



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
Are your clinical insights actually influencing decisions, or just sitting in dashboards no one opens?
That is the uncomfortable question most healthcare apps avoid in a workflow where every second counts; even the best recommendations fail if they arrive too late or in the wrong place. This is where the cds hooks specification changes the game, by bringing real-time, context-aware guidance directly into the clinician’s moment of action, where it can finally drive outcomes instead of being ignored.
I. Why CDS Hooks Have Moved from Nice-to-Have to Strategic Requirement
A. The market problem healthcare apps still have not solved
Most healthcare apps fail at the exact moment they are needed. Not because the logic is wrong. Not because the data is missing. But the insight shows up in the wrong place.
Think about this: a clinician is reviewing a patient’s chart under time pressure. Would they open a separate dashboard to check recommendations? Almost never.
Clinical guidance today often lives outside the workflow. That creates friction. And friction kills adoption.
Here’s what happens in practice:
- * Clinicians switch tabs or systems to access insights
- * Decision-making slows down
- * Recommendations get ignored
Then comes the second issue. Custom integrations.
Every health system, every EHR, every workflow variation forces teams into building one-off integrations. These are expensive to maintain and hard to scale. What works for one client breaks for another.
And then there is alert fatigue.
Clinicians are already overwhelmed. Poorly timed or irrelevant alerts train them to ignore even the useful ones.
So the real problem is not a lack of decision support.
It is decision support that shows up too late, in the wrong place, or too often.
If your healthcare app does not integrate into the clinical workflow at the point of decision, it risks becoming invisible.
B. Why this matters more in value-based care
Value-based care changes the rules.
In fee-for-service, delays in insight might reduce efficiency. In value-based care, they directly impact revenue, quality scores, and patient outcomes.
What happens when a care gap is identified after the patient has already left? The opportunity is gone.
VBC depends on timely, context-aware interventions. Not reports. Not dashboards. Action.
Key pressure points include:
- * Preventive care gaps that go unaddressed
- * Medication risks that are not flagged at prescribing time
- * Referral inefficiencies that increase the cost of care
That is the shift.
Real-time guidance beats retrospective analytics. Every time.
Point-of-care nudges can:
- Trigger preventive screenings
- Suggest better medication options
- Guide referral decisions
- Close care gaps before they become costly
This is where most digital health products fall short. They generate insight. But they fail to activate it.
In value-based care, timing is not a feature. It is the product.
C. Why “just adding AI” does not solve the architecture problem
There is a growing assumption in healthcare product strategy:
“If we add AI, clinicians will use it.”
That assumption breaks quickly in real workflows.
AI can generate accurate predictions. It can surface risk scores. It can even recommend next-best actions.
But without the right delivery mechanism, it creates more friction than value.
Here is the reality:
- Insight without workflow placement slows clinicians down
- Intelligence without standards creates integration debt
- Recommendations without context reduce trust
This is not a model problem. It is an architecture problem.
Clinicians trust systems that:
- Deliver insights at the right moment
- Explain why a recommendation matters
- Fit naturally into their workflow
That is exactly what the CDS Hooks specification enables.
It provides a standards-based way to trigger decision support precisely when a clinical action is happening.
No extra clicks. No separate dashboards. No guesswork.
It connects intelligence to action.
AI tells you what to do. CDS Hooks ensures it shows up when it matters.
II. What the CDS Hooks Specification Actually Is
A. Plain-English definition
CDS Hooks is a way to deliver the right clinical insight at the exact moment a decision is being made.
At its core, the CDS Hooks Specification is an HL7 standard that allows healthcare systems to trigger decision support automatically during a clinician’s workflow.
No extra clicks. No switching systems. Just timely guidance.
Imagine this: a clinician is about to prescribe a medication. What if guidance appeared right then, based on that exact patient’s data? That is CDS Hooks in action.
It works by listening for specific workflow events inside an EHR. When that event happens, it calls an external service that returns relevant recommendations.
Key characteristics:
- Event-driven: triggers based on clinical actions, not schedules
- Context-aware: uses real patient and workflow data
- Non-disruptive: integrates directly into existing interfaces
- According to HL7, CDS Hooks is designed to “deliver decision support in real time, within the clinical workflow, without requiring users to leave their current system.”
This matters more than it sounds. Because the difference between “available insight” and “used insight” is workflow alignment.
CDS Hooks turns passive intelligence into active, in-the-moment guidance.
B. The core building blocks
To understand how CDS Hooks works, break it into a few simple components.
Each piece plays a specific role in delivering decision support at the right time.
1. CDS client
This is usually the EHR. It detects workflow events and triggers CDS Hooks.
2. CDS service
An external system that evaluates logic, rules, or models and returns recommendations.
This is where your product logic lives.
3. Hook
A defined event, such as:
- opening a patient’s chart
- prescribing medication
- signing an order
The hook determines when decision support is triggered.
4. Context
Data about the current workflow. For example:
- patient ID
- encounter details
- selected medication
This ensures recommendations are relevant.
5. Prefetch
Preloaded FHIR data is sent along with the request to reduce latency.
Faster response. Better experience.
6. Cards
The output is shown to the clinician.
These can include:
- Suggestions,
- warnings, actionable buttons
If the card is weak, adoption drops. This is where UX matters most.
7. SMART app launch
For deeper workflows, CDS Hooks can launch a SMART on FHIR app.
This allows:
- advanced interaction
- documentation support
- care plan workflows
CDS Hooks is not one feature. It is a coordinated system that connects workflow, data, and intelligence.
C. How CDS Hooks differs from related standards
Many teams confuse CDS Hooks with other interoperability approaches. That leads to poor architecture decisions early on.
Let’s clarify.
1. CDS Hooks vs SMART on FHIR
- CDS Hooks = triggers decision support
- SMART on FHIR = runs applications inside the EHR
One tells you when to act. The other gives you a place to act.
They are complementary, not competing.
2. CDS Hooks vs standalone CDS portals
Standalone portals require clinicians to leave their workflow.
That creates:
- low usage
- delayed decisions,
- fragmented care
CDS Hooks removes that barrier entirely.
3. CDS Hooks vs one-off API integrations
Custom APIs work, but they do not scale well.
Each new client means:
- new integration logic
- new maintenance overhead
- higher cost
The HL7 CDS Hooks Specification standardizes this pattern.
Build once. Reuse across environments.
4. Why CDS Hooks and SMART on FHIR are strongest together
This is where mature products stand out.
- CDS Hooks surfaces the insight
- SMART apps enable deeper workflows
Think of CDS Hooks as the trigger, and SMART as the engine.
The strongest healthcare apps do not choose between standards. They combine them strategically.
D. Common hooks healthcare product teams should know
Choosing the right hook determines whether your CDS logic succeeds or fails.
Here are the most commonly used ones:
1. patient-view
Triggered when a patient’s chart is opened.
Best for:
- care gaps
- risk scores
- population health insights
2. medication-prescribe
Triggered during prescribing.
Best for:
- drug interactions
- formulary checks
- cost optimization
3. order-select
Triggered when a clinician selects an order.
Useful for:
- duplicate checks
- guideline-based suggestions
4. order-sign
Triggered before finalizing orders.
Best for:
- compliance checks
- final validation alerts
Here is where many teams go wrong:
They either trigger too early or too late.
Too early → irrelevant alerts
Too late → missed opportunity to influence decisions
Precision matters more than volume.
The right hook at the right moment turns CDS from noise into action.
III. Why Your Healthcare App Needs the CDS Hooks Specification
A. It embeds decision support where clinicians already work
The fastest way to lose adoption is to ask clinicians to leave their workflow.
That is the reality most healthcare apps face.
A physician is reviewing a patient. Time is tight. Decisions stack up. Will they open another tool for guidance? Unlikely.
This is where the cds hooks specification changes the equation.
Instead of pulling users out, it brings decision support directly into theEHR workflow.
The impact is immediate:
- Fewer clicks
- Faster decisions
- Higher likelihood of action
That is not a small lift. That is the difference between usage and abandonment.
But it goes deeper.
When guidance appears at the right moment:
- It aligns with clinical intent
- It supports judgment instead of interrupting it
- It feels like assistance, not interference
This is how trust is built.
Short sentence. Matters.
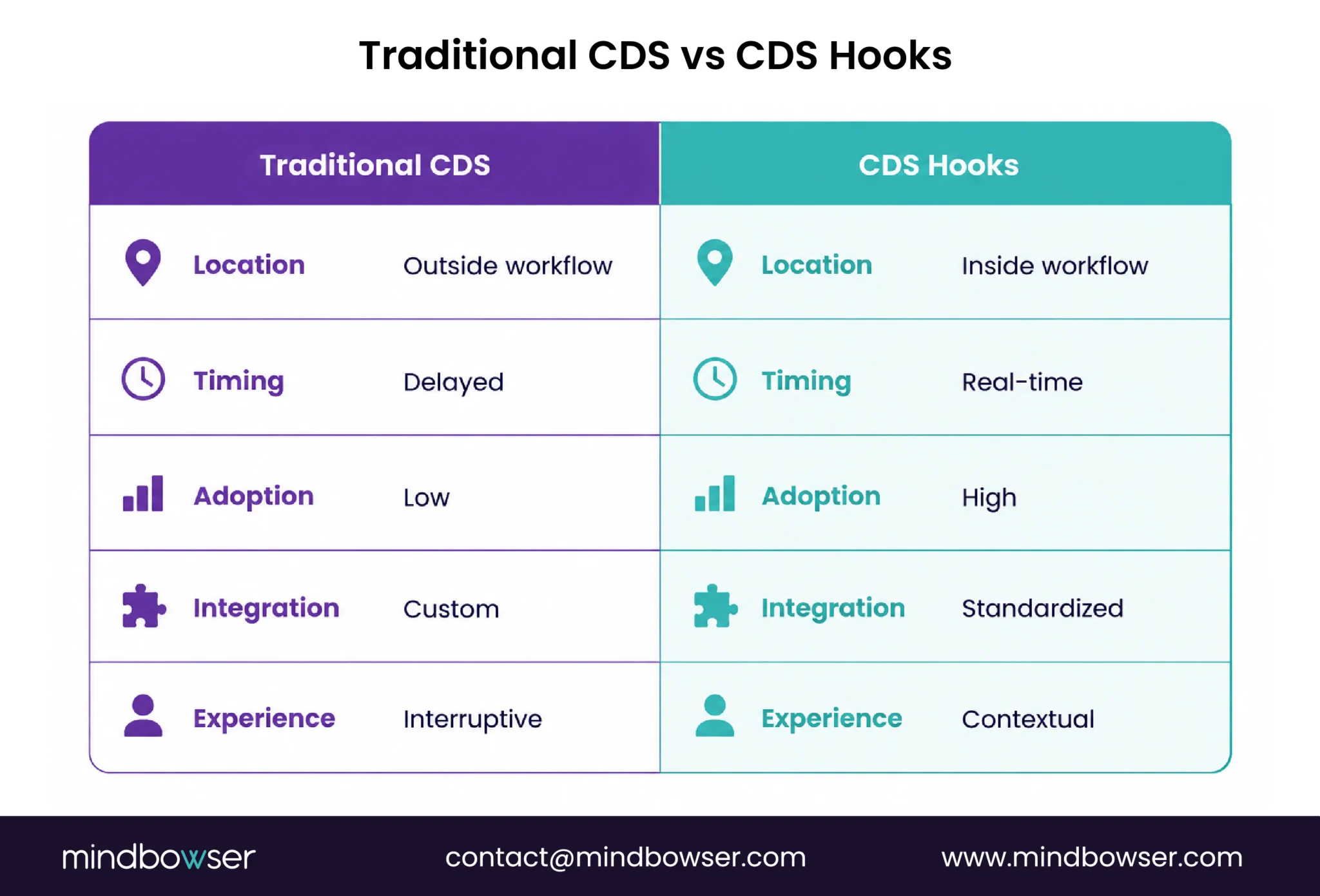
Contrast that with traditional CDS:
- Alerts fire too early or too late
- Context is missing
- Clinicians dismiss them reflexively
If your app is not inside the workflow, it is outside the decision.
B. It reduces integration complexity
Custom integrations are where good product strategies go to stall.
Every new client brings:
- Different EHR configurations
- Different workflows
- Different data access patterns
- This creates a cycle of rework.
How many times can your team rebuild the same logic for different environments before velocity drops?
The HL7 CDS Hooks Specification introduces a standardized trigger-response model.
That changes how teams build.
Instead of writing custom logic for each integration, you:
- Define hooks once
- Build reusable CDS services
- Apply consistent patterns across clients
This leads to:
- Lower engineering overhead
- Faster onboarding for new customers
- Predictable scaling across settings
In practice, teams that adopt standards like CDS Hooks reduce the need for one-off integrations and can reuse the same decision support services across multiple EHR environments, significantly lowering long-term integration effort.
That is not just technical efficiency. It is roadmap acceleration.
Less rework. More forward motion.
And there is a strategic upside.
Standardization makes your product:
- Easier to partner with
- Easier to extend
- Easier to sell to enterprise buyers
CDS Hooks replaces fragile, one-off integrations with a repeatable architecture.
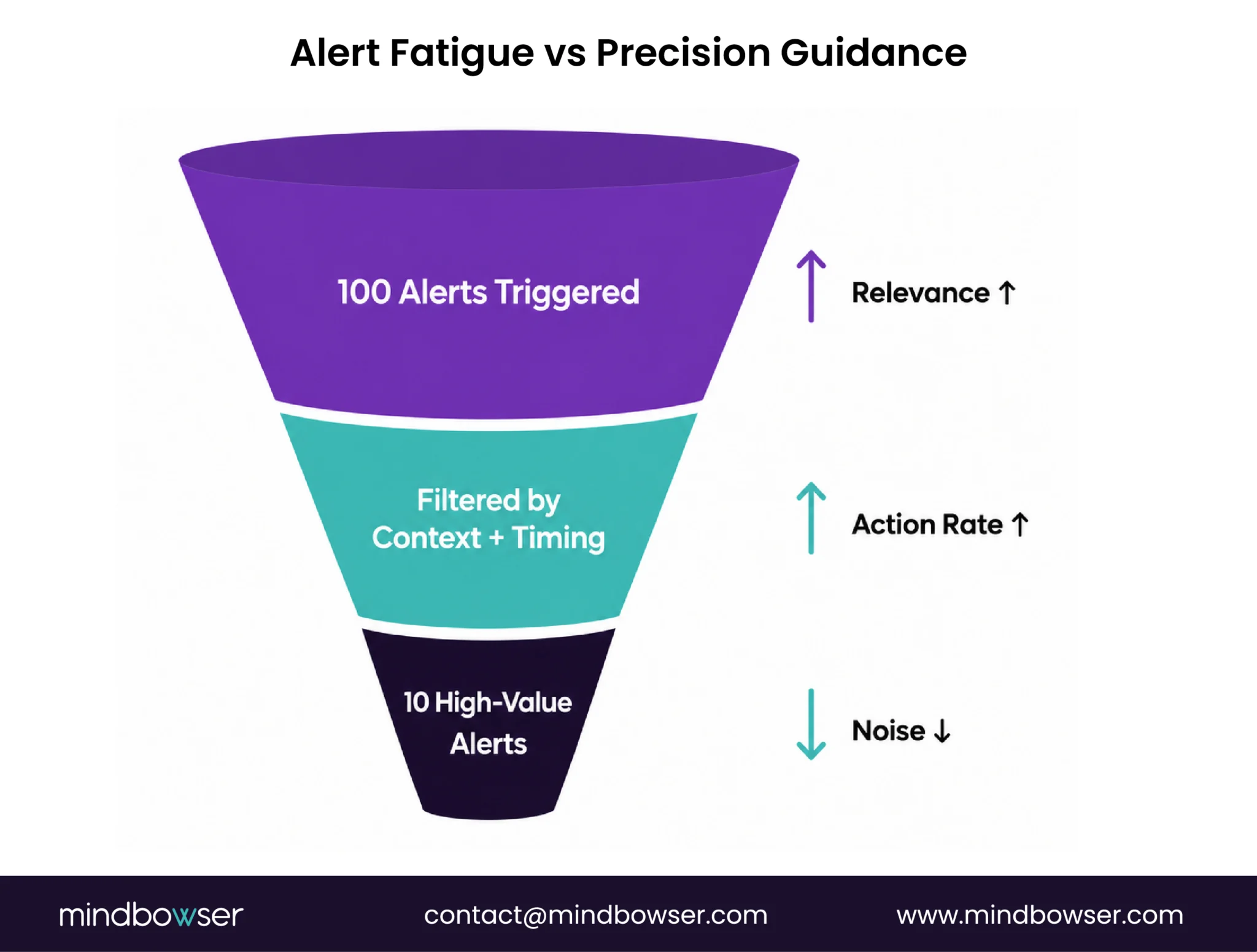
C. It improves relevance and can reduce alert fatigue
Alert fatigue is not about volume. It is about irrelevance.
Clinicians ignore alerts because they do not trust them.
What happens when a system fires ten alerts and only one is useful? The next ten get ignored.
The CD’s hooks specification addresses this by focusing on timing and context.
Key advantages:
- Triggers fire at meaningful clinical moments
- Context includes real patient and workflow data
- Prefetch reduces delays and improves responsiveness
This enables:
- Patient-specific recommendations
- Actionable suggestions instead of generic warnings
- Better alignment with clinical decision-making
The CDC highlights that improving relevance and timing can significantly reduce ignored alerts and improve patient safety outcomes.
But there is a design responsibility here.
Teams must:
- Limit unnecessary triggers
- Focus on high-value interventions
- Design clear, actionable cards
A vague alert is as bad as no alert.
Precision beats volume. Always.
When done right:
- Clinicians see fewer alerts
- But act on more of them
CDS Hooks helps shift from noisy alerts to meaningful guidance.
D. It creates a stronger foundation for VBC use cases
Value-based care demands actionable intelligence at the point of care.
Not reports. Not dashboards. Action.
CDS Hooks enables exactly that.
It activates use cases like:
- Risk-based recommendations: flag high-risk patients in real time
- Medication safety: suggest safer or cost-effective alternatives
- Care-gap closure: prompt screenings and preventive actions
- Referral optimization: guide network-efficient decisions
- Chronic disease workflows: support ongoing management
What changes when these insights appear during the encounter instead of after? Outcomes.
That is the margin. That is performance.
And importantly:
- These interventions become part of the workflow
- Not an extra task
This is how population health becomes point-of-care action.
Short. Clear.
CDS Hooks turns VBC strategy into executable workflows.
E. It future-proofs your product strategy
Healthcare IT is moving toward modular, interoperable systems.
Large, closed platforms are giving way to:
- API-driven architectures
- Standards-based integrations
- Composable ecosystems
The question is simple: will your product fit into that future?
The CDs hooks specification aligns directly with this shift.
It enables:
- Easier integration with EHRs and partner platforms
- Faster extension into new use cases
- Stronger positioning in enterprise evaluations
From a buyer’s perspective:
- CIOs want predictable integration
- CTOs want clean architecture
- CMIOs want workflow alignment
- CDS Hooks checks all three.
It also strengthens:
- Partner ecosystems
- Payer-provider collaborations
- Digital health platform integrations
This is not just a technical choice. It is a market positioning decision.
Products built on standards signal maturity. And maturity builds trust.
CDS Hooks prepares your product for where healthcare is going, not where it has been.
IV. How CDS Hooks Works in the Real World
A. A simple workflow example
CDS Hooks is simple in concept. The value comes from execution.
Let’s walk through a real-world scenario.
A clinician opens a patient chart during a routine visit. What happens behind the scenes?
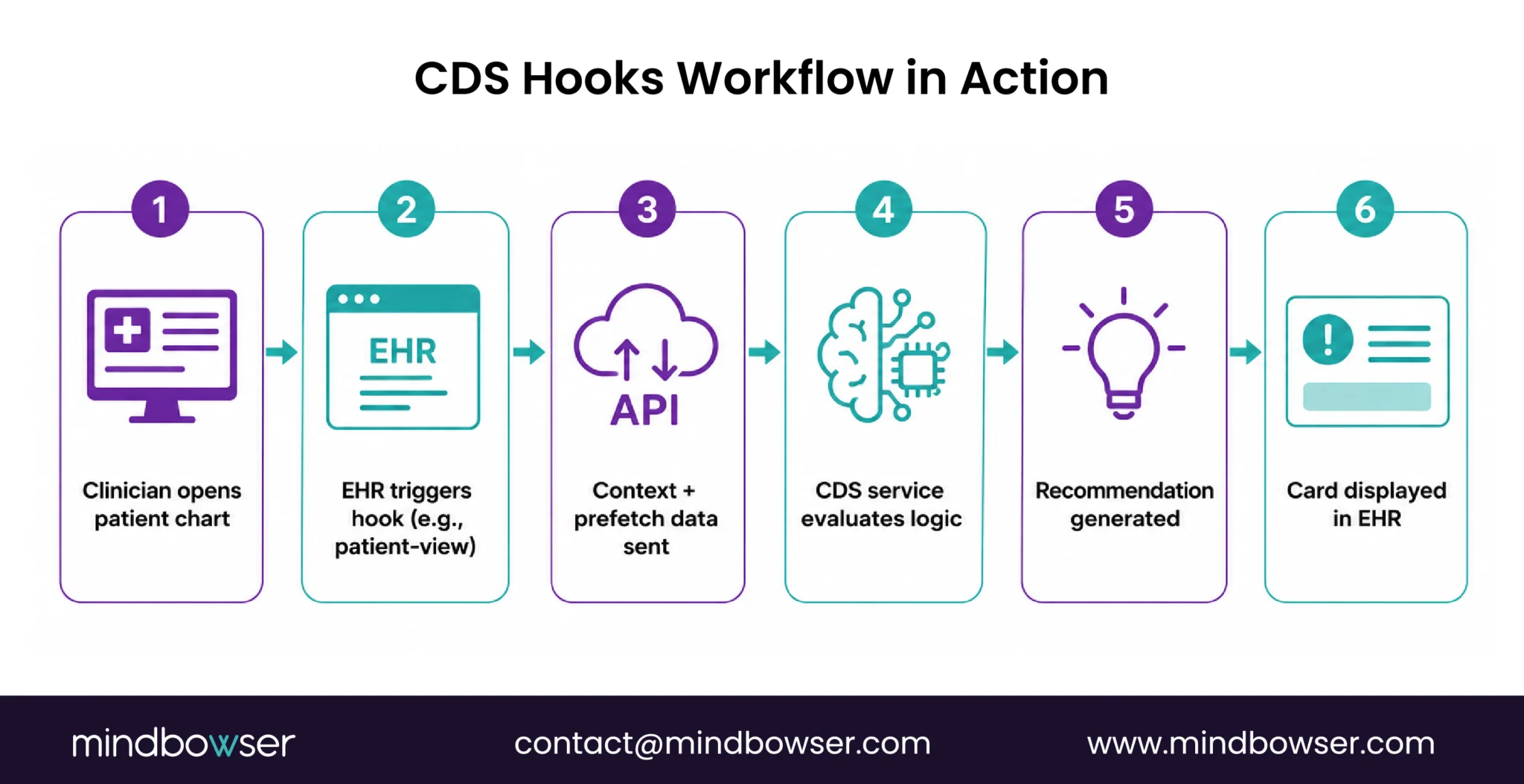
Here is the sequence:
- The clinician opens the chart
- The EHR detects this action and triggers a hook (e.g., patient-view)
- The EHR sends relevant context and prefetch data to a CDS service
- The CDS service evaluates rules, guidelines, or AI models
- The service returns a card with recommendations
- The EHR displays that card inside the workflow
All of this happens in seconds.
No disruption. No extra system.
The clinician sees guidance exactly when they need it.
Now consider the difference.
Without CDS Hooks:
- Insight lives in a dashboard
- Action requires manual lookup
- Timing is inconsistent
With CDS Hooks:
- Insight appears during the decision
- Action is immediate
- Workflow stays intact
This is where theory becomes practice.
CDS Hooks connects workflow events to real-time clinical intelligence.
B. Example use cases worth highlighting
The power of CDS Hooks comes from how it is applied.
Here are high-impact use cases healthcare leaders should pay attention to:
1. Medication safety check during prescribing
When a clinician prescribes medication:
- The system checks for drug interactions
- Flags contraindications
- Suggests safer alternatives
All before the prescription is finalized.
2. Lower-cost therapeutic alternative suggestion
During prescribing:
- The CDS service evaluates formulary data
- Recommends cost-effective options
This directly impacts patient affordability and adherence.
3. Gaps-in-care prompt for preventive screening
When viewing a patient:
- The system identifies missed screenings
- Prompts the clinician to act
According to CMS, closing preventive care gaps can significantly improve quality scores and reimbursement in VBC models.
4. Readmission risk or care-management referral trigger
For high-risk patients:
- CDS flags elevated readmission risk
- Suggests care management enrollment
This shifts intervention from reactive to proactive.
5. Prior authorization or documentation support prompt
Before order completion:
- The system surfaces documentation requirements
- Reduces claim denials
These are not theoretical use cases. They directly impact cost, quality, and operational efficiency.
CDS Hooks enables high-value interventions at the exact point they matter.
C. Where teams struggle during implementation
CDS Hooks is straightforward. Implementing it well is not.
Many teams underestimate the design and operational complexity.
Here are the most common failure points:
1. Choosing the wrong hook
Trigger too early → irrelevant guidance
Trigger too late → missed intervention
Timing defines usefulness.
2. Sending too much or too little context
Too little → weak recommendations
Too much → slower performance
Balance is critical.
3. Slow service response times
Clinicians will not wait.
If latency is high:
- Cards appear too late
- Trust drops
Deloitte notes that latency above a few hundred milliseconds significantly reduces clinician engagement with CDS tools.
Speed is part of the experience.
4. Weak card UX and unclear actions
A card that:
- Lacks clarity,
- has no clear next step,
- feels generic
- …will be ignored.
A good recommendation with poor UX still fails.
5. Governance gaps
Teams often overlook:
- Who owns clinical content
- How evidence is updated
- How overrides are tracked
Without governance:
- Quality degrades
- Risk increases
This is where many implementations stall.
CDS Hooks’ success depends as much on workflow design and governance as it does on technology.
V. What Healthcare Leaders Should Evaluate Before Implementing CDS Hooks
A. Product and workflow fit
CDS Hooks does not create value by default. It amplifies what is already well-designed.
That means the first question is not technical. It is strategic.
Where in your workflow does a decision actually need support?
Leaders should focus on four core questions:
1. Which workflow moment matters most
Not every step needs decision support.
Focus on:
- High-risk decisions
- High-cost actions
- High-variation workflows
Precision beats coverage.
2. Which users need the guidance
Different roles need different insights:
- Physicians → clinical recommendations
- Care managers → risk and follow-up actions
- Admin staff → documentation and authorization prompts
One-size guidance fails fast.
3. Which action should happen next
Every CDS interaction should answer:
“What should I do now?”
If the next step is unclear, adoption drops.
4. How success will be measured
Define metrics early:
- Action rate on CDS cards
- Workflow completion time
- Impact on quality measures
- Cost or utilization changes
No measurement, no impact.
Start with workflow clarity. Technology follows.
B. Technical readiness
Even the best use case fails without the right technical foundation.
The CDs hooks specification depends on a few key capabilities.
1. EHR compatibility and hook availability
Not all EHRs support the same hooks.
Evaluate:
- Which hooks are available
- How are they triggered
- Any vendor-specific limitations
2. FHIR maturity and data access patterns
CDS Hooks relies heavily on FHIR.
Key questions:
- Is patient data accessible in real time?
- Are the required resources available?
- Is the data normalized and usable?
Incomplete data leads to weak recommendations.
3. Security and authentication
Healthcare data demands strict controls.
Ensure:
- Secure API communication
- OAuth2-based authentication
- Compliance with HIPAA expectations
Trust starts with security.
4. Low-latency service design
Speed matters.
Your CDS service must:
- Respond within milliseconds
- Handle concurrent requests
- Scale without performance drops
- Slow systems get ignored.
5. Observability and feedback loops
You need visibility into:
- When hooks are triggered
- How cards perform
- Where failures occur
Deloitte reports that systems with strong observability improve reliability and adoption rates significantly.
You cannot improve what you cannot see.
Technical readiness determines whether CDS Hooks performs or frustrates.
C. Clinical and operational governance
This is where long-term success is decided.
Many organizations treat CDS as a one-time build. It is not. It is an evolving system.
Who owns the logic? Who updates the evidence? Who monitors performance?
Without clear answers, systems degrade quickly.
Key governance areas include:
1. Evidence source and maintenance
- Where do recommendations come from?
- How often are they updated?
Clinical credibility depends on this.
2. Escalation rules for warnings vs recommendations
Not every alert should interrupt.
Define:
- What is critical
- What is informational
Over-alerting erodes trust.
3. Clinical review process
Every CDS rule or model should be:
- Reviewed by clinicians
- Validated for accuracy
- Approved before deployment
4. Override capture and monitoring
When clinicians ignore recommendations:
- Capture the reason
- Analyze patterns
- Improve logic
Overrides are insight, not failure.
5. Measuring adoption and outcome impact
Track:
- Usage rates
- Action rates
- Clinical outcomes
This is not optional. It is foundational.
Governance turns CDS Hooks from a feature into a reliable clinical system.
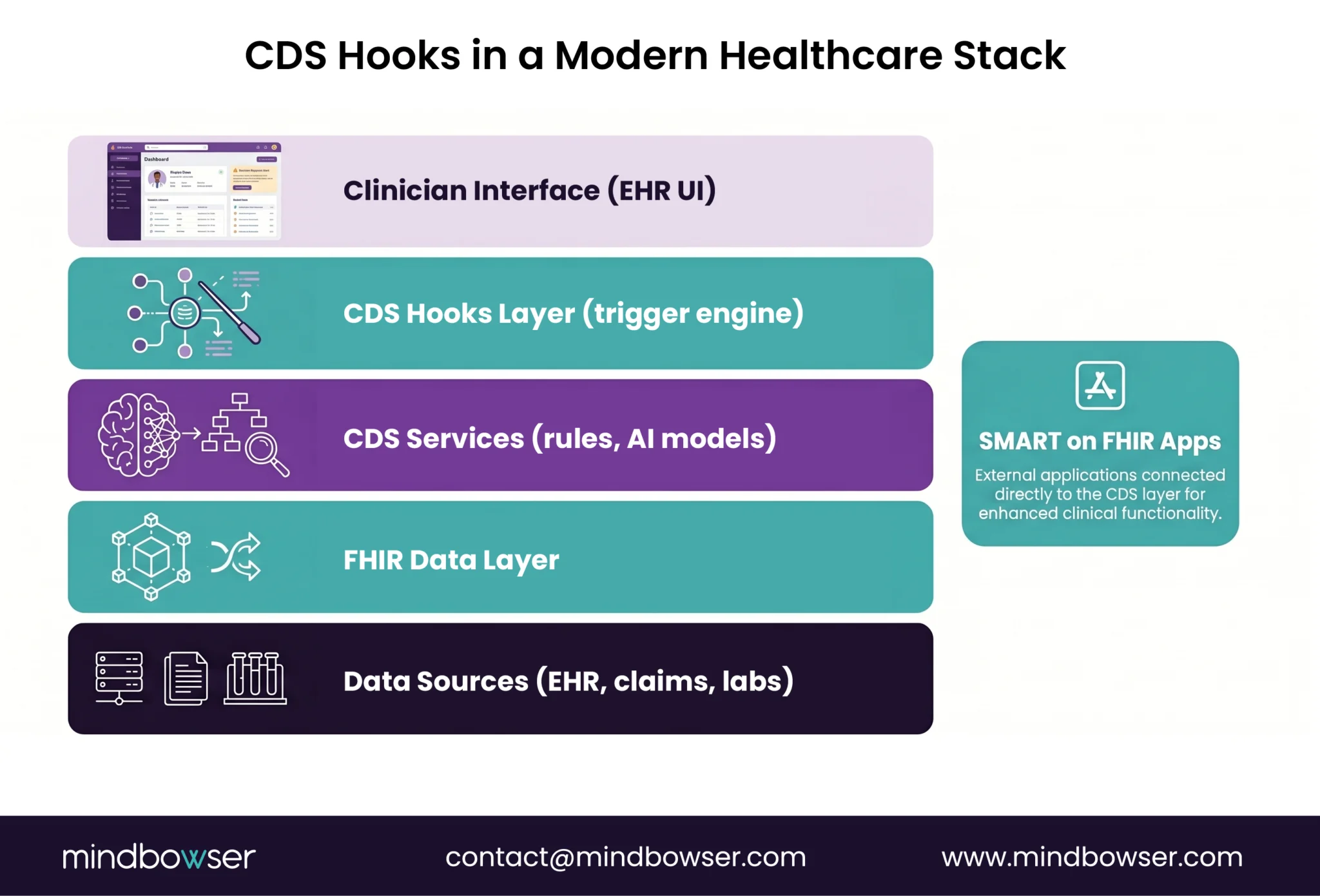
VI. Where CDS Hooks Fit in a Modern VBC and Digital Health Stack
A. For provider organizations
Provider organizations are under constant pressure to improve quality while controlling cost.
The challenge is not a lack of data. It is activating that data inside daily clinical workflows.
What happens when care teams have insights but cannot act on them during the visit? Performance gaps persist.
This is where the CDs hooks specification fits directly into the care delivery layer.
It enables:
- Real-time support for quality measures
- Consistent guidance across clinicians
- Workflow-aligned interventions without disruption
CDS Hooks helps standardize that consistency.
For example:
- A care gap alert appears during a visit, not after
- A medication recommendation aligns with the current patient context
- A referral suggestion supports network efficiency
This shifts organizations from reactive care to proactive intervention.
And importantly:
- Clinicians stay focused
- Workflow remains uninterrupted
CDS Hooks helps providers turn population health goals into point-of-care execution.
B. For digital health product companies
Digital health products live or die based on adoption.
You can have strong analytics, accurate models, and compelling dashboards. But if clinicians do not use them, the product stalls.
Why do many digital health tools struggle in enterprise sales cycles? Because they sit outside the workflow.
The HL7 CDS Hooks Specification changes how products integrate and how they are perceived.
It enables:
- Direct integration into EHR workflows
- Faster path to enterprise-grade interoperability
- Clear alignment with clinical operations
- This matters during sales.
Enterprise buyers evaluate:
- Integration effort
- Workflow disruption
- Clinical usability
Products built with CDS Hooks:
- Reduce integration concerns
- Demonstrate workflow alignment
- Signal architectural maturity
Deloitte notes that interoperability readiness is one of the top evaluation criteria for healthcare IT buyers.
This is not just technical. It is commercial.
It also supports:
- Easier partnerships with providers and payers
- Faster deployment across multiple clients
- More credible positioning in competitive deals
CDS Hooks strengthens both product architecture and market positioning.
C. For VBC-focused applications
Value-based care applications depend on timely action.
Risk scores, care pathways, and population analytics only matter if they influence decisions during care delivery.
What is the value of identifying a high-risk patient if no action is taken during the encounter?
CDS Hooks activates these insights.
Key applications include:
1. Risk stratification activation
Surface high-risk indicators during patient encounters and guide next steps.
2. Care pathway adherence
Prompt clinicians to follow evidence-based pathways in real time.
3. Network steering and referral quality
Guide referrals toward high-quality, cost-efficient providers.
4. Cost and quality improvement opportunities
Highlight actions that improve both clinical outcomes and financial performance.
McKinsey reports that embedding decision support into workflows can significantly improve adherence to care pathways and reduce variation.
This is where VBC strategy becomes operational reality.
Without CDS Hooks:
- Insights remain disconnected
- Actions are delayed
- Outcomes suffer
With CDS Hooks:
- Insights trigger action
- Action improves outcomes
- Outcomes drive value
CDS Hooks is the execution layer for value-based care applications.
VII. How Mindbowser Can Help
A. Strategy and discovery
Most teams start with technology. The smarter ones start with workflow.
Mindbowser helps you identify where CDS Hooks will actually drive action, not just where it can be implemented.
We focus on:
- High-impact workflow moments
- Clinical + product alignment
- VBC use cases tied to measurable ROI
Where does guidance change outcomes, not just inform decisions?
That clarity prevents wasted builds and accelerates value.
Start with the right use case, not just the right standard.
B. Architecture and implementation
CDS Hooks works best when designed for your environment, not forced into it.
Mindbowser builds secure, standards-aligned CDS Hooks architectures tailored to your EHR and FHIR setup.
Key focus areas:
- Low-latency CDS service design
- Clean hook selection and trigger logic
- SMART on FHIR integration for deeper workflows
We design for:
- Reliability
- Speed
- Clinical usability
A slow or poorly timed CDS system fails, no matter how good the logic is.
Architecture determines whether CDS Hooks scales or stalls.
C. Validation and scale
Initial deployment is only the starting point.
Sustained success depends on continuous tuning.
Mindbowser helps you:
- Refine card UX and timing
- Reduce unnecessary alerts
- Improve recommendation relevance
We also track:
- Adoption rates
- Response latency
- Clinical and business impact
This is how systems stay trusted.
CDS Hooks delivers value when it is measured, refined, and scaled.
The Moment Your Product Either Delivers or Disappears
Clinical insight only creates value when it shows up at the moment of decision. That is the dividing line between products that get used and those that get ignored. The CDs hooks specification gives healthcare apps a clear, standards-based way to deliver real-time, context-aware guidance inside the workflow where clinicians already operate. The question is no longer whether your app has intelligence, but whether that intelligence appears exactly when action is possible. In a value-based care environment, timing drives outcomes, outcomes drive revenue, and workflow drives adoption. If your product cannot meet clinicians in their moment of decision, it risks becoming invisible.
The CDS Hooks Specification is an HL7 standard that enables real-time clinical decision support within EHR workflows using event-based triggers.
CDS Hooks triggers recommendations during workflow events, while SMART on FHIR enables full applications to run inside the EHR.
It is related but separate. CDS Hooks uses FHIR data but is its own HL7 specification.
It improves adoption by delivering guidance at the point of care, reducing workflow disruption, and increasing action rates.
Yes. By triggering guidance at the right moment with relevant context, it reduces unnecessary or ignored alerts.

