



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
Alert fatigue in healthcare, particularly in Clinical Decision Support Systems (CDSS), occurs when excessive alerts overwhelm clinicians, leading to higher override rates, missed care gaps, and burnout.
To address this effectively, organizations must go beyond surface-level fixes and focus on structured approaches like workflow alignment, alert prioritization, and governance frameworks. A deeper breakdown of strategies can be found in this guide on reducing CDSS alert fatigue.
A 90-day roadmap can help identify problem alerts, redesign them, and track outcomes, improving clinician trust and reducing burnout.
Reducing alert fatigue CDSS issues requires workflow-aware alert design, structured override logic, and disciplined interruptive thresholds.
Watch: How CDSS Reduces Alert Fatigue
I. The Alert Fatigue Problem in Healthcare Is Now a Scaling Problem
A. What “Cdss Alert Fatigue” Actually Means In Day-to-day Care
A physician clicks “override” without reading. Again.
Not because they do not care. Because they cannot keep up.
That is CDSS alert fatigue in practice. It is not a technical issue. It is a behavioral shift created by overload.
At its core, CDSS alert fatigue happens when clinicians receive so many alerts that they begin to ignore them, even when some are clinically critical. The paradox is uncomfortable but real. The more alerts you add to improve safety, the greater the chance clinicians will tune them out.
As alert fatigue in healthcare continues to rise, clinicians are increasingly forced to prioritize speed over attention, leading to higher override rates.
Override rates for drug interaction alerts often exceed 85% in clinical settings.
In contrast, organizations implementing workflow-aligned CDS platforms have reported up to 87% provider engagement, demonstrating that alert fatigue can be significantly reduced.
Pause on that. If nearly 9 out of 10 alerts are ignored, what signal remains?
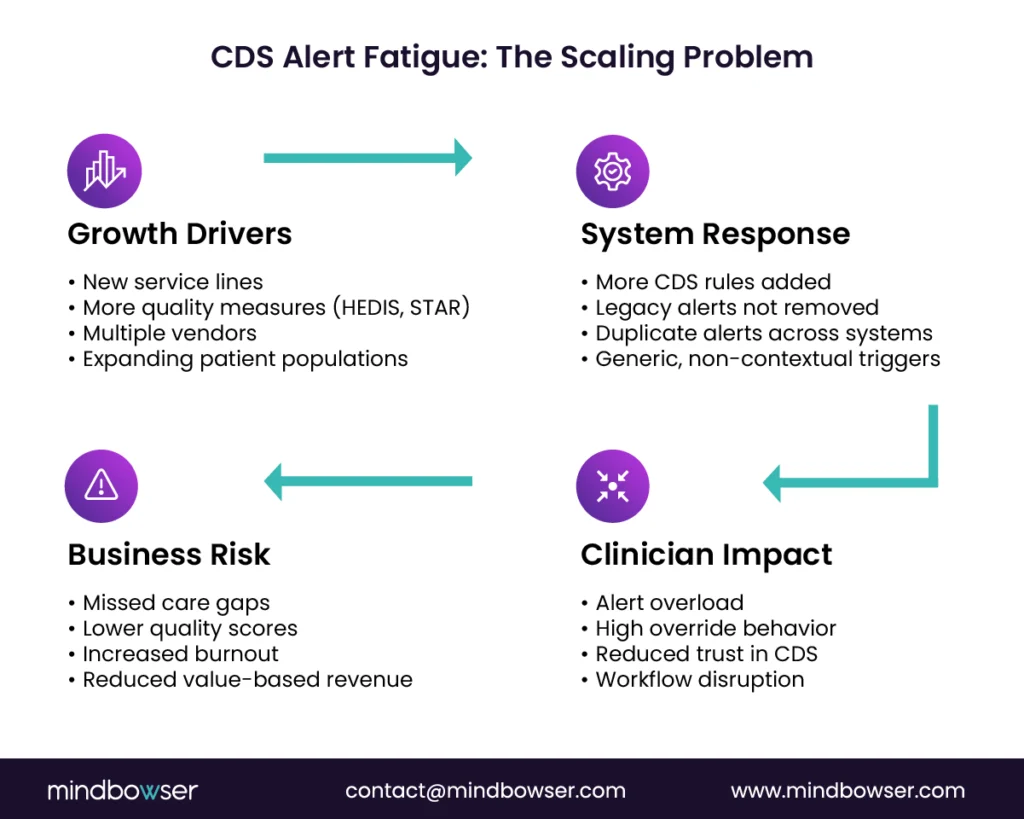
Now layer in scale. New service lines. New quality measures. New payer rules. New vendors. Each introduces additional rules into your clinical decision support system. None removes old ones.
What happens next?
A cardiologist managing value-based contracts sees 40 alerts per patient encounter. A primary care physician juggling HEDIS measures gets interrupted mid-documentation. A pharmacist receives duplicate alerts across systems.
This is not just noise. It is operational drag.
The downstream impact shows up where leaders care most:
- Missed care gaps that affect quality scores
- Lower clinician adoption of CDS tools
- Increased burnout and turnover risk
- Delayed time-to-action in critical decisions
“Clinicians spend nearly 50% of EHR time on administrative tasks, including alerts.”
That time is not neutral. It displaces clinical judgment.
For organizations moving into value-based care, the hidden cost compounds. Missed interventions. Lower STAR ratings. Reduced shared savings.
If you want a deeper look at how modern systems are evolving, this breakdown provides useful context.
Alert fatigue is not about too many alerts. It is about too many irrelevant interruptions at the wrong moment.
B. The enterprise pattern behind alert fatigue
Walk into any health system, and you will see a familiar pattern.
High-volume interruptive alerts dominate the workflow. Best Practice Advisories fire frequently. Medication alerts trigger regardless of context. Duplicate alerts appear across modules.
Individually, each alert makes sense. Together, they collapse into noise.
Consider this scenario. A hospital rolls out new sepsis protocols. Alerts are added for early warning scores, antibiotic timing, and lab triggers. At the same time, medication safety alerts continue unchanged. Preventive care reminders remain active.
No coordination. No prioritization.
Now the clinician sees:
- A drug-drug interaction alert
- A sepsis alert
- A vaccination reminder
- A documentation prompt
All within seconds.
Which one matters most?
The system does not help them decide. So they default to speed. Click. Override. Move on.
“When alerts lack specificity or clinical context, override rates increase significantly.”
This creates what many CMIOs describe as “checkbox medicine.” Clinicians respond to alerts to clear them, not because they trust them.
Trust erodes quietly. Then quickly.
Once lost, it is hard to rebuild.
Three signals of this enterprise pattern:
- Volume without hierarchy: Everything feels urgent, so nothing is
- Lack of context: Alerts do not reflect patient condition, setting, or role
- Duplication across systems: Same alert, different screens, repeated friction
The result is predictable. Alert fatigue becomes embedded in the culture.
C. Why this is a workflow problem, not a clinician problem
It is tempting to frame this as a training issue. Or a compliance issue.
It is not.
It is a workflow design failure.
Ask a simple question. When does the alert fire relative to the decision?
- Too early, and it gets ignored.
- Too late, and it becomes irrelevant.
- Too often, it becomes invisible.
Most clinical decision support system workflow designs break at this exact point.
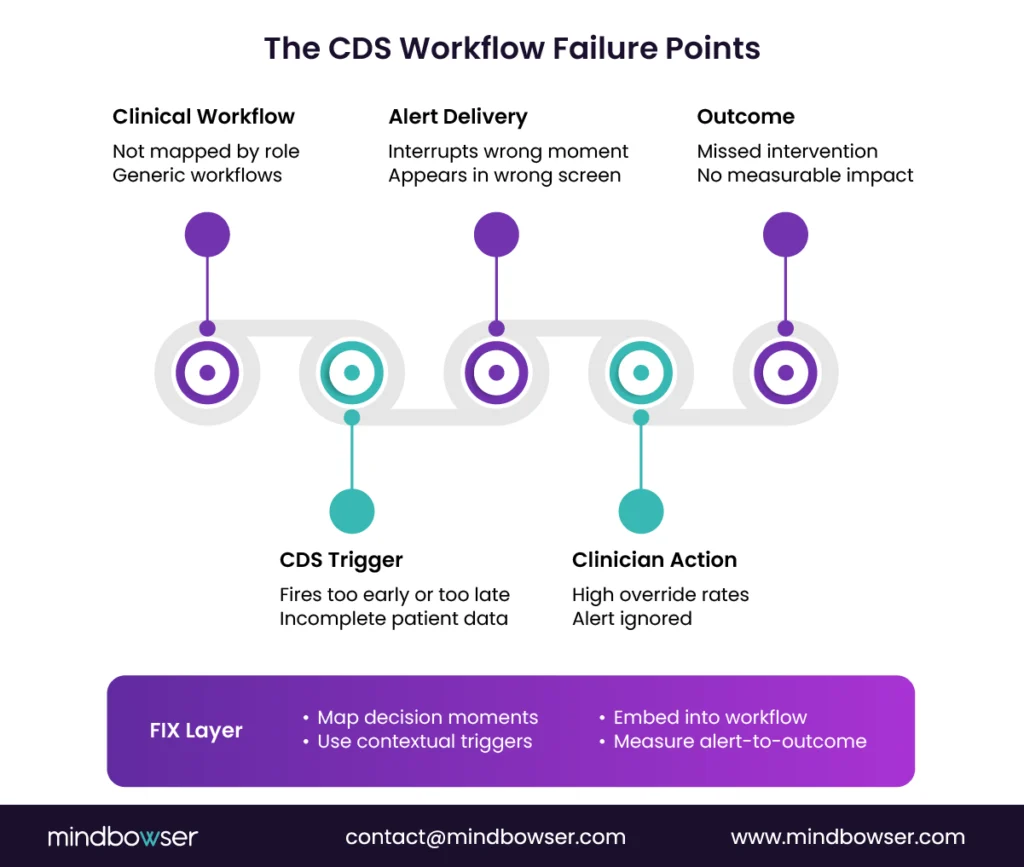
Common failure modes include:
- Alerts firing before sufficient patient data is available
- Interruptions during documentation instead of decision-making
- Alerts routed to the wrong role
- Poor data quality leading to false positives
- No ownership of alert lifecycle or performance
Imagine a pharmacist receiving a medication alert that should have been resolved upstream. Or a physician interrupted during note completion for a decision already made.
That is not clinician behavior. That is system design.
“Poorly designed CDS contributes directly to clinician burnout and reduced effectiveness. – National Academy of Medicine“
Here is the shift leaders need to make.
Stop asking: Why are clinicians ignoring alerts?
Start asking: Why are alerts interrupting at the wrong moment?
Because when CDS aligns with workflow, behavior changes naturally. Adoption rises. Overrides drop. Outcomes improve.
The path forward is not more alerts. It is a better orchestration.
Three levers define that shift:
- Governance that owns alert quality and lifecycle
- Workflow integration that respects clinical context
- Measurement that ties alerts to outcomes, not volume
We will unpack each in the next section.
Fix the workflow, and alert fatigue starts to resolve itself. Ignore it, and scaling makes the problem worse.
II. Design CDS That Clinicians Will Follow: Workflow-First, Tiered, Measured
A. Build the clinical decision support system workflow around the “moment of decision”
What if your most important alert shows up after the decision is already made?
It happens more often than most leaders realize.
The core mistake in many clinical decision support system workflow designs is timing. Alerts are triggered by data availability, not by clinical intent. That disconnect is where CDSS alert fatigue begins to compound.
Effective CDS starts with one question.
Where is the real moment of decision?
For a physician, it may be during order entry.
For a nurse, during triage or medication administration.
For a pharmacist, during verification.
Yet many systems fire alerts during documentation or chart navigation. The result is predictable. The alert feels irrelevant, even if its logic is sound.
“CDS interventions are significantly more effective when delivered at the point of decision rather than before or after.”
Leading organizations map these decision points explicitly by role. Not generically. Not by system module. By actual workflow behavior.
1. Map decisions by role, not system
A CMIO-led team should identify high-impact decisions across:
- Ordering workflows
- Medication reconciliation
- Discharge planning
- Preventive care gap closure
Then align CDS triggers to those exact steps.
2. Decide interruption versus guidance
Not every alert deserves to interrupt.
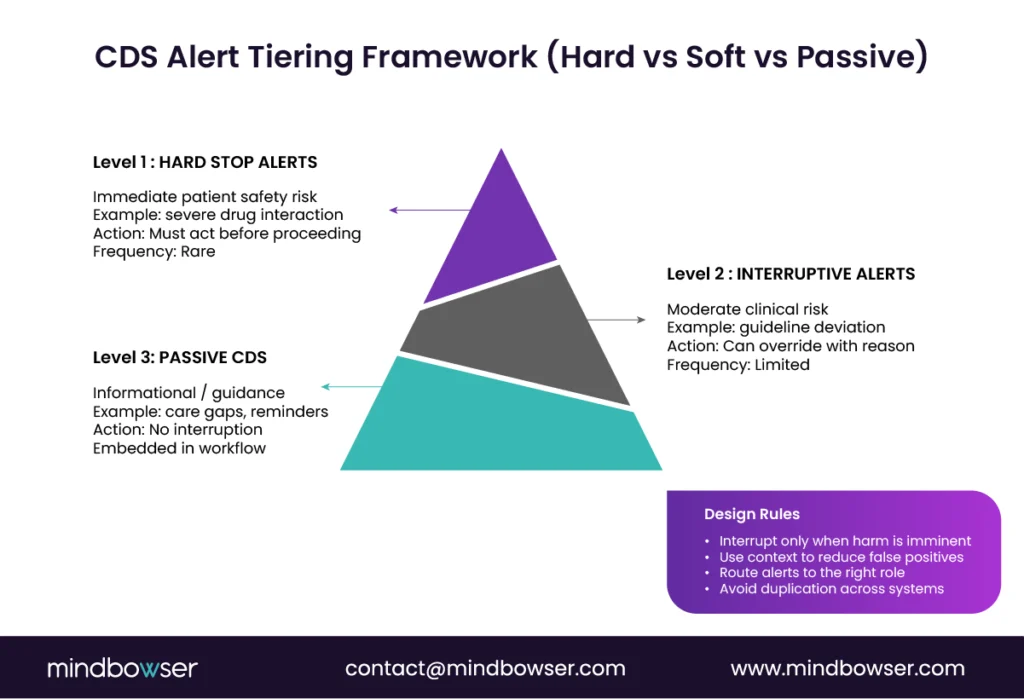
Interruptive alerts should be rare and reserved for high-severity, time-sensitive risks. Everything else should guide, not block.
Think of it this way:
- Interrupt only when harm is imminent
- Guide when improvement is possible
- Inform when awareness is enough
3. Embed CDS into existing screens
Clinicians should not have to leave their workflow to consume CDS.
Embedding guidance directly into order sets, documentation templates, and patient summaries reduces friction and improves adherence. No clicks. No pop-ups. Just context.
This works. Period.
If CDS is not aligned to the moment of decision, it will be ignored regardless of its clinical value.
B. How to integrate clinical decision support into workflow without creating noise
Do your alerts compete with the clinician’s attention, or support it?
This is where most systems fail quietly. They add more signals instead of improving relevance.
To integrate clinical decision support into the workflow effectively, the goal is simple. Reduce interruption. Increase precision.
Start by replacing interruptive alerts with passive CDS wherever possible.
Instead of a pop-up warning, present:
- Inline recommendations within order sets
- Risk scores embedded in patient summaries
- Care gap indicators are visible during chart review
These are not ignored because they do not interrupt. They assist.
“Passive CDS interventions often achieve higher adoption when embedded naturally into workflows.”
Next, use context aggressively.
A medication alert should consider:
- Patient age and comorbidities
- Care setting (ED vs inpatient vs outpatient)
- Current medication list and recent changes
Without this, alerts feel generic. And generic alerts are ignored.
Finally, route alerts to the right role.
A physician does not need every medication-level warning. Many can be routed to pharmacy workflows. Similarly, preventive care reminders may be more effective at the nursing or care coordinator level.
Three design shifts reduce noise immediately:
- From interruptive to passive, where possible
- From generic to context-aware triggers
- From physician-only to role-based routing
Integration is not about adding CDS everywhere. It is about placing the right signal in the right workflow at the right time.
C. Tiering, suppression, and de-duplication as an executive policy
If everything is urgent, nothing is.
This is where executive leadership must step in. Alert design cannot be left to individual teams or vendors. It requires policy-level control.
Tiering is the foundation.
Not all alerts carry the same risk. Yet many systems treat them equally.
A clear tiering model should define:
- High severity (hard stop): Immediate patient safety risk
- Medium severity (interruptive but overridable)
- Low severity (passive guidance)
Without this structure, clinicians face a flat hierarchy of interruptions.
Next comes suppression.
Repeated alerts within the same encounter quickly create fatigue. If a clinician has already acknowledged an alert, it should not reappear unless conditions change.
De-duplication is equally critical.
The same alert firing across multiple systems or modules erodes trust: one signal, one place, one time.
Reducing duplicate and low-value alerts can significantly improve clinician adherence to high-priority CDS.
Finally, establish sunset rules.
Every alert should have an owner, a review date, and a measurable outcome. If it no longer adds value, it should be retired.
Executive takeaway:
- Tier alerts by severity
- Suppress unnecessary repetition
- Eliminate duplicates across systems
- Enforce lifecycle management
Alert quality is not a build problem. It is a governance policy decision.
D. Measure what matters so improvement does not turn into opinion wars
If two leaders disagree about the effectiveness of CDS, who is right?
The one with data.
Without measurement, CDS optimization becomes subjective. One team argues for more alerts. Another pushes for fewer. Clinicians push back. Nothing changes.
The solution is to define and track the right metrics.
Start with alert burden.
- Alerts per encounter
- Interruptive alerts per clinician per shift
- Alert distribution by role
Then move to behavior.
- Override rates by alert type
- Acceptance rates
- Time-to-action after alert
High override rates often indicate poor alert relevance rather than clinician non-compliance.
Finally, connect alerts to outcomes.
This is where executive value becomes clear.
- Did the alert reduce adverse drug events?
- Did it improve the performance of the quality measure?
- Did it close care gaps faster?
Without this linkage, CDS remains a cost center. With it, CDS becomes a performance driver.
Governance dashboards should make this visible at an enterprise level. Not buried in reports. Not delayed by months.
Real-time or near-real-time visibility allows teams to adjust quickly.
For leaders, this is the shift from activity to impact.
Measure alerts the same way you measure revenue cycle or quality metrics. Because they directly influence both.
Ready to Reduce Alert Fatigue and Scale Clinical Decision Support That Works?
III. Reduce Risk While Scaling: Governance, Safety, and the Real Costs of Overrides
A. The risks of bypassing CDSS alerts (and why leaders should care)
What happens when the one alert that matters gets ignored?
Not hypothetically. In your system. Today.
This is where CDSS alert fatigue stops being an efficiency issue and becomes a patient safety risk.
When override behavior becomes normalized, clinicians stop evaluating alerts individually. They respond based on pattern recognition. Click through. Move on.
“Studies show override rates for high-severity alerts can still exceed 50%, raising safety concerns.”
That number should concern every CMIO and CMO.
Because not all overrides are wrong, but an unmanaged override culture is dangerous.
Consider the variation:
- Emergency department clinicians override alerts differently from inpatient teams
- Specialists respond differently from primary care physicians
- Night shifts behave differently from day shifts
Without visibility, this variation goes unnoticed.
Now layer in risk.
A drug-drug interaction alert is ignored. A contraindicated medication is administered. An adverse event follows. The root cause analysis points back to the CDS alert.
But here is the uncomfortable truth.
The alert did not fail. The system around it did.
“An alert ignored once becomes an alert ignored forever.”
The risks of bypassing CDSS alerts include:
- Increased adverse drug events
- Delayed interventions in critical conditions
- Missed preventive care opportunities
- Legal and compliance exposure
For value-based organizations, the impact extends further.
- Lower quality scores
- Financial penalties
- Reduced shared savings
Overrides are not just clicks. They are signals of system failure that leaders must actively manage.
B. Governance is the scaling mechanism
Who owns your alerts today?
If the answer is unclear, that is the problem.
Scaling CDS without governance is like scaling clinical operations without protocols. It creates variation, inconsistency, and risk.
A formal CDS governance model serves as the control layer that helps prevent alert fatigue while preserving safety.
At the center is a multidisciplinary governance council.
This is not an IT-only function. It must include:
- CMIO or clinical leadership
- Pharmacy leadership
- Nursing representation
- Quality and safety teams
- Informatics and IT
Their mandate is simple. Own the lifecycle of every alert.
1. Define a clear change control model
Every new alert should answer:
- What problem does this solve?
- Who is the target user?
- What is the expected outcome?
- How will success be measured?
No clear answer. No deployment.
2. Standardize enterprise patterns
Consistency matters.
Define standards for:
- Alert tiering
- Trigger logic
- Display format
- Override reasons
This reduces cognitive load and improves trust.
3. Assign ownership and accountability
Every alert should have:
A clinical owner
A review cadence
A performance baseline
If no one owns it, it will not improve.
Governance is not bureaucracy. It is enablement.
It allows systems to scale without collapsing under their own complexity.
You cannot scale CDS safely without governance in place. It is the operating system behind every effective program.
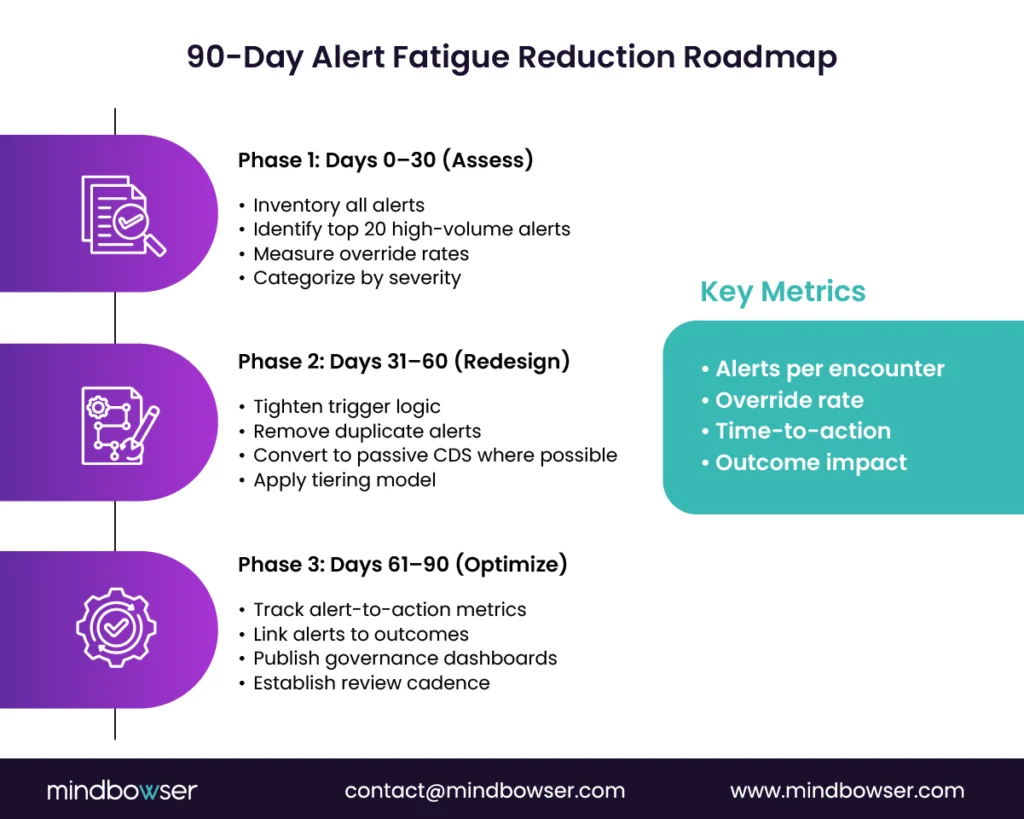
C. A practical roadmap to cut alert burden in 90 days, then keep improving
Can you reduce alert fatigue in 90 days?
Yes. If you focus.
Not by rebuilding everything. By targeting what matters most.
This is the playbook many high-performing organizations follow.
1. First 30 days
Start with visibility.
- Inventory all active alerts across systems
- Categorize by volume, severity, and override rate
- Identify the top 20 alerts contributing to alert burden
Most organizations find that a small subset of alerts drives the majority of fatigue.
This is your leverage point.
2. Days 31-60
Now redesign.
- Tighten trigger logic using patient context
- Remove or suppress duplicate alerts
- Reclassify alerts based on severity tiering
- Shift low-value interruptive alerts to passive CDS
This is where quick wins happen.
Clinicians feel the difference almost immediately.
3. Days 61-90
Link changes to outcomes.
- Track changes in override rates
- Measure alert-to-action improvements
- Monitor impact on safety and quality metrics
Then publish scorecards.
Transparency drives accountability. And momentum.
Finally, establish a quarterly review cadence.
Because CDS is not a one-time project. It is a continuous product.
You do not need a year-long transformation to reduce alert fatigue. You need focus, governance, and measurable action.
IV. How Mindbowser Can Help
A. CDS optimization and workflow engineering for VBC scale
What if your CDS worked the way your clinicians actually practice?
Not how the system was configured years ago. Not how a vendor template assumed.
That is where most organizations are stuck.
They inherit a clinical decision support system that was built incrementally. New alerts added. Old ones are rarely removed. Workflow assumptions never revisited.
Mindbowser approaches CDS as a product, not a configuration.
We start with workflow mapping workshops led by clinical and informatics stakeholders. Not theoretical flows. Real-world behavior across roles, settings, and decision points.
This includes:
- Mapping high-impact clinical decisions by role
- Identifying where alerts interrupt versus assist
- Quantifying alert burden and override patterns
From there, we design a workflow-first CDS model.
No more alerts. Better placement. Better timing. Better targeting.
Then we operationalize governance.
Many organizations know they need governance. Few have an operating model that works at scale.
We help establish:
- CDS governance councils with defined ownership
- Alert lifecycle management frameworks
- Tiering, suppression, and review protocols
- Outcome-linked measurement models
This is where systems shift from reactive cleanup to proactive control.
And yes, speed matters.
Using accelerators aligned to HIPAA and SOC 2 design principles, teams can implement these changes faster without compromising compliance or control.
Workflow-first CDS design paired with governance is how you scale safely and sustain value-based outcomes.
B. Interoperability and data quality foundation
If your data is wrong, your alerts will be wrong.
Simple. But often overlooked.
Logic flaws do not cause many cases of CDSS alert fatigue. They are caused by poor data quality and fragmented interoperability.
An alert fires because a medication list is outdated.
A risk score is triggered when the lab data are incomplete.
A preventive care alert appears because external data was not reconciled.
Clinicians notice. Trust drops.
To fix this, CDS must be built on a reliable data foundation.
Mindbowser focuses on strengthening:
- Real-time data integration across EHRs, labs, and external systems
- Accurate medication and problem list reconciliation
- Context-aware data ingestion using standards like FHIR and CDS Hooks
This reduces false positives. And false positives are a primary driver of alert fatigue.
“Improving data quality significantly reduces unnecessary alerts and increases clinician trust in CDS. –ONC “
We also design CDS triggers that account for data variability.
Instead of firing alerts based on incomplete inputs, systems can:
- Delay triggers until sufficient data is available
- Adjust logic based on confidence levels
- Suppress alerts when data gaps are detected
This is how CDS becomes reliable.
Better data leads to fewer, more accurate alerts. And accurate alerts are the foundation of clinician trust.
C. Digital health build and modernization for CDS at scale
Can your current CDS architecture support where you are headed?
Value-based care. Multi-system integration. AI-assisted workflows.
If not, alert fatigue will keep returning.
Modern CDS requires more than rule tuning. It requires architectural evolution.
Mindbowser supports digital health teams in building CDS capabilities that scale with organizational growth.
This includes:
- Non-interruptive CDS patterns embedded directly into workflows
- Smart order sets that guide decisions without pop-ups
- Context-aware recommendations using patient-specific data
- Analytics frameworks that link CDS activity to outcomes
We also support modernization through interoperable architectures using CDS Hooks and FHIR.
This allows CDS to operate across systems rather than just within a single EHR.
And importantly, it enables continuous improvement.
Because CDS should not be static.
It should learn from:
- Clinician behavior
- Outcome data
- Workflow changes
And evolve accordingly.
This is where many organizations see a step-change in performance.
From reactive alert management to proactive decision support.
Scaling CDS requires modern architecture, not just better rules. Build for adaptability, and alert fatigue becomes manageable.
D. CDS at Scale: Fix the Design, Not the Clinician
CDSS alert fatigue is not a user problem. It is a system design signal. When alerts grow without workflow alignment, governance, and measurement, clinicians adapt by ignoring them. The fix is not fewer alerts, but better-timed, role-aware, outcome-driven decision support. Organizations that treat CDS as a product and consistently follow a clear workflow, tiering, governance, and measurement model consistently reduce fatigue while improving safety and value-based performance. Design CDS to fit clinical reality, and adoption follows
Designing CDS for Better Outcomes and Reduced Alert Fatigue
Alert fatigue in CDSS is a predictable outcome of poor system design. By aligning alerts with workflow, implementing tiering, and ensuring strong governance, healthcare organizations can reduce fatigue while improving safety and clinician satisfaction. A structured 90-day roadmap can help prioritize and redesign alerts for better outcomes, driving long-term success in clinical decision support.
Reducing alert fatigue in healthcare requires a shift toward workflow-aligned, context-aware CDS design supported by governance and continuous measurement.
CDSS alert fatigue occurs when clinicians receive too many or poorly timed alerts, leading them to override or ignore them. Over time, this reduces trust in the system and increases the risk of missing critical warnings. It is both a workflow and a patient safety issue.
The best clinical decision support system workflow aligns alerts with the exact moment of decision-making and tailors them by role. It minimizes interruptions, embeds guidance into existing screens, and uses tiering to prioritize high-risk alerts. This improves adoption and reduces unnecessary overrides.
You reduce pop-ups by shifting from interruptive alerts to passive, embedded CDS within workflows. Use patient context and route alerts to the right roles to improve relevance. This keeps clinicians informed without disrupting their flow.
Bypassing CDSS alerts can lead to adverse drug events, missed diagnoses, and gaps in care. Over time, it creates a culture where even critical alerts are ignored. This increases both safety risks and compliance exposure.
Track alert volume, interruptive alerts per user, and override rates to measure fatigue. Pair these with outcome metrics like reduced adverse events and improved quality scores. Linking alerts to outcomes proves real value.
Interruptive alerts should be reserved for high-risk situations requiring immediate action. Passive CDS should handle all other guidance within the workflow. This balance reduces fatigue while maintaining safety.
Alert fatigue in healthcare occurs when clinicians are exposed to excessive clinical decision support alerts, causing them to ignore or override even critical warnings.
Common causes include high alert volume, poor timing, lack of clinical context, duplicate alerts, and poorly aligned clinical workflows.
Alert fatigue can be reduced by implementing workflow-aligned CDS, alert tiering, suppression of duplicate alerts, context-aware triggers, and strong governance frameworks.
Replace free-text override boxes with a fixed list of 5 to 10 structured codes. Examples: “clinically appropriate,” “patient already on combination,” “monitoring planned,” “alternative not available,” “low risk for this patient,” “deferred to pharmacist,” “other (free text required).” Structured codes generate tunable data: which codes get selected, on which alerts, by which clinicians. That data drives quarterly alert retirement and re-tiering. Free-text boxes generate noise that cannot be analyzed at scale. A perioperative-readiness deployment we shipped iterated from 12 codes to 7 after pilot data showed which codes never got selected, and override-rate trend improved over the next two quarters.
![5 Types of Clinical Decision Support Systems: Which One Fits Your Hospital? [2026]](https://www.mindbowser.com/wp-content/uploads/2026/03/medical-technology-network-telemedicine-health-insurance-virtual-hospital-healthcare-1024x585.jpg.webp)

