BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
AI voice agents for healthcare are moving from call center automation tools to enterprise infrastructure supporting patient access, revenue protection, and value-based care performance. When deeply integrated with the EHR and deployed in high-volume workflows like scheduling, eligibility verification, and post-discharge outreach, voice AI can achieve 70%+ containment, reduce call volumes by 30-50%, and contribute to measurable improvements in quality metrics under risk contracts.
The key to ROI is disciplined deployment, HIPAA-compliant architecture, and clear executive KPIs tied to labor stabilization, booking lift, denial reduction, and readmission exposure. For health systems operating under value-based models, structured voice engagement is no longer optional; it is a margin protection strategy.
Section I: What AI Voice Agents for Healthcare Actually Mean for Health Systems
AI voice agents for healthcare are no longer pilot experiments. They are operational infrastructure.
If you lead patient access, IT, digital innovation, or revenue cycle, you already feel it. Call volumes are up. Staffing costs are rising. Patients expect 24/7 access. Meanwhile, value-based care contracts demand better follow-up, fewer readmissions, and measurable engagement.
This is the pressure point.
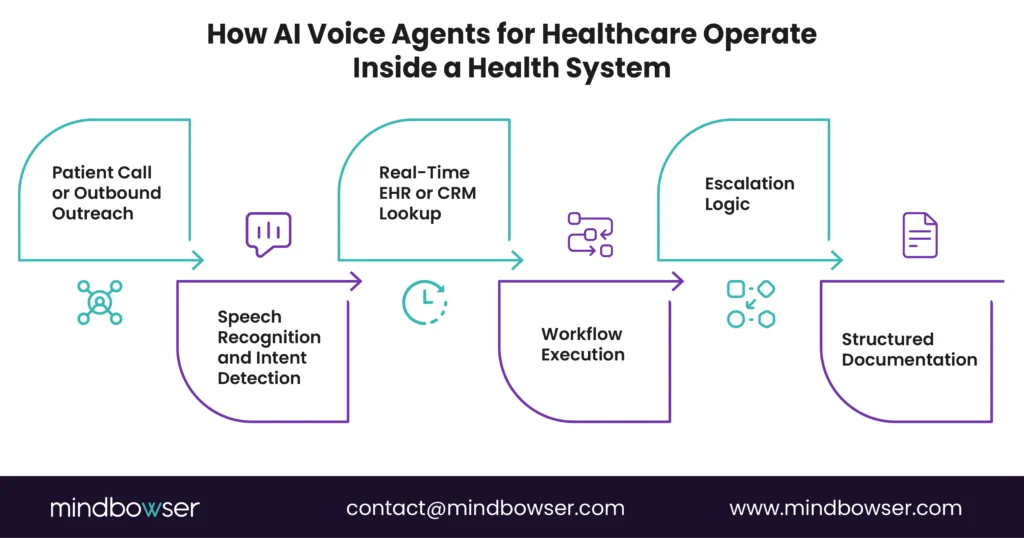
AI voice agents for healthcare sit at the intersection of patient access, call center automation, and quality performance. They answer calls, schedule visits, check eligibility, conduct outreach, and document interactions directly into your EHR or CRM. Not as a chatbot bolted on top. As an integrated, HIPAA-compliant voice AI layer embedded into your workflows.
Let’s define what that actually means.
A. From IVR Trees to Conversational Infrastructure
Most health systems still run on legacy IVR trees. Press 1. Press 2. Wait. Transfer. Repeat.
Patients drop. Agents burn out. Revenue leaks.
Voice AI healthcare replaces rigid scripts with natural language conversations. A patient says, “I need to see my cardiologist next week,” and the voice agent interprets intent, checks availability in real time, verifies insurance, and books the visit.
No menu maze. No hold music.
The contrast is simple:
- Old model: reactive, labor-heavy, limited hours
- New model: proactive, automated, 24/7 coverage
AI call center healthcare tools shift the voice from a cost center to a capacity engine.
B. Where AI Voice Agents Drive Measurable ROI
Executives evaluating AI voice agents for healthcare platforms want one answer: Does it move metrics?
The short answer is yes, when deployed in high-volume, rules-driven workflows.
Common high-impact use cases include:
- Appointment scheduling and rescheduling
- Eligibility and benefits verification
- Referral management
- Medication refill requests
- Post-discharge follow-up outreach
Mindbowser’s Voice AI use case analysis shows containment rates of 70%-85% in scheduling workflows, with a measurable lift in completed bookings and fewer abandoned calls. In VBC outreach programs, automated follow-up reduced avoidable readmissions and improved the capture of quality reporting.
This is where value-based care voice AI becomes strategic. Proactive voice outreach for preventive screenings, chronic care check-ins, and discharge follow-up aligns directly with HEDIS and CMS quality metrics.
C. Compliance Is Not Optional: HIPAA-Compliant Voice AI by Design
Now the risk question.
Voice conversations involve PHI. That means HIPAA, audit trails, encryption, access controls, and Business Associate Agreements.
A true HIPAA-compliant voice AI platform must include:
- End-to-end encryption
- Role-based access controls
- Detailed audit logging
- SOC 2 controls
- Clear data retention policies
If it cannot pass your security review, it cannot go live. Period.
This is where architecture matters. Custom-built, healthcare-native AI voice agents that integrate directly with your EHR and CRM stack, rather than routing PHI through generic consumer AI tools, reduce compliance exposure and improve operational control.
For CIOs and CTOs, this is not just a tech decision. It is a governance decision.
Related read: AI Agents in Healthcare: Top Use Cases and Leading Solutions
Section II: High-Impact Use Cases Where AI Voice Agents for Healthcare Deliver ROI
Not all automation is equal. Focus on volume, variability, and value.
If you are evaluating AI voice agents for healthcare, the fastest path to ROI is not broad deployment. It is precision deployment. Start where call volume is high, workflows are rules-based, and financial or quality impact is measurable.
That usually means patient access first. Then the revenue cycle. Then, value-based care outreach.
Let’s break it down.
A. Appointment Scheduling and Rescheduling: The Front Door Multiplier
Scheduling is the highest-volume workflow in most health systems. It is also where abandonment rates quietly erode revenue.
Patients call to book, change, or cancel visits. Agents toggle between EHR screens. Wait times stretch. Some patients hang up.
Voice AI healthcare platforms can:
- Interpret natural language requests
- Check provider availability in real time
- Apply scheduling rules
- Verify insurance
- Send confirmations via SMS or email
Healthcare IT News reports that organizations are achieving 30-50% call deflection in the early phases of AI deployment. In scheduling-specific workflows, containment rates can reach 70-85% when tightly integrated with the EHR.
That translates to:
- More completed bookings
- Fewer abandoned calls
- Lower average handle time
- Extended 24/7 coverage without overtime
For VP Patient Access leaders, this is capacity expansion without adding FTEs. For CFOs, it is incremental revenue capture.
Short version. Scheduling pays first.
B. Eligibility and Benefits Verification: Revenue Protection at Scale
Eligibility checks are repetitive, time-sensitive, and error-prone when manual.
Patients call to confirm coverage. Agents toggle between payer portals. Information is sometimes outdated. Denials increase.
AI call center healthcare systems can automate eligibility verification in real time through payer integrations, confirm co-pays, and document results directly into the revenue cycle system.
Impact areas include:
- Reduced front-end denials
- Faster registration workflows
- Shorter call durations
- Improved price transparency
For revenue cycle leaders, this is not just efficiency. It is cash flow stability.
C. Post-Discharge Follow-Up and VBC Outreach: Quality Meets Automation
This is where value-based care voice AI becomes strategic.
Under VBC contracts, health systems are accountable for readmissions, medication adherence, and preventive engagement. Yet manual outreach is inconsistent. Staff turnover disrupts continuity. Patients miss follow-up calls.
Voice agents patient access teams can deploy automated, conversational follow-up calls that:
- Confirm medication pick-up
- Screen for red-flag symptoms
- Schedule follow-up appointments
- Escalate high-risk responses to nurses
Becker’s Hospital Review reports that health systems are turning to AI‑driven engagement tools to strengthen patient navigation, improve adherence, and support value‑based care performance.
Containment rates for post-discharge follow-up average around 60-70%, with measurable reductions in avoidable readmissions when escalation protocols are embedded into care management workflows.
This is where automation supports outcomes, not just operations.
D. High-Impact Use Cases Comparison
Below is a structured view of where AI voice agents for healthcare drive the strongest early returns.
| Use Case | Containment Rate | ROI Impact | VBC Alignment |
| Appt Scheduling | 70–85% | +25% bookings | Preventive care |
| Eligibility Checks | ~80% | Revenue recapture | Access lift |
| Post-Discharge Follow-Up | ~65% | -15% readmits | Quality scores |
Interpretation for executives:
- Scheduling increases top-line revenue
- Eligibility protects the margin
- Follow-up outreach protects quality incentives and shared savings
Three levers. Revenue, margin, quality.
The common thread is integration. Containment rates drop fast when voice AI operates outside the EHR or lacks real-time data access.
Real-World Use Cases: AI Voice Agents in Action
To further illustrate the impact of AI voice agents, let’s explore how solutions are transforming healthcare workflows:
Use Case: AI Receptionist – Streamlining Patient Access
- Task: Handles call routing, appointment scheduling, and patient inquiries automatically
- Impact: Reduces call center volumes by 30-50%, decreases abandoned call rates, and improves patient booking completion
Use Case: AI Scribe – Reducing Clinician Burnout and Improving Documentation Accuracy
- Task: Automatically transcribes clinician-patient interactions into clinical notes
- Impact: Reduces manual documentation work, improves documentation accuracy, and ensures clinical quality metrics are captured for value-based care performance
Section III: HIPAA, Risk, and Architecture: What CIOs Must Validate Before Deployment
AI voice agents for healthcare touch PHI on day one. That makes compliance a board-level issue, not an IT experiment.
If a patient says their date of birth, diagnosis, insurance ID, or medication list, your voice AI platform is handling protected health information. There is no gray area.
So the question is not “Can it automate calls?”
The question is “Can it pass legal, security, and audit review?”
Let’s unpack what that means for CIOs, CTOs, and compliance leaders evaluating HIPAA-compliant voice AI.
A. HIPAA-Compliant Voice AI: What Legal Teams Now Expect
Healthcare organizations remain fully accountable for how AI vendors process, store, and transmit PHI.
In practical terms, your AI voice agent healthcare platform must provide:
- Signed Business Associate Agreement
- End-to-end encryption in transit and at rest
- Role-based access controls
- Detailed audit logs of every interaction
- Defined data retention and deletion policies
- SOC 2 Type II controls
If the vendor cannot demonstrate this in documentation and technical review, the deal stalls. Or worse, it moves forward and creates exposure.
Contrast matters here.
Consumer voice AI tools are built for convenience. Healthcare voice AI must be built for control.
That difference shows up in architecture.
Compliance is not a feature. It is the foundation.
B. Architectural Choices That Reduce Risk
Here is where technical leaders need clarity.
AI voice agents for healthcare typically include:
- Speech recognition layer
- Natural language understanding engine
- Dialogue management
- EHR or CRM integration layer
- Analytics and reporting dashboard
The risk question is simple. Where does PHI travel?
In poorly designed systems, voice data routes through third-party AI APIs that are not healthcare-specific. Data residency is unclear. Logging is incomplete.
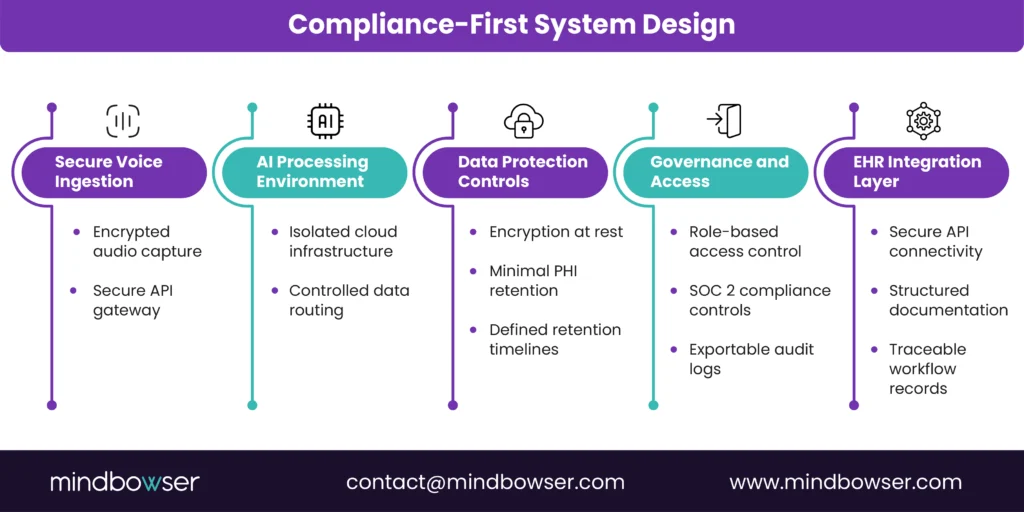
In healthcare-native architectures, the voice stack is designed with:
- Isolated environments
- Encrypted API gateways
- Secure EHR integration
- Minimal data retention
- Full traceability for audit review
For CTOs, this is not theoretical. It affects incident response plans, vendor risk scoring, and cyber insurance posture.
This works. Period. But only when the architecture matches the risk profile.
C. Integration Depth: The Hidden Compliance Multiplier
Compliance and integration are linked.
If your voice agent patient access workflow cannot securely write structured data back into the EHR, staff will resort to manual entry. That introduces errors. It also fragments the audit trail.
The lesson is clear. A voice AI tool that cannot integrate deeply becomes a silo. Silos create risk.
From an operations standpoint, integration also affects containment rates. When eligibility verification, scheduling rules, and provider availability are connected in real time, automation improves. When data is stale, transfers increase.
Risk and ROI move together.
D. Executive Risk Checklist Before Signing
Before approving an AI call center healthcare deployment, leadership teams should ask:
- Does the vendor sign a BAA and provide SOC 2 documentation?
- Where is PHI stored, and for how long?
- Can we restrict data retention?
- Are audit logs exportable for compliance review?
- What is the incident response protocol?
- How does the platform integrate with our EHR and CRM?
No shortcuts.
Ready to Integrate AI Voice Agents for Patient Access and Care Quality in 2026?
Section IV: Vendor Evaluation and Platform Selection: How to Choose AI Voice Agents for Healthcare That Actually Scale
Buying AI voice agents for healthcare is not a software purchase. It is an operational commitment.
You are not just evaluating features. You are evaluating:
- Compliance posture
- Integration depth
- Containment proof
- Financial return
- Multisite scalability
This is where many pilots stall. The demo sounds great. The ROI slide looks compelling. Then integration drags, containment underperforms, or compliance flags emerge late in the cycle.
Let’s bring structure to the evaluation.
A. The Executive Scorecard for AI Voice Healthcare Vendors
AI voice healthcare vendors are increasingly evaluated based on integration maturity, EHR connectivity, and ability to drive operational outcomes, rather than solely on conversational quality.
In other words, conversation alone is not enough.
Here is a weighted framework aligned to CIO, CTO, and revenue cycle priorities:
| Criterion | Weight | Key Metrics |
| HIPAA Compliance | 30% | SOC2, Audit Trails |
| Integration Depth | 25% | EHR/CRM APIs |
| Containment Rate | 20% | >75% proven |
| TCO / ROI | 15% | <6-month payback |
| Scalability | 10% | Multisite support |
Why this weighting?
- Compliance (30%) protects enterprise risk
- Integration (25%) drives operational performance
- Containment (20%) determines FTE displacement and cost savings
- TCO and ROI (15%) validate financial return
- Scalability (10%) ensures growth without reimplementation
Three filters. Risk, Return, Readiness.
If a vendor scores high in conversational fluency but low in EHR integration or audit traceability, it is not enterprise-ready.
B. Containment Claims vs. Proven Performance
Vendors will advertise containment rates of 80% or higher. The real question is: in what workflow, and under what integration conditions?
Containment depends on:
- Real-time EHR data access
- Accurate scheduling logic
- Up-to-date payer integration
- Clear escalation rules
If a voice AI healthcare platform cannot complete the full workflow without transferring to a human agent, containment erodes fast.
During evaluation, ask for:
- Use-case-specific containment benchmarks
- Production references in comparable health systems
- Metrics segmented by workflow, not blended averages
Blended numbers hide weak links.
From a call center operations perspective, even a 30-40% deflection rate can dramatically reduce queue times and burnout. But enterprise leaders need proof.
Show me the numbers in production.
C. Total Cost of Ownership: Beyond License Fees
AI call center healthcare investments are often evaluated against FTE reduction alone. That is too narrow.
A realistic TCO model includes:
- Platform licensing
- Implementation and integration services
- Ongoing model tuning
- Cloud infrastructure
- Internal governance oversight
Now contrast that with value drivers:
- Reduced live agent headcount growth
- Extended service hours without overtime
- Increased completed bookings
- Fewer front-end denials
- Reduced readmissions under VBC contracts
When deployments focus on high-volume workflows like scheduling and eligibility, sub-6-month payback is achievable in many mid-market health systems.
The CFO question is simple: Does this convert fixed labor cost into variable automation cost while preserving quality?
When done right, yes.
D. Multisite and Enterprise Scalability
Voice agents patient access leaders in multisite systems face a specific challenge. Standardizing workflows across hospitals, specialty groups, and ambulatory centers.
AI voice agents for healthcare must support:
- Site-specific scheduling rules
- Multiple EHR instances, if applicable
- Language support
- Call routing logic by geography or specialty
Scalability is not about call volume alone. It is about configuration flexibility without creating maintenance chaos.
For Directors of Digital Health Innovation, this becomes a platform decision. Choose once. Deploy many times.
Section V: Connecting AI Voice Agents for Healthcare to Value-Based Care and Enterprise ROI
This is where AI voice agents for healthcare shift from automation to financial strategy.
Most systems begin evaluating voice AI under patient access or call center efficiency. That is rational. Labor costs are rising. Call volumes are increasing. Staffing is unstable.
But under value-based care, access is not just operational. It is economic.
Every missed follow-up.
Every unclosed care gap.
Every undocumented outreach attempt.
They carry financial consequences.
A. The VBC Economics: How Voice AI Protects Shared Savings
Under downside risk and shared savings contracts, reimbursement is directly influenced by:
- Readmission rates
- Preventive screening completion
- Medication adherence
- Risk-adjusted quality scores
- Documented patient engagement
Manual outreach cannot scale to tens or hundreds of thousands of lives. Staffing grows linearly. Risk exposure does not shrink.
AI voice agents for healthcare change the operating model.
They can:
- Contact 100% of discharged patients within 24 to 48 hours
- Identify red-flag symptoms through structured conversational screening
- Rebook missed follow-ups immediately
- Document every attempt for quality reporting and audit defense
Consider the math:
- A 1% quality score lift on a $100 million VBC contract equals $1 million
- A 10% reduction in avoidable readmissions lowers penalty exposure
- Increased preventive compliance strengthens risk-adjusted revenue
Small percentage changes, large financial implications.
Value-based care voice AI industrializes engagement, protecting margins under risk.
B. The ROI Stack: Cost Stabilization, Revenue Lift, and Incentive Protection
CIOs and CFOs do not approve projects because they sound modern. They approve them because they move numbers.
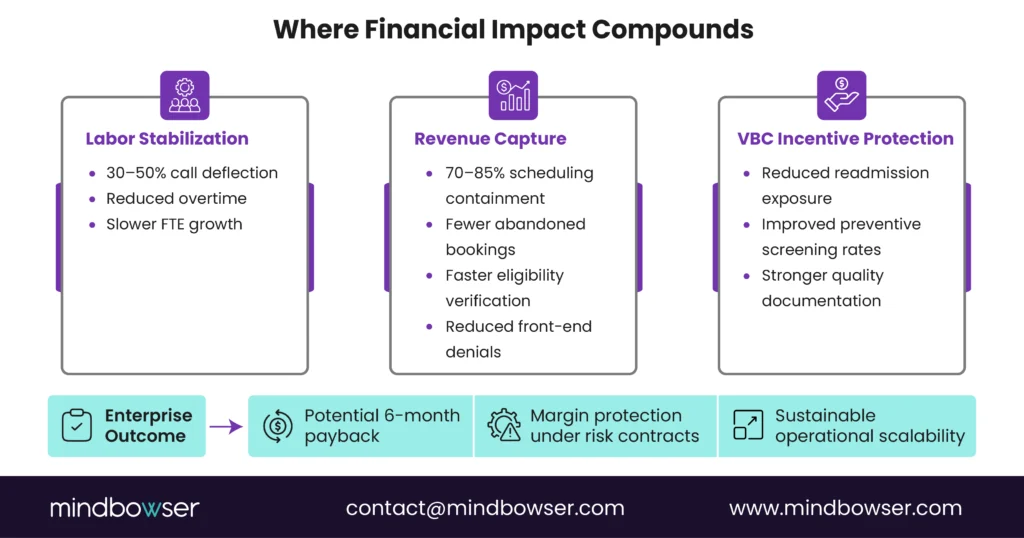
The financial impact of AI voice agent deployments in healthcare typically compounds across three layers.
1. Operating Expense Stabilization
- 30 to 50% call deflection in early deployment phases
- Reduced overtime
- Slower growth in call center FTEs
This does not always eliminate headcount. It prevents uncontrolled expansion.
For operations leaders, that means predictable staffing models.
2. Revenue Protection and Capture
When scheduling workflows reach 70% to 85% containment with deep EHR integration:
- Completed bookings increase
- Abandoned calls decline
- Eligibility verification accelerates
- Front-end denials decrease
Revenue cycle leaders see cleaner intake.
Access leaders see higher throughput.
This is not a theoretical lift. It is captured revenue that would otherwise leak away due to friction.
3. Quality Incentive and Risk Mitigation
For VBC populations, proactive voice outreach supports:
- Post-discharge follow-up completion
- Preventive care scheduling
- Chronic care engagement documentation
- Early identification of deterioration risk
Each of these ties directly to quality scores, shared savings eligibility, and penalty avoidance.
Individually modest gains can compound into meaningful shifts in contract performance.
Efficiency alone justifies investment.
Quality alignment accelerates return.
This works. Period.
C. Architecture as Financial Control
One nuance often overlooked at the executive level: AI voice agents for healthcare create structured engagement data.
Every conversation can:
- Update the EHR
- Log patient responses
- Time-stamp outreach attempts
- Trigger escalation workflows
- Feed performance dashboards
Under value-based contracts, documentation equals defensibility.
If outreach is not recorded, it does not count toward quality reporting. If escalation logic is unclear, liability risk increases.
For CIOs, this is systems orchestration.
For CFOs, this is revenue assurance.
For VBC leaders, this is gap closure at scale.
Three executive lenses. One platform decision.
D. Scaling Without Operational Shock
Enterprise rollouts fail when they expand too fast.
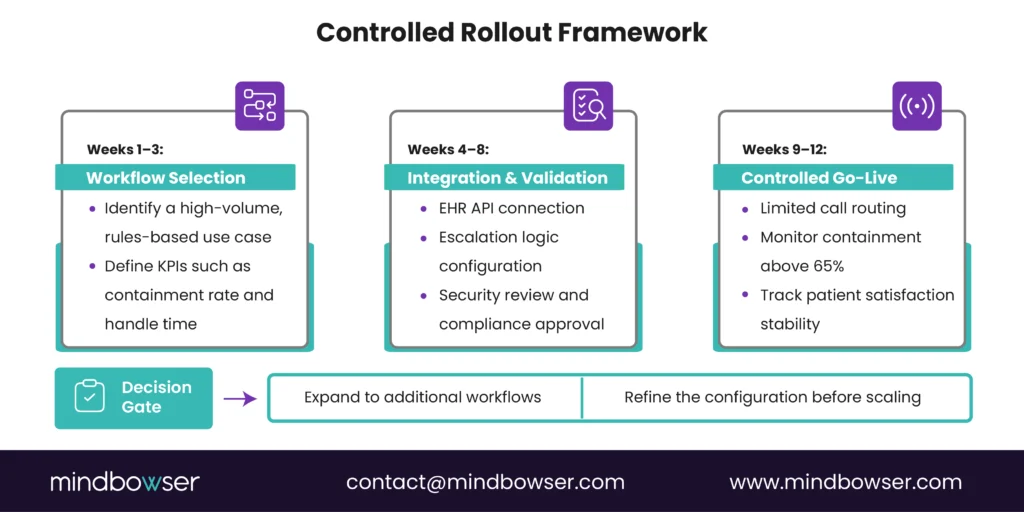
The disciplined path:
- Select a high-volume, rules-driven workflow such as scheduling or eligibility
- Define KPI thresholds before go-live
- Validate containment above 65%
- Confirm patient satisfaction stability
- Expand into adjacent workflows such as discharge outreach
AI call center healthcare platforms should prove performance before broad deployment.
Decision gates reduce political risk.
Measured expansion builds internal trust.
E. What This Decision Signals to Your Organization
Approving the deployment of AI voice agents in healthcare is not just a technology move. It signals operational maturity.
It says:
- Access is strategic
- Engagement must be measurable
- Automation must connect to the margin
- Compliance is engineered from day one
The systems that outperform under value-based care will not simply hire more staff.
They will structure engagement with discipline.
AI Voice Agents for Healthcare Are an Operating Decision
AI voice agents for healthcare have moved beyond experimentation and into enterprise strategy.
They stabilize patient access operations, reduce revenue leakage, and directly support value-based care performance under shared-savings and downside-risk contracts. For CIOs and CTOs, this is an integration and governance decision; for Patient Access and Revenue Cycle leaders, it is a throughput and margin decision.
Health systems that deploy intentionally will convert voice from a cost center into a performance lever, strengthening both operational resilience and financial outcomes under risk.
The main risk is uncontrolled PHI handling, so vendors must provide a signed BAA, encryption, SOC 2 controls, audit logs, and clearly defined data retention policies.
A focused pilot integrating one workflow can take 4-8 weeks, while enterprise-wide rollouts depend on EHR complexity and multisite configuration.
Health systems often see 70%+ containment in scheduling, 30-50% call deflection early on, reduced denials, and a six-month payback when labor savings and VBC incentives compound.
Pilot success should be measured by containment rate above 65%, reduced transfers and handle time, stable patient satisfaction, and measurable follow-up or readmission impact for VBC use cases.