



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
The CMS AUC mandate is gone, rescinded effective January 2025. But 1,039 of the 1,356 FDA-cleared AI devices are radiology products, and the hard problem is now integration, not model availability. Most imaging departments run five or more cleared AI vendors with disconnected dashboards. The winning architecture normalizes findings to FHIR through a single clinical decision support orchestration layer. Image-processing CDS is regulated as SaMD under FDA; the orchestration layer around it is generally exempt under Section 3060.
1. The Market Reset: Why Radiology CDS Looks Different in 2026
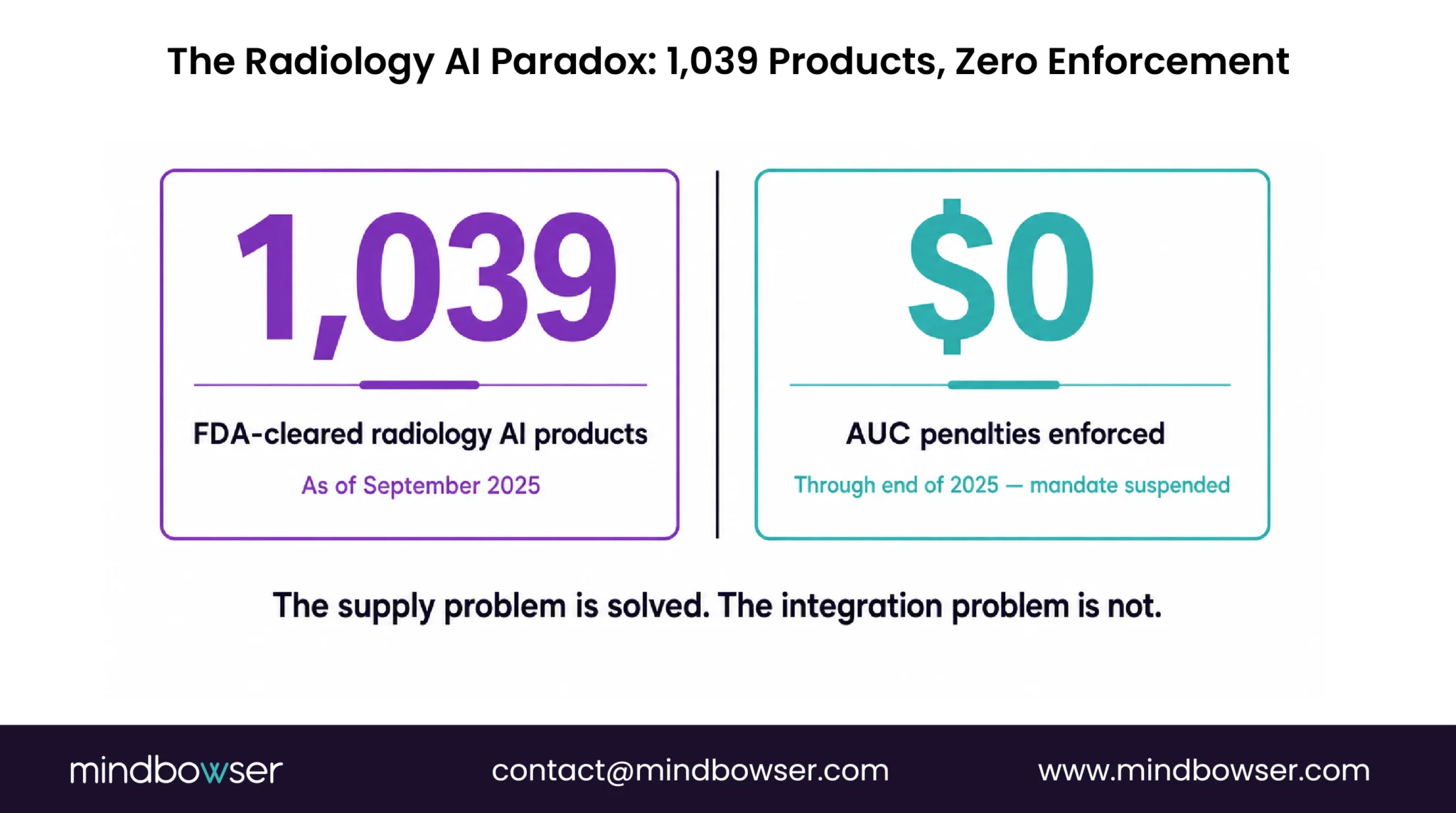
As of September 2025, the FDA has authorized 1,356 AI-enabled medical devices, and 1,039 of them, seventy-seven percent, are radiology products. The question buyers ask us has changed. Three years ago it was “is there an AI cleared for stroke detection on non-contrast CT.” Now the question is “how do we run five of them on the same study without breaking the radiologist’s worklist.”
Vendor concentration on the FDA list runs as follows. GE HealthCare leads with 115 radiology AI authorizations. Siemens Healthineers has 86, Philips 48, Canon 41, United Imaging 38, Aidoc 30. The Imaging Wire’s December 2025 tally confirms the vendor mix and the continued radiology dominance of the AI/ML clearance pipeline.
The historical investment driver is gone. The Protecting Access to Medicare Act of 2014 mandated that ordering physicians consult appropriate use criteria via a qualified clinical decision support mechanism before placing advanced imaging orders for Medicare beneficiaries. CMS paused the program in the CY 2024 PFS Final Rule, rescinded the regulations at 42 CFR 414.94, and ASNC reports CMS instructed contractors to remove all national and local edits related to the AUC program for claims with dates of service on or after January 1, 2025. No payment penalties were ever enforced. ACR Select, National Decision Support Company, and the qualified-CDSM cohort lost the regulatory tailwind that built the original market.
What remains as investment driver is operational, not regulatory. Joint Commission accreditation pressure across roughly 4,200 hospitals. Leapfrog Group public safety scoring across roughly 2,200 reporters. And the daily friction of running multiple AI vendors in production, each with its own dashboard, each posting findings into a different lane.
That is the inheritance every radiology CDS project starts with in 2026. A surplus of cleared models, no mandate driving adoption, and a department-level integration deficit.
2. What Is Radiology Clinical Decision Support?
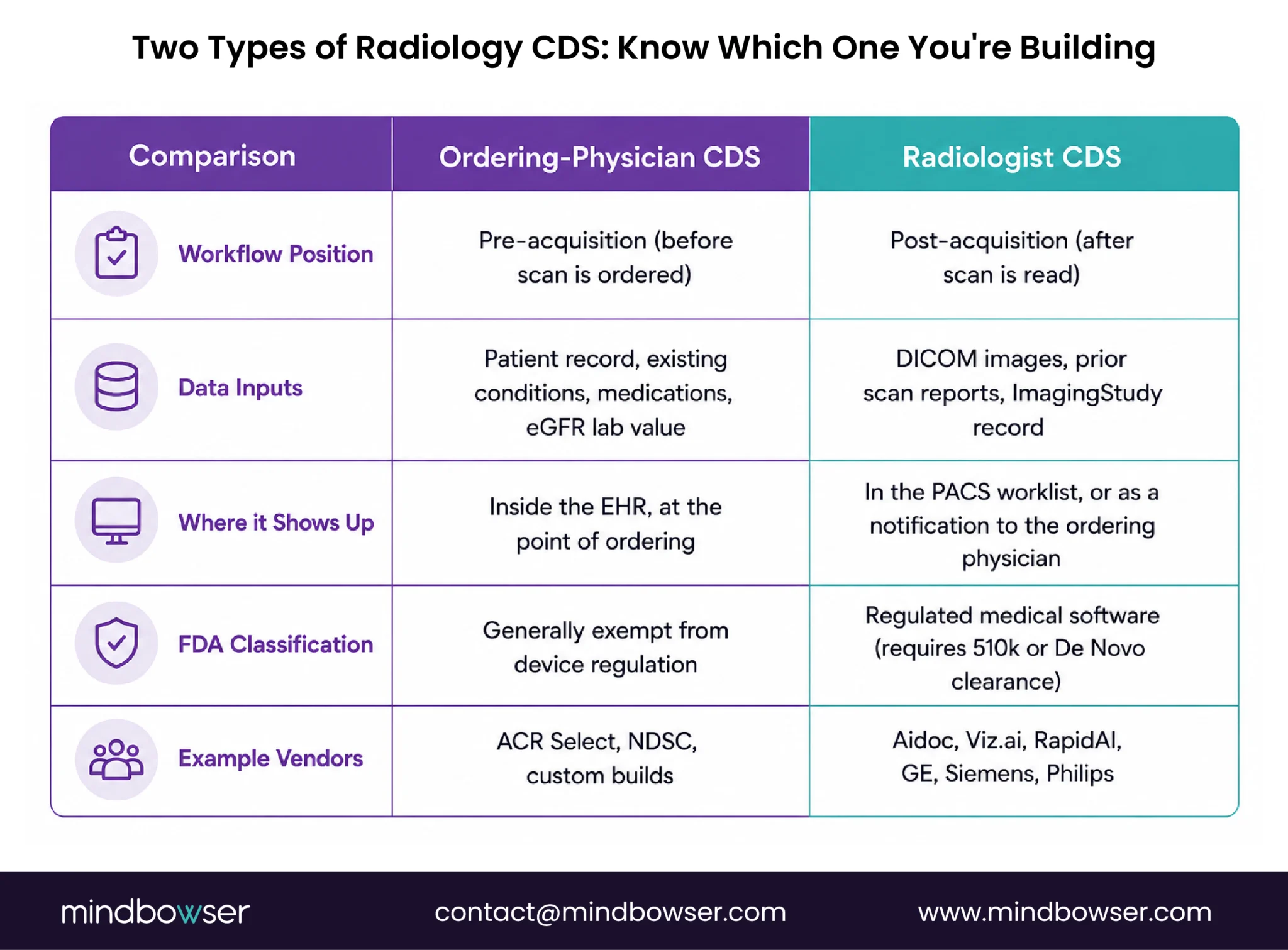
Radiology clinical decision support is the layer of software that guides imaging decisions at two distinct points in the workflow. The first is when an ordering physician selects an imaging study, before the order is committed; this is ordering-physician-facing CDS, often consulting protocol guidelines or contrast-safety logic. The second is when a radiologist interprets the resulting images; this is radiologist-facing CDS, often AI-assisted finding detection or worklist prioritization. Both layers consume FHIR ServiceRequest and ImagingStudy data and surface guidance through CDS Hooks, PACS workflow integration, or both.
The bifurcation matters because most radiology buyers conflate the two and most vendors specialize in one. Aidoc, Viz.ai, and RapidAI are radiologist-facing; they read pixels and post findings. ACR Select and the older qualified-CDSM cohort are ordering-physician-facing; they consult criteria pre-acquisition. A complete radiology CDS deployment usually needs both layers, on different rails, integrated into the same patient record.
The architecture below covers both layers, with the radiologist-facing pipeline taking the heaviest build because that is where the cleared-vendor sprawl lives.
3. The DICOM-to-CDS-Card Pipeline (Architecture)
The pipeline shape we build for radiology CDS is the same shape we shipped for Remedy Robotics, where DICOM processing went from weeks to a single day with a 99 percent PHI de-identification success rate. Five stages, each one a build decision.
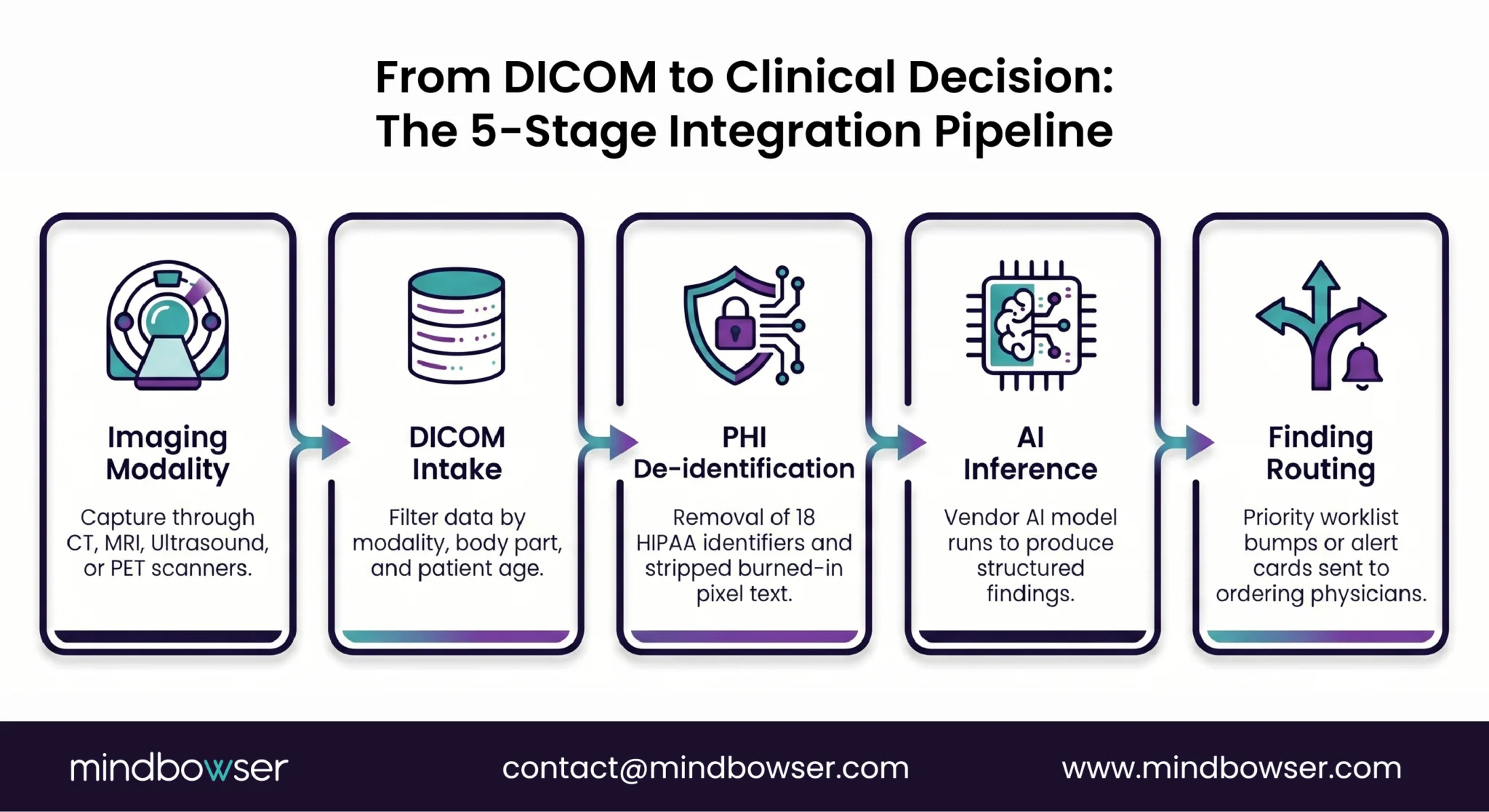
- One: DICOM intake. The imaging modality (CT, MRI, ultrasound, PET, nuclear medicine) writes a study to the PACS or VNA. The AI inference layer subscribes to new studies via DIMSE C-MOVE or via DICOMweb services, specifically QIDO-RS for query, WADO-RS for retrieval, and STOW-RS for downstream storage. Build decision at this stage: which subset of studies routes to AI inference, and on what trigger. A common pattern is modality plus body part plus age filter; for example, head CT in adults routes to a stroke-detection model, head CT in children does not.
- Two: PHI de-identification. Eighteen HIPAA identifiers strip from DICOM headers and from burned-in pixel annotations before the study leaves the institution boundary for vendor-hosted inference. Our PHISecure accelerator handles the identifier list and the pixel-burned-in annotation detection across DICOM, NIfTI, and video formats. The Remedy build hit 99 percent de-identification success because the pixel-burned-in step, the one most vendors get wrong, was treated as a primary requirement rather than an afterthought.
- Three: AI inference. The vendor model runs (typically a containerized inference service or a vendor API). Output is a structured finding with location, confidence score, and severity. For a stroke-detection model on a non-contrast head CT the output looks like “intracranial hemorrhage detected, location left frontal, confidence 0.94, severity high.” Build decision: which vendors to integrate, and how their output schemas reconcile.
- Four: Finding routing. The finding posts to the patient record as a FHIR
DiagnosticReportlinked to the originatingImagingStudy, or as a structuredObservationif the finding is a quantitative measurement. The 2024 RSNA Radiology IHE primer is the standards anchor for how AI radiology output integrates with healthcare enterprise profiles. - Five: Surface. Either a worklist priority bump in the PACS (for radiologist-facing) or a CDS Card via
order-selecton the ordering physician’s screen (for ordering-physician-facing). Both surfaces consume the same finding object; the routing logic decides which surfaces fire for which finding type.
The pipeline is the foundation. The ordering-physician layer and the radiologist layer both run on top of it.
4. CDS Hooks order-select for Imaging Orders (Ordering-Physician-Facing CDS)
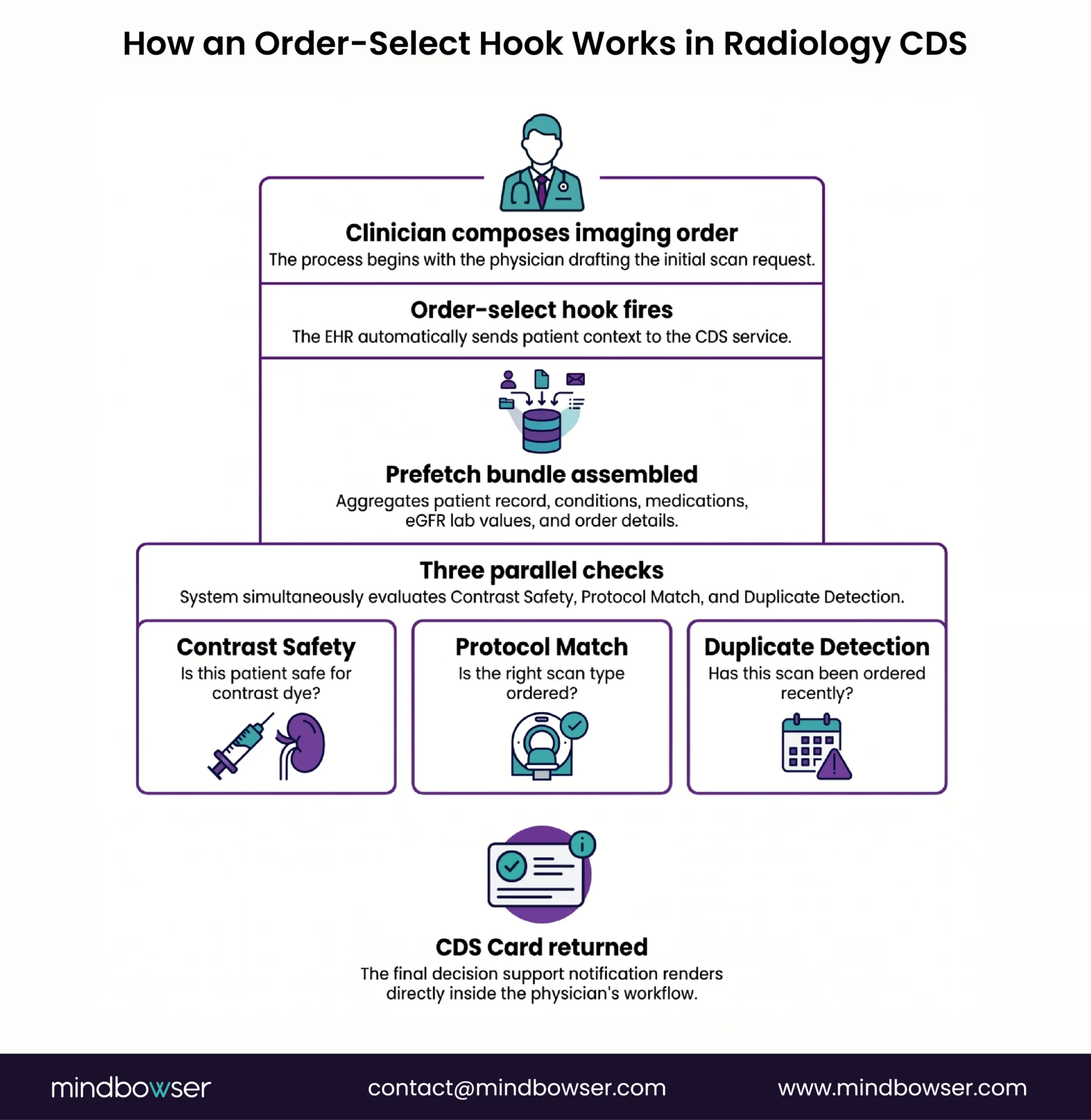
CDS Hooks defines two hooks relevant to imaging orders. order-select fires several times as the clinician composes an order, before the clinician signs. order-sign fires once at signing. The HL7 CDS Hooks library recommends order-select for imaging because guidance lands earlier in the decision moment, when the clinician can still reroute or modify the order without rework.
The prefetch contract for an imaging-order CDS service typically includes ServiceRequest (the imaging order being composed), Patient (demographics, age), Condition (active diagnoses such as pregnancy or kidney disease), Observation (recent labs including eGFR for contrast safety), and MedicationRequest (relevant medications such as metformin pre-contrast or anticoagulants pre-procedure). The CDS service evaluates these resources against institution-specific protocols and returns a CDS Card with structured guidance.
Use cases that survive the AUC mandate’s death:
- Contrast safety. eGFR-based recommendations for contrast type, hydration protocols, or alternative imaging when renal function is impaired.
- Radiation considerations. Pediatric and pregnancy-aware dose protocols. The system flags when radiation dose can be reduced or avoided altogether (ultrasound or MRI alternatives).
- Duplicate-imaging detection. Recent prior studies of the same body part; flags ordering when a recent prior would answer the clinical question.
- Evidence-based protocol matching. Lyme suspected on cranial nerve symptoms, the system surfaces MR brain plus spine rather than CT chest, with a brief evidence note.
- Voluntary AUC consultation. ACR Select and the original qualified-CDSM cohort still operate. They pivoted from regulatory check to voluntary clinical guidance. Some institutions keep the consultation for quality programs unrelated to the rescinded mandate.
The mechanism is the same one our team built for PeriopMD on a different prefetch contract. PeriopMD reached 87 percent provider engagement on its preoperative-labs CDS Hooks build because the alert design respected the clinician’s workflow. The same design discipline transfers to imaging-order CDS. The pattern is documented in our CDS Hooks technical guide.
5. AI Vendor Sprawl: Integrating Multiple Cleared Models into One Radiologist Worklist
Honest problem statement. The radiology departments we talk to do not have an AI availability problem. They have an AI integration problem.
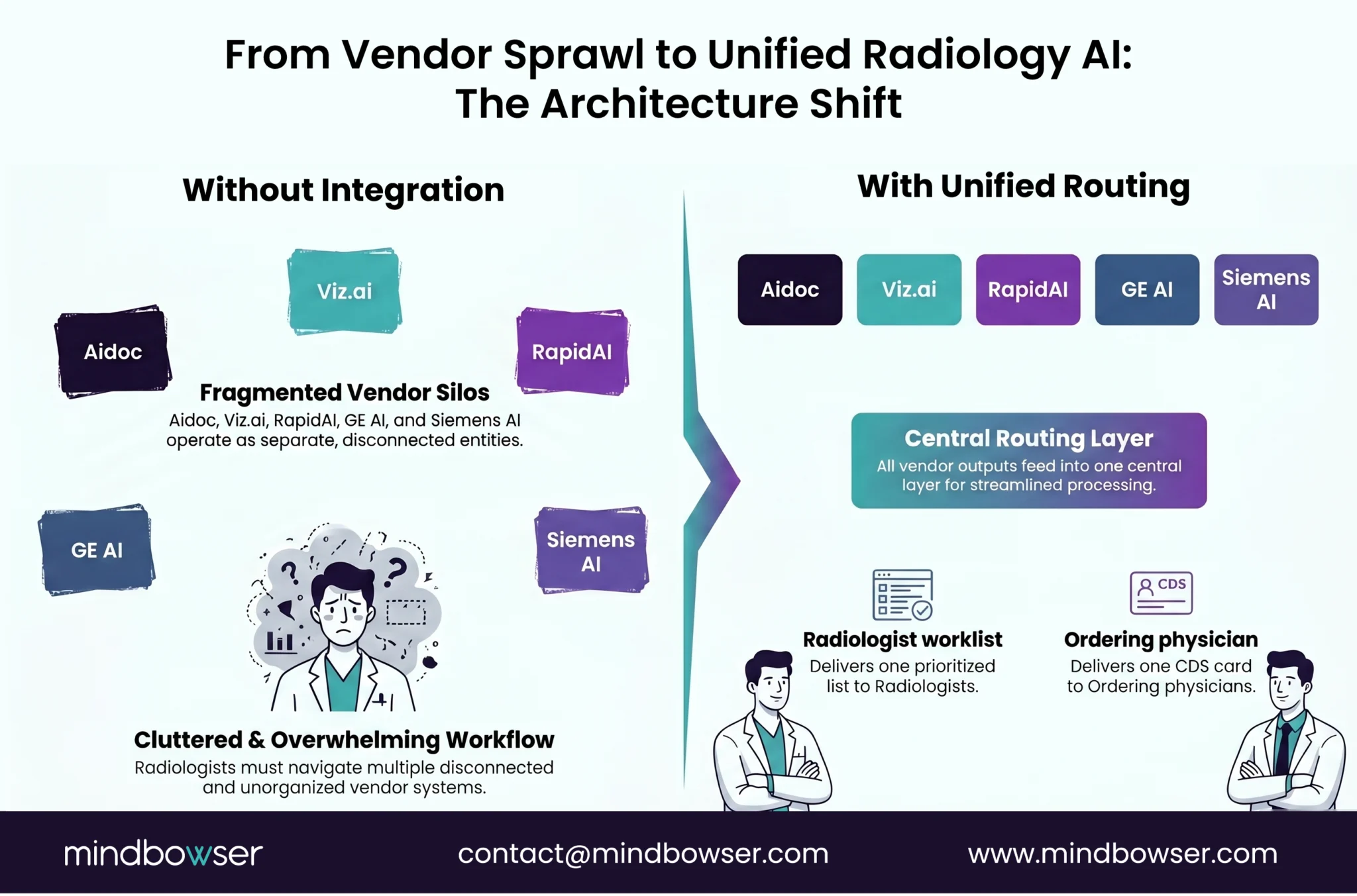
Aidoc operates 18 FDA clearances and is deployed in more than 1,600 hospitals worldwide and 150 plus US health systems. Viz.ai operates 13 cleared algorithms and is deployed in over 1,600 hospitals. RapidAI specializes in emergency findings detection. The big imaging OEMs (GE, Siemens, Philips, Canon) ship cleared AI in bundles attached to their modalities. A 350-bed academic medical center can easily run five to eight AI vendors in production.
Each vendor ships its own dashboard. Each posts findings on its own notification path. None of them coordinates with the others on worklist priority logic. Radiologists context-switch between four to five UIs per shift to triage findings that should land in one ordered queue.
The Mayo Clinic Proceedings: Digital Health team framed the integration challenge 00121-4/fulltext) accurately in 2024. Their 2024 review of AI radiology workflow integration concluded that the bottleneck is not model accuracy but the operational discipline of routing AI findings into the EHR and notification systems with clear urgency rules. The integration question, not the model accuracy question, is what stalls deployment.
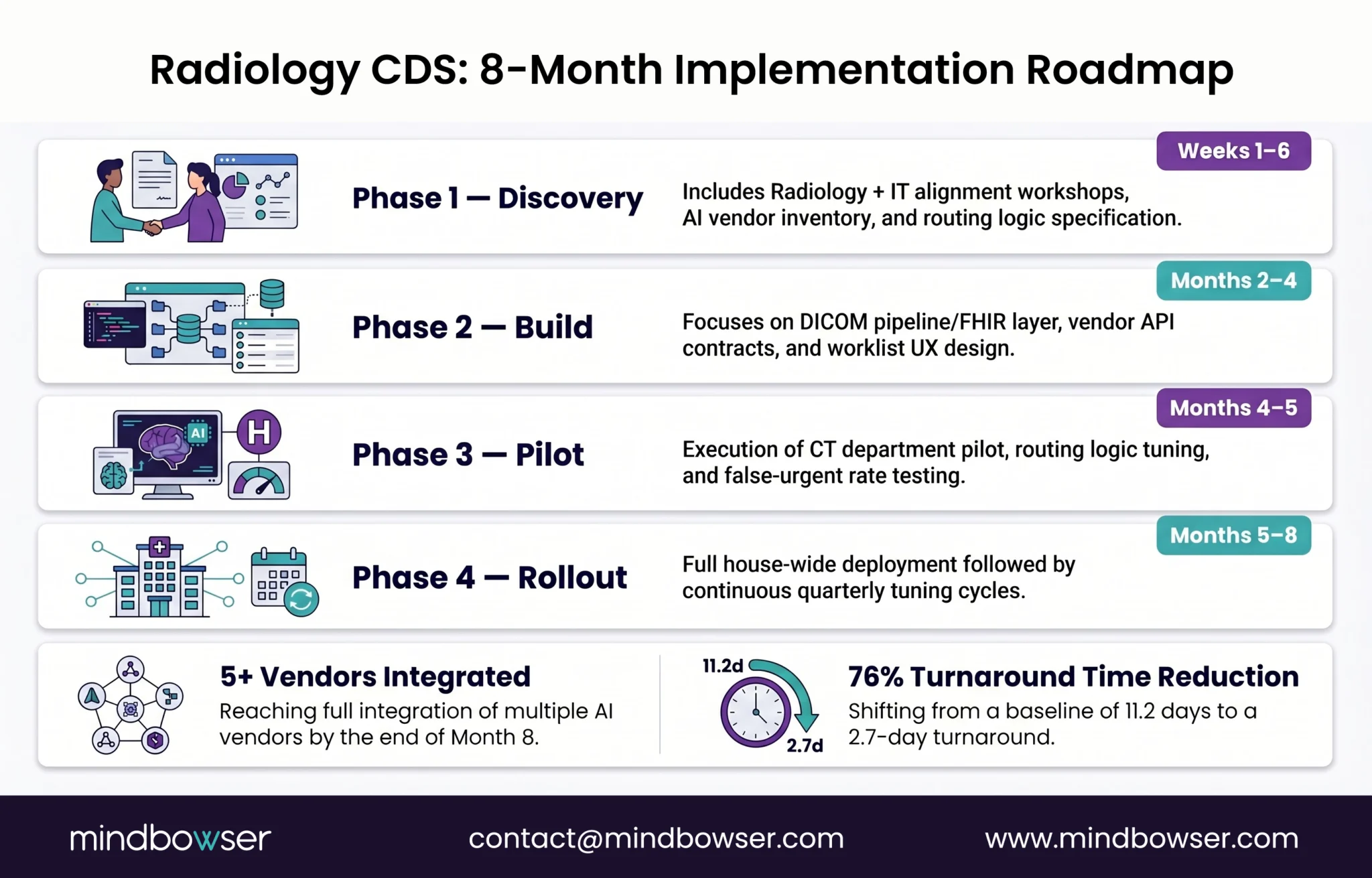
The architecture that consolidates the sprawl looks like this. A routing layer ingests findings from N vendor APIs or webhook endpoints. The layer normalizes vendor-specific output schemas into FHIR Observation or DiagnosticReport. Institution-specific priority logic applies on top of the normalized output (stroke-suspected high priority, subdural hemorrhage high priority, incidental pulmonary nodule low priority pending follow-up). A single ordered worklist plus a deterministic notification path posts to the radiologist’s PACS surface. The arXiv 2025 study on AI-triage report turnaround time reported interpretation delivery dropping from 11.2 days to 2.7 days when AI findings routed through priority logic rather than separate dashboards. The time-savings are integration savings, not AI savings.
A note on what we ship and what we do not. Mindbowser does not have a packaged radiology-CDS accelerator. Our HealthConnect CoPilot accelerator is the FHIR data layer that holds ServiceRequest, ImagingStudy, and DiagnosticReport. PHISecure handles DICOM PHI de-identification. Both are plumbing. The routing engine, the priority logic, the worklist UX, and the FDA orchestration documentation are custom build, modeled on the Remedy Robotics pipeline shape and the PeriopMD CDS Hooks pattern. There is no shortcut here, and saying otherwise would oversell what the accelerators do.
The Mindbowser pattern transfers laterally to other CDS scopes. We covered the same architectural discipline in the medication safety clinical decision support write-up; the prefetch contract is different, the rules engine is different, the discipline is identical.
6. FDA Classification: When Radiology CDS Is Regulated (Most of It Is)
The regulatory picture for radiology CDS is the inverse of medication safety. Most radiology AI CDS is regulated.
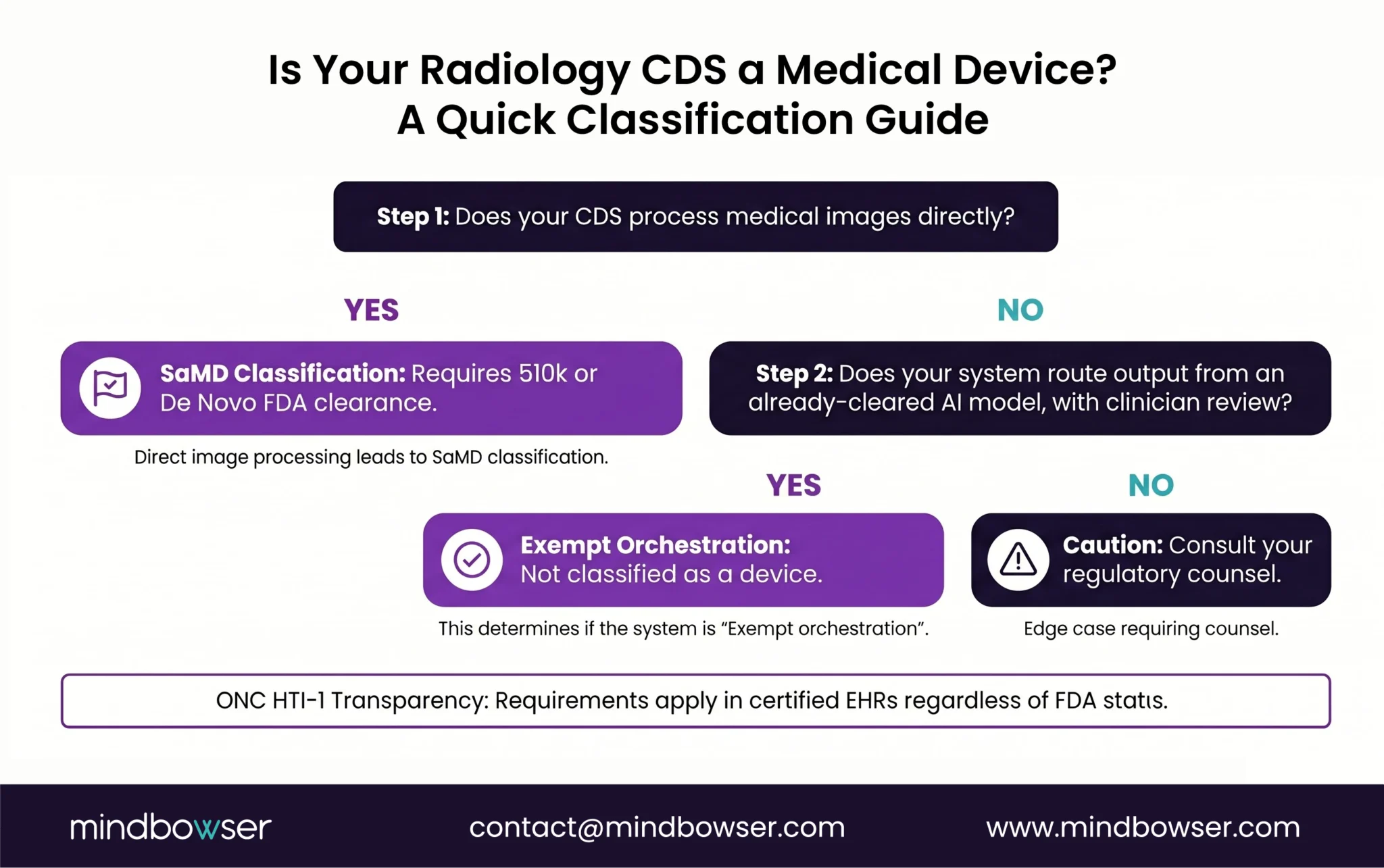
Section 3060 of the 21st Century Cures Act (21 USC 360j(o)) exempts CDS from FDA device regulation when four criteria hold. The first criterion is that the software does not acquire, process, or analyze a medical image, signal, or pattern from an in vitro diagnostic. Radiology AI processes medical images by definition. Most radiology AI CDS therefore falls outside the Section 3060 exemption and is regulated as Software as a Medical Device under the FDA 510(k) or De Novo pathway.
The FDA’s January 6, 2026 revised CDS Guidance (which replaces the September 2022 version) reaffirms this boundary. Image-derived CDS is regulated. Clinician-reviewable basis is required for transparency. Aidoc, Viz.ai, RapidAI, and the OEM-bundled AI products all hold FDA 510(k) clearances for the specific indications they target. The clearance count itself has become a competitive metric.
The integration layer is where the build sits in exempt territory. The routing engine that ingests findings from already-cleared AI services, normalizes them to FHIR, applies institution priority logic, and surfaces them through the radiologist’s worklist consumes regulated AI output. It does not itself process images. The radiologist reviews the basis for each finding before acting. This is exempt orchestration. The build pattern we use: license the cleared AI components as regulated devices; build the integration around them as exempt orchestration; document the boundary explicitly in a Quality System Documentation file so an auditor can trace which components are cleared and which are not.
ONC’s HTI-1 Final Rule (89 FR 1192, effective February 8, 2024) adds a layer when the radiology CDS runs inside certified health IT. Decision Support Intervention transparency requirements apply, covering predictive and rule-based DSIs. Disclosure obligations include source attributes, intended use, validation methodology, and fairness review. Radiology AI vendors typically produce the disclosure documentation as part of FDA clearance; the institution’s job is surfacing it inside the EHR consistent with HTI-1.
7. What Does Building Radiology CDS Look Like at a 350-Bed AMC?
The shape of an engagement at a 350-bed academic medical center, drawn from the Remedy Robotics pipeline pattern adapted for full radiology-CDS scope. Roughly 390 US AMCs sit in the early-adopter pool for multi-vendor AI integration; the pattern below is what works at that scale and scales down to community hospitals once a reference architecture exists.
- Phase 1, weeks 1 through 6. Radiology and IT workshops to inventory existing AI vendors in production, map current notification flows, and identify priority-routing pain. Common discovery: the same radiologist receives stroke-detection alerts from one vendor, subdural hemorrhage alerts from another, and pulmonary embolism alerts from a third, with no shared priority logic. Output of phase 1 is a routing logic specification, a vendor inventory, and a top-five-priority-conflict list.
- Phase 2, months 2 through 4. DICOM intake pipeline build. PHI de-identification configured for the modality mix in production. FHIR layer wired up for
ImagingStudy,ServiceRequest, andDiagnosticReport. Vendor API contracts integrated for the top three cleared AI products in use. Routing engine built with priority logic from phase 1. Worklist surface designed against actual radiologist read sequences. CDS Hooksorder-selectservice deployed in EHR sandbox for ordering-physician-facing use cases. - Phase 3, months 4 through 5. Pilot with one modality. CT is the common starting point because cleared-product density is highest there and study volume generates tuning data quickly. The pilot generates two weeks of routing data. Worklist priority logic tunes against actual read times. Notification flow tests for false-urgent rate. Order-select CDS pilots with one ordering specialty (typically emergency medicine).
- Phase 4, months 5 through 8. House-wide rollout across modalities. Tuning loop continues quarterly. The KPI is interpretation turnaround time on priority findings; the arXiv 2025 reference benchmark is 2.7 days post-routing, down from 11.2 days pre-routing.
A scope conversation about cost. Cleared AI product licenses are typically 30 to 50 percent of total project spend; each vendor is its own license, and the institution often licenses three to five concurrently. The custom integration (DICOM intake plus PHI de-identification plus routing engine plus worklist UX plus FDA orchestration documentation) is the rest. A 350-bed AMC engagement runs eight months from first workshop to house-wide rollout. Multi-site systems and imaging-AI vendors commercializing for multi-tenant deployment scale differently and often longer.
For deeper architecture detail, our advanced clinical decision support write-up covers the rules-engine and integration patterns at protocol depth.
What This Means for Your Build
The radiology AI clearance pipeline has solved the model-availability problem. The CMS AUC mandate has stopped driving radiology-CDS investment. What is left is an integration build, and the build sits in two layers. The ordering-physician layer runs on CDS Hooks order-select with a contrast-safety and protocol-matching prefetch contract. The radiologist layer runs on a DICOM intake pipeline plus a multi-vendor routing engine plus a single worklist surface. Both layers consume FHIR. Both surface to the radiologist or ordering physician through the systems they already use.
Most of the cleared AI is regulated SaMD. The integration around it is generally exempt orchestration if the radiologist reviews the basis. License the components, build the integration, document the boundary.
If you are a VP Radiology evaluating multi-vendor AI integration, or a CTO at a Series B imaging AI company building toward multi-tenant deployment, the build pattern is well-documented now. We have shipped the DICOM pipeline shape (Remedy Robotics: weeks to one day, 99 percent PHI de-identification) and the CDS Hooks pattern (PeriopMD: 87 percent provider engagement). The radiology scope combines them.
Request an Assessment. A 30-minute scoping conversation, your AI vendor inventory plus our integration architecture, no obligation. Start a Conversation.
Conclusion
The AUC mandate is gone and it is not coming back in any form that will drive procurement decisions. What remains is an operational deficit, imaging departments running three to five cleared AI vendors, each with a separate dashboard, each posting findings into a different lane, each requiring a radiologist to context-switch. The answer is not a new vendor. It is a DICOM intake pipeline that normalizes findings from already-cleared models to FHIR and surfaces them through a single worklist. The orchestration layer does not need an FDA clearance when radiologists review the basis for each finding. What it needs is a clean PHI de-identification step, a routing engine that maps modality to model, and a FHIR DiagnosticReport structure the PACS can consume. The cleared models exist. The integration layer is the build.
No. CMS paused the AUC program in the CY 2024 PFS Final Rule (effective January 2024) and rescinded the regulations at 42 CFR 414.94 effective January 1, 2025. CMS instructed contractors to remove all national and local AUC claim edits for claims with dates of service on or after January 1, 2025. No payment penalties were ever enforced under the program. CMS may reevaluate AUC under future rulemaking, but as of 2026 the mandate is operationally dead and AUC consultation is voluntary, not required.
Radiology CDS is the layer of software that guides imaging decisions at two points in the workflow. The first is when an ordering physician selects an imaging study; this is ordering-physician-facing CDS, often using CDS Hooks order-select to consult contrast safety, radiation considerations, duplicate-imaging detection, and protocol matching. The second is when a radiologist interprets the resulting images; this is radiologist-facing CDS, typically AI-assisted finding detection or worklist prioritization. Both layers consume FHIR data and surface guidance through CDS Hooks or PACS workflow integration.
The pipeline runs in five stages. DICOM intake pulls new studies from the modality or VNA via DIMSE or DICOMweb (QIDO-RS, WADO-RS, STOW-RS). PHI de-identification strips 18 HIPAA identifiers and burned-in pixel annotations before the study leaves the institution boundary. AI inference runs (vendor model). The structured finding posts to the patient record as a FHIR DiagnosticReport linked to the originating ImagingStudy. The finding then surfaces through a worklist priority bump in the PACS for radiologist-facing alerts, or through a CDS Card on the ordering physician’s screen for pre-acquisition alerts.
Most of it is. CDS that processes medical images falls outside the Section 3060 Non-Device CDS exemption and is regulated as Software as a Medical Device under FDA 510(k) or De Novo pathway. Aidoc, Viz.ai, RapidAI, and OEM-bundled AI products all hold FDA clearances for their specific indications. The integration layer that routes findings from already-cleared AI services into a unified worklist is generally exempt orchestration if the radiologist reviews the basis for each finding. ONC HTI-1 DSI transparency requirements (89 FR 1192) apply when the CDS runs inside certified health IT.
Cost is scope-driven. Cleared AI product licenses are typically 30 to 50 percent of total project spend, with each vendor as its own license; institutions often run three to five concurrently. The custom integration (DICOM intake + PHI de-identification + routing engine + worklist UX + FDA orchestration documentation) is the rest. A 350-bed academic medical center engagement runs eight months phased across discovery, build, pilot, and house-wide rollout. The KPI is interpretation turnaround time on priority findings.


