



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
Native EHR drug-interaction alerts get overridden 90% of the time, the failure is architectural, not algorithmic. Alerts arrive without patient context and route to the wrong clinician. A custom medication-safety clinical decision support system using CDS Hooks order-sign, a tiered rules engine, and split pharmacist/prescriber routing cuts overrides sharply. The drug database is plumbing; the differentiator is alert design. Most medication-safety CDS qualifies for FDA Section 3060 exemption when clinicians can review the basis for each recommendation.
1. Why Native EHR Drug-Interaction Checking Stops Working
In my cardiac care years, I learned to dismiss drug-interaction alerts the same way every other physician on the floor did. By reflex. In under a second. Before the screen finished rendering.
I was not careless. I was conditioned. So was every resident, every senior consultant, every pharmacist I worked with. The alert system had taught us, through hundreds of low-value warnings a day, that the alert was almost certainly noise. The override key became muscle memory.
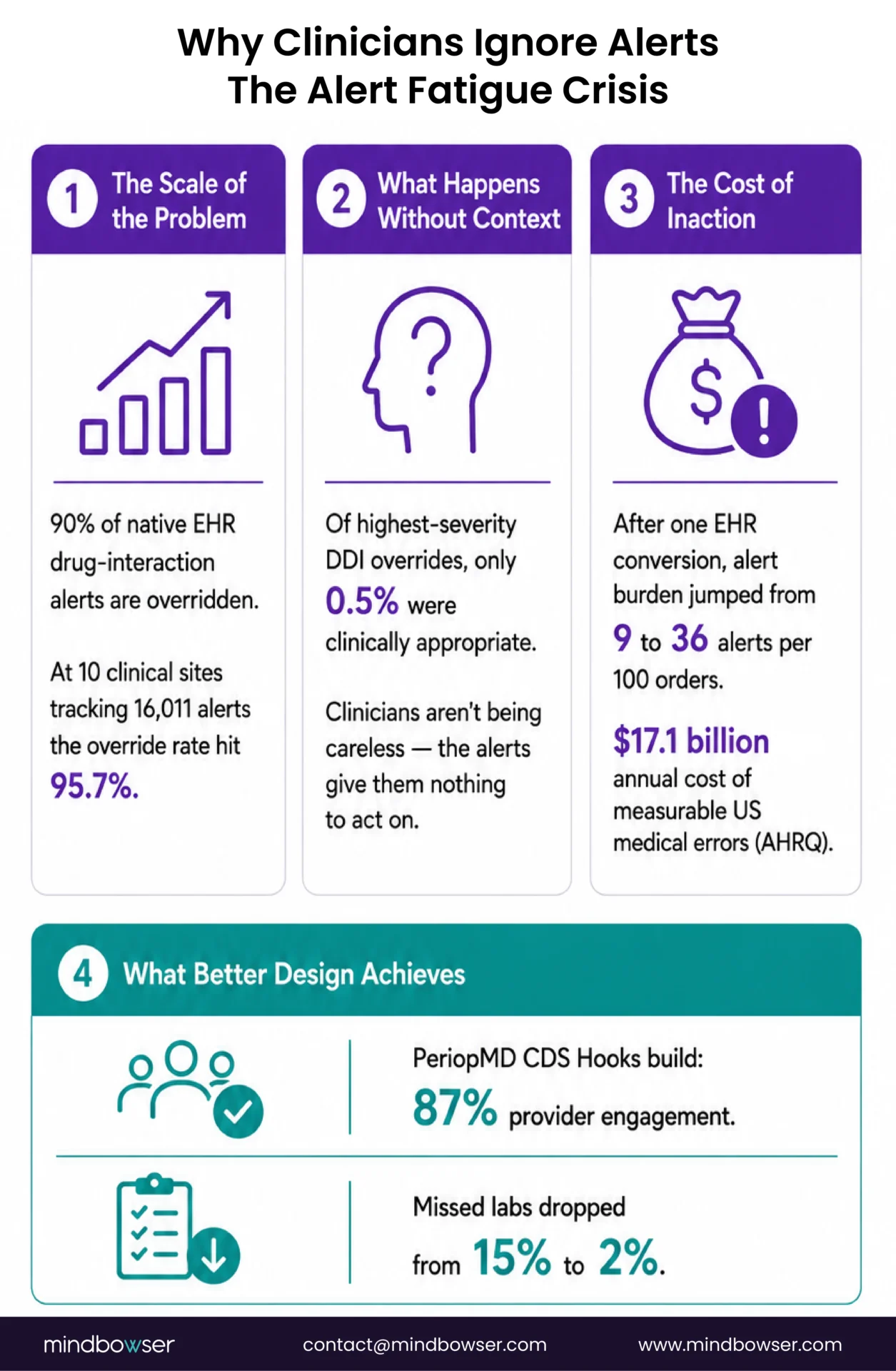
The literature now confirms what we knew on the floor. A 2024 systematic review and meta-analysis by Felisberto and colleagues, published in Health Informatics Journal, found that physician alert override rates run at 90 percent (95 percent CI, 85, 95 percent). Drug-drug interaction overrides specifically range from 55 percent to 98 percent across studies. That is not a few outliers. That is the standard operating reality.
The structural picture is worse than the headline. Wong and colleagues, studying Brigham and Women’s Hospital after their conversion to a commercial EHR (Journal of General Internal Medicine, 2018), found that DDI alerts increased from roughly 2 per 100 orders to about 11 per 100 orders. Total medication alert burden went from 9 to 36 per 100 orders. Same clinicians. Same patients. Four times the alert volume. Override rates stayed flat at 90 percent or higher.
And the most painful number comes from Cho and colleagues, writing in JAMIA in 2019, who looked across 10 clinical sites and 16,011 alerts. 95.7 percent were overridden. Override appropriateness ran at 45.4 percent overall. For the highest-severity DDIs (the alerts most likely to flag a genuine adverse drug event), only 0.5 percent of overrides were judged appropriate. The same study cataloged 177 distinct override reasons. Most had nothing to do with drug interactions.
Why does this matter beyond clinician fatigue? AHRQ pegs the annual cost of measurable medical errors at $17.1 billion in the United States. Medication errors are a meaningful share. The system designed to prevent them is the same system clinicians have learned to ignore.
That is the inheritance every medication-safety CDS project starts with. Not a missing alert. A trust deficit.
2. What Is Medication Safety Clinical Decision Support?
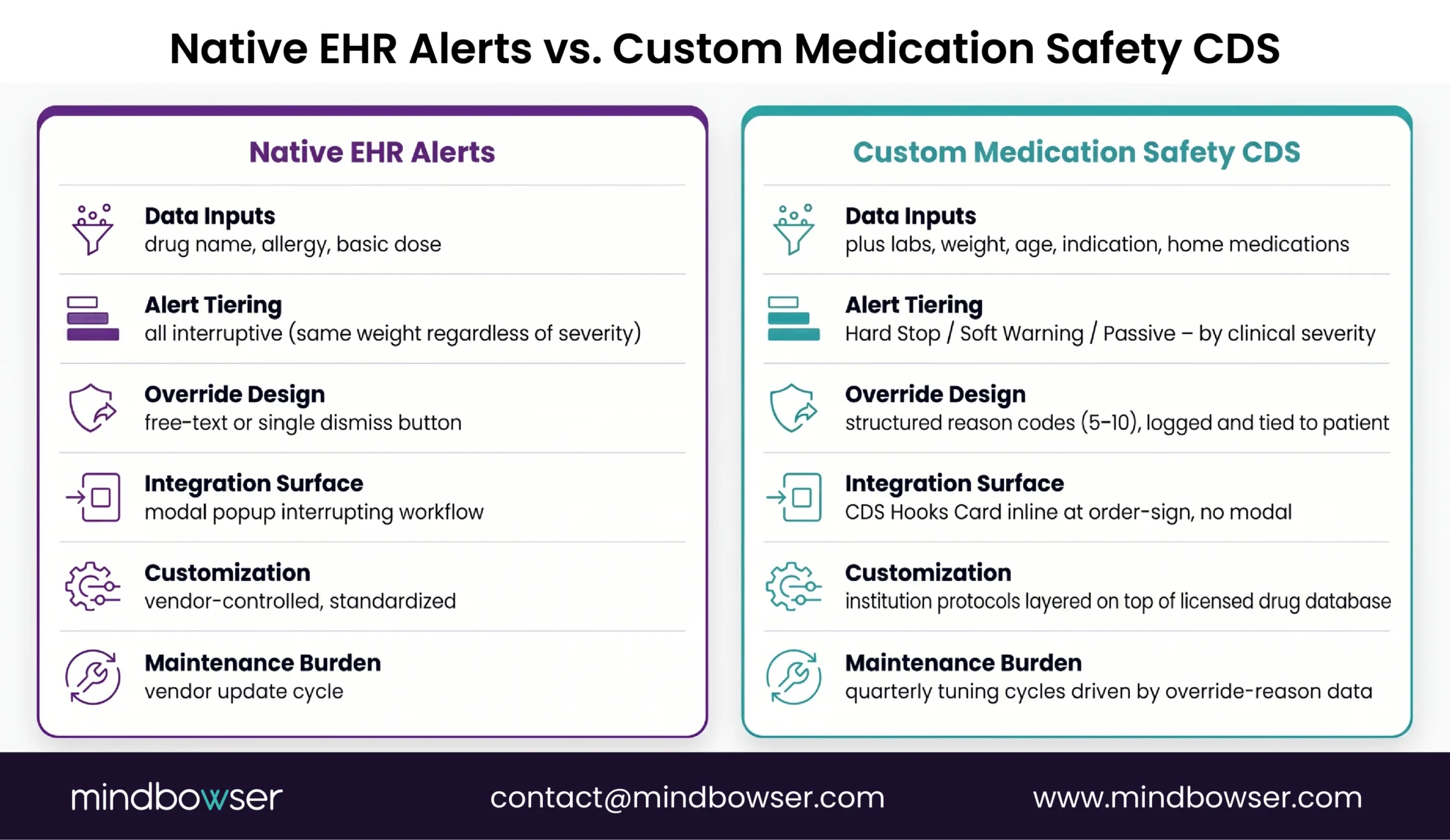
Medication safety clinical decision support is the layer of software that evaluates a drug order against a patient’s current medications, allergies, conditions, labs, and clinical context, at the moment of prescribing, and surfaces only the alerts that matter, in a form clinicians can act on. It includes drug-drug interaction checking, allergy cross-referencing, dose validation against patient-specific factors, and contraindication detection.
Two layers exist in most implementations, per AHRQ’s Making Healthcare Safer IV review of computerized CDS for medication errors. Basic CDS covers drug-allergy checking, basic dosing guidance, formulary decision support, duplicate-therapy checking, and DDI checking. Advanced CDS adds dose adjustment for renal insufficiency and geriatric patients, drug-disease contraindication, drug-pregnancy checking, and medication-related lab guidance.
A useful clarification I make with every buyer I talk to: a drug-interaction database is not a CDS. First Databank, Medi-Span, Micromedex, and Wolters Kluwer Lexicomp are content sources. The CDS is the integration layer, the rules engine, the alert design, and the workflow surface that wraps that content. Most hospitals already license one of those databases through their EHR. The pain is not the database. It is what surrounds it.
3. How Does CDS Hooks Solve the Medication-Safety Integration Problem?
This is where the persona shifts. I’m still writing from the clinical side, but what follows is the architecture our engineering team built solving this exact problem, and the pattern we apply to medication-safety implementations today.
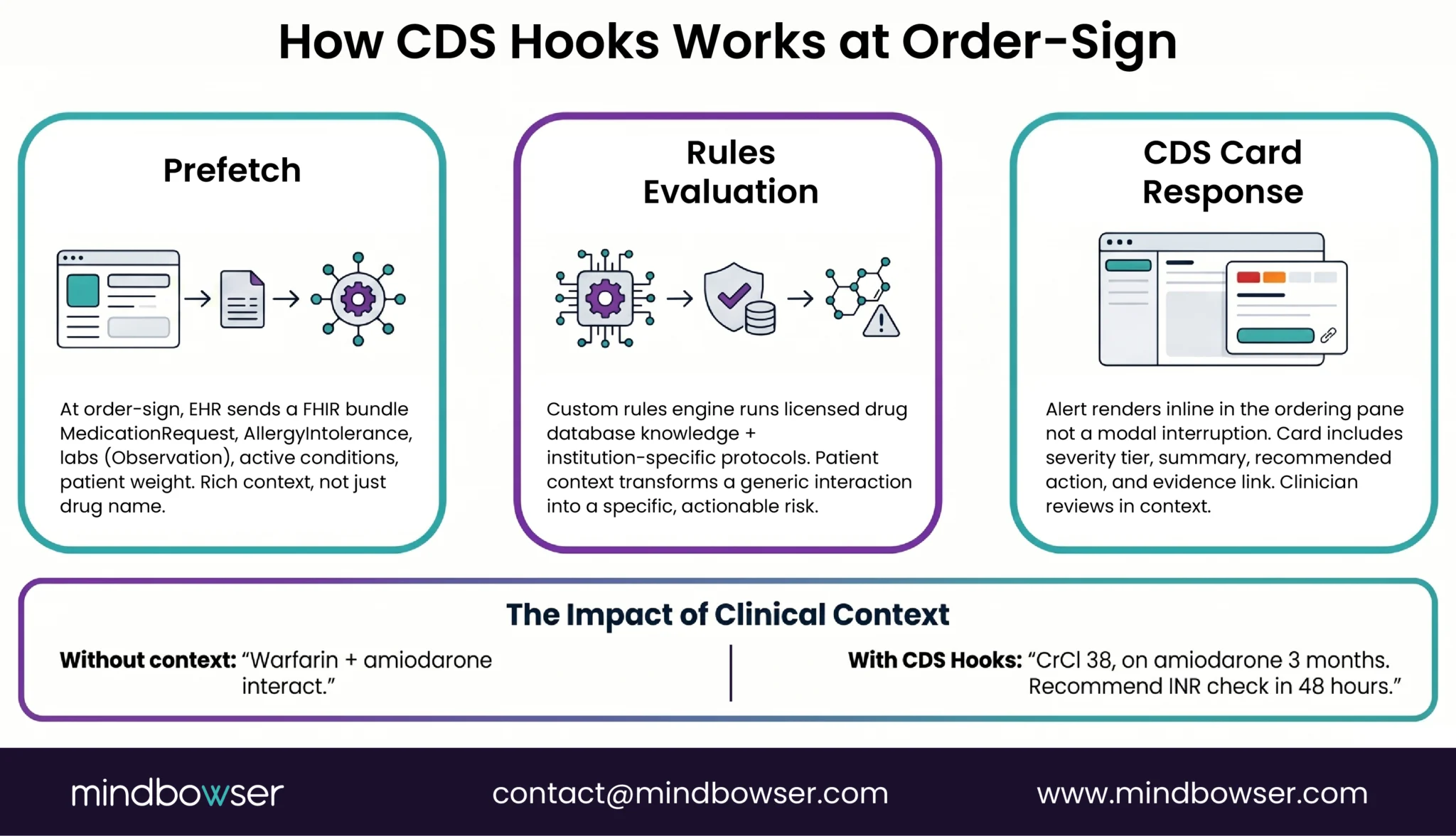
CDS Hooks is the HL7 specification that lets an EHR call an external decision-support service at specific workflow events, then display the response as a card inside the clinician’s screen. The mechanism that matters most for medication safety is the order-sign hook. It fires the moment a prescriber clicks Sign on a medication order, before the order is committed.
Three things have to happen well in the next half second.
- One: prefetch. The CDS service tells the EHR ahead of time which FHIR resources it needs. For medication safety that includes
MedicationRequest(the order being signed plus current orders),MedicationStatement(active home medications),AllergyIntolerance(the allergy list),Observation(renal function values, weight, recent labs), andCondition(active diagnoses such as pregnancy, kidney disease, liver disease). The EHR bundles those resources and ships them with the hook call. This is what makes the difference between an alert that says “warfarin and amiodarone interact” and an alert that says “this patient is on amiodarone, has a creatinine clearance of 38, and just had warfarin started; recommend INR check in 48 hours.” Same database. Different context. Different override rate. - Two: rules evaluation. The service runs the prefetch bundle through a rules engine. The engine evaluates against the licensed drug knowledge base (FDB, Medi-Span, Lexicomp, whichever the institution has) and against institution-specific protocols. Cardiology might have a custom rule for amiodarone-warfarin that the off-the-shelf database does not encode. Pediatrics has weight-based dosing logic. Oncology has chemotherapy-specific contraindications. The engine layers these on top of the licensed content.
- Three: response. The service returns a CDS Card. Not a modal. A structured object with a severity, a summary, a recommended action, and a link to evidence. The EHR renders it inline. The clinician sees structured guidance, not a popup that blocks the chart.
A 2022 JMIR Medical Informatics implementation study by Cho and colleagues at KAIST built exactly this architecture for drug-allergy interaction checking, using CDS Hooks order-sign with MedicationRequest and AllergyIntolerance prefetch. The paper confirms the pattern works in production. The detail they spent the most time on was not the rules logic. It was the prefetch contract and the alert-card design.
I will link to our CDS Hooks technical guide for readers who want to follow the protocol depth. The point here is that the integration mechanism is solved. The integration design is the work.
4. Why Tiered Alert Design Is the Hard Part, Not the Drug Database
Honest answer. You can buy the best drug knowledge base on the market. If you wire it into the same alert pattern your EHR already uses, your override rate will not move.
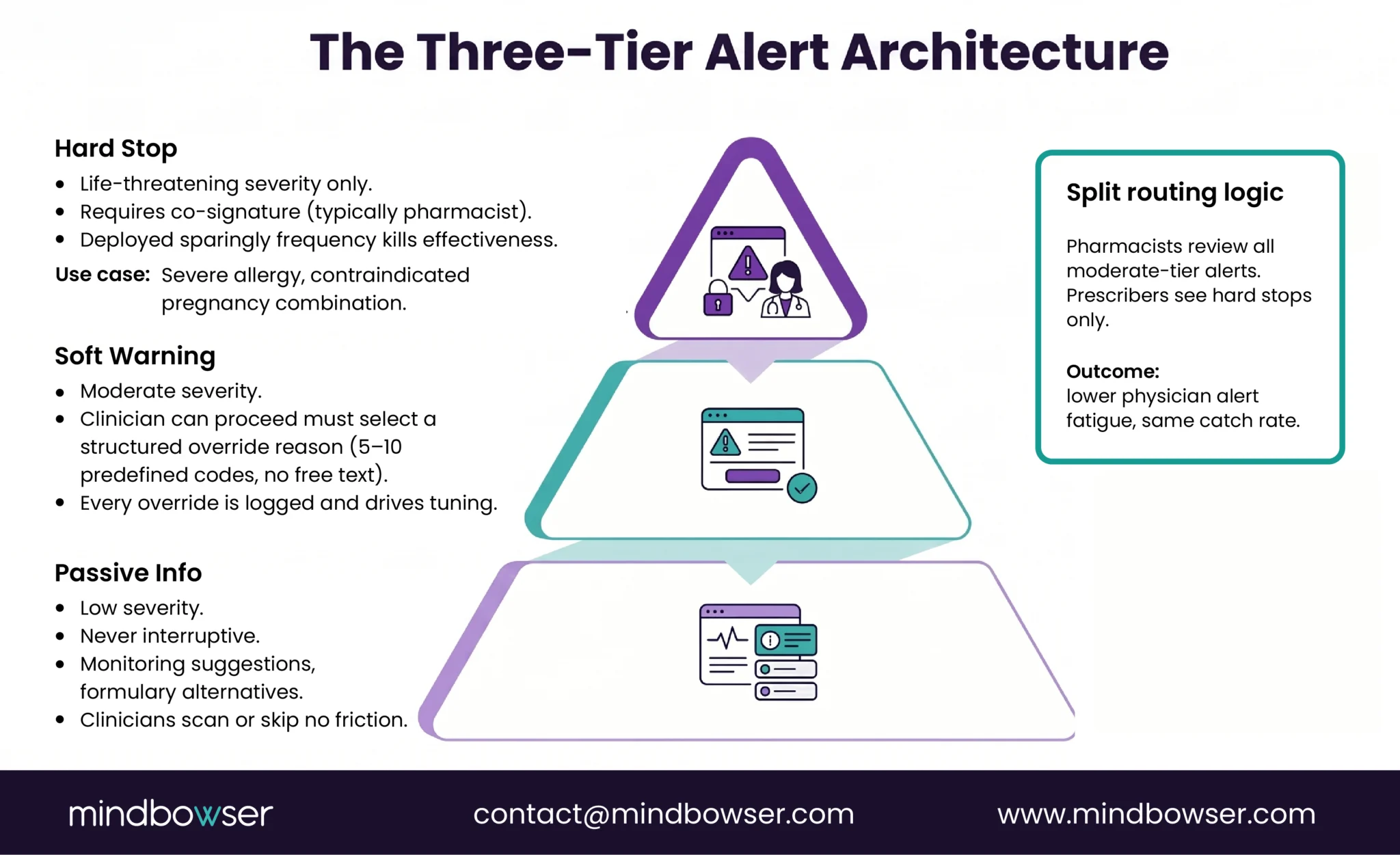
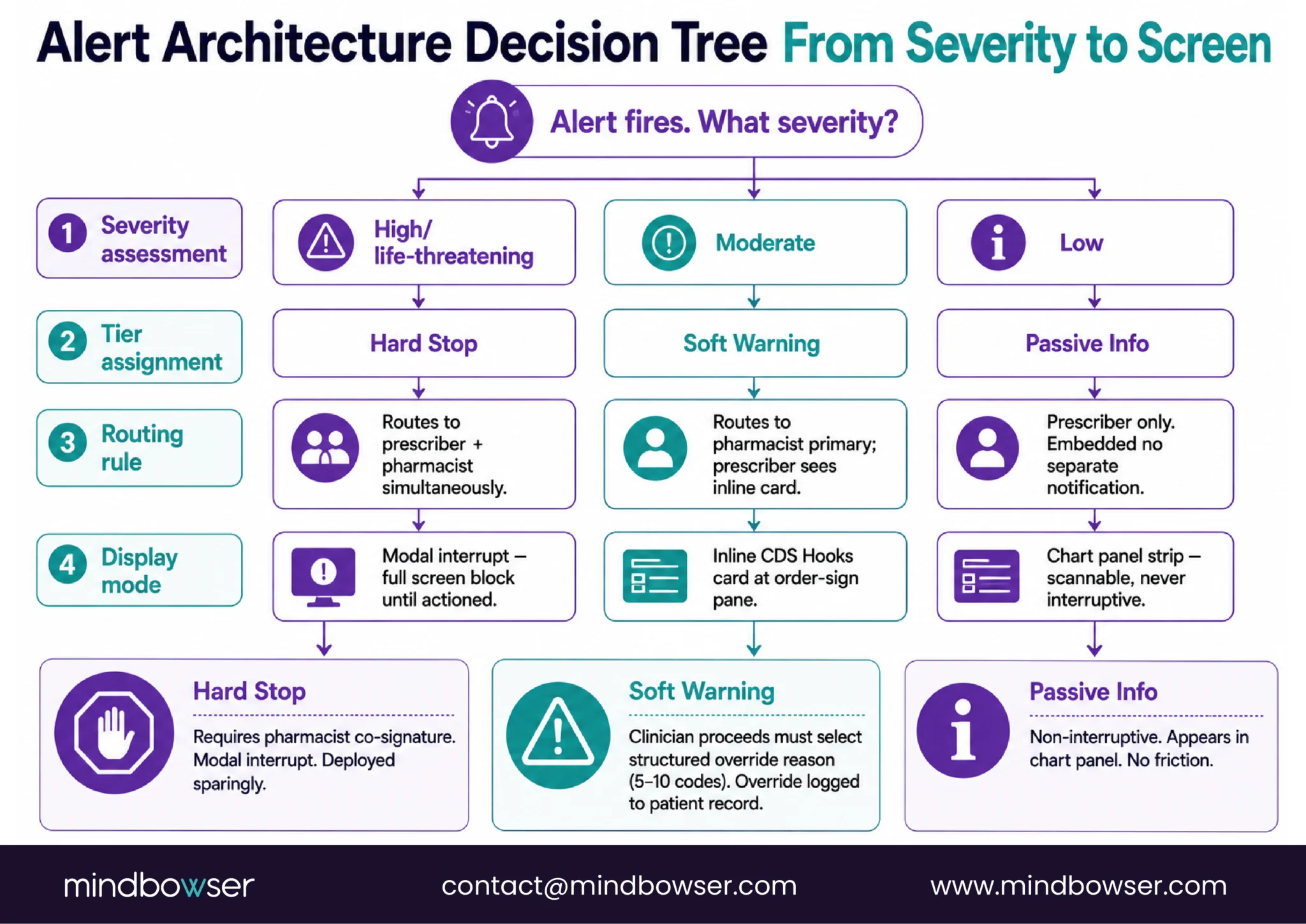
The pattern that does work has three tiers.
- Hard stop. Reserved for life-threatening interactions where the order should not proceed without explicit clinical reasoning. Example: a known severe allergy to a beta-lactam antibiotic, or a contraindicated drug combination in pregnancy. Hard stops require a co-sign, usually from a pharmacist, before the order commits. They are rare by design. If hard stops fire often, they stop being hard stops.
- Soft warning. The default for moderate interactions. The clinician can proceed, but the system requires a structured override reason from a short list (5 to 10 codes, not free text). The clinician picks the reason in one click. The reason is logged for audit and tuning.
- Passive info. Low-severity interactions, monitoring suggestions, formulary alternatives. Surfaced in the chart but never interruptive. The clinician can scan or skip without breaking workflow.
The routing layer matters as much as the tiering. A pattern documented in an AHRQ-cited Healthcare IT News piece and confirmed in several JAMIA override studies is the split-tier deployment. Some hospitals disable moderate alerts for physicians but keep them active for pharmacists. The pharmacist reviews and approves before the order commits. The physician sees only hard stops. Override rates fall on the physician side. Catch rates stay high on the pharmacist side. The system gets used because each clinician sees only what their role can act on.
This is also where the JAMIA Cho 2019 finding about 177 distinct override reasons becomes actionable. Most of those reasons were not relevant to DDI. They were generic excuses to dismiss a popup. A medication-safety CDS that ships with 177 free-text reasons is broken on day one. One that ships with 7 structured reason codes (“clinically appropriate,” “patient already on combination,” “monitoring planned,” “alternative not available,” “low risk for this patient,” “deferred to pharmacist,” “other (free text required)”) gives you data you can tune on. The override-reason data tells you which alerts to retire, which to retier, which to route differently.
One preoperative-labs CDS Hooks implementation hit strong provider engagement not because we had a better lab database, but because we got this layer right. The same design discipline transfers to medication safety. We start by reading the override-reason data on top alerts the institution has live, and the redesign writes itself.
If alert fatigue is the symptom, this is the design layer where it gets reduced.
Build Smarter Medication Safety CDS With CDS Hooks, Tiered Alerts, And Clinician-reviewed Logic.
5. Where Do Commercial DDI Databases Fit in a Custom Medication-Safety CDS?
Most hospitals I talk to already license a drug knowledge base. The buyer question is rarely “replace the database.” It is “how do I get more out of the one I already have.” That is the right question.
Commercial drug content covers roughly 80 percent of common interactions reliably. The gap is institution-specific protocols. Formulary alternatives change quarterly. Specialty restrictions exist for a reason and are not in any vendor’s standard package. A multi-site system might have one campus that does cardiothoracic surgery and another that does not, and the alert profile should differ.
The build pattern is straightforward. License remains the content source. The custom rules engine adds institution logic, severity tiering, and routing on top. The CDS Hooks service is the delivery mechanism. The clinician surface is institution-controlled.
I want to be honest about what we ship here, and what we do not.
Mindbowser does not have a packaged medication-safety CDS accelerator. Our HealthConnect CoPilot accelerator is the FHIR data layer that pulls MedicationRequest, AllergyIntolerance, and lab observations into the prefetch contract. That is plumbing, not the engine. Our AI Medical Summary accelerator can extract medication context from clinical notes (indication, dose history, prior reactions) when that context is not structured in the EHR; that is useful for richer rules evaluation, but again it is an input, not the engine.
The rules engine itself is a custom build. The tier logic is a custom build. The override-reason taxonomy is a custom build. The institution-specific protocol layer is a custom build. We model the build on proven implementation patterns and the JMIR 2022 reference, but the engagement is shaped to the institution’s licensed database, formulary, specialty mix, and pharmacy workflow.
There is no shortcut accelerator that compresses this work, and saying otherwise would be selling a story we cannot deliver.
That honesty is the position. The buyer making a build-versus-buy decision needs to know the database is not the differentiator, the build is. The build is what reaches 87 percent engagement.
6. Is Medication Safety CDS Regulated by the FDA?
This is the single biggest question I get from digital health companies building medication-safety products. Quick answer: most medication-safety alert software stays exempt from FDA device regulation; AI/ML CDS that processes images or signals does not.
The statutory ground is 21 USC 360j(o), the Section 3060 Non-Device CDS exemption of the 21st Century Cures Act. FDA’s interpretation lives in two guidance documents.
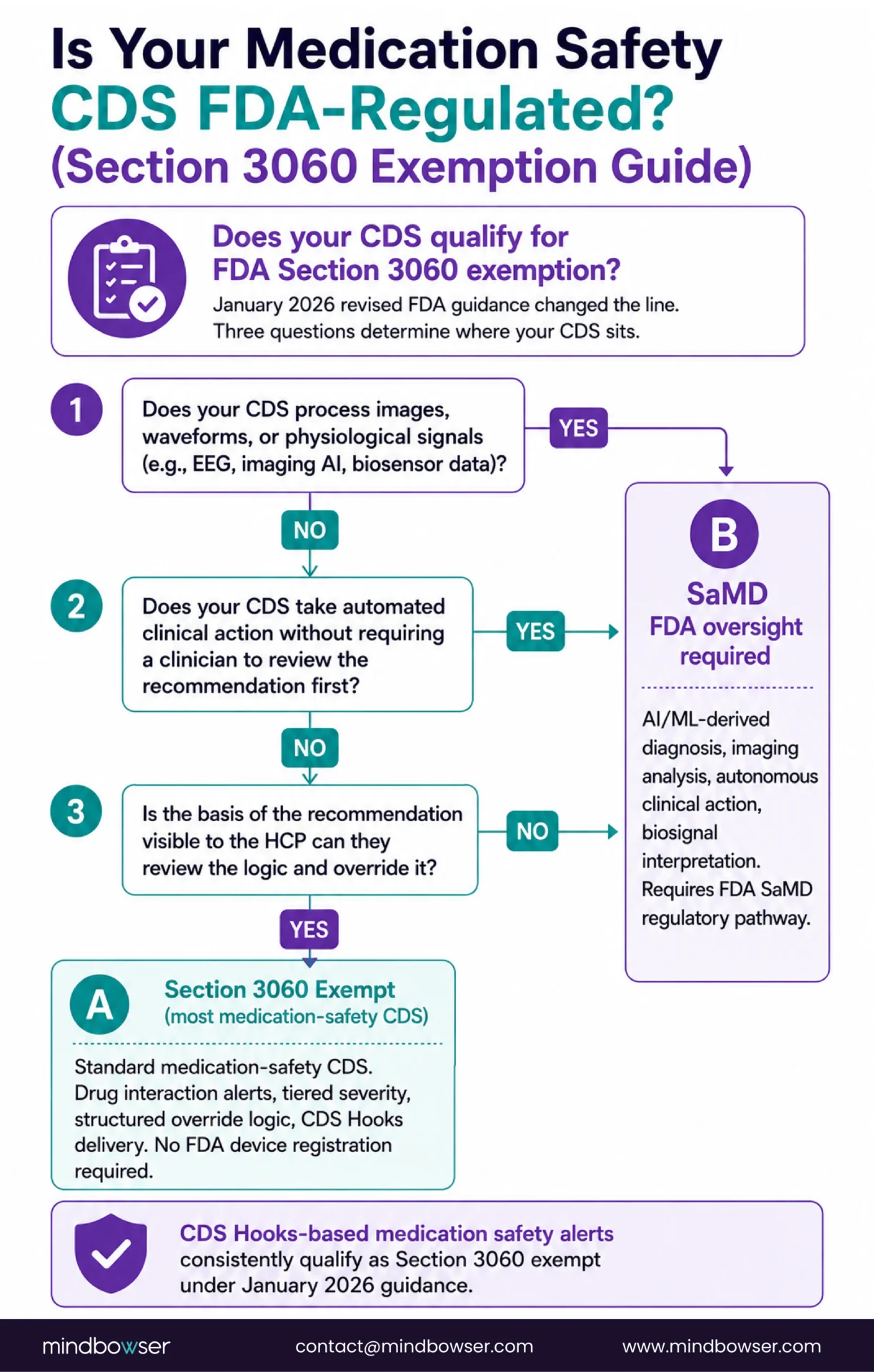
The September 2022 final guidance, Clinical Decision Support Software, set the four-criteria test. The CDS qualifies for exemption if it (1) does not process medical images, signals, or specimens; (2) displays, analyzes, or prints medical information; (3) supports or recommends to a healthcare provider regarding prevention, diagnosis, or treatment; and (4) is intended to enable the HCP to independently review the basis for the recommendation.
The January 6, 2026 revised guidance supersedes the 2022 version. Two practical changes for medication-safety builders. First, the revision explicitly allows single-recommendation CDS to qualify when only one option is clinically appropriate, which had been ambiguous before. Second, FDA put heavier emphasis on transparency and on avoiding time-critical reliance on opaque recommendations. The implication: a medication-safety CDS that surfaces a recommendation, shows the clinician the rule and the data the rule fired on, and lets the clinician decide, fits squarely inside the exemption.
Where it gets regulated. AI/ML CDS that processes signals (for example, an ECG-derived QT-prolongation alert that auto-suggests a dose change without clinician review of the basis) crosses into Software as a Medical Device territory. Image-derived medication recommendations (a dermatology AI suggesting a topical regimen from a skin photo) cross over too.
Adjacent rule. ONC’s HTI-1 Final Rule (89 FR 1192, Doc 2023-28857, effective February 8, 2024) requires certified health IT to disclose details about predictive and rule-based decision support interventions. If your medication-safety CDS runs inside a certified EHR, it falls under the DSI transparency requirements. The disclosure burden is documentation: source attributes, intended use, validation, fairness review.
Practical takeaway for the buyer. Most institution-built medication-safety CDS, with rule-based logic and clinician-reviewable basis, stays exempt. A digital health company commercializing a multi-tenant medication-safety product faces a sharper question: does any part of your decision logic process signals or images, and can the clinician review the basis for each recommendation? If yes-then-yes, exempt. If yes-then-no, plan for a 510(k) pathway and a quality system from day one.
7. What Does Building Medication-Safety CDS Look Like at a 250-Bed Hospital?
The shape of a real engagement, drawn from a live CDS Hooks deployment and adapted for a medication-safety scope. Phases vary. The skeleton is consistent.
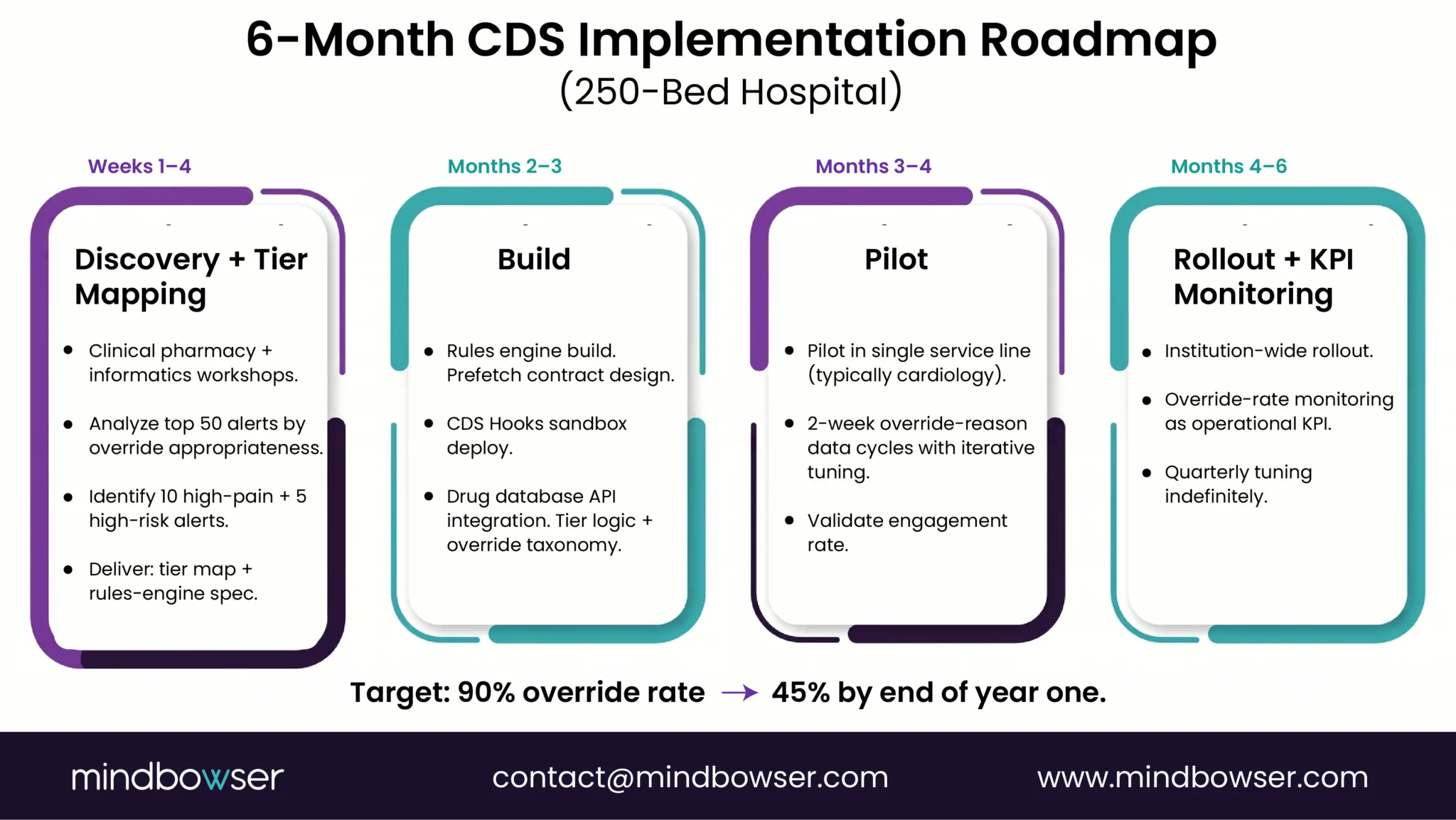
- Phase 1, weeks 1 through 4. Clinical pharmacy plus informatics workshops. We pull the override-reason data on the top 50 alerts the institution currently fires. We classify them by severity, override appropriateness, and routing pattern. We meet with the cardiology, oncology, and ICU pharmacists to identify the 10 alerts that cause the most pain and the 5 high-risk interactions that fire too rarely. The output is a tier map, a rules-engine spec, and a list of institution-specific protocols to encode.
- Phase 2, months 2 through 3. Rules engine build, prefetch contract design, CDS Hooks service deployed in the EHR sandbox. The HealthConnect CoPilot data layer is wired up. Drug knowledge base API integration. Tier logic encoded. Structured override-reason taxonomy locked. This is the bulk of the engineering work and runs in parallel with workshops continuing on edge cases.
- Phase 3, months 3 through 4. Pilot in one service line. Cardiology is a common starting point because the interaction landscape is well-understood and the volume is high enough to generate tuning data quickly. The NPI registry shows 7,486 cardiology organizations across the top 15 states, so the pattern is reusable. Pilot generates two weeks of override-reason data; we tune; we generate two more weeks; we tune again.
- Phase 4, months 4 through 6. House-wide rollout. Override-rate monitoring becomes the operational KPI. Quarterly tuning loop continues indefinitely. The system gets better with use, not worse.
A scope conversation about cost. I will not pretend there is a clean number that fits every institution. The licensed drug knowledge base typically costs less than 15 percent of total project spend. The custom rules engine, integration, tier design, workflow training, and tuning loop are the rest. A 250-bed Joint Commission, accredited hospital, with one EHR (Epic or Oracle Health), one drug content vendor, and one pharmacy informatics champion, runs the scope I described above. A multi-site system or a digital health vendor commercializing for multi-tenant use scales differently.
The KPI is override-rate improvement against an honest baseline. A preoperative-labs CDS Hooks implementation significantly reduced missed lab rates and reached strong provider engagement, not through a better database, but through the design discipline described above. The medication-safety equivalent is a bigger lift because the baseline override rate is higher. We aim to halve it in year one. That is realistic. Going from 90 percent override to 45 percent override is not just a metric change. It is the difference between a CDS clinicians ignore and a CDS clinicians use.
I will link to our advanced clinical decision support architecture write-up for readers who want the deeper technical layer.
What This Means for Your Build
If you take one thing from this piece, take the architecture, not the database choice. Native EHR drug-interaction checking is overridden 90 percent of the time because the alert pattern was designed in 1998 and not redesigned for the data we now have. CDS Hooks gives you the integration mechanism. Rich prefetch gives you patient context. Tiered alerts give you the clinician’s trust. Split routing gives the pharmacist the right work and the prescriber a quieter screen.
The drug database matters, but it is the smallest layer. The rules engine, the tier logic, the override-reason discipline, and the workflow surface are where override rates fall.
If you are a CMIO or a chief pharmacy officer evaluating whether to expand a commercial DDI license or build a custom medication-safety layer, the answer is usually both. License the content. Build the surface. The pattern works. We can show you what that build looks like at your scope.
Request an Assessment. A 30-minute scoping conversation, your override data plus our build pattern, no obligation. Start a Conversation here.
Conclusion
A 90% override rate is not a clinician problem. It is an architecture problem. Native EHR drug-interaction checking was designed for compliance, not for clinical action, same severity tier for every alert, no patient context, no distinction between pharmacist and prescriber routing. Closing that gap requires three decisions made in sequence: which drug knowledge base covers your formulary, how your rules engine maps dose, renal function, and patient context into severity tiers, and how alert UX splits the routing so the right clinician sees the right card at the right workflow step. The drug database is the commodity. The architecture is the differentiator. Most implementations that reach sub-30% override rates do it without a 510(k), the Section 3060 exemption holds when clinicians can review the basis for each recommendation. Build for that from the start.
A 2024 systematic review by Felisberto and colleagues found physician alert override rates run at 90 percent (95 percent CI, 85, 95 percent). The cause is not clinician indifference. It is alert design. Native EHR drug-checking ships with all alerts interruptive, no severity tiering, no patient context, and free-text override reasons. The 2019 Cho JAMIA study cataloged 177 override reasons across 10 sites; most were unrelated to drug interactions. Clinicians override because the alerts arrive without the context that would make them actionable.
Native checking uses the drug name, allergy list, and basic dose against a vendor-controlled rule set, all interruptive. Custom medication-safety CDS adds patient context (labs, weight, renal function, indication, current home meds), severity-based tiering (hard stop, soft warning, passive), structured override reasons, split routing for pharmacists versus prescribers, and institution-specific protocols layered on top of the licensed drug knowledge base. The license is the same. The surface is different.
CDS Hooks is the HL7 specification for invoking decision support at workflow events. The order-sign hook fires when a prescriber clicks Sign on a medication order. The EHR sends a prefetch bundle (MedicationRequest, AllergyIntolerance, Observation for renal/labs, Condition) to the CDS service. The service evaluates against the rules engine and returns a CDS Card with severity and recommendation. The card renders inline in the EHR. No popup. No workflow break.
Most medication-safety CDS qualifies for the Section 3060 Non-Device CDS exemption. The FDA’s January 2026 revised guidance kept the four-criteria test (no image or signal processing, displays medical info, supports the HCP recommendation, lets the HCP review the basis) and clarified that single-recommendation CDS can qualify when only one option is clinically appropriate. AI/ML CDS that processes signals or images, or that auto-actions without clinician review, falls under SaMD regulation and follows a 510(k) pathway. ONC’s HTI-1 Final Rule adds DSI transparency requirements for CDS running inside certified EHRs.
Cost is scope-driven, not packaged. The licensed drug knowledge base (FDB, Medi-Span, Lexicomp) is typically less than 15 percent of total project spend. The custom rules engine, CDS Hooks integration, tier design, override-reason taxonomy, pilot tuning, and workflow training are the rest. A 250-bed hospital with one EHR and one drug content vendor runs a six-month engagement. Multi-site systems and digital health vendors commercializing for multi-tenant use scale differently. The KPI is override-rate improvement against an honest baseline, not a feature checklist.

