



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
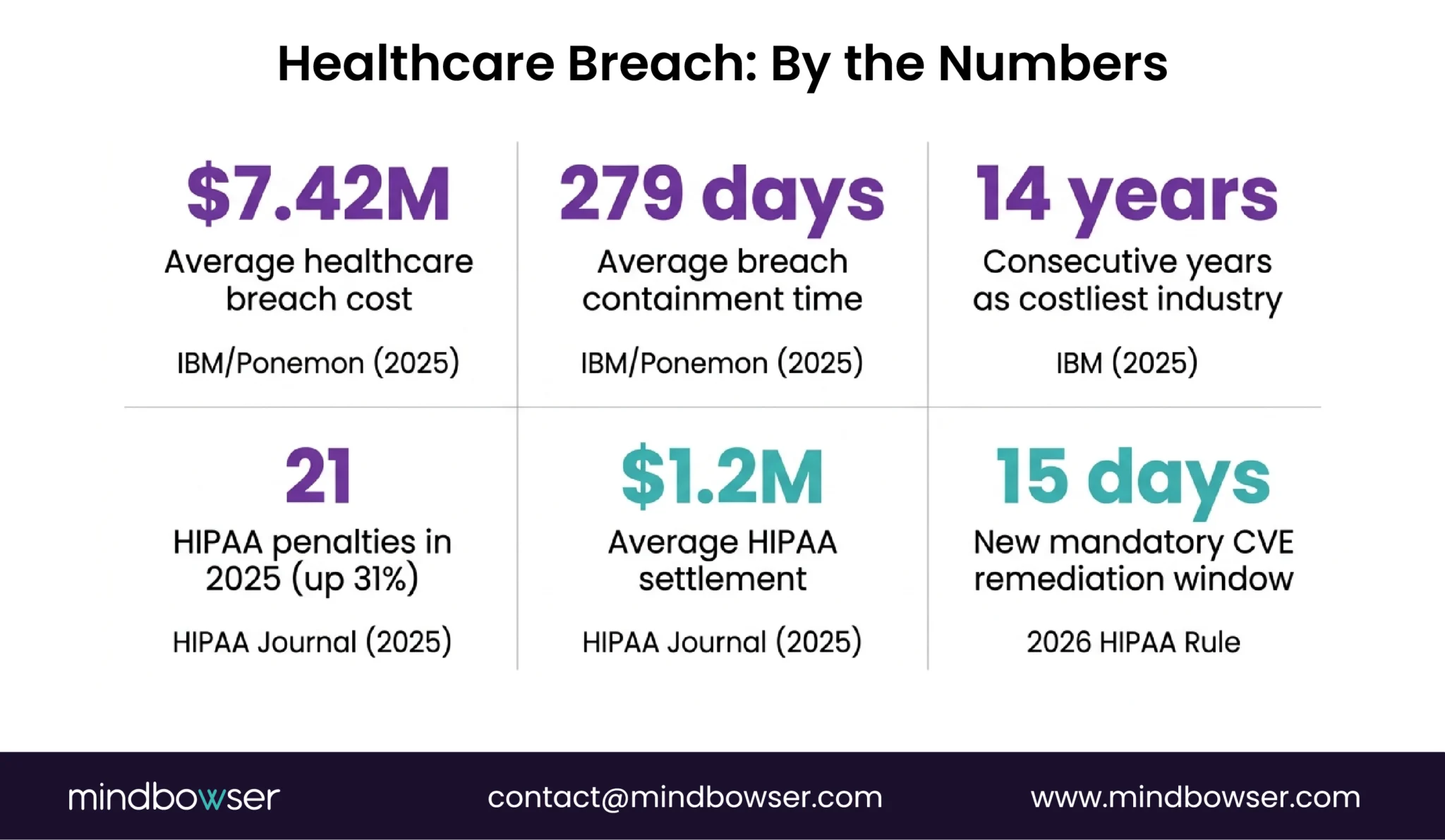
The average healthcare data breach costs $7.42 million (IBM/Ponemon, 2025). The 2026 HIPAA Security Rule update is eliminating “addressable” specs – controls that were optional are becoming mandatory. If you’re building a custom EHR, security can’t be a layer you add after development. It has to be the foundation. This guide covers the 6 security architecture layers, HIPAA/SOC 2/HITRUST compliance paths, and what the 2026 rule changes mean for custom EHR builders.
$7.42 million. That’s the average cost of a healthcare data breach in 2025 – and healthcare has been the costliest industry for breaches 14 years running. Containment takes 279 days on average – 5 weeks longer than any other sector.
Now add this: HHS is finalizing major updates to the HIPAA Security Rule, targeted for May 2026, that eliminate many “addressable” implementation specs. Controls that were previously flexible are becoming mandatory. MFA for all remote ePHI access. AES-256 encryption at rest with no exceptions. Critical vulnerability remediation within 15 calendar days.
If you’re building a custom EHR, the security conversation isn’t “should we do this.” It’s “can we ship if we don’t?”
I. Why is EHR Security Different from General Application Security?
If you’ve secured a SaaS application or an e-commerce platform, you might think EHR security is the same problem with HIPAA paperwork on top. It’s not. Four things make it fundamentally different:
- PHI classification changes everything. Every data element in an EHR is potentially Protected Health Information. HIPAA’s “minimum necessary” rule means your access controls can’t just be role-based – they need to restrict data to the minimum required for each user’s function. A billing clerk sees billing data. A nurse sees clinical data. A behavioral health therapist sees therapy notes that are segmented under 42 CFR Part 2 from the rest of the record.
- Breach notification is legally mandated. Within 60 days of discovering a breach affecting 500+ individuals, you must notify HHS, affected patients, and prominent media outlets. There’s no “we’ll disclose when we’re ready.” The clock starts at discovery.
- The penalty structure has teeth. Average HIPAA settlement in 2025: $1.2 million. 21 penalties imposed in 2025, up 31% from 2024. And the 2026 rule changes will make more controls mandatory – expanding the surface area for enforcement actions.
- Healthcare takes the longest to detect breaches. 279 days average (IBM, 2025). That’s 9 months of exposed PHI before you even know something’s wrong. Your security architecture needs to prevent breaches AND detect them faster than the industry average.
The 2026 rule change to watch: HHS is eliminating the distinction between “required” and “addressable” implementation specifications under 45 CFR Part 164. What this means in practice: controls like encryption, MFA, and audit logging that organizations could previously skip with documented justification are becoming mandatory with no exception. Estimated finalization: May 2026. Compliance deadline: likely late 2026 or early 2027 (180-day window).
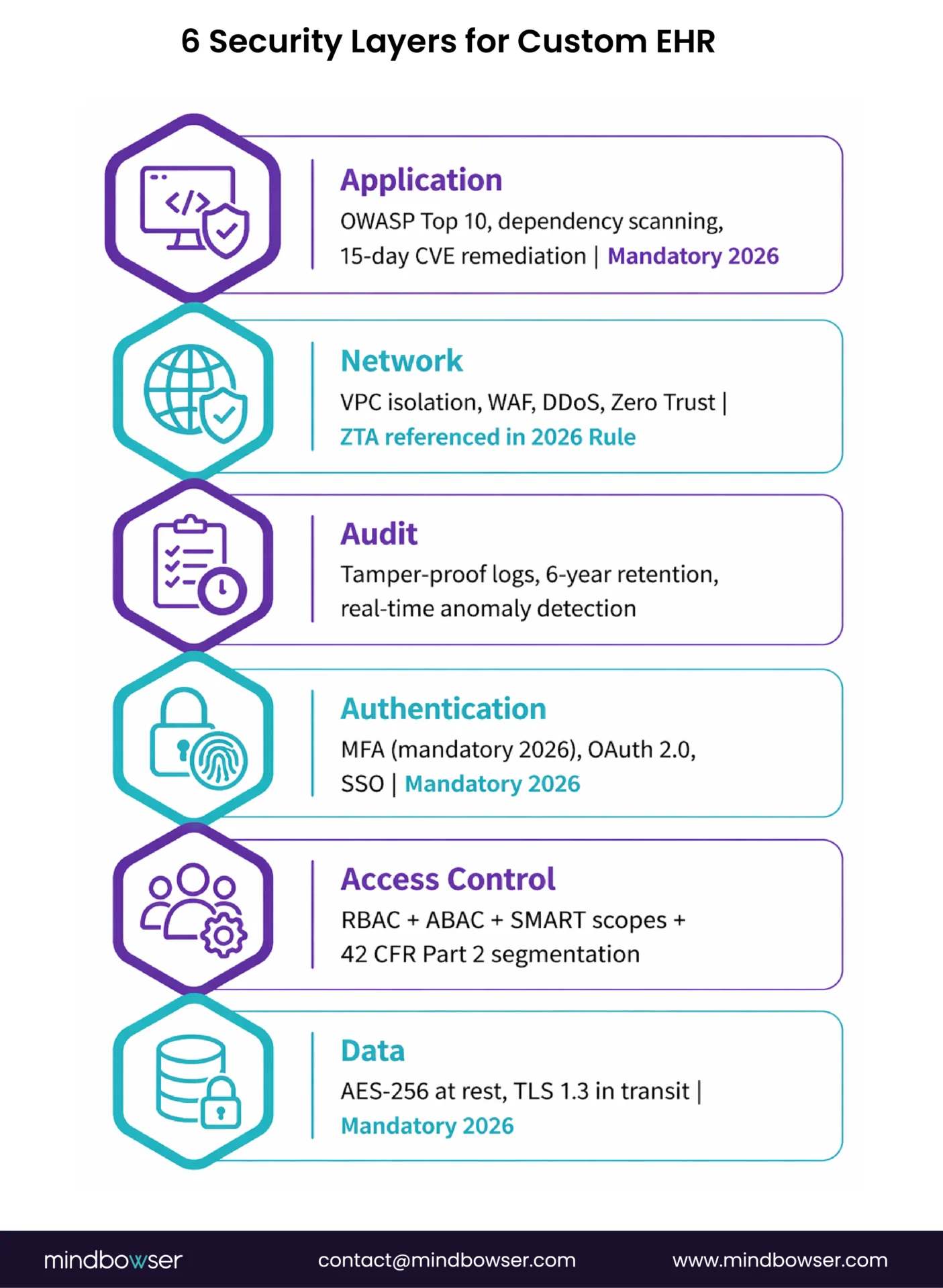
II. What Are the 6 Security Architecture Layers for Custom EHR?
Every custom EHR needs six layers. Skip one, and you’ll find out during a penetration test, an audit, or a breach.
A. Layer 1: Data Layer (Encryption)
- At rest: AES-256 minimum. Database-level encryption. Full-disk encryption on all endpoints. Encrypted backup storage.
- In transit: TLS 1.2+ (TLS 1.3 preferred). All API calls, all data exchange, all internal service communication.
- Key management: AWS KMS, Azure Key Vault, or GCP Cloud KMS. Keys rotated on schedule. Never store encryption keys alongside the data they protect.
Under the 2026 HIPAA Security Rule updates, AES-256 at rest and TLS 1.2+ in transit are no longer “addressable.” They’re mandatory for any system handling ePHI.
B. Layer 2: Access Control
Three mechanisms, layered:
- RBAC (Role-Based Access Control): Clinician, nurse, admin, billing, patient roles with predefined permissions
- ABAC (Attribute-Based Access Control): Dynamic policies based on attributes – department, location, time of day, device type
- SMART on FHIR scopes: For third-party app authorization. Granular scopes define exactly which FHIR resources and operations an app can access.
The 42 CFR Part 2 requirement: Behavioral health and substance use disorder records require separate consent-based access controls. A PCP can’t automatically see therapy notes. The access control architecture must support record segmentation, not just role-based visibility.
C. Layer 3: Authentication
- MFA (Multi-Factor Authentication): Mandatory for all remote ePHI access under 2026 HIPAA updates. Not optional. Not “recommended.”
- OAuth 2.0 + OpenID Connect: For application-level authentication
- SSO (SAML/OIDC): For enterprise clients with existing identity providers
- Session management: Automatic timeout (15-minute inactivity for clinical workstations), re-authentication for sensitive operations
D. Layer 4: Audit and Logging
- Comprehensive logging: Every resource access, every modification, every query. Who accessed what, when, from where, what they did.
- Tamper-proof trails: Logs stored in append-only storage. Cannot be modified or deleted by the application or its administrators.
- Retention: Minimum 6 years (HIPAA requirement). Many organizations retain 7-10 years for legal protection.
- Real-time alerting: Anomaly detection on access patterns. If a user who normally accesses 20 records/day suddenly accesses 2,000, trigger an alert.
Why audit logging matters beyond compliance: It’s your breach detection mechanism. The 279-day average detection time (IBM, 2025) is partly because organizations don’t monitor access patterns in real time. Good audit architecture with anomaly detection can cut that to days.
E. Layer 5: Network Security
- VPC isolation: EHR infrastructure in a private VPC. No public subnets for databases or application servers.
- WAF (Web Application Firewall): Protects API endpoints from injection, XSS, and other OWASP attacks
- DDoS protection: AWS Shield, Cloudflare, or equivalent. Clinical systems can’t go down because of a volumetric attack.
- Network segmentation: Database tier separated from application tier. Each microservice has minimum required network access.
- Zero Trust Architecture: The 2026 HIPAA Security Rule explicitly references ZTA as the expected security model. Verify every request, trust no network segment by default.
F. Layer 6: Application Security
- Input validation: All user input sanitized before processing. FHIR resource validation against profiles.
- OWASP Top 10: Addressed in code review and automated scanning. Injection, broken auth, sensitive data exposure, XML external entities, broken access control, security misconfiguration, XSS, insecure deserialization, component vulnerabilities, insufficient logging.
- Dependency scanning: Automated scanning for known vulnerabilities in third-party libraries. Patch critical CVEs within 15 days (2026 HIPAA requirement).
- Container security: If running in Kubernetes, scan images for vulnerabilities. Enforce pod security policies. No running as root.
Build Custom EHR with Mindbowser
III. How Do You Architect HIPAA Compliance for Custom EHR?
HIPAA has three safeguard categories. All three apply to custom EHR.
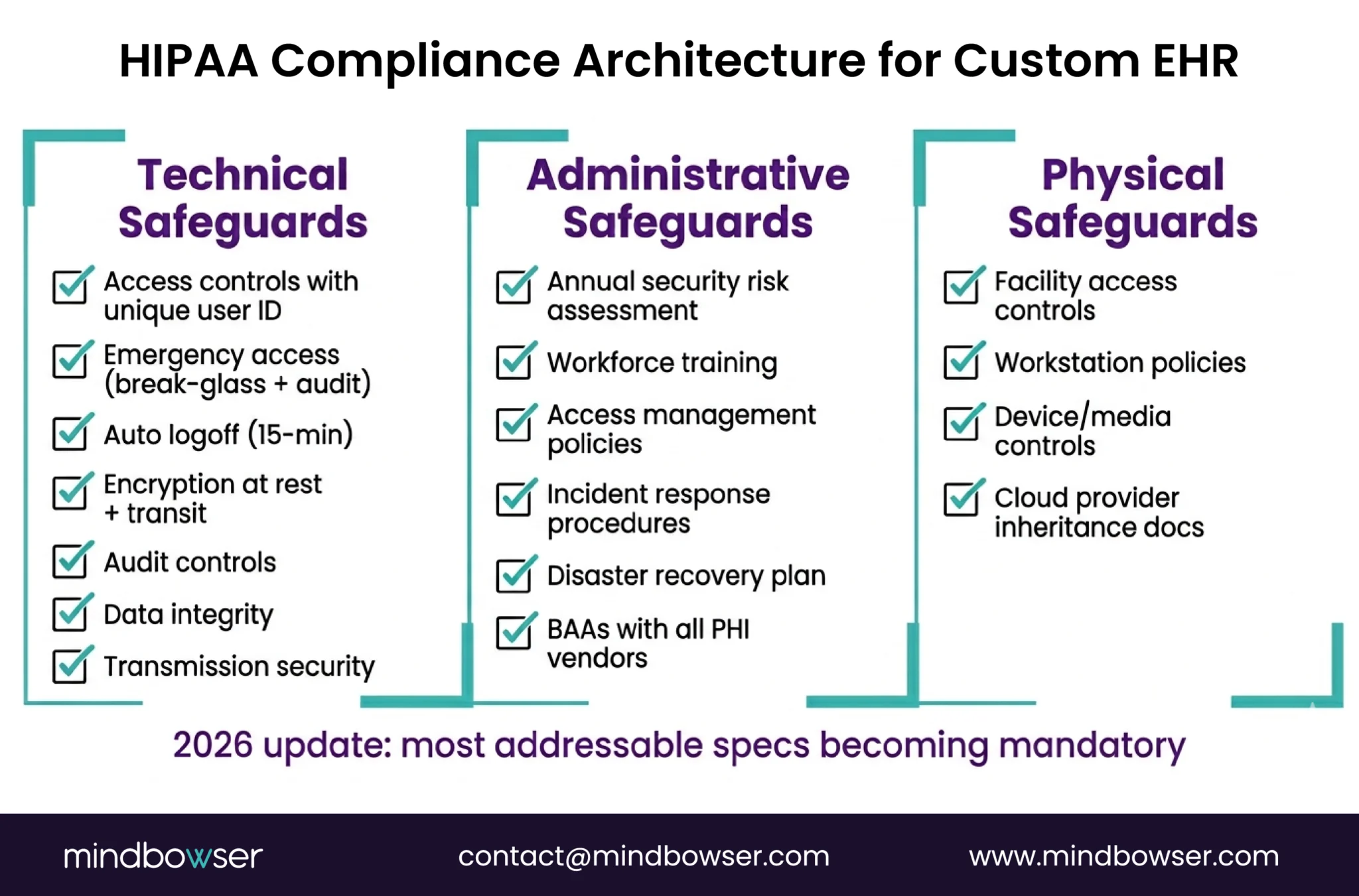
A. Technical Safeguards (what the system does)
- Access controls with unique user identification
- Emergency access procedures (break-glass with audit trail)
- Automatic logoff (15-minute clinical standard)
- Encryption at rest and in transit (mandatory under 2026 updates)
- Audit controls with comprehensive logging
- Data integrity controls (checksums, validation)
- Transmission security (TLS 1.2+)
B. Administrative Safeguards (what the organization does)
- Security Risk Assessment (annual requirement – not optional)
- Workforce security training
- Information access management policies
- Security incident response procedures
- Contingency/disaster recovery plan
- Business Associate Agreements (BAAs) with every vendor handling PHI
C. Physical Safeguards (where the data lives)
- Facility access controls (for any on-prem components)
- Workstation use policies
- Device and media controls
- For cloud-hosted custom EHR: Cloud provider’s physical security inherits (AWS SOC 2, Azure compliance) – but you still need cloud-specific controls (S3 bucket policies, IAM, encryption configuration)
The BAA chain for a Medplum-based custom EHR:
Your organization -> Mindbowser (BAA) -> Medplum (BAA) -> AWS (BAA)
Each link in the chain needs a signed BAA. If any link is missing, you have a HIPAA gap. We handle this as part of every custom EHR engagement – the BAA chain is established during Phase 1 (Discovery), not Phase 4 (Deployment).
IV. When Do You Need SOC 2 vs HITRUST?
Both are compliance frameworks. They solve different problems.
The 2026 update: Practice administrators must now obtain annual written verification from cloud vendors, including SOC 2 Type II or HITRUST certification reports. This isn’t new guidance – it’s becoming a mandatory verification requirement.
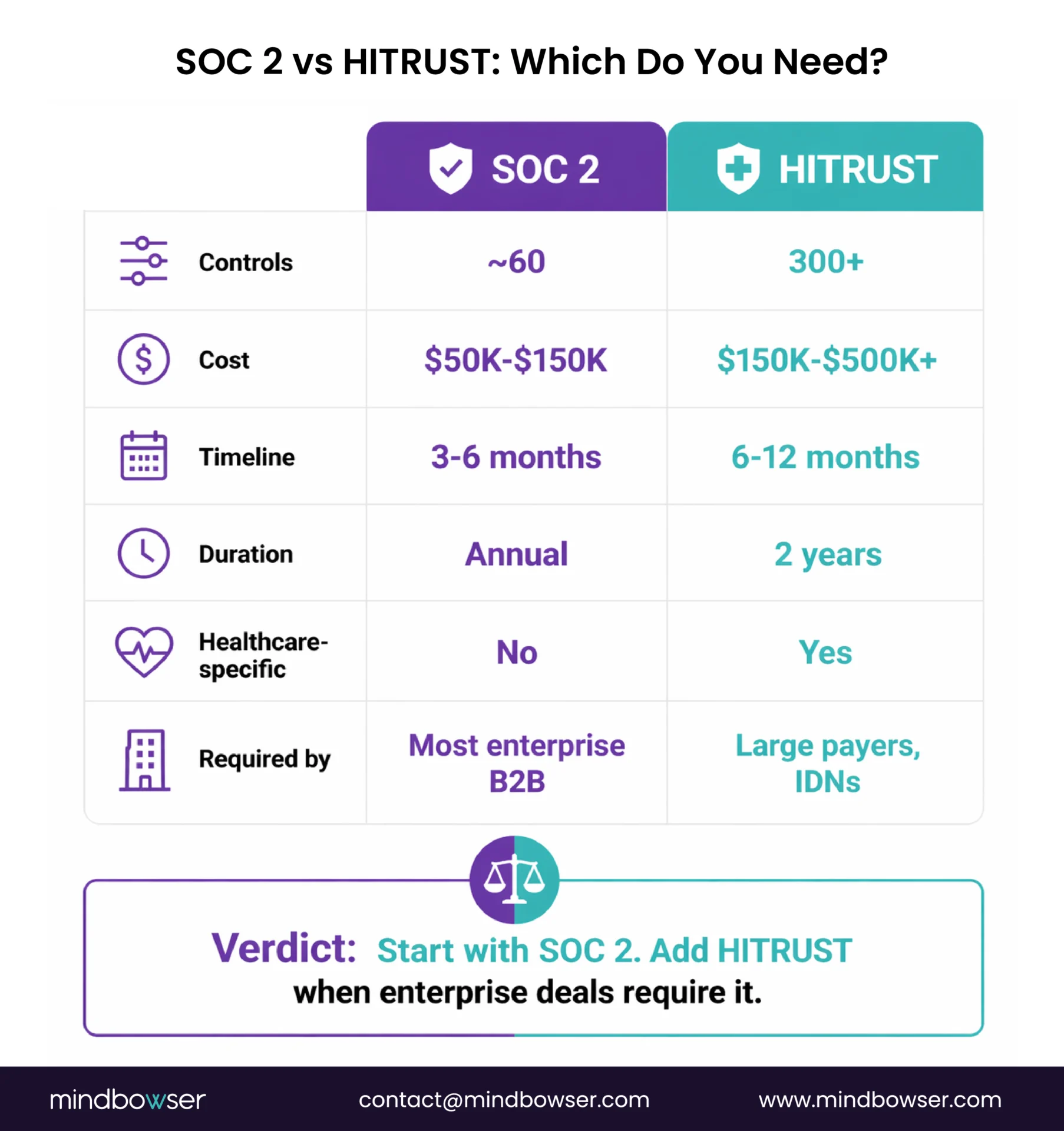
A. Our recommendation for custom EHR builders:
- Start with SOC 2 Type II. Lower cost ($50K-$150K), faster to achieve (3-6 months), covers most buyer requirements.
- Pursue HITRUST when selling to large payers or IDNs. They’ll ask for it. It’s the healthcare gold standard.
- If building on Medplum: Medplum is SOC 2 ready by design and pursuing HITRUST certification in 2026. Your application layer needs its own compliance posture, but the platform handles infrastructure-level controls.
We use a HIPAA-compliant data handling framework, our HIPAA-compliant data handling accelerator – on every custom EHR build. It provides the encryption, access control, and audit logging framework so compliance is infrastructure, not a project. For builds on Medplum, PHISecure layers on top of the platform’s baseline to handle edge cases: migration data handling, bulk processing, multi-system integration, and custom audit requirements.
Need the security architecture right from day one? Tell us about your compliance requirements and we’ll scope the security layers alongside the clinical build.
V. What Does Security Testing Look Like for Custom EHR?
Four testing cadences. All are required, not optional.
A. Penetration Testing (Annual + Major Release)
- External pen test by a third-party firm
- Scope: API endpoints, authentication, access controls, FHIR resource authorization, data exposure
- For custom EHR: include SMART on FHIR scope testing – can an app with patient/read scope access data it shouldn’t?
B. HIPAA Security Risk Assessment (Annual)
- Required by HIPAA. Not optional. Not “recommended.”
- Covers: all ePHI-containing systems, risk identification, risk ranking, mitigation plan
- The 2026 rule changes strengthen this: risk assessments must be more thorough and documented
C. Vulnerability Management (Continuous)
- Automated dependency scanning (Dependabot, Snyk, or equivalent)
- Critical CVEs: remediate within 15 calendar days (2026 HIPAA requirement)
- High CVEs: remediate within 30 days
- Medium/low: scheduled patching cycle
D. Third-Party Audits (Annual or Per-Requirement)
- SOC 2 Type II audit (if pursuing certification)
- HITRUST assessment (if pursuing certification)
- Custom security reviews for enterprise clients who require them
- Budget $50K-$150K/year for ongoing security testing and audit costs
EHR Security Architecture: Where to Start
EHR security isn’t a feature. It’s the architecture. Every layer – encryption, access control, authentication, audit, network, application – has to be designed in from day one. Bolting security onto a finished application is 3-5x more expensive than building it in.
Three things worth remembering:
- The 2026 HIPAA Security Rule changes are real and imminent. “Addressable” is becoming “mandatory.” MFA, AES-256, 15-day vulnerability remediation, Zero Trust Architecture. If your custom EHR doesn’t meet these by late 2026, you have a compliance gap.
- Start with SOC 2, add HITRUST when enterprise deals require it. SOC 2 costs $50K-$150K and takes 3-6 months. HITRUST costs $150K-$500K+ and takes 6-12 months. Build on a platform with baseline compliance Medplum architecture guide so your audit scope is your application layer, not the entire infrastructure stack. If you’re still planning your overall approach, our EHR modernization guide maps security requirements to each development phase.
- Budget 15-25% of your build cost annually for security and compliance. Penetration testing, risk assessments, vulnerability management, audit costs, and compliance updates are ongoing. For a $200K custom EHR build, that’s $30K-$50K/year. This isn’t optional spending. It’s the cost of handling PHI.
Building a custom EHR and need the security architecture right from the start? Tell us about your compliance requirements and we’ll scope the security layers alongside the clinical build.
A custom EHR needs 6 security layers: (1) Data encryption – AES-256 at rest, TLS 1.2+ in transit; (2) Access control – RBAC + ABAC + SMART on FHIR scopes, with 42 CFR Part 2 segmentation for behavioral health; (3) Authentication – MFA (mandatory under 2026 HIPAA updates), OAuth 2.0, SSO; (4) Audit logging – comprehensive, tamper-proof, with real-time anomaly detection; (5) Network security – VPC isolation, WAF, DDoS protection, Zero Trust Architecture; (6) Application security – OWASP Top 10, dependency scanning, 15-day critical CVE remediation. All six layers must be designed in from day one, not added post-development.
It depends on the builder, not the model. A well-architected custom EHR with proper security layers, penetration testing, and SOC 2/HITRUST certification can be more secure than off-the-shelf because security is designed for your specific data model and access patterns rather than configured generically. However, a poorly built custom EHR without proper security architecture is less secure than a mature commercial EHR with years of security hardening. The key differentiator: build on a platform with baseline compliance (like Medplum – SOC 2 ready, ONC certified, pursuing HITRUST) so you inherit infrastructure security and focus your effort on application-layer controls.
HITRUST CSF (Common Security Framework) is the gold standard healthcare security certification. It incorporates requirements from HIPAA, NIST, PCI, ISO 27001, and other frameworks into a single unified framework with 300+ controls (5x more than SOC 2). HITRUST r2 certification is a 2-year certification with interim testing at year 1. Cost: $150K-$500K+ including assessment and remediation. Timeline: 6-12 months. Large payers, integrated delivery networks, and health systems increasingly require HITRUST from vendors handling PHI. The latest version is CSF v11.7.0 (December 2025). Medplum is pursuing HITRUST certification for its hosted environment in 2026.
HIPAA compliance in custom EHR requires three safeguard categories: Technical (encryption, access controls, audit logging, session management), Administrative (annual security risk assessments, workforce training, incident response procedures, BAAs with all vendors), and Physical (facility access controls, device policies – or inherited from cloud provider for cloud-hosted EHR). The critical architectural decisions: establish the BAA chain during discovery (your org -> builder -> platform -> cloud provider), implement encryption before storing any PHI, build audit logging as infrastructure (not an afterthought), and plan for the 2026 HIPAA Security Rule updates that eliminate “addressable” specs and make controls like MFA, AES-256, and 15-day vulnerability remediation mandatory.

