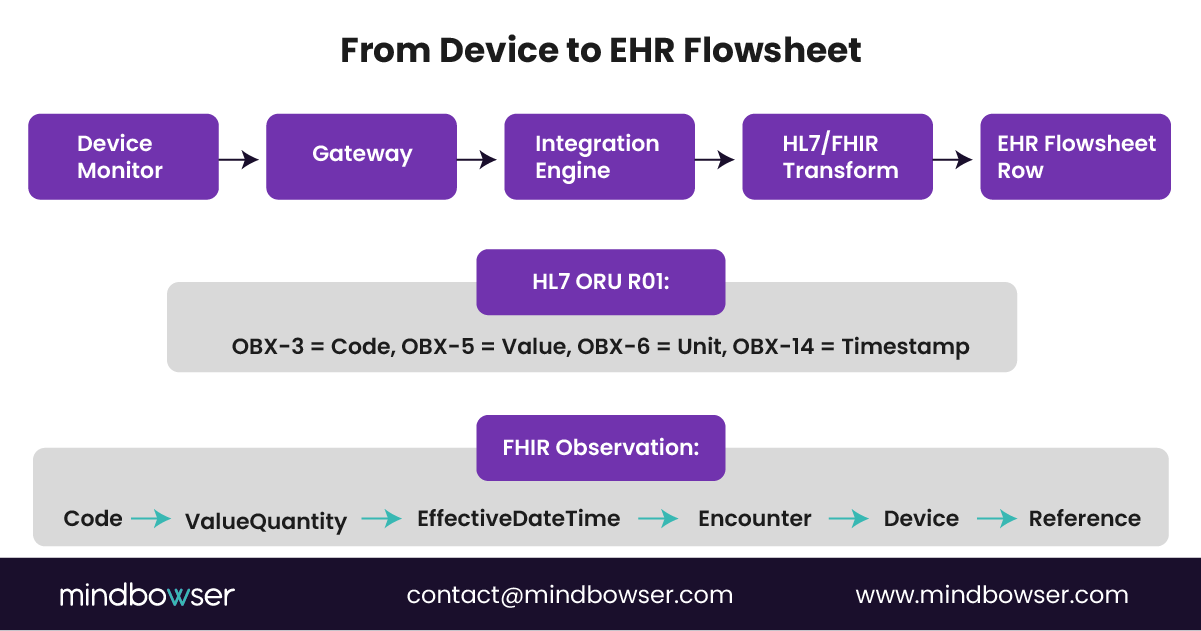
Hospitals typically choose between HL7 ORU messages and FHIR Observations to transport anesthesia data into the EHR. Both work if implemented correctly.
- HL7 ORU R01
- Each metric is sent as one OBX segment.
- OBX-3 carries the identifier (LOINC or IEEE code).
- OBX-5 holds the actual value.
- OBX-6 specifies the UCUM unit.
- OBX-14 timestamps the reading.
- This method has been adopted for decades and is well-supported by Epic and Cerner device gateways.
- FHIR Observation
- Each metric is coded using Observation.code.
- The value is stored in valueQuantity.
- effectiveDateTime ties it to the procedure timeline.
- subject and encounter ensure the observation belongs to the right patient and case.
- A device reference can be added for traceability.
- FHIR is increasingly preferred for forward-looking interoperability, especially as USCDI expands.
C. One Mapping Sheet, Two Outputs
The most efficient strategy is to maintain a single mapping workbook and use it to generate both HL7 and FHIR transforms. This avoids discrepancies between interfaces and gives the hospital flexibility if it transitions from HL7 to FHIR in the future.
IV. Identity, Encounter, and Workflow Integrity
Capturing anesthesia data is not just about sending values into the EHR. It is about ensuring that every value belongs to the correct patient, under the correct encounter, and at the appropriate point in the care journey. If identity and encounter alignment are off, the integration loses trust immediately.
A. Patient and Encounter Matching
The EHR must always know which patient and which encounter a monitoring value belongs to. That requires:
- Patient Identifier: Use the MRN or enterprise ID that is consistent across the hospital. Avoid relying on temporary IDs from device consoles unless they are reconciled at the gateway.
- Encounter Identifier: Tie each value to the active surgical encounter. If this linkage breaks, data may be misdirected to the wrong visit or fail to appear at all.
- Surgical Context: Ensure the integration respects start and stop times for anesthesia. This prevents values from bleeding into unrelated encounters or overlapping cases.
B. Device to Patient Association
At the gateway level, devices must be linked to the correct patient before data flows. This is often where errors occur, especially in busy ORs where multiple cases are turning over quickly. A strong integration design includes:
- Rules that bind the device session to a patient encounter when anesthesia begins.
- Alerts or warnings if a device is not assigned or if a mismatch occurs.
- Clear workflows for clinicians to correct an assignment without interrupting monitoring.
C. Transitions of Care
Anesthesia does not end when the patient leaves the OR. Recovery areas, such as PACU, must also display accurate monitoring values. Integrations need to handle these transitions seamlessly.
- Handoff Integrity: Ensure that values captured during anesthesia are accurately transferred into the PACU record without duplication or loss.
- Continuity Across Units: If a patient moves from the OR to the ICU, the encounter linkage must remain intact.
- Audit Trails: Each transition should leave a record showing how values were passed along and confirmed.
D. Why This Integrity Matters
If identity or encounter mapping fails, the hospital faces more than annoyance. Misfiled data can lead to gaps in regulatory reporting, disputes during audits, and even clinical errors if anesthesia values are missing when they are most critical. For CTOs and CMIOs, ensuring identity and workflow integrity is not optional. It is the foundation on which all other integration benefits rest.
Bottom line: accurate identity, correct encounter linkage, and clean handoffs are what make anesthesia monitoring data usable. Without these controls, even perfectly captured signals will fail to serve clinicians, compliance officers, or financial teams.
Map It Once. Deploy Across Every Site
V. Validation With Clinicians
Technology alone does not guarantee a successful anesthesia integration. Clinicians must see the data land where they expect it, in the right format, and with the right level of reliability. Without their validation, even the most technically correct integration will not be adopted.
A. The Golden Dataset Approach
The most effective way to validate anesthesia monitoring integration is to build a golden dataset. This is a carefully selected set of records that represent the most common and the most challenging cases.
- Sample Size: Typically, ten to twenty records are sufficient to capture the range of values clinicians want to verify.
- Content: Each record should include TOF ratios, TOF counts, PTC values, and single twitch responses at different stages of anesthesia.
- Expected Outputs: Alongside the device values, the golden dataset must include screenshots of the EHR flowsheet showing exactly where each metric should appear.
This dataset serves as the baseline against which integration outputs are evaluated. Every transformation, whether HL7 or FHIR, is measured against this set.
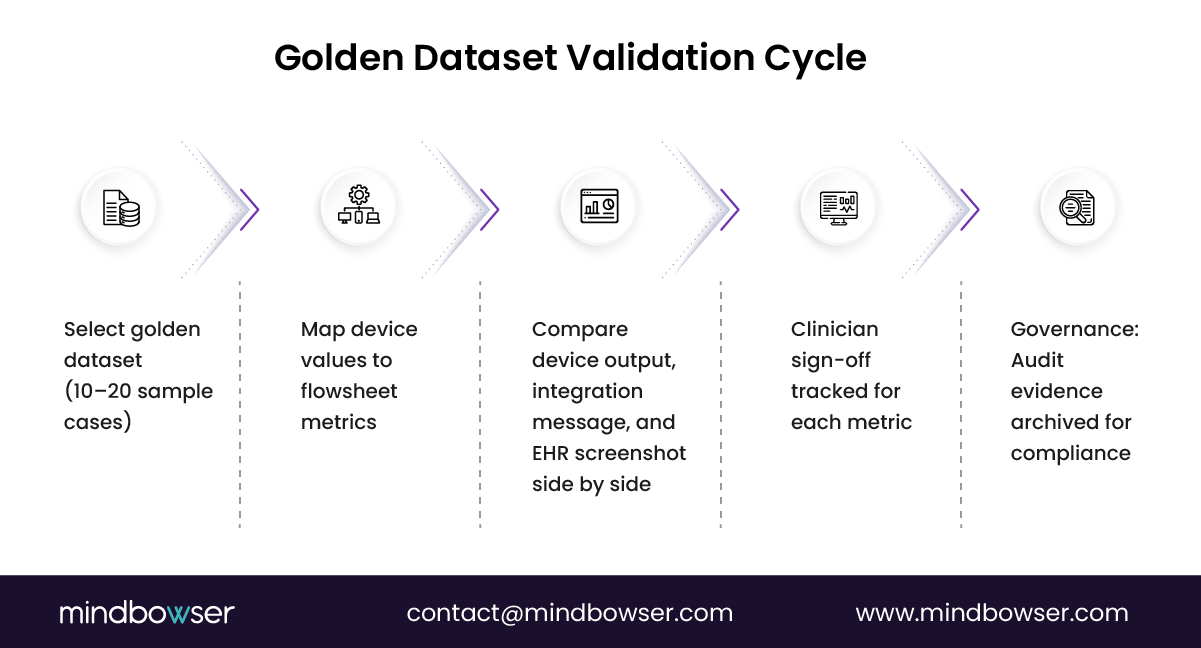
B. Side-by-Side Review
Once the integration is running, the golden dataset is used for side-by-side comparison. For each metric:
- Confirm that the captured value matches the device output.
- Verify the timestamp aligns with the clinical event.
- Verify the flow sheet row placement and labeling.
- Review unit consistency and rounding behavior.
The clinician review team should be able to flip between the mapping workbook, the sample message, and the EHR screenshot. This allows them to validate not only accuracy but also usability.
C. Sign-Off Tracker
Validation is incomplete without accountability. A sign-off tracker should record:
- Which clinician reviewed each metric?
- The date of review.
- The approval decision or requested correction.
This creates a governance trail that satisfies both clinical leadership and compliance auditors.
D. Governance and Auditability
Hospitals should keep the golden dataset, validation reports, and sign-off tracker under version control. This ensures that if a regulator or internal auditor questions data integrity, the hospital can produce evidence that the integration was validated and approved by frontline clinicians.
E. Why Validation Matters
A project may check every technical box, but without clinician validation, trust will not exist. Anesthesiologists rely on these values during surgery and during handoffs to PACU or ICU teams. Their approval is what turns integration from a theoretical capability into a daily clinical tool.
VI. Pitfalls to Avoid
Even well-planned anesthesia monitoring integrations can stumble if the common pitfalls are not addressed early. These mistakes often surface during go-live when clinicians are under pressure and their tolerance for technical errors is low.
A. Units Drift
One of the fastest ways to lose a clinician’s trust is to be inconsistent. For example, a TOF ratio may appear as a raw ratio on one line and as a percentage on another. If UCUM standards are not enforced, values drift and comparisons become unreliable. The fix is strict unit mapping and rejection of non-standard units at the interface level.
B. Timestamp Mismatch
Device clocks rarely match the EHR clock exactly. Without synchronization, values can appear minutes off, creating confusion about when events occurred. In anesthesia, where induction and emergence timing matter, this discrepancy can become a safety issue. Integrations must normalize timestamps to the hospital time source before sending them into the EHR.
C. Duplicate Writes
Retries are common in interface engines, but without idempotency rules, the same value may be written twice. Clinicians then see duplicate TOF readings, which makes the flowsheet look messy and can affect decision-making. The solution is to include unique identifiers for each observation, allowing the EHR to recognize and reject duplicates.
D. Over-Sampling
Some device vendors default to pushing values every few seconds. While this looks thorough, it overflows the flowsheets with noise and makes review more difficult. Clinicians do not want 200 entries of a stable TOF ratio; they want representative, clinically relevant values. The capture cadence should be agreed upon with anesthesia leadership, typically every one to five minutes, depending on context.
E. Artifact Handling
Muscle relaxant monitors are not perfect. Poor electrode contact, patient movement, or interference can produce faulty values. If integrations blindly capture every number, the EHR will be filled with misleading data. A better approach is to flag questionable readings and prevent them from cluttering the chart. This builds clinician confidence that what they see in the EHR reflects real signals.
F. Site-Specific Customization Traps
Hospitals often customize flowsheet rows and labels. If integration logic is not designed to handle site variation, scaling to new sites becomes painful. Maintaining a single global code set with site-specific row mapping is the best way to avoid rework.
G. Lack of Validation Loops
Skipping the golden dataset review or ignoring clinician feedback is another pitfall. When this happens, integration may technically function, but it may never achieve widespread adoption. Continuous validation and periodic audits must be baked into the workflow.
Why Avoiding Pitfalls Matters
Every one of these pitfalls has real consequences. Units drift creates confusion. Timestamp mismatches threaten patient safety. Duplicate values and clutter erode trust. Artifact noise reduces chart clarity. Customization traps slow down rollouts. For leadership, the question is not whether pitfalls exist, but how quickly they are prevented.
VII. ROI and Strategic Benefits
Anesthesia monitoring EHR integration is not just a clinical quality initiative; it is also a key component of patient safety. It is a business decision with measurable returns. Hospitals that invest in this capability see benefits across efficiency, compliance, and financial performance.
A. Efficiency Gains
Manual transcription consumes time in the OR and again later when clinicians re-enter values into the EHR. Even a few minutes per case scales into hundreds of wasted hours across a perioperative program. By capturing values directly into flowsheets:
- Clinicians save time during critical phases of surgery.
- Chart completion occurs more quickly, resulting in reduced after-shift overtime.
- Nursing staff in PACU and ICU receive more precise handoff data, reducing clarification calls and delays.
In practice, some hospitals have reported a 20- to 30-percent reduction in anesthesia documentation time once automated capture is live. That directly translates into increased clinical capacity without the need for additional staff.
B. Compliance and Risk Reduction
The compliance stakes are high. CMS Conditions of Participation explicitly require anesthesia records to be complete and contemporaneous. Manual entry invites transcription errors and missing values, which can trigger deficiencies during surveys. Integration supports:
- Automated documentation that satisfies CMS and ASA requirements.
- Readiness for MIPS quality measures, such as perioperative temperature management.
- Seamless reporting to registries like NACOR, especially as Epic’s new Anesthesia Community Registry rolls out nationally.
Compliance is not just about avoiding penalties. It also reduces the legal and reputational risks associated with incomplete anesthesia records.
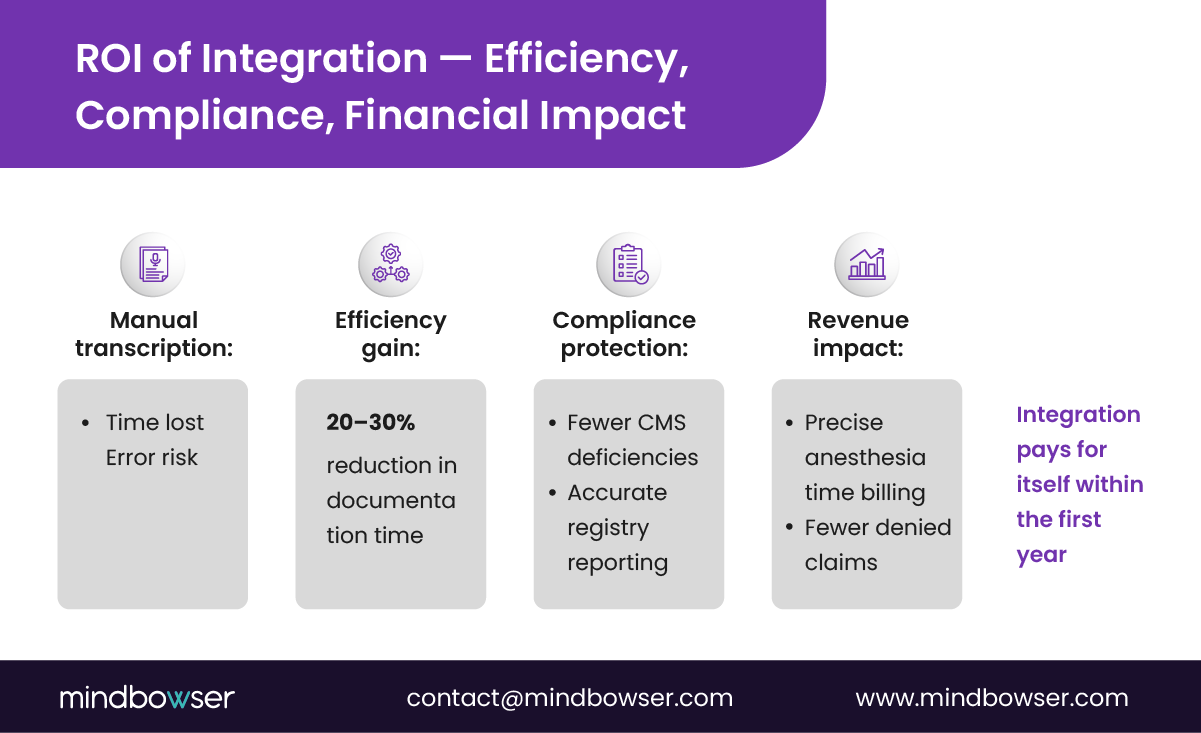
C. Financial Impact
Every minute of anesthesia is a billing opportunity, and every missing value is a potential denial. Integration improves revenue capture by:
- Accurately recording anesthesia start and stop times, eliminating disputes with payers.
- Supporting precise anesthesia time unit billing, which drives case revenue.
- Providing defensible audit trails that reduce write-offs in contested claims.
Hospitals that have implemented direct anesthesia monitoring integration report improved charge reconciliation and fewer compliance-related billing holds. For a mid-market health system, even a small reduction in denials translates into millions of dollars retained annually.
D. Strategic Positioning
Beyond operational gains, integration positions the hospital for future initiatives. As USCDI expands and FHIR adoption accelerates, perioperative data will increasingly feed into population health analytics, readmission risk scoring, and AI-driven safety monitoring. By building this foundation now, hospitals prepare themselves for regulatory shifts and technology partnerships that will demand structured anesthesia data.
Why ROI Matters
Executives often see integration projects as cost centers. The reality is different here. Anesthesia monitoring integration improves efficiency, strengthens compliance, and protects revenue. The result is not just safer care but also stronger financial performance.
VIII. How Mindbowser Can Help
Hospitals do not need another generic integration vendor. They need a partner who has walked into the OR, sat with anesthesiologists, and mapped out every flowsheet row before a single line of code was written. At Mindbowser, that is how we approach anesthesia monitoring EHR integration.
A. Proven Integration Playbooks
We have delivered integrations across Epic EHR, Cerner EHR, Meditech EHR, and Altera environments. The lesson is always the same: success comes from discipline in mapping and validation. Our playbooks include:
- Reusable HL7 and FHIR connectors that already understand how to structure anesthesia monitoring data.
- Mapping templates for TOF ratio, PTC, twitch amplitude, and other key metrics.
- Unit normalization libraries that enforce UCUM standards and reject non-standard inputs before they reach the EHR.
These playbooks shorten timelines while protecting against the pitfalls that derail projects during go-live.
B. Case Study Lens
When we partnered with a perioperative technology vendor to integrate device data into an Altera EHR environment, the biggest win was compliance. By embedding golden dataset validation into the workflow, the hospital reduced transcription error rates to near zero. In another engagement, we collaborated with a healthcare system that required reconciling anesthesia times with Epic. By aligning flowsheet mapping across multiple campuses, they improved billing accuracy and accelerated revenue cycle reconciliation.
These are not theoretical wins. They are practical outcomes that align with CFO and CMIO priorities: faster charts, fewer compliance findings, and stronger revenue integrity.
C. Accelerators That Deliver Speed
Mindbowser’s accelerators compress delivery timelines without sacrificing quality:
- HealthConnect CoPilot: A reusable integration framework that speeds up device-to-EHR connectivity.
- AI Medical Summary: Provides perioperative teams with summarized anesthesia data in a format that supports handoffs and audits.
- AI Readmission Risk: Extends perioperative monitoring into predictive analytics, helping identify patients at risk of complications after surgery.
These accelerators ensure integrations launch faster, reduce testing cycles, and scale across hospitals without rework.
D. Compliance by Design
Every Mindbowser engagement is built around HIPAA and SOC 2 standards. We maintain a strict validation framework, including version-controlled mapping workbooks, audit logs, and sign-off trackers. That gives CIOs and compliance officers the assurance that integrations are not only functional but also defensible during CMS surveys or payer audits.
Why Mindbowser
Hospitals that invest in anesthesia monitoring integration need more than code. They need a partner that understands the clinical workflow, the regulatory environment, and the financial implications. Mindbowser brings all three together with proven playbooks, accelerators, and a compliance-first design.
Conclusion
Anesthesia monitoring EHR integration is no longer optional. Manual transcription slows clinicians, creates errors, and exposes hospitals to compliance risk. Automated capture of TOF ratios, PTC values, and twitch responses directly into flowsheet rows transforms how perioperative teams work. It enhances safety during surgery, strengthens compliance with CMS and ASA standards, and ensures revenue integrity through accurate capture of anesthesia time.
Hospitals that delay integration will face growing challenges as registries, payers, and regulators demand structured perioperative data. Those who act now gain immediate efficiency, reduced risk, and stronger financial performance.
For CTOs, CMIOs, and CFOs, the decision is straightforward. Investing in anesthesia monitoring EHR integration is not a cost center. It is a measurable ROI engine that protects both patients and the organization’s bottom line.
Choose the delivery method your hospital’s EHR supports most reliably. HL7 ORU R01 is a mature and widely adopted standard. FHIR Observations are future-facing and align with expanding USCDI requirements. Keep your mapping workbook portable so you can support both.
Use IEEE 11073 or a local code in the interim, and track it in your mapping workbook. When a standard code becomes available, the transition is straightforward.
Implement UCUM standards at the integration layer. Reject or flag non-standard units before they are entered into the EHR. This prevents unit drift and protects clinical trust.
Yes. Keep them in separate rows. Make the derivation explicit in the workbook so clinicians and auditors understand the relationship.
Use the golden dataset approach. Provide side-by-side comparisons of device output, integration messages, and flowsheet screenshots. Maintain sign-off logs from clinical reviewers. This creates an audit-ready evidence trail.

