



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
AI Clinical Decision Support Tools are shifting care delivery from reactive alerts to real-time, context-aware decision-making. Traditional CDS tools helped standardize care, but today they struggle with alert fatigue, fragmented data, and workflow friction. AI-driven systems solve this by enabling risk prediction, personalized recommendations, and proactive intervention. The result: better clinical outcomes, improved value-based care performance, and stronger clinician trust when implemented with the right workflow, data, and governance strategy.
More alerts + more data ≠ better decisions, so what actually improves clinical outcomes?
Traditional CDS tools were built to guide care, but today they often create noise instead of clarity.
AI Clinical Decision Support Tools shift the model from reactive alerts to real-time, context-driven decisions, helping health systems improve outcomes, reduce cost, and restore clinician trust.
The difference is not more intelligence, it’s better-timed, better-informed decisions at the point of care.
I. Why traditional CDS tools are no longer enough
A. The promise of CDS tools and where they fall short
Clinical decision support tools were built with a clear goal: help clinicians make safer, evidence-based decisions at the point of care. And for a time, they delivered.
Early CDS tools introduced types of clinical decision support systems like rules-based alerts for drug interactions, preventive care reminders, and guideline adherence. They reduced variability. They improved compliance.
But here’s the problem.
What happens when the system treats every patient the same?
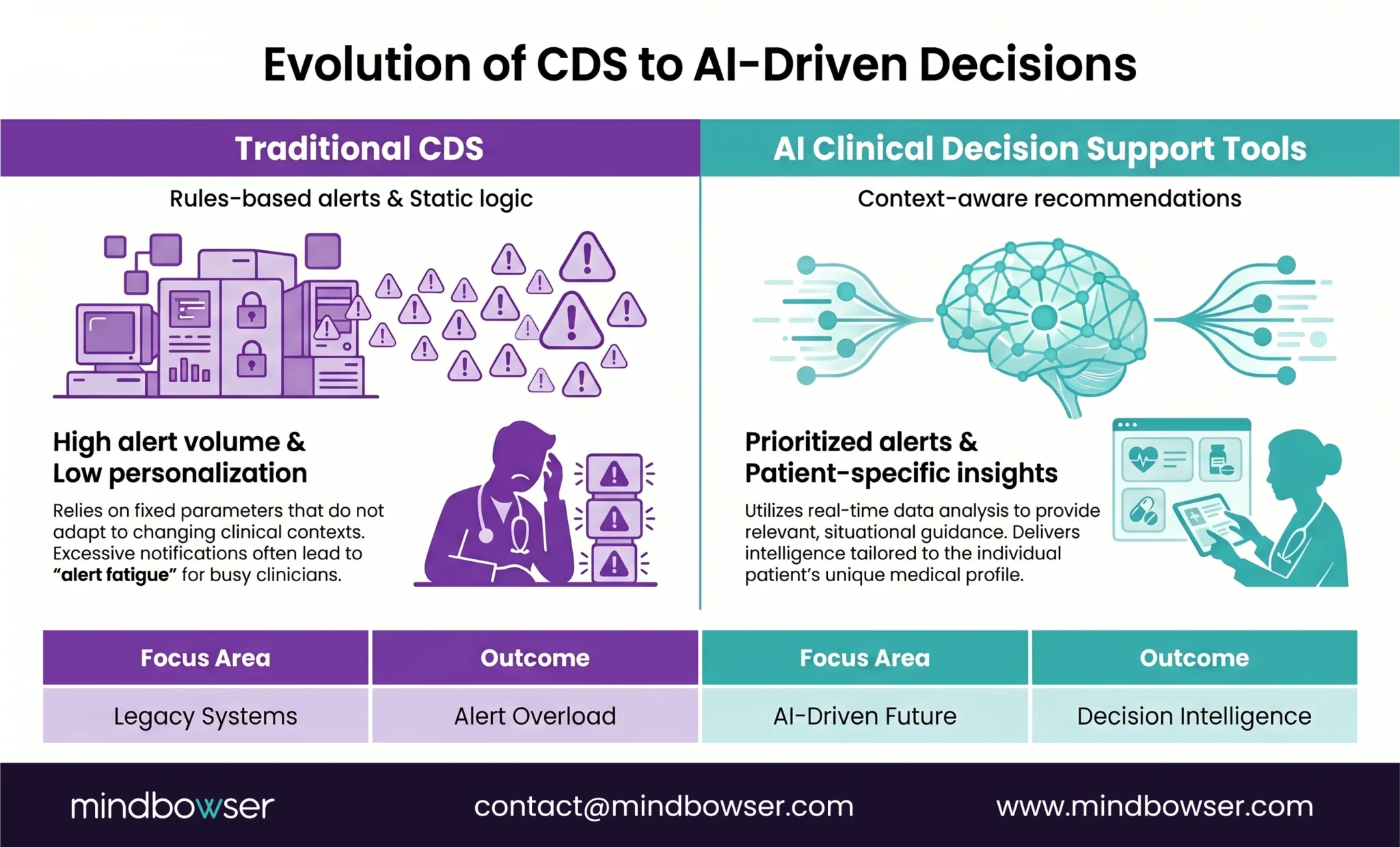
Rules-based CDS tools rely on static logic. If condition X is met, trigger alert Y. That worked when data was limited, and care pathways were simpler. Today, care is anything but simple.
Modern patients come with layered conditions, longitudinal histories, and fragmented data trails. Static CDS cannot interpret nuance. It cannot prioritize signals. It cannot adapt in real time.
So what do clinicians do?
They override.
The signal gets buried in noise. Trust erodes. The tool becomes background clutter instead of decision support.
Short sentence. Big impact.
Static CDS tools no longer match the complexity of modern care delivery.
The original promise of CDS tools still mattersbut their current form cannot keep up with today’s clinical and operational demands.
B. The operational realities hospitals and healthtech teams face today
Walk into any care setting today, and you’ll see the gap immediately. Not theoretical. Operational.
A physician opens the EHR during rounds. Ten alerts fire. Which one actually matters?
This is where traditional clinical decision support tools begin to break under pressure.
First, Alert fatigue in clinical decision support is no longer a side effect; it’s a systemic risk. Clinicians are conditioned to override because too many alerts lack context or urgency. The result? Critical signals get missed alongside low-value ones. A Joint Commission review linked alert fatigue directly to patient safety events, underscoring its seriousness.
Second, data fragmentation limits decision quality. Clinical decisions today depend on inputs from EHRs, claims, labs, imaging systems, and even patient-generated data from wearables. Yet most CDS tools operate within a narrow slice of that data.
No full picture. No continuity. Just partial signals.
Third, workflow friction slows care instead of supporting it. Many CDS tools interrupt at the wrong time or require extra clicks, forcing clinicians to step outside their natural workflow. In high-pressure environments, even a few seconds of friction compounds into frustration.
And then there’s the bigger shift.
Healthcare organizations are now balancing quality outcomes, cost control, and value-based care VBC performance simultaneously.
But that requires better decisions, earlier interventions, and coordinated action across teams.
Traditional CDS tools were never designed for that level of complexity.
They inform. They don’t orchestrate.
Hospitals don’t just need decision support anymore. They need decision alignment across fragmented data, pressured workflows, and value-based outcomes.
C. Why AI Clinical Decision Support Tools are the next step
Here’s the shift. Quiet, but decisive.
Traditional CDS tools answer: “Does this rule apply?”
AI Clinical Decision Support Tools answer: “What matters most for this patient, right now?”
That difference changes everything.
Want to understand how Clinical Decision Support evolved from static rules engines to machine learning, multimodal AI, and emerging agentic systems? Read our detailed guide on whether Clinical Decision Support Systems use AI and how modern AI-driven CDS differs from traditional CDS architectures.
From one-size-fits-all alerts to context-aware recommendations
AI-driven systems analyze patterns across patient history, comorbidities, labs, medications, and even population-level trends. Instead of firing generic alerts, they prioritize what’s clinically relevant. A diabetic patient with rising creatinine and recent medication changes? That gets flagged differently than a stable case.
This isn’t more alerts. It’s smarter prioritization.
From retrospective reporting to real-time intervention
Legacy CDS often looks backward at what happened, what was missed. AI flips that model. It predicts deterioration, flags risk earlier, and enables intervention before escalation.
The impact is measurable. A study published in Nature Medicine found that AI-based early warning systems can identify patient deterioration up to 48 hours earlier than traditional methods.
Time gained is outcome gained.
From isolated rules to longitudinal patient risk insight
Modern care isn’t episodic. It’s continuous AI Clinical Decision Support Tools connect data across encounters, settings, and timeframes to build a longitudinal risk profile.
That means:
- Not just identifying a problem
- But understanding the trajectory
- And predicting what comes next
Three layers. One decision advantage.
What if your CDS system didn’t just react, but anticipated?
This is where clinician trust starts to rebuild. When signals are fewer, sharper, and explainable, adoption follows.
AI doesn’t replace CDS, it completes it.
AI Clinical Decision Support Tools move healthcare from reactive alerts to proactive, context-driven decision intelligence. And that shift is no longer optional; it’s operational.
II. What AI Clinical Decision Support Tools actually change
A. Core capabilities that modernize legacy CDS tools
This is where CDS stops being reactive and starts becoming predictive.
AI Clinical Decision Support Tools don’t just improve existing features. They redefine what decision support means inside a clinical workflow.
Let’s break down what actually changes.
1. Risk stratification and early deterioration detection
AI models continuously analyze patient data to identify who is at risk before symptoms escalate. This includes vitals, labs, historical trends, and subtle clinical signals that static rules miss.
Instead of waiting for thresholds to be crossed, clinicians get early warnings with context. Sepsis risk. Cardiac deterioration. ICU transfer probability.
Earlier signal. Earlier action.
2. Personalized treatment and care pathway recommendations
No two patients follow the same path. AI-driven CDS adapts recommendations based on individual patient profiles, comorbidities, and response patterns.
This moves care from standardized protocols to precision-guided pathwayswhile still aligning with clinical guidelines.
What’s the best next step for this specific patient, not the average one?
That’s the shift.
3. Medication safety, interaction checking, and smarter alert prioritization
Traditional CDS floods clinicians with drug alerts. AI filters them.
By evaluating patient-specific risk, medication history, and context, AI Clinical Decision Support Tools prioritize high-risk interactions and suppress low-value noise.
The result: fewer alerts, higher trust, better adherence.
4. Evidence retrieval and guideline support at the point of care
Clinicians don’t have time to search journals during the encounter. AI surfaces relevant clinical evidence and guidelines in real time, tied directly to the patient’s condition.
This bridges the gap between knowledge and action.
5. Population health and care gap identification for VBC programs
Beyond individual encounters, AI enables organizations to identify care gaps, rising-risk cohorts, and intervention opportunities across populations.
AI makes that visible and actionable.
Five capabilities. One outcome: better decisions at scale.
AI Clinical Decision Support Tools transform CDS from a passive alert system into an active, intelligence-driven clinical partner.
B. Where AI-enhanced CDS tools create measurable value
Leaders don’t invest in AI for features. They invest for outcomes.
This is where AI Clinical Decision Support Tools separate signal from noise. Not in theory, but in measurable impact across cost, quality, and operations.
1. Reducing unnecessary utilization
AI helps identify which interventions are avoidable before they happen. Unnecessary admissions. Redundant tests. Preventable ED visits.
By flagging high-risk patients early, organizations can intervene upstream rather than react downstream.
According to CMS, avoidable hospital readmissions cost Medicare over $26 billion annually. Even a small reduction creates meaningful financial lift.
Less waste. Better allocation.
2. Improving quality measure performance
Quality programs depend on timing, adherence, and documentation. AI-driven CDS ensures that care gaps are identified and addressed in real time, not retrospectively.
This directly impacts:
- HEDIS measures
- STAR ratings
- Value-based reimbursement
Are we catching the gap during the visitor discovering it months later?
That timing difference drives performance.
3. Supporting care managers and physicians with the same shared signal set
One of the biggest operational gaps today is misalignment between frontline clinicians and care management teams.
AI Clinical Decision Support Tools create a shared, prioritized view of patient risk, enabling both teams to act on the same insights.
No duplicate work. No conflicting signals.
Just coordinated action.
4. Strengthening documentation and handoffs
AI can surface missing documentation elements, suggest coding improvements, and ensure continuity across transitions of care.
This improves:
- Clinical accuracy
- Reimbursement integrity
- Handoff clarity between teams
Small fixes. Big downstream impact.
5. Helping organizations move from reactive care to proactive care
This is the real shift.
Traditional models respond after the event. AI enables intervention before escalation, whether to prevent deterioration, avoid readmission, or close a care gap.
That’s not incremental improvement. That’s operational transformation.
Reactive → proactive → predictive. Three stages. One direction.
AI Clinical Decision Support Tools don’t just improve decisions, they reshape how care is delivered, measured, and scaled across the enterprise.
C. High-value use cases to feature in the blog
This is where AI Clinical Decision Support Tools prove their worth inside real clinical moments.
Not dashboards. Not reports. Decisions that change outcomes.
1. Sepsis and deterioration alerts
Sepsis remains one of the leading causes of hospital mortality, yet early detection is notoriously difficult. AI models analyze subtle shifts across vitals, labs, and patient history to flag deterioration risk hours before traditional triggers.
This gives clinicians a critical window to intervene early.
What if escalation could be prevented instead of managed?
2. Readmission risk and discharge planning
Discharge is not the end of care. It’s a transition point.
AI Clinical Decision Support Tools assess readmission risk at the patient level, factoring in clinical, behavioral, and social determinants. This enables tailored discharge plans, follow-ups, and prioritized care management.
The result:
- Fewer avoidable readmissions
- Better continuity of care
- Improved VBC performance
3. Medication optimization and adverse event prevention
Medication-related harm is a persistent issue. The WHO estimates medication errors cost the global healthcare system $42 billion annually.
AI enhances medication safety by:
- Identifying high-risk drug combinations
- Adjusting recommendations based on patient-specific factors
- Prioritizing clinically significant alerts
Fewer alerts. Better decisions.
4. Chronic disease pathway support in cardiology, diabetes, and oncology
Chronic care is where fragmentation hurts the most.
AI-enabled CDS supports longitudinal care pathways, ensuring patients stay aligned with evidence-based treatment plans across visits, providers, and settings.
This is especially impactful in:
- Cardiology (heart failure management)
- Diabetes (glycemic control and complication prevention)
- Oncology (treatment sequencing and monitoring)
Consistency becomes achievable.
5. Prioritization for care management and population health teams
Care teams can’t act on every patient at once. AI helps them focus where it matters most.
By ranking patients based on risk, care gaps, and intervention potential, AI Clinical Decision Support Tools enable targeted outreach and efficient resource allocation.
Right patient. Right time. Right intervention.
Five use cases. One pattern: earlier insight, smarter action.
The value of AI Clinical Decision Support Tools shows up in moments where timing, precision, and prioritization directly impact outcomes.
III. How to implement AI Clinical Decision Support Tools without repeating old CDS mistakes
A. Start with the right clinical and business problem
Most AI CDS initiatives fail before they start because they start too broadly.
Teams try to solve everything. Multiple conditions. Multiple workflows. Multiple stakeholders.
The result?
Dilution. Confusion. No measurable impact.
Where does AI actually move the needle today?
The answer is rarely “everywhere.” It’s one high-friction workflow with clear consequences.
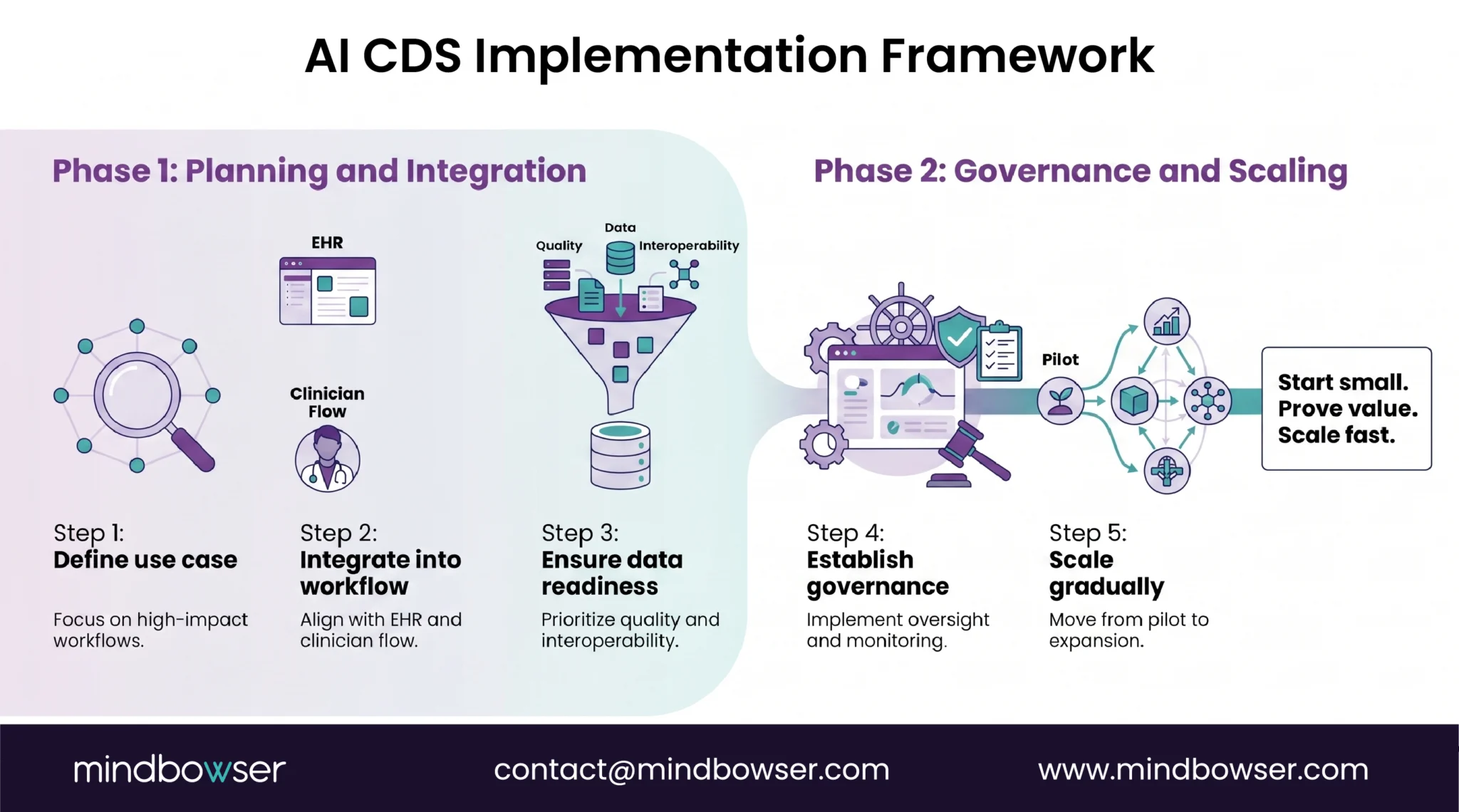
1. Pick one workflow with clear pain and measurable value
Start where the stakes are visible:
- High readmission rates
- Delayed deterioration detection
- Inefficient care management prioritization
Choose a use case where improvement can be quantified in clinical and financial terms.
One workflow. One problem. One outcome.
2. Tie the use case to outcomes, not just model accuracy
A model with 90% accuracy means nothing if it doesn’t change decisions.
This is where many teams go wrong. They focus on:
- Precision
- Recall
- AUC scores
Instead of asking:
Did this change what the clinician did?
Adoption and actionability matter more than model performance alone.
3. Define the VBC metric, clinical metric, and operational metric up front
Before implementation, align on three layers of success:
- Clinical metric: mortality reduction, complication rates, deterioration events
- Operational metric: alert response time, care manager efficiency, workflow adherence
- VBC metric: readmission rates, cost per episode, quality scores
According to CMS, hospitals participating in value-based programs can see payment adjustments tied directly to these outcomes, making measurement financially material.
No baseline? No proof.
Define success before you build.
Short sentence. Critical rule.
The strongest AI Clinical Decision Support Tools implementations start narrow, align to outcomes, and prove value early before scaling across the enterprise.
B. Build for workflow fit, not feature count
More features don’t drive adoption. Better workflow fit does.
This is where many AI Clinical Decision Support Tools quietly fail. The model works. The insights are accurate. But clinicians don’t use it.
Why?
Because it doesn’t fit how care is delivered.
If a tool interrupts at the wrong moment, will anyone trust it, no matter how smart it is?
1. Embed into existing EHR and clinician workflow
Clinicians should not have to leave their primary system to access decision support. AI CDS must live inside the EHR workflow, not alongside it.
That means:
- Surfacing insights within chart review
- Integrating into order entry and documentation flows
- Minimizing clicks and navigation
If it feels like extra work, it won’t be used.
2. Decide when the tool should interrupt and when it should stay passive
Not every insight deserves an alert.
High-risk, time-sensitive events? Interrupt.
Lower-priority recommendations? Stay passive and visible.
This balance is critical to reducing alert fatigue while preserving urgency.
Think in tiers:
- Interruptive alerts for immediate action
- Inline suggestions for contextual guidance
- Background signals for longitudinal tracking
Signal hierarchy matters.
3. Design for explainability and quick clinician judgment
Clinicians don’t trust black boxes. Nor should they.
AI outputs must be:
- Explainable (why this recommendation?)
- Transparent (what data was used?)
- Actionable (what should I do next?)
A 10-second decision window is often all you get.
Can a clinician understand and act without hesitation?
That’s the bar.
4. Create escalation, override, and feedback mechanisms
No system gets every decision right. And clinicians need control.
Effective AI Clinical Decision Support Tools include:
- Clear override options
- Escalation pathways for high-risk cases
- Feedback loops to capture clinician input
This does two things:
- Maintains clinical autonomy
- Improves system performance over time
Adoption grows when clinicians feel in control, not constrained.
AI Clinical Decision Support Tools succeed when they fit naturally into clinical workflows, respect clinician judgment, and prioritize the right signals at the right time.
C. Get the data and interoperability layer right
AI is only as good as the data it sees and the speed at which it sees it.
This is where many AI Clinical Decision Support Tools underperform. Not because the models are weak, but because the data foundation is fragmented, delayed, or incomplete.
If your system sees only half the patient story, how accurate can the decision be?
1. EHR integration
The EHR remains the system of record. AI CDS must integrate deeply into it, not just pull data, but write insights back into clinician workflows.
This includes:
- Real-time data ingestion
- Contextual display within patient charts
- Bi-directional communication
Loose integrations create lag. Tight integrations create trust.
2. FHIR and CDS Hooks considerations
Modern interoperability standards like FHIR and CDS Hooks enable AI systems to trigger insights at the right moment in the workflow.
For example:
- A CDS Hook fires during order entry
- AI evaluates patient context instantly
- A recommendation is surfaced in-line
No delay. No disruption.
Timing is everything.
Organizations that invest in standards-based integration reduce implementation friction and future-proof their architecture.
3. Data quality, provenance, and latency
Not all data is equal.
AI Clinical Decision Support Tools depend on:
- Clean data (accurate, structured, normalized)
- Trusted data sources (clear provenance)
- Low latency (real-time or near real-time updates)
A delayed lab result or missing medication history can change a decision entirely.
Garbage in. Risk out.
4. Governance for model drift and content updates
Clinical data evolves. So should your models.
Without governance:
- Models degrade over time
- Clinical guidelines become outdated
- Performance silently drops
Effective organizations establish:
- Monitoring for model drift
- Scheduled retraining cycles
- Clinical validation of updates
Data isn’t a backend concern. It’s a clinical risk factor.
AI Clinical Decision Support Tools deliver value only when data is accurate, interoperable, and available in real time. Get this wrong, and everything downstream suffers.
D. Treat governance as a design requirement
AI in clinical care is not just a technology decision. It’s a safety decision.
And safety doesn’t get added later. It must be designed in from day one.
Who is accountable when an AI recommendation is wrong or ignored?
That question defines your governance model.
1. Clinical oversight and multidisciplinary review
AI Clinical Decision Support Tools must be guided by clinical leadership, not just technical teams.
This includes:
- Physicians validating use cases and outputs
- Pharmacists reviewing medication-related logic
- Care teams aligning on workflow impact
Decisions are clinical. Oversight must be, too.
2. Regulatory and compliance checkpoints
Healthcare AI operates in a regulated environment. Governance must ensure alignment with:
- HIPAA for data privacy
- FDA guidance for clinical decision support (where applicable)
- Internal compliance policies
Miss this, and risk compounds fast.
Compliance is not a blocker. It’s a guardrail.
3. Human-in-the-loop safeguards
AI should support decisions, not replace them.
Effective systems ensure:
- Clinicians can review and validate recommendations
- Critical decisions require human confirmation
- Override pathways are always available
This maintains clinical accountability and patient safety.
4. Bias monitoring and safety review
AI models can inherit bias from historical data. Left unchecked, this can lead to uneven care delivery.
Organizations must:
- Monitor outcomes across demographics
- Identify disparities in recommendations
- Adjust models and thresholds accordingly
Equity is not optional. It’s measurable.
5. Ongoing performance audits after go-live
Deployment is not the finish line.
Post-launch, teams should continuously track:
- Model performance
- Alert effectiveness
- Clinician adoption and override patterns
Organizations that actively monitor AI systems post-deployment achieve significantly higher sustained ROI compared to those that don’t.
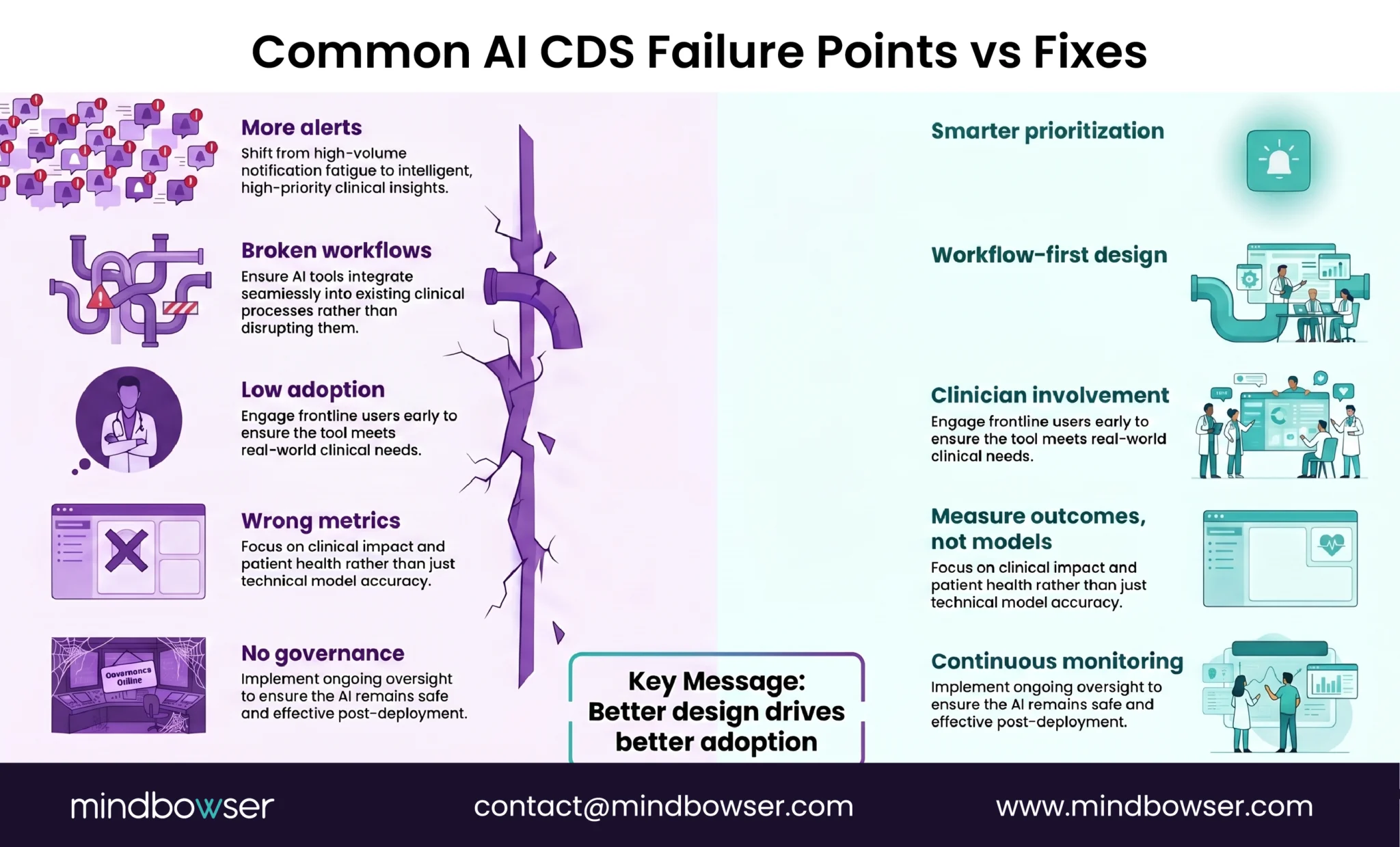
Governance is what turns AI from a pilot into a reliable clinical system.
Treat governance as a core design layer, not an afterthought. It ensures safety, trust, compliance, and long-term performance.
E. Roll out in phases
Big-bang AI deployments rarely work in clinical environments.
Too many variables. Too many stakeholders. Too much risk.
The organizations that succeed with AI Clinical Decision Support Tools take a different path. They prove value in controlled settings, then scale with confidence.
Can you demonstrate impact before expanding across the enterprise?
That’s the goal.
1. Pre-implementation assessment
Before building anything, assess:
- Clinical workflow readiness
- Data availability and quality
- Stakeholder alignment
This step identifies constraints early and prevents costly rework later.
Clarity upfront saves months downstream.
2. Pilot in a narrow clinical setting
Start small. One unit. One condition. One workflow.
For example:
- Sepsis detection in the ICU
- Readmission risk in cardiology
- Care gap closure in a VBC population
A focused pilot allows teams to validate performance in real-world conditions without overwhelming the system.
3. Measure override rates, utilization, outcomes, and trust
Success isn’t just about model accuracy.
Track:
- Override rates (Are clinicians trusting the tool?)
- Utilization (Is it being used consistently?)
- Clinical outcomes (Is care improving?)
- Clinician feedback (Does it fit workflow?)
These signals determine whether the tool is truly adding value.
If clinicians ignore it, does performance even matter?
4. Expand by service line, site, or pathway
Once validated, scale deliberately:
- Extend to adjacent service lines
- Roll out across facilities
- Apply to similar clinical pathways
Each expansion should build on proven success, not assumptions.
5. Build an operating model for scale
Sustained success requires structure.
This includes:
- Defined ownership (clinical + technical)
- Governance frameworks
- Ongoing monitoring and iteration processes
Scaling AI is not a rollout. It’s an operating capability.
AI Clinical Decision Support Tools succeed when rolled out iteratively, measured rigorously, and scaled intentionally, not deployed all at once.
IV. What leaders should ask before choosing an AI CDS platform
A. Clinical fit questions
Not all AI Clinical Decision Support Tools are clinically useful, even if they look impressive on paper.
The real test is simple.
Does this tool improve decisions at the exact moments clinicians struggle today?
That’s where leaders should start.
1. Which decision points does it support well?
Every platform has strengths. Some excel in acute care. Others in chronic disease management or population health.
Leaders need clarity on:
- Where the tool performs reliably
- Which clinical workflows does it enhance
- Where it should not be used
Precision in scope prevents overreach in deployment.
2. Can clinicians understand the logic and source evidence?
Trust is built on transparency.
If clinicians cannot answer:
- Why was this recommendation made?
- What data was used?
- Which guideline or evidence supports it?
They will hesitate or override.
Effective AI CDS platforms provide:
- Clear rationale behind recommendations
- Links to supporting clinical evidence
- Simple, interpretable outputs
If it can’t be explained in seconds, it won’t be trusted.
3. How does it reduce alert noise rather than add to it?
Many tools claim intelligence but still generate excessive alerts. Leaders must evaluate:
- Alert prioritization logic
- Suppression of low-value signals
- Customization based on clinical context
The goal is not more alerts. It’s fewer, better ones.
AI Clinical Decision Support Tools succeed only when clinicians trust, understand, and consistently act on the recommendations provided.
B. Technical fit questions
A strong clinical tool fails fast if it doesn’t fit your architecture.
This is where many AI Clinical Decision Support Tools stall, not because of poor capability, but because of integration friction, latency, and scalability gaps.
Will this system work inside our environment, or force us to rebuild around it?
That’s the real question.
1. How does it integrate with our EHR and existing architecture?
Your EHR is the center of gravity. Any AI CDS platform must integrate without disrupting:
- Clinical workflows
- Data pipelines
- Existing applications
Leaders should evaluate:
- Depth of integration (read-only vs bi-directional)
- Real-time vs batch processing
- Impact on system performance
If integration is heavy, adoption will be light.
2. Does it support FHIR, CDS Hooks, SMART on FHIR, or API-based workflows?
Modern interoperability standards are not optional; they’re foundational.
Look for support across:
- FHIR for structured data exchange
- CDS Hooks for real-time decision triggers
- SMART on FHIR for app-level integration
- APIs for flexibility across systems
These standards determine how easily the tool:
- Fits into workflows
- Scales across systems
- Adapts to future needs
Standards reduce friction. Proprietary models increase it.
3. How is performance monitored and retrained over time?
AI is not static. Performance shifts as data, populations, and care patterns evolve.
Leaders must ask:
- How is model performance tracked?
- What triggers retraining?
- How are updates validated clinically?
Without this, models degrade quietly and decisions suffer.
McKinsey research shows that organizations that actively manage and scale AI initiatives are significantly more likely to achieve sustained value from their investments.
AI without lifecycle management is a short-lived advantage.
Technical fit ensures AI Clinical Decision Support Tools are deployable, scalable, and sustainable, not just promising in isolation.
C. Business fit questions
Even the best AI Clinical Decision Support Tools fail if the economics don’t hold.
This is where executive alignment happens.
Does this investment translate into measurable financial and operational impact?
That answer must be clear before selection, not after deployment.
1. What ROI should we expect in 6, 12, and 24 months?
Leaders should push for time-bound, outcome-linked ROI projections, not vague value claims.
Evaluate across:
- Reduced readmissions
- Lower unnecessary utilization
- Improved coding and reimbursement accuracy
Deloitte highlights that AI-enabled care interventions can deliver measurable ROI when applied to high-impact clinical workflows.
No timeline, no accountability.
2. How will it affect VBC performance, utilization, and care management efficiency?
AI CDS must directly support value-based care goals:
- Improved quality scores
- Reduced cost per episode
- Better care team productivity
This is where impact compounds.
Does it just inform decisions or improve system-wide performance?
That distinction defines long-term value.
3. What staffing, governance, and change management effort is required?
AI is not plug-and-play. It requires:
- Clinical champions
- Governance structures
- Training and adoption programs
Underestimating this leads to stalled deployments.
The hidden cost is not the tool, it’s the change effort.
Business fit ensures AI Clinical Decision Support Tools are not just clinically and technically sound, but financially justified and operationally sustainable.
Ready to move from reactive alerts to real-time AI decision support? Let's talk about your CDS goals.
V. Common implementation mistakes that weaken AI Clinical Decision Support Tools
A. Treating AI as a layer on top of broken workflows
AI does not fix bad workflows. It amplifies them.
This is the most common and costly mistake.
Organizations take existing CDS tools, layer AI on top, and expect transformation. What they get instead is more alerts, more noise, and the same underlying friction.
If clinicians are already ignoring alerts, what happens when you add smarter ones?
They still ignore them.
1. More alerts, same workflow problems
Without redesigning workflows, AI simply increases signal volume.
Even if accuracy improves, poor timing and placement mean:
- Alerts fire at the wrong moment
- Clinicians are interrupted unnecessarily
- Decision support feels like a disruption
Better intelligence, wrong delivery.
2. No service-line ownership
AI CDS often gets deployed as a centralized initiative with no clear ownership at the clinical level.
The result:
- No accountability for outcomes
- No alignment with service-line priorities
- Limited adoption at the frontline
Effective implementations assign ownership within specific clinical domainscardiology, oncology, and critical care, where impact is measurable.
3. No frontline clinician involvement
Tools designed without clinician input rarely fit real workflows.
This leads to:
- Misaligned recommendations
- Poor usability
- High override rates
Clinician involvement is one of the strongest predictors of CDS adoption success.
No clinician voice = no clinician trust.
AI Clinical Decision Support Tools only work when paired with workflow redesign, clear ownership, and frontline engagement.
B. Measuring the wrong success signals
What you measure shapes what you improve and what you miss.
Many AI Clinical Decision Support Tools appear successful on paper but fail in practice because teams track the wrong metrics.
If the model performs well but no one acts on it, is it actually working?
That’s the disconnect.
1. Over-focusing on model performance
Teams often prioritize:
- Accuracy
- Precision
- Recall
These are important but incomplete.
A high-performing model that doesn’t influence decisions delivers zero real-world value. Clinical environments are not test datasets. They are dynamic, pressured, and human-driven.
Performance without action is just math.
2. Under-measuring adoption, overrides, and actionability
The real indicators of success are behavioral:
- Are clinicians using the tool?
- How often are alerts overridden?
- Are recommendations leading to action?
These signals reveal whether AI is trusted and embedded in workflow.
Adoption is the true KPI.
3. Ignoring downstream care and financial outcomes
Even when adoption is measured, many teams stop there.
They fail to connect AI CDS impact to:
- Clinical outcomes (reduced complications, improved recovery)
- Operational outcomes (efficiency, throughput)
- Financial outcomes (cost savings, VBC performance)
This breaks the value chain.
Did the decision change, and did that change matter?
That’s the metric that counts.
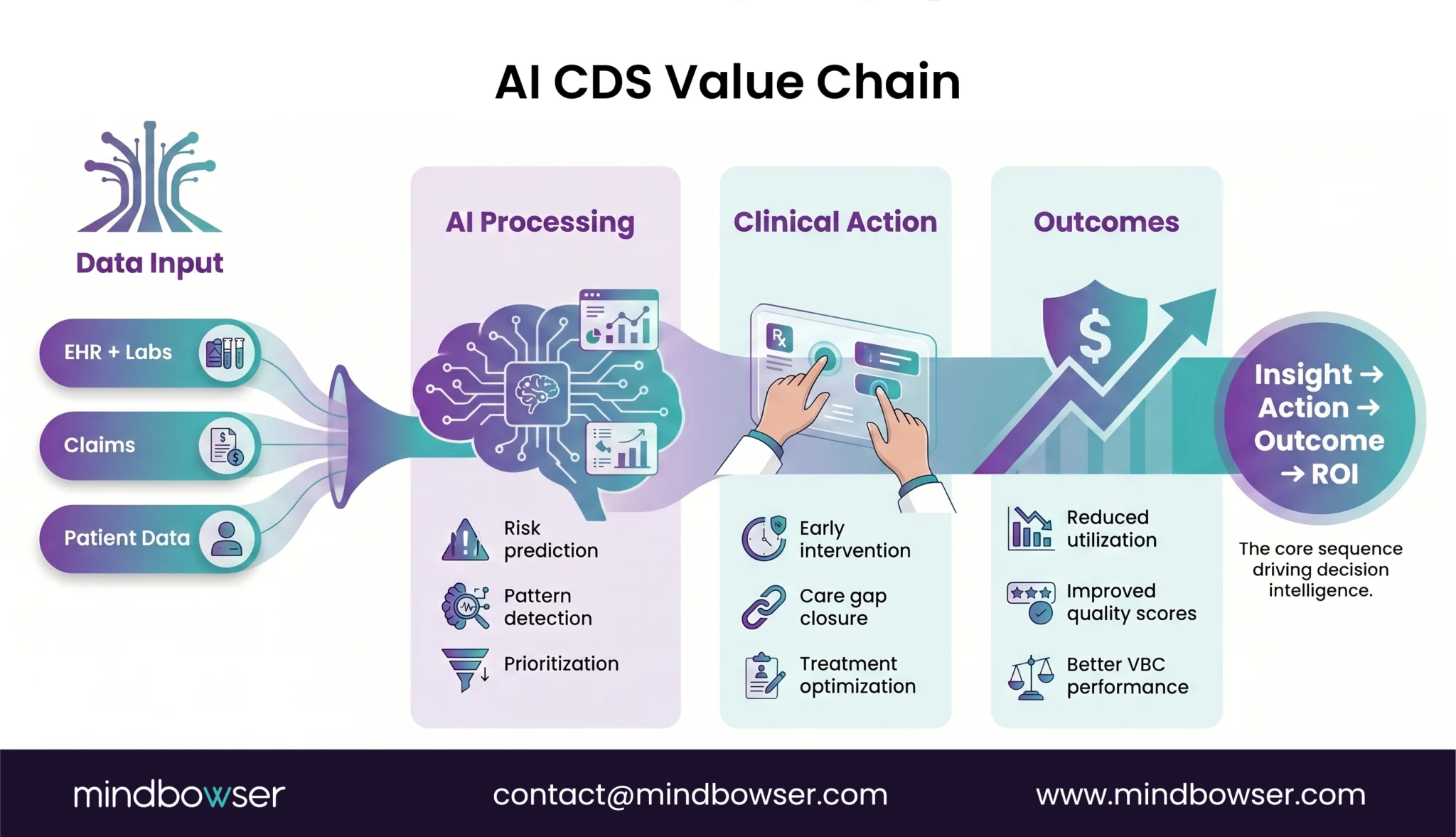
Insight → action → outcome → value. Miss one step, and ROI disappears.
AI Clinical Decision Support Tools must be evaluated based on real-world impact, not just technical performance.
C. Underinvesting in change management
AI doesn’t fail because of technology. It fails because people don’t adopt it.
This is the quiet breakdown in many AI Clinical Decision Support Tools deployments. The system is live. The models are working. But usage stalls.
Do clinicians know when to trust the system and when to question it?
If that’s unclear, adoption drops fast.
1. No champion network
Successful implementations are not driven by central teams alone. They rely on clinical champions at the frontline.
These champions:
- Advocate for the tool
- Guide peers on usage
- Provide real-time feedback
Without them, AI remains “someone else’s initiative.”
Adoption spreads peer-to-peer, not top-down.
2. No training for when to trust, challenge, or escalate
Training often focuses on how the tool works, not how to use it in real decisions.
Clinicians need clarity on:
- When to act immediately
- When to validate the recommendation
- When to override or escalate
This builds confidence and appropriate reliance.
Without it, hesitation takes over.
3. No closed loop for clinician feedback
If clinicians flag issues but nothing changes, trust erodes quickly.
Effective AI Clinical Decision Support Tools include:
- Feedback capture within workflow
- Review mechanisms for recurring issues
- Iteration cycles based on real usage
According to McKinsey’s State of AI research, organizations that embed AI into workflows and actively engage users see higher adoption and sustained value.
Feedback is not optional. It’s fuel for improvement.
Change management determines whether AI Clinical Decision Support Tools become trusted clinical partners or ignored background systems.
VI. How Mindbowser can help
A. Strategy to implementation support
Most teams know AI Clinical Decision Support Tools matter. Few know where to start.
That’s where execution breaks.
Mindbowser approaches this differently. Not as a tool deployment but as a clinical and operational transformation initiative.
We begin with:
- Use-case discovery aligned to VBC goals and digital priorities
- Workflow mapping across clinicians, care managers, and operational teams
- Data and interoperability planning to ensure real-time, reliable inputs
Where does AI actually improve decisions today, and how will that show up in outcomes?
That question drives every engagement.
Clarity first. Then build.
B. Build and scale capabilities
Once the foundation is clear, execution focuses on embedding intelligence into real workflows.
Mindbowser supports:
- AI model integration into EHR-connected clinical workflows
- Explainable UX so clinicians can trust and act on recommendations quickly
- Governance frameworks, testing protocols, and post-launch monitoring
This ensures systems are not just accurate but usable, trusted, and scalable.
Short sentence.
Adoption follows design.
C. Why Mindbowser is a strong fit for this work
This work requires more than engineering. It requires a healthcare context.
Mindbowser brings:
- Deep experience in healthcare and digital health delivery
- Compliance-first product engineering (HIPAA and SOC 2 aligned by design)
- A custom-built approach, not force-fitting rigid products into complex workflows
- Proven ability to connect clinical workflows, data systems, and measurable business outcomes
Build what fits your system, not the other way around.
That’s the difference.
The decision shift ahead
AI Clinical Decision Support Tools are not about adding intelligence; they’re about improving decisions where they matter most.
When embedded into workflows, grounded in data, and measured by outcomes, they reduce noise, guide action, and strengthen both clinical and financial performance.
The opportunity is clear: move from reactive alerts to proactive, trusted decision-making at scale.
AI Clinical Decision Support Tools use real-time data and machine learning to provide context-aware clinical recommendations. Unlike traditional CDS, they adapt to patient-specific conditions and evolving risk signals.
Traditional CDS relies on static rules and generic alerts, while AI CDS delivers dynamic, prioritized, and personalized insights. This reduces alert fatigue and improves patient care
Yes, modern AI CDS tools are designed to integrate directly into EHR workflows using standards like FHIR and CDS Hooks, learn more about the role of EHR in clinical decision support.. This ensures insights are delivered at the right moment in the care process.
Common challenges include workflow misalignment, poor data quality, and lack of clinician adoption. Successful implementations focus on governance, usability, and clear outcome measurement.
AI CDS tools help identify care gaps, prioritize high-risk patients, and enable early intervention. This leads to better quality scores, reduced costs, and improved patient outcomes.

