



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
A clinical decision support system is shifting from static alerts to dynamic, workflow-embedded intelligence inside the EHR. Over the next 24-36 months, success will hinge on AI-assisted evidence retrieval, alert precision, multi-modal data integration, and measurable ROI. Health systems that treat CDSS as an operational capability, not a tool, will improve safety, reduce clinician burden, and drive value-based care outcomes.
Watch: Future Trends in Clinical Decision Support Systems
I. The Clinical Decision Support System Is Being Rebuilt for Point-of-Care Reality
A. From “alerts” to decision advantage at the point of care
Most clinical decision support systems did not fail because of bad logic. They failed because of bad timing.
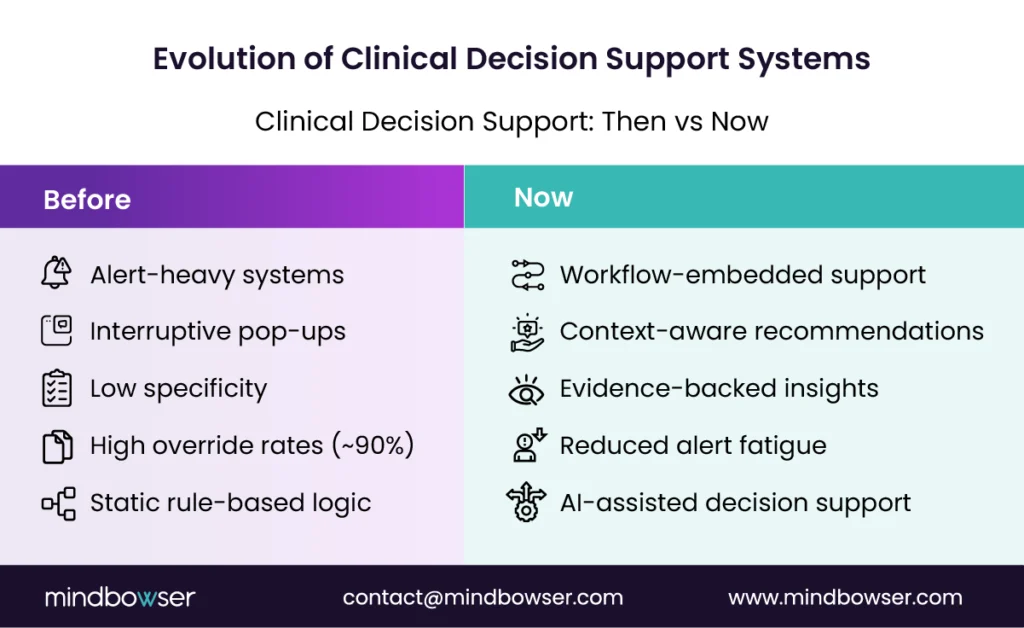
For years, CDSS meant interruptive alerts. Pop-ups. Hard stops. Generic reminders that showed up at the worst possible moment. Clinicians clicked through them, often within seconds. The result? Alert fatigue became a patient safety risk, not just a usability issue.
According to studies, up to 90% of alerts are overridden, often because they lack context or relevance. That is not a technology failure. It is a workflow failure.
Picture this:
A physician is managing a complex inpatient case. Labs are evolving. Comorbidities stack up. An alert fires based on a static rule written months ago.
It is ignored. Understandably.
What changes now is fundamental.
Modern point-of-care decision support is no longer interruptive. It is embedded, contextual, and timed to clinical intent. Instead of forcing decisions, it supports them in flow.
Three shifts define this evolution:
1. Context replaces generic logic
CDSS now considers patient history, current workflow, specialty, and setting. Not just a rule.
2. Timing aligns with decision moments
Instead of firing at random, support appears only when orders are being placed or diagnoses are being evaluated.
3. Outcomes become the benchmark
The new expectation is clear: improve safety, reduce variation, and increase throughput. If it cannot be measured, it will not be funded.
This is where advanced clinical decision support separates itself.
It is not about more alerts. It is about better decisions, faster.
CDSS is moving from noise to signal. And clinicians can feel the difference.
B. The “AI clinical decision support system” shift: conversational plus constrained
AI is entering CDSS fast. But not the way most people think.
This is not about replacing clinical judgment. It is about making evidence easier to access, faster to interpret, and safer to apply.
The rise of the AI clinical decision support system is centered on one idea:
Conversational access to trusted evidence, inside the workflow.
Imagine this scenario:
A clinician reviews a complex case and asks, “What do current guidelines recommend for this patient profile?”
Instead of searching across tabs, PDFs, and memory, the system responds instantly with:
- A summarized recommendation
- Supporting guideline citations
- Context aligned to the patient’s condition
No guesswork. No hallucination risk.
That last point matters.
1. Conversational, but evidence-grounded
Modern CDS does not “generate” answers freely. It retrieves from validated clinical sources and presents them in structured, explainable formats. This is the core of evidence-based clinical decision support.
According to McKinsey, AI can improve clinical workflow efficiency and reduce clinician burden when paired with trusted data sources. The gain is not just speed. It is confidence.
2. Role clarity is non-negotiable
AI is an assistant. Not a decision-maker.
The system supports clinical reasoning. It does not override it. This distinction is critical for both regulatory acceptance and clinician trust.
Assist, not replace. Guide, not decide.
3. Embedded directly into EHR workflows
The real shift is where AI lives.
It is no longer a separate tool. It is being integrated into EHR clinical decision support layers within systems such as Epic and Cerner. That means:
- In-chart summarization
- Order recommendation support
- Documentation assistance tied to clinical context
No context switching. No disruption.
Here’s the tension:
If AI is too open, it becomes unsafe.
If it is too rigid, it becomes ignored.
The winning model sits in between. Constrained intelligence with clinical guardrails.
AI in CDSS is not about automation. It is about trusted acceleration of clinical thinking.
C. The market forces shaping investment and adoption
Follow the money. It tells you where CDSS is going.
The clinical decision support system market is not growing because of interest. It is growing because health systems are under pressure to prove outcomes.
Margins are tight. Clinician burnout is high. Value-based care contracts are expanding. In this environment, CDS is no longer a “nice-to-have.” It is becoming infrastructure for clinical and financial performance.
1. Buyers are paying for measurable outcomes
The conversation has changed in boardrooms.
It is no longer:
“Does this CDS tool have features?”
It is now:
“Does this reduce readmissions, improve adherence, or prevent denials?”
Clinical impact, operational efficiency, financial return. That triad defines buying decisions.
2. EHR integration is now a growth gate
If a solution does not integrate deeply into Epic or Cerner, it struggles to scale.
Why?
Because clinicians will not adopt tools that live outside their workflow. Period. Even the most advanced clinical decision support software fails if it requires extra clicks, logins, or mental context switching.
This is why EHR clinical decision support integration is no longer a feature. It is a requirement.
No workflow fit. No adoption.
3. “Advanced clinical decision support” is becoming an enterprise capability
Forward-looking health systems are moving beyond isolated tools.
They are building CDSS as a shared capability layer across:
- Inpatient care
- Ambulatory settings
- Population health programs
- Virtual care environments
This includes shared services like evidence retrieval, orchestration, and monitoring.
Here’s the strategic shift:
Instead of buying a CDSS tool for each use case, organizations are investing in platform thinking.
Because fragmentation does not scale.
The market is rewarding CDSS that fits the workflow, proves ROI, and scales across the enterprise.
II. Future Trends in Clinical Decision Support Systems (What Will Matter Most in the Next 24-36 Months)
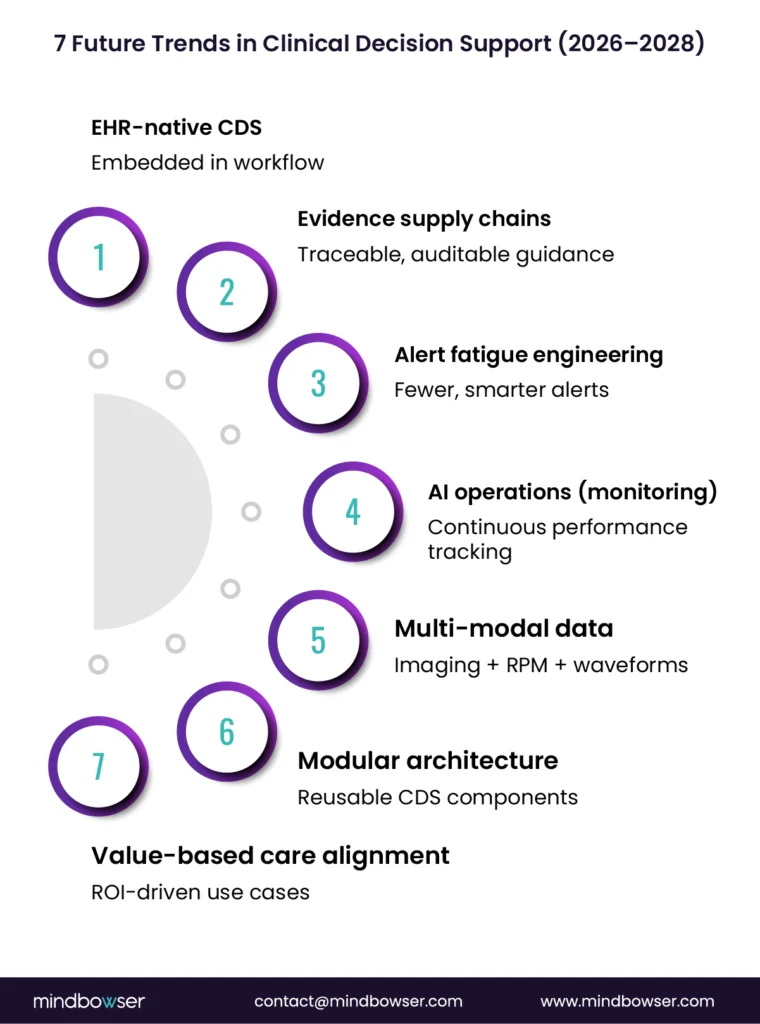
A. Trend 1: EHR-native, workflow-embedded CDSS becomes the default
The future of the clinical decision support system lives inside the EHR. Not beside it.
This is the single most important shift shaping the next wave of CDSS adoption.
For years, healthcare organizations experimented with external tools layered on top of the EHR. Some delivered insights. Most failed to gain traction.
Why?
Because clinicians do not leave their workflow to think.
They think inside it.
That is why EHR-native CDSS is becoming the default architecture. Decision support is now embedded directly into clinical workflows, appearing exactly when decisions are made.
1. In-workflow evidence retrieval and summarization
Instead of searching across multiple systems, clinicians access real-time, patient-specific evidence directly in the chart.
This includes:
- Guideline summaries aligned to patient context
- Risk scores calculated dynamically
- Recommendations backed by citations
Physicians spend nearly half their time on EHR and desk work.
2. Adaptive order sets and care pathways
Traditional order sets are static. They assume every patient fits a predefined path.
Modern healthcare decision support systems change that.
They adapt based on:
- Comorbidities
- Prior treatments
- Real-time clinical signals
One pathway does not fit all.
Instead, CDS dynamically adjusts recommendations, making care pathways context-aware rather than rule-bound.
3. Reducing clicks and cognitive load becomes a KPI
This is new.
Health systems are now measuring CDSS success not just by outcomes, but by interaction efficiency.
- Fewer clicks per order
- Reduced navigation steps
- Faster time-to-decision
Ask yourself:
Is your CDSS helping clinicians think, or slowing them down?
Because if it adds friction, it will be bypassed.
The winning CDSS systems are invisible. They work inside the workflow, at the moment of decision, without adding burden.
B. Trend 2: Evidence supply chains get productized (and audited)
Evidence is no longer static content. It is becoming an operational pipeline.
In the past, clinical decision support systems relied on guidelines that were manually updated, loosely governed, and often outdated by the time they reached clinicians.
That model is breaking.
Today, health systems are demanding traceability, freshness, and accountability in every recommendation surfaced at the point of care.
Why this shift now?
Because when CDSS influences decisions, it also inherits clinical risk.
According to WHO, up to 1 in 10 patients experience harm in healthcare settings, with a significant portion linked to decision variability and outdated practices. CDSS is now expected to reduce that variability rather than contribute to it.
1. Every recommendation must show its source
Modern evidence-based clinical decision support systems are built to answer one critical question:
“Where did this recommendation come from?”
That means:
- Direct citation of guidelines, studies, or pathways
- Version control tied to clinical updates
- Transparent logic behind recommendations
No black boxes. No blind trust.
2. Content freshness becomes a safety requirement
Clinical knowledge evolves fast. What was standard six months ago may already be outdated.
This is pushing organizations to treat evidence like software:
- Continuous updates
- Validation workflows
- Deployment cycles
Static content = clinical risk
Living evidence = safer decisions
3. Governance models become non-negotiable
Health systems are formalizing the management of CDS content.
This includes:
- Clinical review boards for approval
- Defined update cadences
- Rollback mechanisms when guidance changes
Here is the shift in simple terms:
Evidence + Governance = Trust at scale
Without governance, even the best CDSS logic fails to be adopted.
And here’s the tension:
Move too slow, and evidence becomes stale.
Move too fast, and trust erodes.
The winners balance both.
CDS is no longer just about delivering guidance. It is about managing the lifecycle of clinical evidence with precision.
Ready to Build Clinical Decision Support That Fits Your Workflow and Proves ROI?
C. Trend 3: Alert fatigue engineering becomes a competitive differentiator
Health systems are no longer asking how many alerts a CDSS can generate. They are asking how many can be eliminated.
This is a turning point.
For years, more alerts were seen as better safety coverage. But the reality proved the opposite. Excessive alerts created noise, slowed clinicians down, and led to widespread overrides.
According to studies, override rates can exceed 85-90%, which means most alerts are not trusted or not useful in context.
So what changed?
Leading organizations are now treating alert design as an engineering discipline, not a configuration task.
1. From high-volume alerts to high-confidence interventions
Instead of firing on every possible condition, modern advanced clinical decision support systems prioritize:
- High-risk scenarios
- Clinically meaningful thresholds
- Context-aware triggers
The goal is simple:
Say less. Mean more.
Fewer alerts x Higher relevance = Better adherence
This shift directly improves both clinician trust and patient safety.
2. Personalization by role, specialty, and care setting
An ED physician and a primary care provider do not need the same alerts. Neither does an inpatient nurse nor a specialist.
Modern CDSS adapts based on:
- Clinical role
- Specialty
- Care setting (ED, inpatient, ambulatory)
Same patient. Different context. Different decision support.
This level of personalization is what makes healthcare decision support systems usable at scale.
3. Continuous tuning using real-world signals
Alert logic is no longer static after deployment.
Health systems are now using:
- Override rates
- Acceptance patterns
- Outcome correlations
to continuously refine CDS behavior.
Feedback loops + Outcome signals = Smarter CDS over time
This is where CDS starts to behave less like a tool and more like a learning system.
But here is the hard truth:
If your CDSS is not being actively tuned, it is already outdated.
The future belongs to CDS systems that earn attention, not demand it.
D. Trend 4: Drift detection, monitoring, and “clinical AI operations” go mainstream
Clinical decision support does not fail at launch. It fails quietly over time.
This is one of the most underestimated risks in modern CDS programs.
Models, rules, and pathways that perform well today can degrade as patient populations shift, clinical practices evolve, and data inputs change. This is known as model drift, and in healthcare, it carries real consequences.
And the dangerous part?
Most teams do not notice until outcomes are impacted.
1. Why CDSS logic decays in real environments
Several factors drive this:
- Changes in patient demographics
- New clinical guidelines
- Shifts in documentation patterns
- Data quality issues over time
Static logic in dynamic environments = declining accuracy
This is why CDSS can no longer be treated as a “set and forget” system.
2. Operational dashboards become essential
Leading health systems are building clinical AI operations layers to continuously monitor CDS performance.
These dashboards track:
- Model accuracy and calibration
- Bias across patient populations
- Alert acceptance and override trends
- Safety signals tied to outcomes
Visibility leads to accountability leads to safer care
Without this, CDSS operates in the dark.
3. Clear playbooks for intervention and rollback
Monitoring alone is not enough. Teams need predefined actions when something goes wrong.
This includes:
- Thresholds for pausing CDSS logic
- Rollback strategies to previous versions
- Clinical escalation workflows
What happens if a recommendation starts causing harm?
If there is no clear answer, the system is not production-ready.
Monitoring + governance = controlled risk
That combination is becoming a baseline expectation for any serious clinical decision support software deployment.
CDS is evolving into a living system that requires continuous oversight, not periodic review.
E. Trend 5: Multi-modal decision support expands beyond text and labs
Clinical decision support is no longer limited to structured data.
For years, CDS systems relied heavily on discrete inputs: lab values, medication lists, coded diagnoses. Useful, but incomplete.
Real clinical signals do not exist in a single format.
They live across images, waveforms, notes, and increasingly, patient-generated data.
This is where the next leap in healthcare decision support systems is happening.
1. Imaging, waveforms, and continuous signals enter CDSS
Modern CDSS is beginning to ingest and interpret:
- Radiology and pathology images
- ECG and waveform data
- ICU monitoring signals
These inputs enable earlier and more precise detection of clinical deterioration.
Health-system case evidence suggests that predictive monitoring can improve early detection and may contribute to lower mortality when embedded into escalation workflows.
Think about the shift:
Instead of reacting to lab changes, clinicians can act on early physiological signals.
That is a different level of intervention.
2. Predictive support for deterioration and chronic care
Multi-modal CDSS enables use cases like:
- Early sepsis detection
- Cardiac event prediction
- Chronic disease progression tracking
These are not static alerts. They are ongoing risk assessments that evolve as the patient does.
More signals leads to earlier detection leads to better outcomes
Used carefully, this improves both acute and longitudinal care decisions.
3. Patient-generated data enters the clinical loop
Remote patient monitoring and wearables are adding a new dimension to healthcare.
- Blood glucose trends
- Activity levels
- Sleep patterns
- Blood pressure readings at home
But this introduces a challenge.
How much data is useful, and how much is noise?
Without guardrails, CDSS risks overwhelming clinicians again.
That is why leading systems apply:
- Threshold-based filtering
- Context-aware prioritization
- Clear escalation pathways
Signal without filtering = noise at scale
The future CDSS sees more, earlier, and across more dimensions, but only succeeds if it prioritizes what truly matters.
F. Trend 6: Modular architectures replace point solutions
One CDS tool per use case is breaking down under scale.
Many health systems took a fragmented approach over the last decade. One tool for sepsis alerts. Another for medication safety. A separate system for population health.
It worked for a while.
But as CDS expands across the enterprise, this model creates duplication, inconsistency, and rising maintenance costs.
Different tools. Different logic. Different outcomes.
That is not sustainable.
1. Why point solutions fail at enterprise scale
Each standalone CDSS tool introduces:
- Separate data pipelines
- Independent logic models
- Disconnected governance processes
Over time, this leads to:
- Conflicting recommendations
- Increased IT overhead
- Slower updates across systems
Fragmentation increases risk, not flexibility.
This is why leading organizations are shifting toward modular CDS architectures.
2. Reusable components become the foundation
Instead of building CDSS repeatedly, health systems are investing in shared components such as:
- Identity and patient context layers
- Data normalization and terminology mapping
- Evidence retrieval engines
- Decision orchestration services
These components can be reused across multiple use cases, reducing duplication and improving consistency.
Build once. Apply everywhere.
That is the architectural shift.
3. Vendor strategy is changing with it
The clinical decision support system market is evolving in response.
Buyers are now evaluating vendors based on:
- Interoperability standards (FHIR, CDS Hooks)
- Ability to integrate into existing ecosystems
- Flexibility to plug into modular stacks
Not just features.
Closed systems are losing ground to interoperable components.
Because health systems want control. Not lock-in.
The future of CDS is not a single product. It is a connected architecture of reusable decision capabilities.
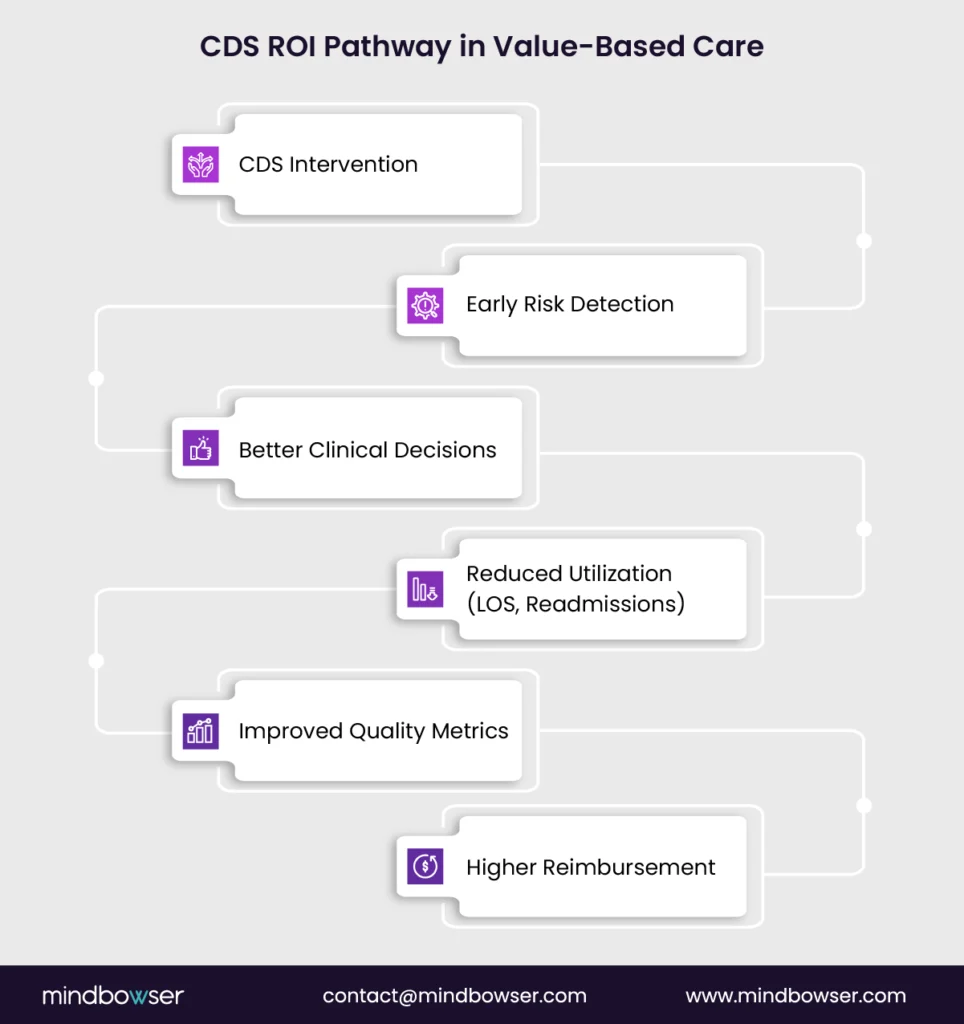
G. Trend 7: Value-based care drives which CDSS use cases win funding
Not all CDSS initiatives will survive budget scrutiny. Only the ones tied to outcomes will.
This is the most decisive shift shaping the clinical decision support system market.
Health systems are moving deeper into value-based care (VBC) models, where reimbursement depends on quality, cost control, and patient outcomes. In this environment, CDS is no longer evaluated solely on capability.
It is evaluated on financial impact.
So the question becomes:
Where does CDS actually move the needle?
1. CDS tied to avoidable utilization gets priority
The highest-funded use cases are those that reduce:
- Hospital readmissions
- Emergency department revisits
- Length of stay (LOS)
These are measurable, high-cost areas where CDSS can directly influence decisions.
Clinical insight leads to better decisions leads to lower utilization
That chain is what CFOs care about.
2. Quality measures and risk adjustment shape CDS design
CDS is increasingly aligned with:
- HEDIS quality measures
- Risk adjustment accuracy
- Documentation completeness
Why?
Better documentation and coding directly impact reimbursement under VBC contracts.
Missed documentation is missed revenue.
CDSS now supports not just care decisions, but also financial accuracy.
3. Equity and variation reduction become measurable outcomes
Variation in care is costly and risky.
Modern clinical decision support software is being used to:
- Standardize care pathways
- Reduce unwarranted variation
- Improve equity across populations
This is no longer a reporting exercise. It is tied to performance metrics and incentives.
Consistency in care = Predictability in outcomes
And predictability is what value-based models reward.
Here’s the strategic reality:
If a CDS use case cannot show ROI in terms of cost, quality, or risk, it will struggle to get funded.
In a VBC world, CDSS wins when it connects clinical decisions directly to financial outcomes.
III. How Buyers Should Evaluate Clinical Decision Support Software in 2026 Budget Cycles
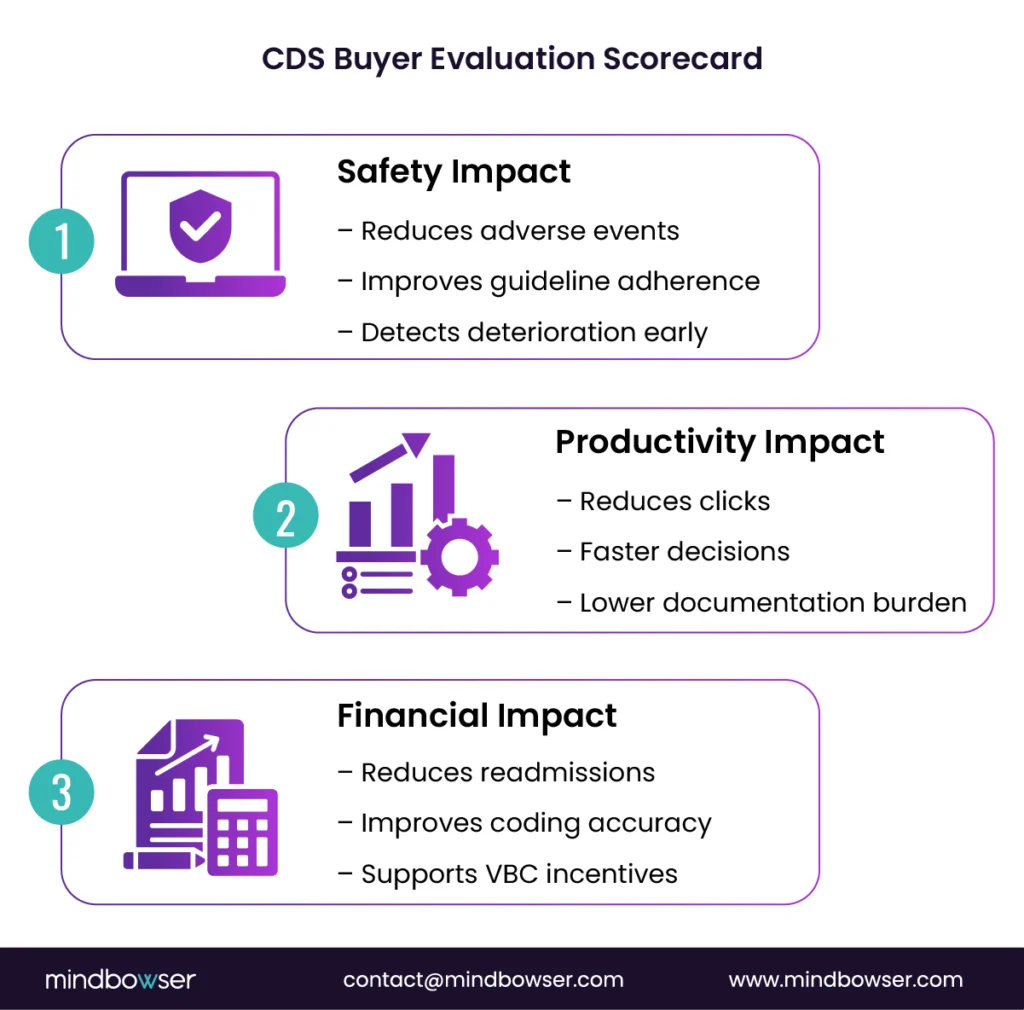
A. The executive scorecard (CIO/CMIO/CFO view)
Buying a clinical decision support system is no longer a technology decision. It is a performance decision.
Executives are not evaluating CDS based on features or demos. They are evaluating it based on what moves clinical, operational, and financial metrics.
That requires a clear scorecard.
1. Safety impact: Does it reduce clinical risk?
At the top of the list is patient safety.
Leaders are asking:
– Does CDS reduce adverse drug events?
– Does it improve guideline adherence?
– Does it catch deterioration earlier?
Better decisions → Fewer errors → Safer care
If CDS cannot demonstrate this, it struggles to justify adoption.
2. Productivity impact: Does it reduce clinician burden?
Burnout is now a financial and operational issue.
CDS must show:
– Reduced time-to-decision
– Lower documentation burden
– Improved workflow efficiency
Does this system save clinician time, or consume more of it?
That question alone determines adoption.
3. Financial impact: does it drive measurable ROI?
This is where decisions get finalized.
Executives expect CDS to influence:
– Avoidable utilization (readmissions, LOS)
– Denial prevention and documentation accuracy
– Quality incentives under VBC contracts
Clinical impact + Operational efficiency = Financial return
That connection must be explicit.
No ROI, no budget.
That is the reality in 2026 planning cycles.
The winning CDS platforms are those that tie clinical improvements directly to operational and financial outcomes.
B. The technical diligence checklist (CTO/VP Apps/Architect view)
A CDS that looks good in a demo can still fail in production.
This is where technical diligence separates successful deployments from stalled pilots.
For CTOs and architects, the focus is not just on capability. It is integration, data integrity, and control.
1. Interoperability: can it plug into your ecosystem?
Modern ehr clinical decision support depends on standards-based integration.
Key requirements include:
– FHIR APIs for data access
– CDS Hooks for real-time workflow triggers
– SMART on FHIR for embedded applications
If these are missing, integration becomes slow, expensive, and fragile.
Standards alignment = Faster integration
Ask this early:
Will this work inside your EHR, or around it?
Because “around it” usually means low adoption.
2. Data readiness: Is your foundation strong enough?
Even the best clinical decision support system fails with poor data.
Key areas to assess:
– Terminology mapping (SNOMED, LOINC, ICD)
– Data completeness and missingness handling
– Provenance tracking (where data came from and when)
If the data is inconsistent, can the CDS still make reliable recommendations?
That is a critical risk.
Clean data → Reliable CDS → Trusted decisions
Without this chain, outputs become questionable.
3. Security and compliance: does it protect PHI end-to-end?
CDS operates on sensitive patient data. There is no margin for error.
Leaders must validate:
– Role-based access controls
– Full audit trails for decisions and recommendations
– Clear PHI boundaries across systems
For organizations operating under HIPAA and SOC 2expectations, this is non-negotiable.
Can you explain who accessed what, when, and why?
If not, compliance risk increases.
Security + Auditability = Operational trust
That trust is essential for both regulators and clinical leadership.
A CDS platform must fit your architecture, trust your data, and protect your patientsor it will not scale.
C. The clinical governance model (what prevents “pilot purgatory”)
Most CDS initiatives do not fail because of technology. They fail because no one owns them clinically.
This is what creates “pilot purgatory.”
A promising clinical decision support system gets deployed, shows early value, and then stalls. No scaling. No sustained adoption.
Why?
Because governance was never defined.
1. Clinical ownership must be explicit
Every CDS intervention needs a named clinical owner.
This includes:
– Approval of logic and evidence
– Accountability for outcomes
– Ongoing review of performance
Without ownership, CDS becomes “IT-driven.” And clinicians disengage.
Clinical ownership → Trust → Adoption
That sequence is predictable.
2. Monitoring and drift response must be operationalized
Governance is not just about approval. It is about ongoing control.
Teams must define:
– What metrics are monitored (accuracy, overrides, outcomes)
– When intervention is required
– Who takes action
If performance drops, who steps in?
If that answer is unclear, risk increases quickly.
3. Change management must be designed, not assumed
Even the best CDS fails if clinicians are not aligned.
Effective programs include:
– Targeted training tied to workflows
– Feedback loops from frontline users
– Clear communication of “why this matters.”
Because adoption is not automatic.
Good logic alone does not drive behavior. Alignment does.
Here’s the pattern:
No ownership → No trust → No adoption → No ROI.
CDS succeeds when it is treated as a clinically governed program, not a technical deployment.
IV. How Mindbowser Can Help Health Systems and Healthtech Teams Win With CDS
A. Build EHR-integrated point-of-care decision support that clinicians will actually use
The hardest part of CDS is not building it. It is making clinicians use it.
This is where most implementations fall short.
At Mindbowser, the focus starts with workflow reality, not features. Because decisions do not happen in dashboards. They happen inside clinical flow.
1. Workflow discovery: where decisions actually happen
Before writing a single rule or model, teams map:
– Where decisions are made (orders, diagnosis, discharge)
– Where friction exists (delays, rework, overrides)
– Where CDS can assist without interrupting
If you place CDS at the wrong moment, it will be ignored.
That is why workflow-first design drives adoption.
2. UX patterns that reduce fatigue and increase adherence
Mindbowser applies proven patterns to ensure CDS is:
– Context-aware, not interruptive
– Minimal in clicks and cognitive load
– Aligned to clinician intent
Right moment + Right context = Higher adherence
This is how to reduce alert fatigue without compromising safety.
3. Deep integration into EHR workflows
CDS is built directly into ehr clinical decision support layers across Epic and Cerner environments.
This includes:
– CDS Hooks-based triggers
– SMART on FHIR embedded apps
– In-workflow recommendations and summaries
No switching systems. No disruption.
CDS works when it feels like part of the workflow, not an add-on.
B. Deliver evidence-based clinical decision support with governance built in
CDS without evidence transparency does not scale. CDS without governance does not last.
This is where many health systems struggle. They implement clinical decision support software, but cannot clearly explain the evidence behind it or manage updates over time.
Mindbowser addresses both from the start.
1. Evidence retrieval and citation by design
Every recommendation is tied to:
– Clinical guidelines
– Peer-reviewed studies
– Approved care pathways
This ensures evidence-based clinical decision support is not just a label, but a verifiable system.
Can your clinicians see why a recommendation exists?
If yes, trust increases. If not, adoption drops.
2. Built-in workflows for updates, review, and audit
Clinical knowledge evolves. CDS must evolve with it.
Mindbowser designs systems with:
– Structured review workflows for clinical leadership
– Version control for guidelines and logic
– Audit trails for every change
Evidence clarity + Governance discipline = Sustained trust
This allows organizations to move fast without losing control.
3. Monitoring and safety guardrails aligned to stakeholders
Governance is incomplete without visibility.
That is why CDS implementations include:
– Performance monitoring dashboards
– Alert acceptance and outcome tracking
– Safety thresholds and escalation triggers
If something goes wrong, how quickly can you detect and respond?
That capability defines maturity.
Trust in CDS is built through transparent evidence, controlled updates, and continuous monitoring.
C. VBC-first CDS use cases that show ROI fast
Speed to ROI is what separates funded CDS programs from stalled ones.
Health systems do not have the luxury of waiting 18 months to prove value. Especially under value-based care, where financial performance is tied directly to clinical outcomes.
Mindbowser prioritizes CDS use cases that deliver measurable impact within months, not years.
1. Readmission risk, care gaps, and chronic disease pathways
These are high-impact, high-frequency use cases.
CDS helps by:
– Identifying patients at risk of readmission before discharge
– Highlighting care gaps in chronic conditions like diabetes or CHF
– Guiding standardized care pathways
What if clinicians could intervene before the risk becomes visible?
That is where CDS drives value.
Earlier intervention → Lower readmissions → Better margins
2. Prior authorization and documentation support
A significant portion of revenue leakage comes from:
– Incomplete documentation
– Missed coding opportunities
– Prior authorization delays
CDS can support clinicians in real time by:
– Suggesting documentation improvements
– Flagging missing elements tied to reimbursement
– Aligning orders with payer requirements
Every missed detail is a missed dollar.
This is where CDS directly impacts the bottom line.
3. Population health layers that translate insight into action
Many organizations already have analytics. What they lack is execution.
Mindbowser connects population health insights to point-of-care decisions by:
– Surfacing actionable insights during encounters
– Prioritizing high-risk cohorts
– Enabling proactive outreach workflows
Insight without action = no value
CDS closes that gap.
The fastest ROI comes from CDS use cases that intervene early, improve documentation, and translate data into action.
The Strategic Shift Leaders Cannot Ignore
The clinical decision support system is no longer an alert engine. It is becoming an orchestrated decision layer. Health systems that continue to treat CDS as a feature will fall behind those that treat it as a core capability tied to outcomes. The shift is clear: EHR-native integration, evidence transparency, operational governance, and ROI alignment are no longer optional. So what should leaders do now? Invest in CDS that fits clinical workflows, proves measurable impact, and evolves continuously with data and guidelines. Because in a value-based care environment, decisions are the product, and CDS is the system that shapes them. The winners will be those who use CDS to improve decisions in real time, not just document them.
A clinical decision support system helps clinicians make informed decisions using patient data, guidelines, and clinical logic. In 2026, it is evolving into an EHR-embedded, workflow-aware system that delivers real-time, evidence-backed recommendations.
An AI clinical decision support system uses machine learning and conversational interfaces to retrieve and summarize evidence. Unlike traditional CDS, it focuses on context-aware assistance and faster decision-making rather than static rule-based alerts.
Hospitals reduce alert fatigue by prioritizing high-confidence, context-aware alerts and eliminating unnecessary interruptions. Continuous tuning using override data and outcomes also improves relevance over time.
Leaders should evaluate workflow integration, evidence transparency, and measurable ROI. Strong interoperability, governance models, and security controls are also critical for long-term success.
Evidence-based clinical decision support improves consistency in care, reduces variation, and supports accurate documentation. This directly impacts quality metrics, cost control, and reimbursement under value-based care models.

