



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
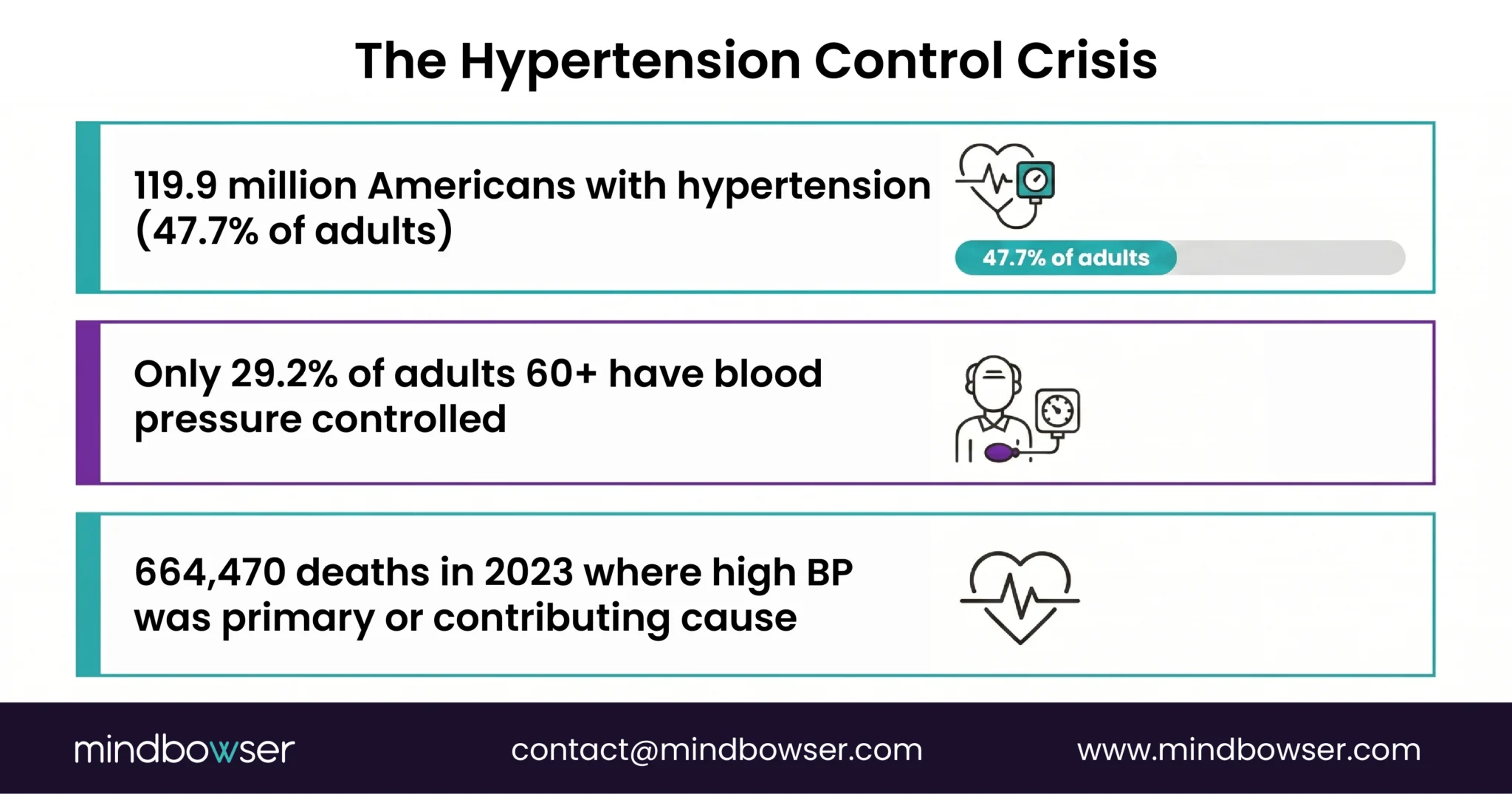
- 47.7% of US adults have hypertension, roughly 119.9 million people (CDC NCHS Data Brief #511, October 2024). Only 29.2% of adults over 60 have their blood pressure under control.
- RPM studies with 6,500+ patients show uncontrolled hypertension dropping from 66.3% to 40.2% (PMC, 2024). Stage 2 hypertension reduction of 75% over 12 months (AJMC, 2025).
- Treatment-resistant patients are hitting the target BP at a 74% rate within one year (AHA, 2024). Then, UnitedHealthcare announced, then paused, RPM coverage limits for chronic hypertension in 2026, keeping only heart failure and pregnancy-related hypertensive disorders.
- Medicare and most commercial payers still cover it. The evidence has never been stronger. The payer environment has never been more fragmented.
I’ve been advising health systems on RPM for years, and hypertension has always been the easy sell: 120 million Americans, simple device protocol, strong outcomes. Then UnitedHealthcare announced, then paused, RPM coverage limits for chronic hypertension in 2026, and every CFO I talk to wants to know if the program still pencils.
It does. But the answer requires more nuance than it did a year ago.
The clinical evidence for remote blood pressure monitoring is, frankly, better than anything I’ve seen for any other RPM condition. Heart failure included. The studies are large, the effect sizes are real, and the results replicate. What changed isn’t the evidence. What changed is one payer’s willingness to pay for it. And that distinction matters more than most coverage analyses acknowledge.
Why Is Hypertension the #1 RPM Use Case by Patient Volume?
The numbers are hard to argue with.
The CDC’s October 2024 data brief reports hypertension prevalence at 47.7% among US adults. That is 119.9 million people. Nearly half the adult population. Among adults 60 and older, prevalence hits 71.6%. High blood pressure was a primary or contributing cause of 664,470 deaths in 2023.
And here is the number that should concern every VP of Population Health: the control rate among adults 60 and older is 29.2%. That means 70.8% of hypertensive adults over 60, the population with the highest cardiovascular risk, have uncontrolled blood pressure. They are in your system. They have appointments. They get prescriptions. Their blood pressure is still not controlled.
The device protocol is the simplest in all of RPM. One blood pressure cuff. Two readings per day. Data flows to the care team. Compare that to COPD (four to five data streams) or diabetes (continuous glucose monitors generating 288 readings per day). Hypertension monitoring is the lowest-friction RPM entry point for any health system.
Every organization running chronic disease management already has these patients in their panels. They don’t need to find them. They need to monitor them.
What Does the Outcome Evidence Actually Show?
This is the strongest evidence of any RPM condition. And I am including heart failure in that comparison.
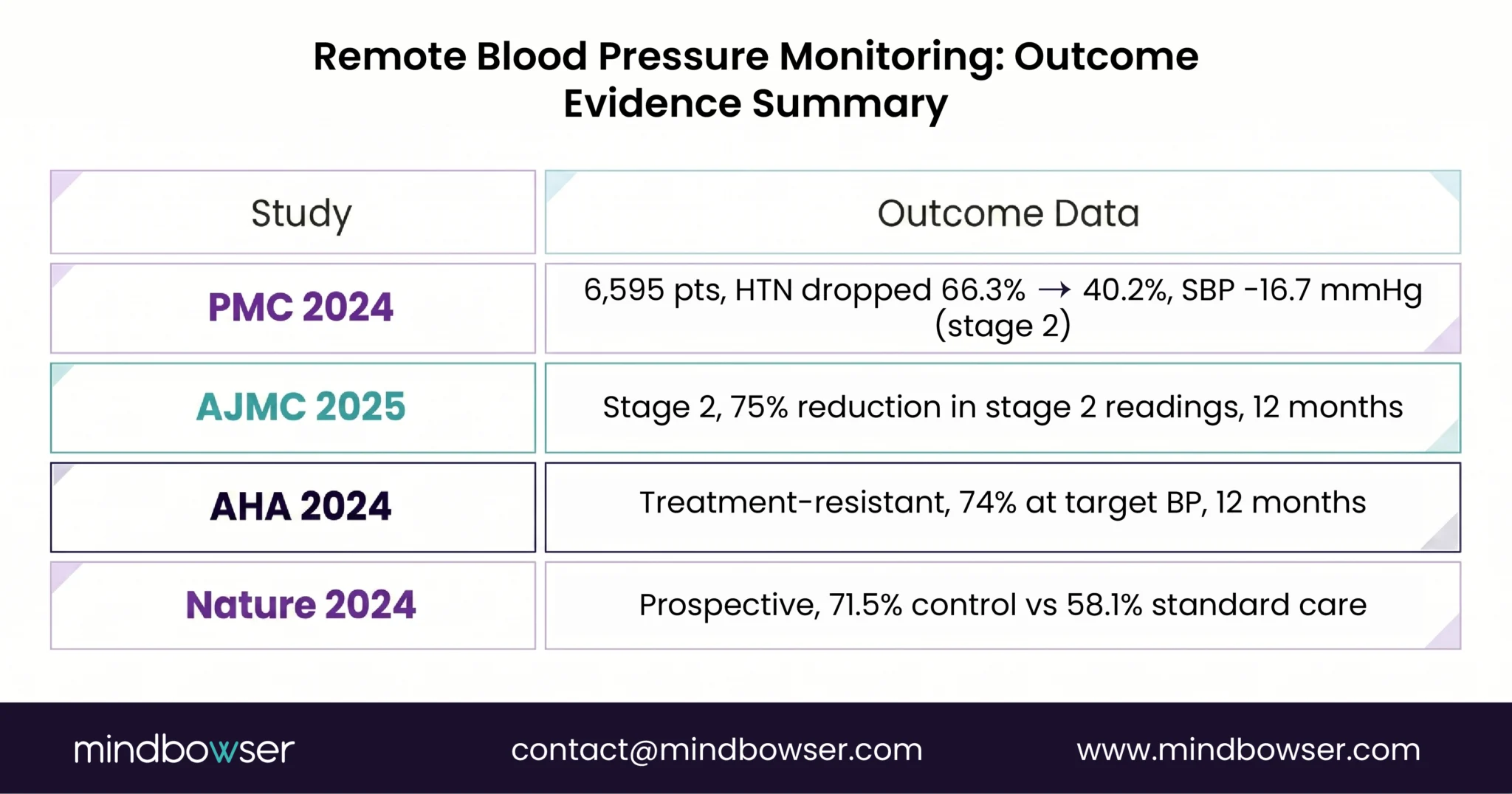
A large retrospective cohort analysis published in 2024 followed 6,595 patients on RPM for at least 90 days. The results: patients with uncontrolled hypertension dropped from 66.3% to 40.2%. That is a 26-percentage-point improvement. Systolic blood pressure improved by 7.3 mmHg across all patients and by 16.7 mmHg for patients with stage 2 hypertension. Mean arterial pressure improved by 8.5 mmHg in all patients with uncontrolled hypertension.
An AJMC study published in 2025 focused specifically on stage 2 hypertension and found RPM associated with a 75% reduction in stage 2 readings over 12 months. Seventy-five percent. In Medicare patients with care coaching, the reductions were statistically significant across every subgroup measured.
The American Heart Association published a 2024 study on treatment-resistant hypertension, the hardest population to treat. Remote blood pressure monitoring combined with pharmacist-led interventions resulted in 74% of patients achieving blood pressure below 140/90 mmHg within one year. Treatment-resistant. The patient’s other interventions had already failed.
A 12-month prospective cohort study published in Nature showed RPM patients achieved blood pressure control at 71.5% versus 58.1% for standard care. A 13-percentage-point gap that was clinically and statistically significant.
At BRI 2026, Jody Underwood and Tamika Rolle from St. Joseph’s presented their heart failure and hypertension RPM program data. The finding that stuck with me: patients NOT enrolled in RPM continued to have readmission rates above 20%. The enrolled patients dropped to single digits. Same patient population. Same hospital. The only variable was monitoring.
I should note what I find genuinely puzzling about the current moment. We have 6,500-patient studies showing 26-point improvements in hypertension control, 12-month data showing 75% stage 2 reduction, and a major insurer responding to this evidence by cutting coverage. I’ve been in healthcare long enough to know that evidence and coverage decisions operate on different timelines. But this gap is wider than usual.
What Blood Pressure Devices Work for Remote Monitoring?
The device decision for blood pressure RPM comes down to one question: does your patient population have reliable access to a smartphone?
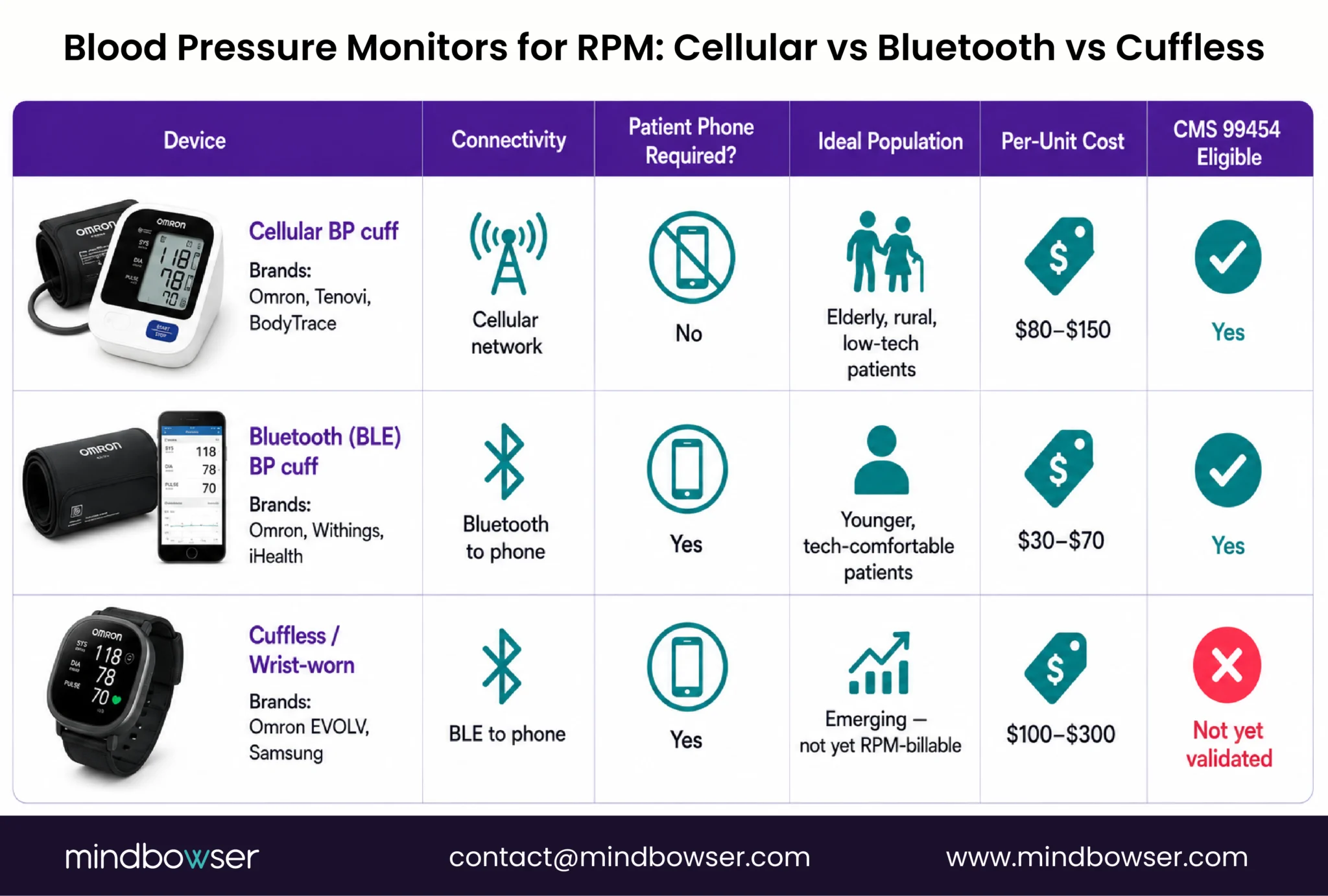
Cellular BP cuffs transmit data directly over the cellular network. No patient phone required. No app to install. No Bluetooth pairing to troubleshoot. The patient puts on the cuff, presses a button, and the reading appears in the care team’s dashboard. Omron, Tenovi, and BodyTrace make cellular-connected cuffs. For patients over 65, for rural populations with inconsistent WiFi, and for programs where you need the lowest possible patient friction, cellular is the right choice. Higher per-unit cost ($80-150), but the compliance gains are worth it.
Bluetooth (BLE) BP cuffs connect to the patient’s smartphone. The reading syncs to an app, which transmits to the monitoring platform. Lower per-unit cost ($30-70), wider device selection, but it introduces two failure points: the patient needs a compatible smartphone, and the Bluetooth pairing needs to work every time. For younger, tech-comfortable populations, BLE is fine. For the 71.6% hypertension prevalence in the 60+ population? Cellular wins.
Cuffless and wrist-worn monitors are emerging. Omron announced the EVOLV with AI-powered AFib detection in 2025. Samsung and Apple are investing heavily in wrist-based BP estimation. These are not yet clinically validated for RPM billing (CMS requires validated cuff measurements for 99454), but they will be within 2 to 3 years. Watch this space.
My recommendation for most programs: start with cellular cuffs for patients 60 and older (your largest hypertension cohort) and BLE cuffs for patients under 50. The compliance data from every program I’ve reviewed supports this split.
What Happened with UHC’s 2026 Coverage Rollback?
This is the story every RPM program director needs to understand clearly, because the headlines don’t capture the full picture.
In late 2025, UnitedHealthcare announced that starting January 1, 2026, RPM coverage would be limited to two conditions: heart failure and hypertensive disorders during pregnancy (Fierce Healthcare, 2025). Chronic hypertension, diabetes, COPD, and every other condition that currently generates RPM billing was excluded. UHC cited “insufficient evidence of efficacy.”
Then, in December 2025, UHC paused implementation after significant industry pushback. A new effective date has not been announced. The policy is in limbo.
Here is what this means practically.
If the policy takes effect as written, chronic hypertension RPM is not billable to UHC plans. That includes UHC Medicare Advantage, UHC Community Plans, and UHC commercial members. Roughly 50 million Americans are on UHC plans. For a health system where UHC represents 30% of the hypertension panel, that is a real revenue hit.
But Medicare fee-for-service still covers hypertension RPM. So do Aetna, BCBS, Cigna, and most state Medicaid programs. The question isn’t whether hypertension RPM is viable. The question is what your payer mix looks like.
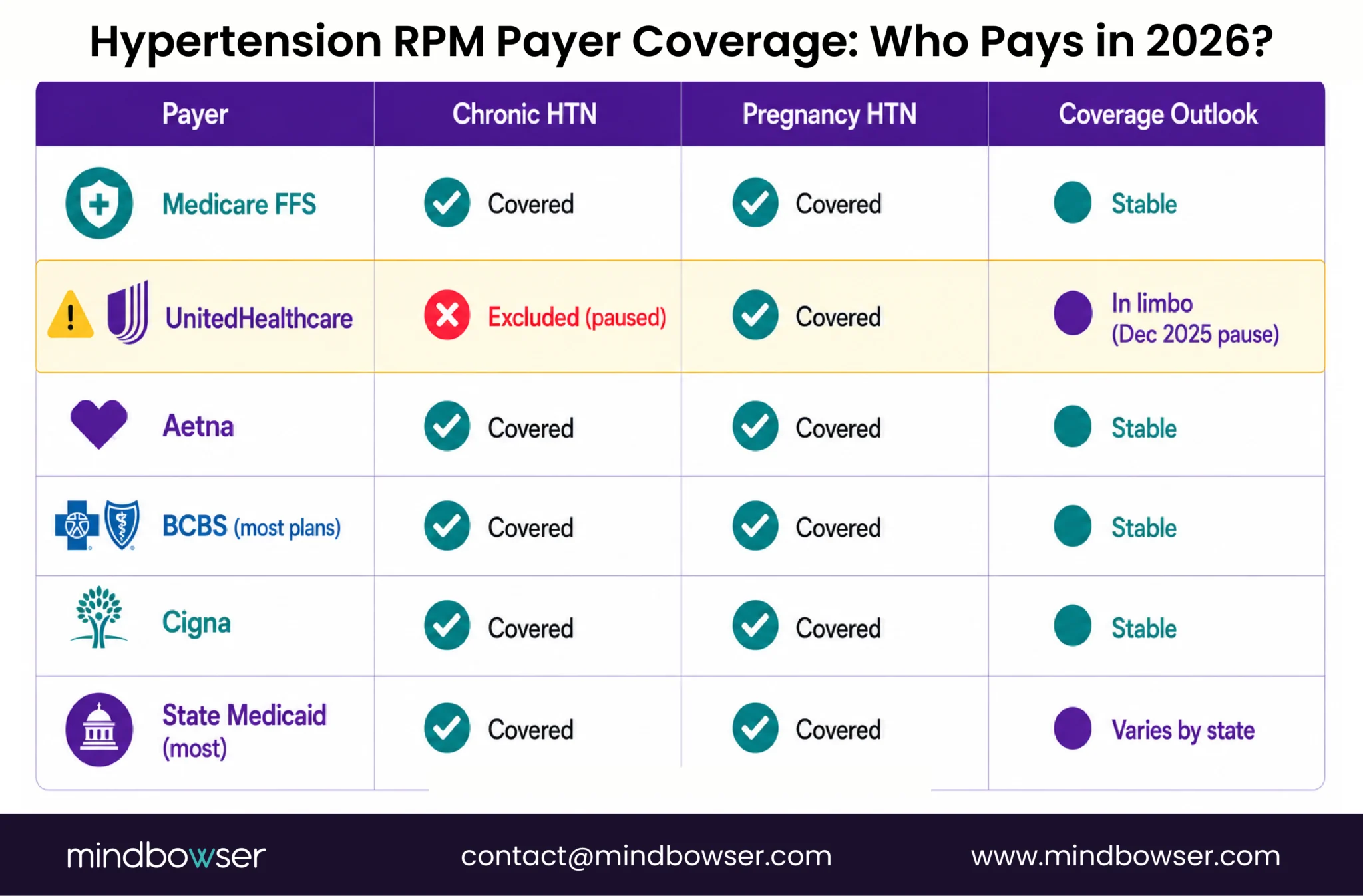
And there is a specific angle worth noting. UHC’s policy explicitly covers “hypertensive disorders during pregnancy” for RPM. If you run a maternal health program, hypertensive pregnancy monitoring (preeclampsia, gestational hypertension, chronic hypertension in pregnancy) is still billable to UHC. More on that in the next section.
I’ll say plainly what many in the industry are thinking: UHC cited insufficient evidence for a condition where we have 6,500-patient retrospective studies, 12-month prospective trials, and AHA-published data on treatment-resistant populations. This is a coverage decision. Not an evidence-based decision. Whether the pause becomes a permanent reversal depends on how loudly the provider community pushes back.
Discuss Blood Pressure RPM Platform Architecture for Multi-condition Programs
How Does CMS Reimburse Blood Pressure RPM in 2026?
The billing structure is identical to all RPM conditions. What makes hypertension financially attractive is the patient volume.
Standard RPM codes: 99453 (setup, ~$19-21), 99454 (device supply, ~$55-64/month), 99457 (first 20 min interactive, ~$50-58/month), 99458 (additional 20 min, ~$42-48/month).
2026 short-duration Codes: New code 99445 covers 2-15 days of monitoring in a 30-day period at ~$47, lower than 99454 and mutually exclusive. The treatment management threshold drops from 20 minutes to 10 minutes. For hypertension patients who forget to take readings some days (common in the first month), this dramatically lowers the billing floor.
Revenue math at scale. Hypertension has the largest addressable RPM patient pool of any condition. The math at scale is different from COPD or diabetes programs.
| Patient Volume | RPM Only (99457+99454) | RPM + CCM Stacked | Annual Revenue Range |
|---|---|---|---|
| 200 patients | $105-122/pt/mo | $167-184/pt/mo | $252K – $441K |
| 500 patients | $105-122/pt/mo | $167-184/pt/mo | $630K – $1.1M |
| 1,000 patients | $105-122/pt/mo | $167-184/pt/mo | $1.26M – $2.2M |
At 1,000 hypertension patients with concurrent CCM enrollment, the program generates $1.26 million to $2.2 million annually. Factor in the UHC payer exclusion: if 30% of those patients are on UHC plans, reduce the RPM-only column by 30%. The CCM billing is unaffected by UHC’s RPM policy.
What About Pregnancy and Preeclampsia Monitoring?
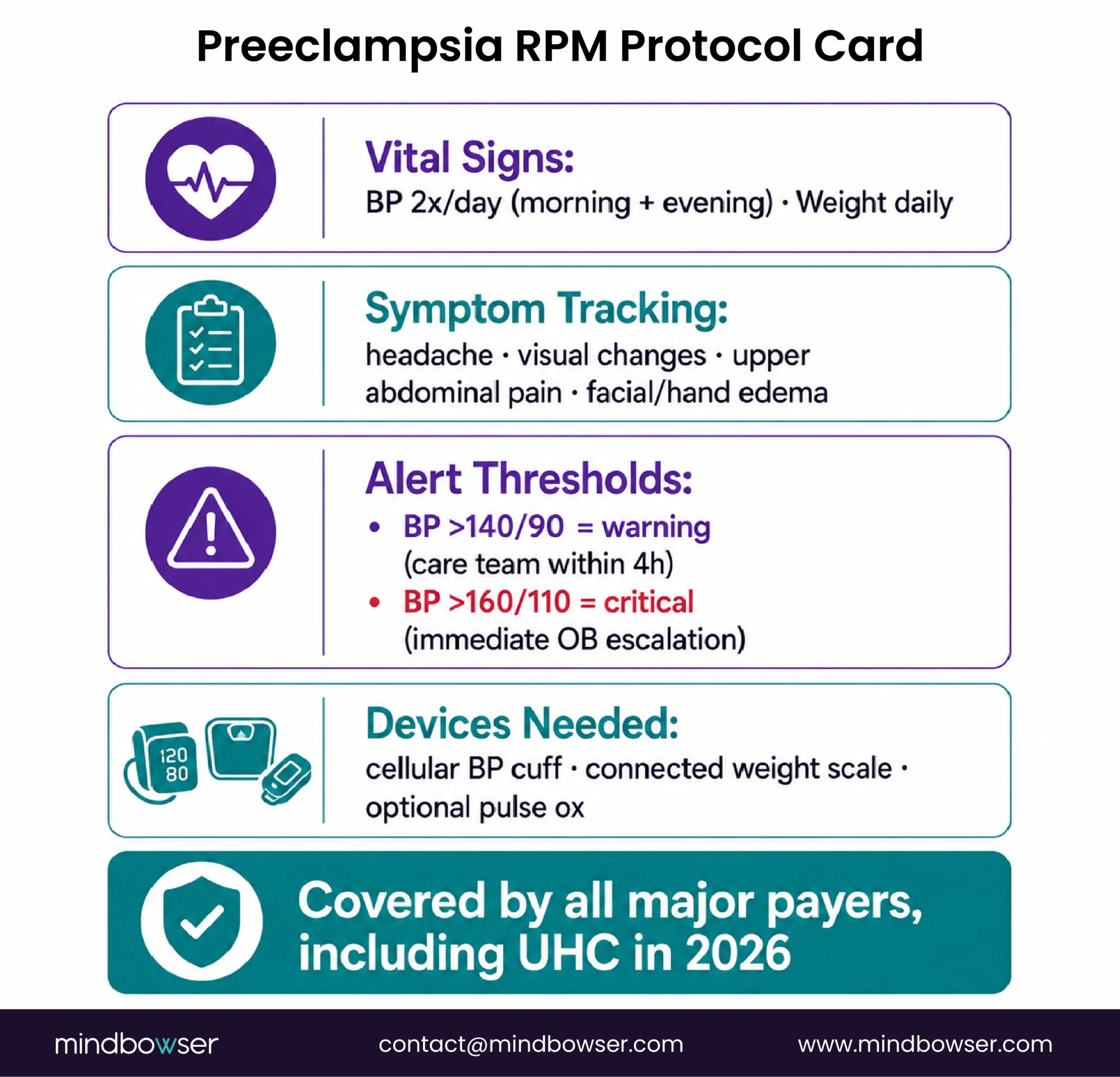
Preeclampsia affects 5 to 8% of pregnancies and remains a leading cause of maternal death in the United States. Remote blood pressure monitoring during pregnancy is one of the most clinically straightforward RPM applications, and it is one of only two conditions UHC explicitly covers for RPM in 2026.
The monitoring protocol is well-defined:
- Blood pressure: twice daily (morning and evening)
- Weight: daily (sudden weight gain of 2+ pounds in 24 hours or 5+ pounds in a week is a preeclampsia warning sign)
- Symptom questionnaire: daily check for headache, visual changes, upper abdominal pain, facial/hand edema
- Alert thresholds: BP above 140/90 mmHg (warning, care team notified within 4 hours). BP above 160/110 mmHg (critical, immediate escalation to OB provider)
The devices are simple: a cellular or BLE blood pressure cuff plus a connected weight scale. Some programs add a pulse oximeter for high-risk patients. Total device cost per patient: $100-200.
For health systems building or expanding maternal health programs, this is a green-light RPM use case under every major payer, including UHC. The clinical protocol is established. The billing pathway is clear. The patient population is identifiable (every OB practice screens for hypertensive risk factors at the first prenatal visit).
For digital health companies building maternal health platforms, BP-centered pregnancy RPM is the foundation layer. CGM integration for gestational diabetes (covered in our diabetes remote patient monitoring guide) adds a second data stream. Activity and sleep monitoring add a third. But blood pressure is where you start, because it is where the highest clinical risk lives.
We are planning a dedicated maternal RPM guide later this year covering the full pregnancy monitoring stack, including preeclampsia, gestational diabetes, and postpartum hypertension. For now, the key message: if you are deciding where to start with pregnancy RPM, start with blood pressure.
Should You Build a Custom BP RPM Platform or Buy Off-the-Shelf?
For single-condition hypertension monitoring with a standard device, off-the-shelf handles it.
CareSimple ranks #2 on Google for “remote blood pressure monitoring” and has built their platform specifically around BP and weight monitoring. HRS, Prevounce, and Tenovi all offer competent hypertension RPM modules. If your program enrolls one condition, uses one device type, and doesn’t need EHR-native dashboards, these platforms cover the use case at reasonable cost.
Where off-the-shelf breaks is the same place it always breaks: complexity, integration, and clinical workflow specificity.
Multi-condition monitoring. A hypertension patient who also has diabetes and CKD needs BP data plus glucose data plus weight data flowing into one clinical view with unified risk scoring. Three conditions, three device types, one patient. Off-the-shelf platforms handle each condition in its own module. Custom platforms unify the view.
Medication titration workflows. Blood pressure RPM is different from COPD or diabetes RPM in one important respect: the clinical response to abnormal readings is frequently a medication change. Titration protocols (increase lisinopril by 10mg if SBP remains above 150 for 5 consecutive days, for example) need to be embedded in the workflow, not just flagged as an alert. Most off-the-shelf platforms alert but don’t support structured titration decision logic.
EHR-native integration. If the cardiologist or PCP needs to see the 30-day BP trend inside Epic during a clinic visit, the data needs to land as FHIR Observations with trend annotations, not in a separate RPM portal. ConnectHealth handles this pipeline.
Pregnancy-specific workflows. Preeclampsia monitoring has different thresholds, different escalation timelines (4-hour response vs 24-hour for chronic HTN), and different clinical team routing (OB provider vs PCP). A program running both chronic hypertension and pregnancy hypertension needs workflow branching that most generic RPM platforms don’t support.
PatientWatch provides the real-time monitoring dashboard layer. For programs combining hypertension with other conditions, ConnectHealth normalizes the multi-device data stream.
What Should Your First 90 Days Look Like?
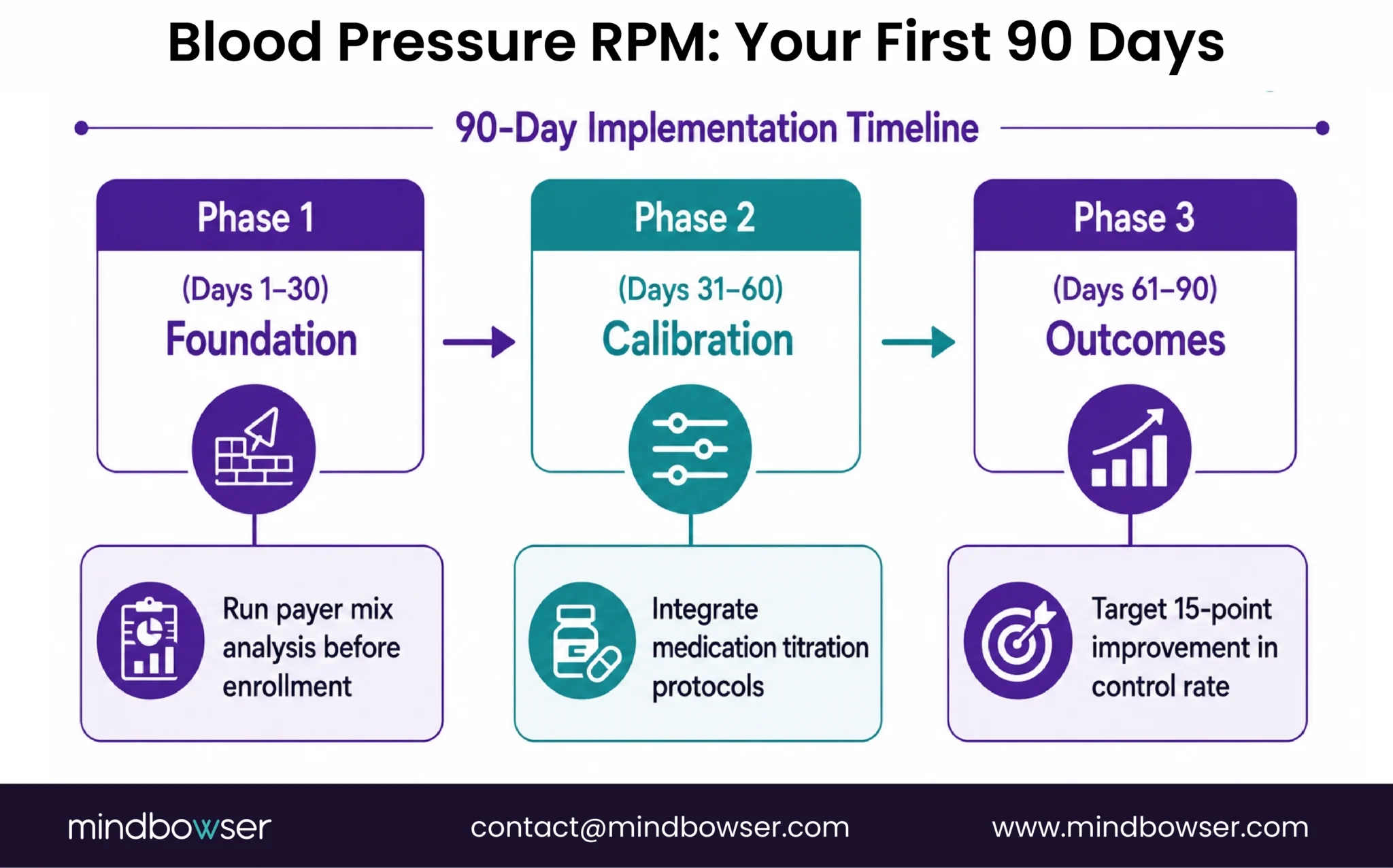
Hypertension RPM has the fastest path to measurable outcomes of any RPM condition. The device is simple, the patient pool is large, and the clinical response (medication titration) produces visible BP changes within weeks.
Phase 1: Foundation (Days 1-30)
- Select devices: cellular BP cuffs for patients 60+ (your largest hypertension cohort), BLE cuffs for patients under 50
- Run payer mix analysis: what percentage of your hypertension panel is on UHC vs Medicare FFS vs other commercial? This determines your revenue ceiling
- Enroll first 100 patients: start with stage 2 uncontrolled (SBP >140). These patients produce the most dramatic outcome improvements and the strongest data for program justification
- Set initial alert thresholds: SBP >160 critical, >150 elevated, <90 hypotension. Adjust after 30 days of real data
- Train care team on documentation for 99457 billing (interactive communication requires documented time)
Phase 2: Calibration (Days 31-60)
- Review alert accuracy and care team response patterns. Which alerts generated medication changes? Which were noise?
- Begin medication titration protocol integration: connect BP readings to titration decision trees in the clinical workflow
- Activate 99457 billing. First month of documented interactive time
- Identify concurrent CCM candidates (most stage 2 hypertension patients have comorbidities qualifying for 99490)
Phase 3: Outcomes (Days 61-90)
- Measure: what percentage of enrolled patients moved from uncontrolled to controlled? The 6,595-patient PMC study saw a 26-point improvement. Your program should target at least 15 points in the first 90 days
- Scale enrollment to 200+. At this volume, the revenue math supports a dedicated care manager
- Add comorbidity devices for qualifying patients (glucose monitors for diabetic hypertension, weight scales for CHF comorbidity)
- Begin the 2026 short-duration billing for patients who monitor inconsistently
The speed of this program is the selling point. Unlike COPD (where outcomes take 6+ months to demonstrate) or diabetes (where A1C is a 90-day lagging indicator), blood pressure responds to medication changes within 1 to 2 weeks. You can show measurable BP improvement in your first billing cycle.
The Evidence Speaks. The Payers Are Catching Up.
Hypertension RPM has the strongest outcome evidence of any remotely monitored condition. The numbers are not ambiguous. Uncontrolled hypertension reduced by 26 percentage points in a 6,595-patient study. Stage 2 hypertension down 75% over 12 months. Treatment-resistant patients hitting target at a 74% rate. Prospective data showing 71.5% control versus 58.1% at one year.
The payer environment is temporarily fractured. UHC’s pause on implementation suggests the policy may not hold in its current form. Industry pushback has been significant. But even if the policy takes effect, Medicare FFS and the majority of commercial payers still cover hypertension RPM. The math works for most programs. It just requires a payer mix calculation it didn’t require before.
I used to tell health systems to lead with heart failure RPM. Simpler to justify, established protocols, unquestioned payer support. The data has changed my mind. Hypertension should be the first RPM condition for most systems: simpler device, larger patient pool, stronger outcomes, faster time to measurable results, and the 70% uncontrolled rate in the 60+ population means you’re not searching for patients. They’re already in your system, with appointments scheduled, and blood pressure still not controlled.
If you’re trying to figure out whether your payer mix supports a hypertension RPM launch in 2026, I’d be happy to walk through the analysis. The calculation is straightforward. The numbers usually surprise people in the right direction.
Three types: cellular-connected cuffs (Omron, Tenovi, BodyTrace) that transmit readings directly over cellular networks without requiring a patient smartphone, Bluetooth cuffs (Omron, Withings, iHealth) that pair with a phone app, and emerging cuffless/wrist-worn monitors (Omron EVOLV) that are not yet validated for CMS RPM billing. For patients over 60, cellular cuffs produce higher compliance rates because they eliminate the smartphone and Bluetooth pairing steps.
Yes. Medicare fee-for-service covers hypertension RPM through CPT 99453 (setup), 99454 (device supply with daily recordings), 99457 (interactive communication), and 99458 (additional time). The 2026 short-duration code 99445 covers 2-15 days of monitoring at the same rate as 99454, lowering the billing floor for patients who monitor inconsistently. There are no condition-specific exclusions for hypertension under Medicare FFS.
As of April 2026, the status is uncertain. UHC announced in late 2025 that RPM coverage would be limited to heart failure and hypertensive disorders during pregnancy, excluding chronic hypertension. After industry pushback, UHC paused implementation in December 2025. A new effective date has not been announced. Programs should verify UHC RPM coverage on a per-patient basis and monitor for policy updates. Chronic hypertension RPM remains billable to Medicare FFS, Aetna, BCBS, Cigna, and most state Medicaid programs.
Standard RPM alert thresholds: systolic BP above 160 mmHg or diastolic above 100 mmHg triggers a critical alert requiring same-day clinical response. SBP above 140-159 or diastolic above 90-99 triggers an elevated alert for next-day review. SBP below 90 or diastolic below 60 triggers a hypotension alert. For pregnancy monitoring, the thresholds are tighter: BP above 140/90 is a warning (4-hour response), and above 160/110 is critical (immediate escalation). Programs should calibrate thresholds based on patient population and refine after 30 days of real data.
Large studies show substantial reductions. A 6,595-patient retrospective study found systolic BP improved by 7.3 mmHg across all patients and 16.7 mmHg for stage 2 hypertension, with uncontrolled rates dropping from 66.3% to 40.2%. A 2025 AJMC study reported 75% reduction in stage 2 hypertension over 12 months. The AHA published data showing 74% of treatment-resistant patients (the hardest to treat) achieved BP below 140/90 within one year when RPM was combined with pharmacist-led interventions.
Yes. Remote monitoring for preeclampsia uses twice-daily blood pressure readings, daily weight measurements (sudden gain is a warning sign), and daily symptom questionnaires (headache, visual changes, edema, upper abdominal pain). Alert thresholds are 140/90 mmHg for warning and 160/110 for critical escalation. Preeclampsia RPM is covered by all major payers including UHC in 2026, as “hypertensive disorders during pregnancy” is one of only two conditions UHC continues to cover for remote monitoring.
Cellular BP cuffs (Omron, Tenovi, BodyTrace) transmit data directly over the cellular network. No smartphone required, no app to install, no Bluetooth pairing. Higher per-unit cost ($80-150) but highest patient compliance, especially for elderly populations. Bluetooth cuffs connect to a smartphone app via BLE, which syncs data to the monitoring platform. Lower cost ($30-70) but requires a compatible phone and reliable Bluetooth pairing. For programs targeting the 60+ hypertension population (the largest cohort), cellular cuffs produce measurably better compliance and should be the default choice.


