



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
Clinical decision support systems (CDSS) fail when treated as alerts—and succeed when designed as workflow-driven, governed, and measurable capabilities. Most myths around CDSS stem from poor integration, over-alerting, and a lack of ownership, not technology gaps. For healthcare leaders in value-based care, the path forward is clear: focus on high-impact decision moments, embed CDSS into clinical workflows, and continuously optimize through governance and outcomes tracking.
What happens when your clinical decision support system is technically sound but clinically ignored?
Many healthcare leaders assume CDSS failures are a technology problem when in reality, they’re a design, workflow, and governance issue.
This piece debunks common misconceptions about Clinical Decision Support Systems (CDSS) through the lens of governance, workflow design, and the Five Rights framework, the foundation that determines whether CDSS deployments improve clinical adoption or create operational friction.
If you are evaluating whether CDSS investment is worth the cost and implementation effort, read our guide on whether Clinical Decision Support Systems are worth it. For a benefits-focused breakdown of measurable clinical and operational outcomes, see our article on the benefits of Clinical Decision Support Systems.
Watch: What Leaders Need to Know About CDSS Myths
I. Clinical Decision Support Systems: What They Are and Why Leaders Still Get Them Wrong
What happens when clinicians stop trusting your decision support system?
It doesn’t fail loudly. It fades quietly into overrides, workarounds, and ignored alerts.
That’s the real risk.
Despite years of investment, many health systems still misunderstand clinical decision support systems (CDSS) at a fundamental level. Not the technology. The role. The operating model. The business value.
CDSS doesn’t scale care; it scales consistency.
And consistency is what value-based care lives or dies on.
Yet most organizations treat CDSS like a feature, not a system. A tool, not a workflow. A build, not a capability.
If you define CDSS incorrectly, you deploy it incorrectly.
A. Clinical decision support definition (plain-English, executive-ready)
Let’s simplify what often gets overcomplicated.
A clinical decision support system delivers the right information to the right person at the right time, within the clinical workflow, to improve decision-making.
That’s it.
Not dashboards no one opens.
Not models sitting in isolation.
Not alerts firing without context.
Its decision influence at the moment matters.
1. What a CDSS is and what it is not
A true clinical decision support definition centers on action, not data.
It includes:
- Order sets that guide evidence-based care
- Risk scores embedded during ordering
- Care gap reminders tied to patient context
- Smart defaults that reduce variation
It does not include:
- Static reports reviewed days later
- Predictive models with no workflow trigger
- Alerts disconnected from clinician intent
And clinicians already have enough noise.
2. CDSS vs EHR vs pathways vs predictive models
Here’s where leaders often blur lines:
- EHR= system of record
- Predictive models = generate risk or probability
- Clinical pathways = define ideal care sequences
- CDSS = activates all of the above at the point of care
CDSS is the delivery mechanism, not the data source.
Think of it as the last mile.
If your predictive model identifies a high-risk patient but doesn’t trigger an intervention during discharge planning, you don’t have CDSS. You have analytics.
3. Where CDSS lives in workflows
This is where most implementations break.
CDSS must live inside:
- Order entry workflows
- Documentation moments
- Care coordination tasks
- Transition-of-care decisions
Not before. Not after.
Right there.
That gap? It’s not technology. Its placement.
CDSS succeeds or fails at the point of decision, not at deployment.
B. What is a clinical decision support system in modern VBC environments
If fee-for-service rewards volume, what does value-based care reward?
Consistency. Compliance. Outcomes.
That’s where clinical decision support systems become strategic.
1. CDSS as a VBC lever
In value-based care (VBC), every missed gap, every variation, every delay has a financial impact.
CDSS becomes the mechanism to:
- Close care gaps in real time
- Standardize evidence-based decisions
- Reduce avoidable utilization
- Support risk-adjusted documentation
- That distinction matters.
2. Where it impacts outcomes
When designed well, CDSS influences:
- Readmission reduction at discharge
- Sepsis early detection in ED workflows
- Medication safety during ordering
- Preventive care adherence in ambulatory settings
According to AHRQ, well-implemented CDSS can improve practitioners’ performance in up to 70% of reviewed studies.
That’s not marginal. That’s operational leverage.
But only when it fits.
3. Adoption challenges in VBC environments
Here’s the tension:
- You need standardization. Clinicians value autonomy.
- CDSS sits right in the middle.
Common challenges:
- Alert fatigue leading to disengagement
- Poor timing within workflows
- Lack of trust in data or logic
- No governance to refine rules over time
A widely cited JAMA study found that override rates for drug alerts can exceed 90%.
That’s not adoption. That’s avoidance.
In VBC, CDSS is not optional, but a poor CDSS is expensive.
C. The business case leaders care about
Let’s move from concept to boardroom.
Why should a CIO, CMIO, or VP Population Health invest here now?
1. Benefits of CDSS in healthcare (when done right)
The benefits of CDSS in healthcare are measurable when tied to workflows:
- Reduced clinical variation
- Improved quality scores (HEDIS, CMS measures)
- Lower readmissions and avoidable ED visits
- Safer medication practices
- Faster, more consistent decision-making
This isn’t theoretical.
It’s operational.
“CDSS turns guidelines into behavior.”
And behavior drives outcomes.
2. Metrics that actually matter
Too many teams measure activity. Few measure impact.
Track what matters:
- Acceptance rate (Did clinicians act?)
- Override rate (Did they reject it?)
- Time-to-decision (Did it speed care?)
- Outcome linkage (Did it change results?)
If you can’t tie CDSS to outcomes, you don’t have a business case. You have a feature set.
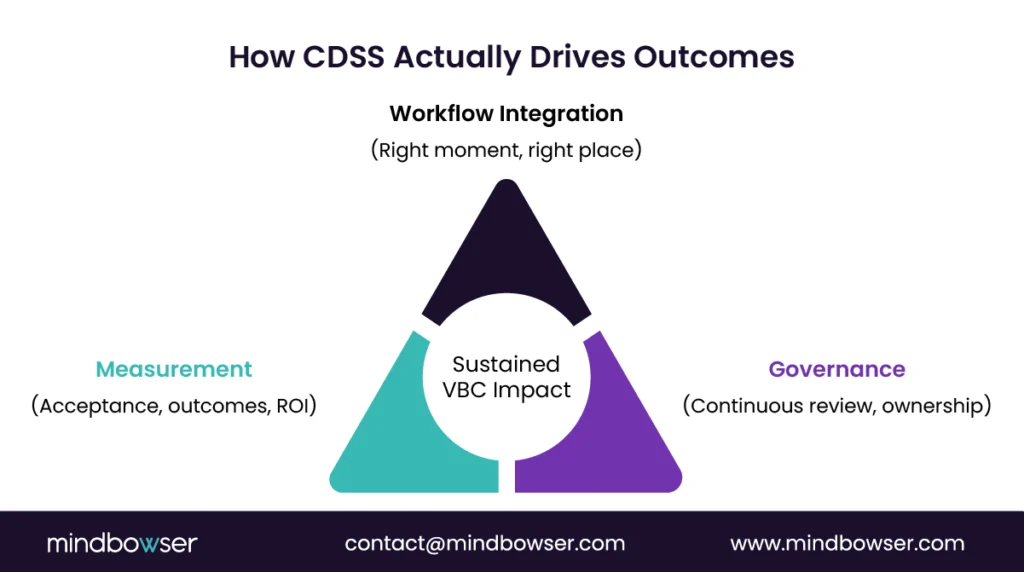
3. Governance as an operating model
Here’s the overlooked truth.
CDSS is not a build. It’s a living system.
Without governance:
- Rules become outdated
- Alerts multiply
- Trust erodes
High-performing organizations treat CDSS like a product:
- Clinical ownership
- Continuous review cycles
- Data quality validation
- Feedback loops from frontline users
“Governance is where CDSS either compounds value or compounds frustration.”
The ROI of CDSS is not in deployment. It’s in sustained relevance.
One last thought before we move on…
If your clinicians see CDSS as an interruption instead of assistance, the problem isn’t adoption.
Its design.
And that’s where the myths begin.
II. The 7 Myths About Clinical Decision Support Systems (and the Reality You Can Operate)
Why do so many CDSS investments stall after go-live?
Not because the technology fails.
Because the assumptions behind it do.
Leaders inherit myths. Teams build around them. Clinicians live with the consequences.
“CDSS doesn’t break all at once; it breaks decision by decision.”
Let’s challenge the seven most persistent misconceptions that quietly derail clinical decision support systems across health systems.
And more importantly, let’s replace them with realities you can operate.
A. Myth 1: “CDSS is just pop-up alerts.”
If your clinicians think CDSS equals interruptions, what have you actually built?
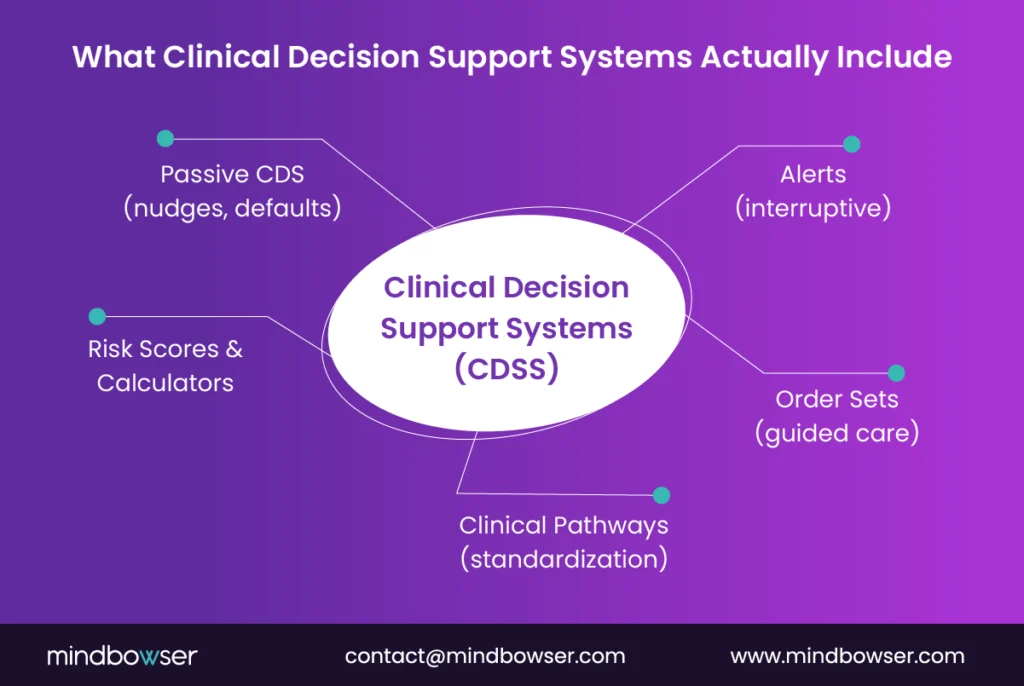
1. Reality: CDSS is a spectrum, not a pop-up
Alerts are the most visible form of CDSS. They’re also the most overused.
But real clinical decision support systems include:
- Order sets that guide evidence-based care
- Clinical pathways embedded in workflows
- Risk calculators triggered at decision points
- Passive nudges like default selections or smart suggestions
“Good CDSS is often invisible.”
When it works, clinicians don’t feel interrupted. They feel supported.
2. Why this myth exists
Early CDSS implementations leaned heavily on interruptive alerts. Why? Because they were easy to deploy and easy to measure.
But easy doesn’t mean effective.
Over time, this created a narrow mental model:
CDSS = alerts.
That assumption still drives design decisions today.
3. VBC implication
In value-based care, outcomes depend on consistent behavior, not forced interruptions.
If your CDSS strategy relies only on alerts:
- You increase fatigue
- You reduce trust
- You miss high-impact, non-interruptive opportunities
If your CDSS starts with alerts, you’ve already limited its impact.
B. Myth 2: “More alerts means safer care.”
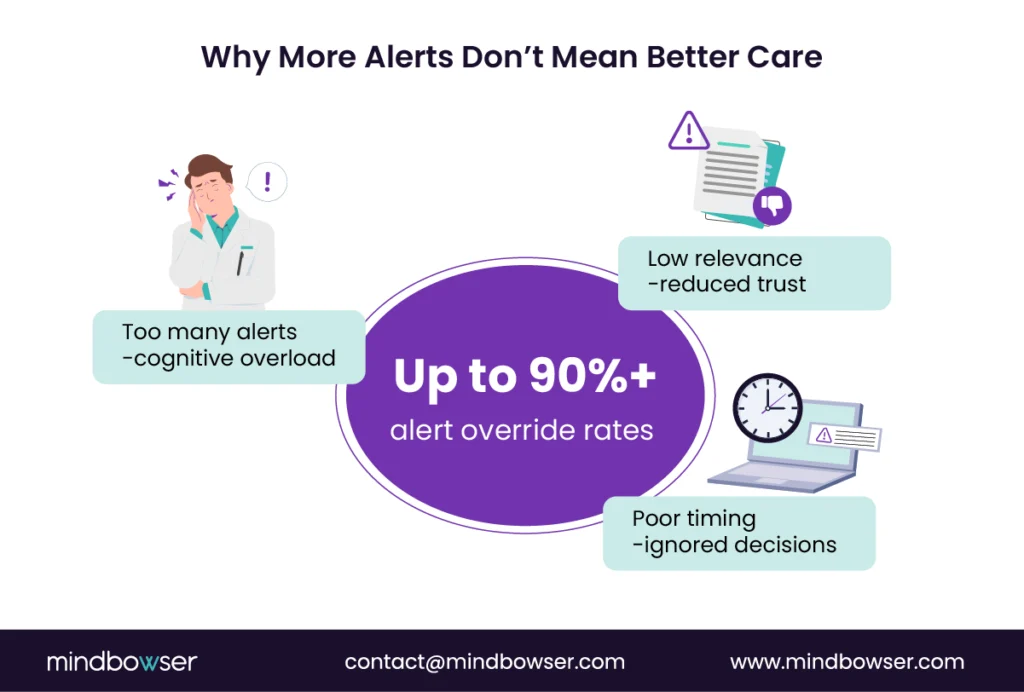
What happens when every decision triggers a warning?
Nothing.
Clinicians stop listening.
1. Reality: Alert fatigue is real and measurable
That’s not clinician negligence. That’s system overload.
“When everything is urgent, nothing is.”
The signal gets buried.
2. What good looks like
High-performing organizations flip the model:
- Fewer alerts
- Higher precision
- Better timing
- Clear clinical relevance
They prioritize:
- High-risk, high-impact interventions
- Context-aware triggers
- Non-interruptive guidance when possible
- One short rule: Earn the interruption.
3. VBC implication
In VBC, alert fatigue isn’t just a usability issue. It’s a financial risk.
Missed interventions mean:
- Unclosed care gaps
- Avoidable readmissions
- Lower quality scores
Safety doesn’t come from more alerts; it comes from better ones.
C. Myth 3: “If we buy a CDSS, adoption will follow.”
Have you ever seen a perfectly functional system that nobody uses?
That’s most CDSS deployments.
1. Reality: Workflow fit drives adoption
Clinicians don’t adopt tools. They adopt workflows that make their job easier.
In perioperative workflows, CDSS adoption improves significantly when decision support is embedded during pre-op clearance rather than post-review.
If CDSS:
- Adds clicks
- Slows decisions
- Interrupts cognitive flow
…it gets ignored.
Even if it’s clinically sound.
2. Common adoption blockers
- Poor placement within the workflow
- Lack of clinician involvement in design
- Misalignment with specialty-specific practices
- Low trust in the underlying data
This isn’t about capability. It’s about fit.
3. VBC implication
In value-based care, non-adoption isn’t neutral. It’s costly.
No adoption means:
- No behavior change
- No outcome improvement
- No ROI
You don’t deploy CDSS, you embed it.
D. Myth 4: “CDSS replaces clinician judgment.”
What do clinicians fear most when new systems are introduced?
Loss of control.
1. Reality: CDSS supports decisions, but it doesn’t make them
A well-designed CDSS:
- Surfaces relevant information
- Highlights risks or gaps
- Suggests evidence-based actions
But the clinician decides.
Always.
CDSS informs. Clinicians decide.
That distinction must be explicit.
2. Messaging internally matters
If leadership positions CDSS as:
- A compliance tool
- A control mechanism
- A replacement for expertise
- Adoption will stall.
Instead, frame it as:
- A cognitive support layer
- A way to reduce variation
- A tool to improve consistency under pressure
3. VBC implication
VBC requires standardization without removing clinical nuance.
CDSS enables that balance.
When clinicians trust CDSS, it amplifies judgment, not replaces it.
E. Myth 5: “CDSS always improves outcomes.”
If CDSS is so effective, why do results vary so widely across organizations?
Because design matters.
1. Reality: Evidence is mixed, and that’s the point
While AHRQ reports great improvements in many use cases, outcomes are not guaranteed.
Some implementations:
- Improve adherence, but not outcomes
- Increase documentation, but not quality
- Add noise without changing behavior
“CDSS doesn’t create outcomes. It influences decisions that may lead to outcomes.”
That’s a subtle but critical difference.
2. Where CDSS works best
Strong use cases share three traits:
- Clear decision moment
- High clinical variation
- Measurable outcome linkage
Examples:
- Sepsis detection
- Discharge planning
- Medication safety
3. VBC implication
In VBC, outcomes are the currency.
If CDSS isn’t tied to:
- Specific workflows
- Defined metrics
- Measurable impact
…it becomes a cost without return.
CDSS effectiveness is designed, not assumed.
F. Myth 6: “The model is the product.”
Is your team celebrating model accuracy or clinical impact?
They’re not the same.
1. Reality: Data quality and trust drive usage
A highly accurate model means nothing if:
- Data inputs are inconsistent
- Outputs aren’t trusted
- Clinicians don’t understand the logic
Trust beats accuracy in real-world adoption.
Every time.
2. Operational impact matters more than model performance
Ask:
- Does this change behavior?
- Does it fit workflow timing?
- Does it improve decisions under pressure?
If not, the model is just academic.
3. VBC implication
In VBC, execution beats prediction.
A slightly less accurate model, well-integrated into the workflow, will outperform a perfect model that sits unused.
The product is not the model; it’s the decision change.
G. Myth 7: “CDSS is a one-time build.”
What happens to your CDSS rules six months after deployment?
If nothing, you have a problem.
1. Reality: CDSS requires continuous evolution
- Clinical guidelines change.
- Workflows shift.
- Data improves.
- Your CDSS must keep up.
Without iteration:
- Alerts become outdated
- Trust declines
- Performance drops
2. Lifecycle management is non-negotiable
High-performing teams implement:
- Regular rule reviews
- Clinician feedback loops
- Performance monitoring
- Rapid iteration cycles
- This isn’t maintenance. It’s a strategy.
3. VBC implication
In VBC, static systems lose value quickly.
Continuous improvement ensures:
- Sustained outcomes
- Ongoing ROI
- Clinical relevance
CDSS is not a project; it’s a living capability.
Ready to Build Clinical Decision Support That Clinicians Actually Use?
III. How to Make CDSS Work in Value-Based Care: A Practical Operating Playbook
So what separates CDSS that gets ignored… from CDSS that drives outcomes?
No more features. Not better models.
It’s how you operationalize it.
CDSS works when it’s treated like a clinical capability, not an IT deployment.
This is where most organizations either unlock value or stall out.
Let’s make it practical.
A. Start with the use cases VBC actually pays for
Are you building CDSS where it matters or where it’s easiest?
That question alone can change your roadmap.
1. Focus on high-cost, high-variation workflows
In value-based care, not all decisions carry equal weight.
Prioritize areas where:
- Cost is concentrated
- Variation is high
- Outcomes are measurable
Examples:
- Readmission prevention at discharge
- Chronic disease management gaps
- ED triage and escalation decisions
“Start where variation is expensive.”
That’s where CDSS earns its place.
2. Define the decision moment clearly
Every effective CDSS use case answers one question:
- Exactly when should this influence a decision?
Not broadly. Precisely.
- During order entry?
- At discharge reconciliation?
- During care plan review?
If the timing isn’t clear, the intervention won’t land.
3. Set success metrics before you build
Too many teams measure after deployment.
High-performing teams define upfront:
- What behavior should change?
- What metric proves it?
- What outcome should improve?
For example:
- Reduce 30-day readmissions by X%
- Increase care gap closure rate by Y%
- Decrease inappropriate antibiotic use
If the use case isn’t tied to VBC economics, it won’t sustain attention.
B. Design principles that reduce fatigue and increase trust
Why do clinicians trust some systems and ignore others?
It’s not complexity. It’s clarity.
1. Apply the Five Rights framework
Every clinical decision support system should deliver:
- Right information
- Right person
- Right intervention format
- Right channel
- Right time in workflow
Miss one, and effectiveness drops.
Miss two, and adoption collapses.
“This works. Period.”
2. Favor non-interruptive design first
Interruptions should be rare and earned.
Instead, use:
- Inline suggestions
- Smart defaults
- Visual cues within workflows
- Context-aware nudges
Interrupt only when:
- Risk is high
- Action is urgent
- The consequence is significant
- That’s how you preserve attention.
3. Make decisions explainable
Would you trust a recommendation you don’t understand?
Neither will clinicians.
Every CDSS intervention should answer:
- Why is this being suggested?
- What data supports it?
- What happens if I ignore it?
Transparency builds trust. Trust drives adoption.
Design for cognitive flow, not system logic.
C. Governance that performs, not governance that meets
Do your governance meetings change anything, or just review dashboards?
That distinction matters more than most leaders admit.
1. Build a continuous review loop
Effective CDSS governance is not quarterly.
It’s continuous.
- Monitor performance metrics (acceptance, overrides)
- Review clinical relevance
- Retire low-value interventions
- Tune high-impact ones
Think: product iteration, not compliance review.
2. Define clear ownership
Who owns CDSS?
If the answer is “everyone,” it’s no one.
High-performing models assign:
- Clinical owners (content and relevance)
- Informatics leaders (workflow fit)
- Technical teams (execution and reliability)
- Clear ownership accelerates decisions.
3. Embed equity and safety checks
CDSS can unintentionally amplify bias if not monitored.
Governance should include:
- Equity impact reviews
- Data quality validation
- Safety event tracking
Because in VBC, outcomes must improve for all populations.
Governance is the engine that keeps CDSS clinically relevant and financially valuable.
IV. How Mindbowser Can Help
You understand the strategy. You see the gaps.
Now the real question is execution.
Building clinical decision support systems that actually influence outcomes requires more than configuration. It requires alignment across workflow, data, governance, and clinical intent.
“CDSS fails in silosand succeeds in systems.”
That’s where Mindbowser operates differently.
A. CDSS strategy and VBC-aligned use case selection
Are you solving the right problems or just building what’s feasible?
1. Identify high-impact opportunities
Mindbowser starts where value-based care creates pressure:
- Readmission reduction
- Chronic disease gap closure
- Risk-adjusted documentation improvement
- Medication safety and utilization
Instead of broad deployments, we define targeted CDSS use cases tied to financial and clinical outcomes.
Because not all decisions are equal.
2. Build a measurement-first plan
Before a single rule is designed, we define:
- Baseline performance
- Target metrics
- Expected behavior change
- Outcome linkage
This ensures every CDSS intervention is tied to:
- A measurable KPI
- A clear ROI pathway
“Measurement isn’t reporting, it’s design.”
We don’t start with technology. We start with impact.
B. Workflow-first design and build
What if your CDSS fit so naturally into workflows that clinicians didn’t notice it?
That’s the goal.
1. EHR-integrated decision support
Mindbowser builds CDSS directly into clinical workflows:
- Order entry optimization
- Discharge planning triggers
- Care coordination touchpoints
- Documentation support
Not bolted on. Built in.
This reduces friction and increases adoption from day one.
2. Data readiness and trust layer
CDSS is only as strong as the data behind it.
We ensure:
- Data normalization across sources
- Real-time or near-real-time availability
- Clear logic transparency for clinicians
Because trust drives usage.
And usage drives outcomes.
3. Accelerated, compliant delivery
With HIPAA and SOC 2 alignment by design, and reusable accelerators, Mindbowser helps teams move faster without compromising safety or compliance.
“Speed matters but only when it’s safe.”
We design CDSS for how care actually happens, not how systems are structured.
C. Implementation, tuning, and lifecycle management
What happens after go-live?
That’s where most CDSS programs lose momentum.
1. Governance model that drives action
Mindbowser helps establish governance that:
- Reviews performance continuously
- Prioritizes high-impact adjustments
- Aligns clinical, technical, and operational teams
Not meetings for visibility. Decisions for improvement.
2. Continuous optimization loops
We monitor:
- Alert acceptance and override rates
- Workflow impact
- Outcome changes
And then refine.
Rapidly.
Because static CDSS loses value fast.
3. Built-in safety and performance guardrails
Every deployment includes:
- Clinical validation checkpoints
- Equity and bias monitoring
- Fail-safe mechanisms for high-risk decisions
This ensures CDSS remains:
- Clinically relevant
- Operationally effective
- Safe at scale
We don’t just implement CDSS; we help you run it as a capability.
CDSS as a Strategic Lever for Value-Based Care
Clinical decision support systems don’t succeed because they exist; they succeed because they are designed, governed, and measured as part of care delivery.
In value-based care, outcomes are shaped by thousands of small decisions made every day.
CDSS brings consistency to those decisions, ensuring the right action happens at the right moment without slowing clinicians down. Organizations that get this right treat CDSS as a living capability aligned to workflows, owned clinically, and continuously improved. Those that don’t see the opposite: alert fatigue, low trust, and no measurable impact.
When CDSS is built around workflow, backed by governance, and tied to outcomes, it becomes a true engine for value-based care, not just another system in the stack.
A clinical decision support system is a tool that delivers the right clinical information to the right person at the right time within the workflow to improve decisions. It goes beyond alerts and includes order sets, pathways, and embedded guidance that influence real-time care.
The benefits of CDSS in healthcare include reduced clinical variation, improved quality scores, safer medication practices, and better care gap closure. When aligned with workflows, CDSS directly supports value-based care outcomes and cost control.
High override rates, often exceeding 90% in some cases, are usually due to alert fatigue and poor workflow integration. When alerts are irrelevant, mistimed, or excessive, clinicians lose trust and begin to ignore them.
No, CDSS is designed to support, not replace, clinical decision-making. It provides evidence-based insights and recommendations, but the final decision always remains with the clinician.
Adoption improves when CDSS is embedded directly into clinical workflows, designed with clinician input, and continuously optimized through governance. Focusing on high-impact use cases and measurable outcomes also drives stronger engagement.

