



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TLDR:
- Eligibility in one sentence: CCM fits when a Medicare patient has 2+ chronic conditions expected to last 12+ months (or until death), and those conditions create meaningful risk (death, acute exacerbation/decompensation, or functional decline). There is no CMS “approved list,” so your defense is based on clinical judgment and documentation, not ICD-10 bingo.
- Operations reality for hospital leaders: Most programs fail at finding the right panel, not billing. Winning pattern: combine problem list + meds + utilization signals (recent ED/IP, polypharmacy, rising A1c/eGFR drift) to build a “probable eligible” workqueue that care management can validate inside Epic/Cerner/Athena/Meditech.
- Scale math you can take to the board: If you have 20,000 eligible Medicare beneficiaries, a 15–20% enrollment rate yields ~3,000–4,000 active CCM patients (and that range is a realistic operational target, not wishful thinking).
- Reimbursement anchor points: Expect ~$68 PMPM (99490, first 20 mins) and ~$110 PMPM (99487, first 60 mins) per 2026 PFS national averages
- Why Mindbowser accelerators matter (and why your compliance team will care): The ROI unlock is repeatable enrollment + audit-ready artifacts. Mindbowser’s HealthConnect CoPilot (FHIR/HL7) plus CarePlan AI / AI Medical Summary accelerators are built to speed eligibility pulls and automate care-plan/export-pack creation, with significant documentation workload reduction via AI automation (e.g., 40% reported in clinical studies)
Common Conditions That Qualify for CCM
Most CCM-eligible patients fall into a predictable set of chronic condition groups. While CMS does not publish an official list, the conditions below are the most commonly used across U.S. health systems:
- Diabetes (Type 1 and Type 2)
- Congestive Heart Failure (CHF)
- Chronic Obstructive Pulmonary Disease (COPD)
- Hypertension (paired with another chronic condition)
- Chronic Kidney Disease (CKD)
- Depression and behavioral health disorders
- Arthritis and chronic musculoskeletal conditions
- Alzheimer’s disease and other dementias
- Osteoporosis
- Cancer and survivorship-related complications
These conditions typically qualify when they require ongoing management, create medication complexity, or introduce risk of hospitalization or functional decline.
Nearly two-thirds of Medicare beneficiaries live with two or more chronic conditions, making CCM eligibility not a niche edge case but a core population health lever. For mid-market systems, this shifts eligibility from a compliance task to a revenue and outcomes strategy.
Who actually qualifies for Chronic Care Management in 2026, and would your answer survive an audit?
For most hospitals, CCM does not stall due to billing or staffing issues. It stalls because eligibility feels fuzzy once you open the EHR.
CMS sets the rule, not a checklist: two or more chronic conditions expected to last at least 12 months with a real risk of decline or decompensation. The challenge in 2026 is translating that definition into repeatable EHR logic that captures revenue without creating compliance exposure.
This guide is built for CIOs, CFOs, CMIOs, and population health leaders who need operational clarity. We will show how to turn CMS criteria into scalable eligibility workflows, where programs fail, and how Mindbowser accelerators shorten time to ROI while keeping audits boring.
CCM eligibility is not a coding exercise. It is an operating system decision.
I. CMS CCM Eligibility Criteria (Current & Forward-Looking)
CMS eligibility for Chronic Care Management is unchanged in principle, but the bar for operational proof is higher in 2026.
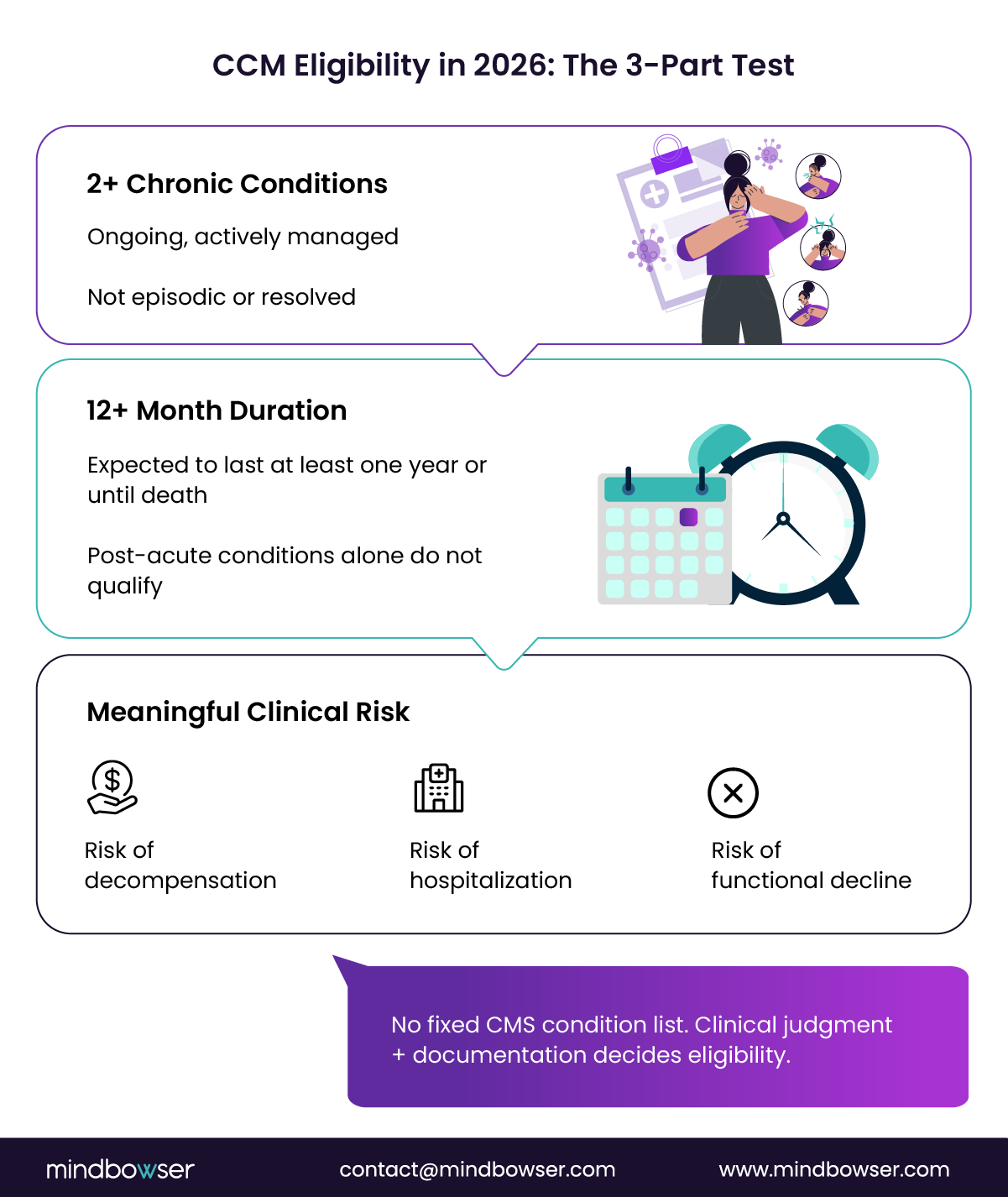
To qualify, a patient must meet all three criteria below. Each must be defensible in the EHR, not just clinically obvious.
- Two or more chronic conditions
The patient must have at least 2 ongoing conditions requiring ongoing management. These are not episodic issues or historical diagnoses left inactive on a problem list. Auditors expect evidence that both conditions are being actively managed. - Expected duration of at least 12 months (or until death)
CMS requires that the clinician reasonably expect each condition to persist for at least 1 year. Post-acute diagnoses, short-term rehab conditions, or recovery-phase complications do not qualify on their own. When eligibility is anchored to a hospitalization without a chronic context, denial risk rises quickly. - Meaningful clinical risk
This is the most misunderstood requirement. CMS does not require extreme severity, but it does require a significant risk of one or more of the following:
- Death
- Acute exacerbation or decompensation
- Functional decline
A patient with diabetes and hypertension may not qualify if both are well controlled. Add polypharmacy, declining lab trends, functional limitations, or recent ED utilization, and the risk threshold is met. Risk signals are what convert diagnoses into eligibility.
While CCM is primarily a Medicare Part B benefit, Medicaid managed care programs and commercial payers are increasingly mirroring CMS eligibility logic in value-based arrangements. Additionally, Rural Health Clinics (RHCs) and Federally Qualified Health Centers (FQHCs) can now leverage expanded APCM-aligned billing pathways, broadening access to CCM-style services across underserved populations.
Why is there no fixed CMS condition list?
CMS intentionally avoids publishing a definitive list of qualifying diagnoses. This flexibility allows clinicians to account for age, comorbid burden, utilization history, and functional status. It also places accountability on the provider. Operationally, this means eligibility must be supported by clinical judgment plus documentation, not ICD-10 codes alone.
For example, an elderly patient with diabetes, hypertension, and moderate arthritis may not appear high-risk in isolation. However, when documented as contributing to mobility limitations, fall risk, and medication complexity, the combined clinical picture clearly meets CCM eligibility thresholds.
CCM eligibility is not a coding exercise. It is a clinical determination that must be repeatable at scale and auditable. Programs that treat eligibility as static logic miss patients on one end and create compliance exposure on the other.
For hospitals building or scaling CCM, see our guide on how to start a chronic care management program with operational workflows and staffing models.
II. Common Qualifying Condition Domains (How Hospitals Find CCM Patients at Scale)
For teams looking for a more direct condition-based reference, the most commonly qualifying CCM conditions across U.S. health systems include:
- Diabetes (Type 1 and Type 2)
- Congestive heart failure (CHF)
- Chronic obstructive pulmonary disease (COPD)
- Chronic kidney disease (CKD)
- Hypertension (when paired with another condition)
- Depression and behavioral health disorders
- Cancer and survivorship-related complications
- Arthritis and chronic musculoskeletal conditions
These conditions typically qualify not because of diagnosis alone, but because they drive ongoing management needs, medication complexity, and measurable risk of hospitalization or functional decline.
CMS does not give a list. Hospitals still need a repeatable way to identify patients without over-enrolling or missing revenue. In practice, high-performing systems organize eligibility around clinical domains, then confirm risk using EHR signals.
Below are the core domains most CCM programs rely on in 2026, compressed for executive use.
1. Cardiometabolic Conditions
This is the largest and most reliable CCM pool.
Typical conditions
- Diabetes mellitus (especially with complications)
- Hypertension paired with another chronic disease
- Heart failure, coronary artery disease, atrial fibrillation
EHR risk flags
- Rising A1c or uncontrolled BP
- Polypharmacy (5+ chronic meds)
- ED visits or admissions related to cardiac or glycemic events
Why this works
Diagnosis alone is weak. Diagnosis plus utilization or medication burden is audit-safe and scalable.
2. Pulmonary and Renal Conditions
These patients drive utilization and readmissions.
Typical conditions
- COPD, persistent asthma, pulmonary fibrosis
- CKD stages 3–5, diabetic nephropathy
EHR risk flags
- ED visits for exacerbations
- Home oxygen or frequent steroid bursts
- Declining eGFR or abnormal albumin ratios
Pulmonary and renal CCM care plans align tightly with quality and value-based performance measures.
3. Neurologic and Functional Conditions
Eligibility here is driven by functional decline, not mortality risk.
Typical conditions
- Stroke with residual deficits
- Parkinson’s disease, multiple sclerosis
- Epilepsy requiring complex medication management
EHR risk flags
- Documented ADL limitations
- Rehab or caregiver involvement
- High coordination burden across specialties
Auditors accept these cases when function and coordination needs are clearly documented.
4. Behavioral Health as a Chronic Driver
Behavioral health is often the second qualifying condition that closes eligibility gaps.
Typical conditions
- Major depressive disorder
- Bipolar disorder
- Anxiety disorders
- Substance use disorder under long-term treatment
EHR risk flags
- Impact on adherence or self-management
- Chronic medication management
- Coexisting cardiometabolic disease
Always document functional impact. Diagnosis alone is not enough.
5. Oncology and Immunologic Conditions
Often under-identified in CCM programs.
Typical conditions
- Active cancer treatment
- Cancer survivorship with chronic effects
- Autoimmune disease (RA, lupus, Crohn’s)
EHR risk flags
- Neuropathy, fatigue, cardiotoxicity
- Immunosuppressive therapy
- Frequent specialty coordination
Survivorship cases frequently qualify but are missed when teams only search for “active cancer.”
6. Other High-Impact Chronic Conditions
Smaller in volume, high in complexity.
Examples
- Chronic liver disease
- HIV
- Sickle cell disease
- Rare genetic or metabolic disorders
These qualify when lifelong management and complication risk are documented.
Strong CCM programs do not ask, “Is this condition allowed?”
They ask, “Does this combination of conditions and signals create ongoing risk we can manage and defend?”
Domains provide structure. Risk signals provide proof.
III. Edge Cases and Exclusions (Where Most Denials Start)
Most CCM denials do not come from obvious mistakes. They come from gray zones where eligibility feels intuitive to clinicians but is weak on paper. Tight programs define these cases upfront, removing guesswork.
1. One Severe Condition That “Feels Like CCM.”
Clinicians often ask whether a single serious illness, such as advanced cancer or end-stage renal disease, qualifies on its own.
It does not. CMS requires two or more chronic conditions.
In practice, this is rarely a true exclusion. Most patients with severe illness also have:
- Depression or anxiety
- Hypertension or diabetes
- Chronic pain or neuropathy
Build a secondary-condition review into oncology and nephrology work queues. Most false exclusions disappear once charts are complete.
2. Post-Acute Conditions Masquerading as Chronic
Recent hospitalizations create noise.
What does not qualify:
- Sepsis, surgery, or trauma alone
- Short-term rehab diagnoses
- Conditions expected to resolve within months
What can qualify:
- When an acute event permanently worsens an existing chronic disease
- When functional decline is expected to persist beyond 12 months
Never anchor eligibility solely on a discharge diagnosis. Auditors flag this quickly.
3. Behavioral Health Without Functional Impact
Behavioral health diagnoses are valid chronic conditions, but only when they impair function or care coordination.
High-risk mistake:
- Enrolling patients with a mental health code but no documented impact on adherence, self-care, or daily function
If the chart does not explain how the condition affects management, the case is vulnerable.
4. Multi-Payer and Non-Medicare Patients
CCM is a Medicare Part B service. Applying Medicare logic to Medicaid or commercial populations creates billing errors.
Best practice:
- Maintain payer-specific eligibility logic
- Route non-Medicare patients to parallel programs when allowed
Programs that skip this step see denial rates climb fast.
5. Concurrency Errors
Concurrency mistakes are one of the fastest ways to lose margin.
Key rules:
- CCM cannot be billed with TCM in the same month
- CCM can run with RPM and BHI if the work is distinct
- CCM and APCM cannot overlap monthly
Audit defense move:
Embed a simple concurrency matrix directly into enrollment and billing workflows.
Edge cases are not rare. They are routine.
Programs that codify decisions and document rationale avoid denials. Programs that debate eligibility on a case-by-case basis invite them.
Identify CCM-Eligible Patients with Confidence
Automate eligibility, streamline documentation, and ensure CMS compliance with AI-powered tools—boosting reimbursement and improving patient outcomes.
IV. APCM vs CCM (How Hospitals Run Both Without Confusion)
When Advanced Primary Care Management (APCM) launched in 2026, many executives asked whether CCM was being replaced. It was not. APCM was designed to fill the gaps CCM intentionally leaves behind.
How the Programs Differ Operationally
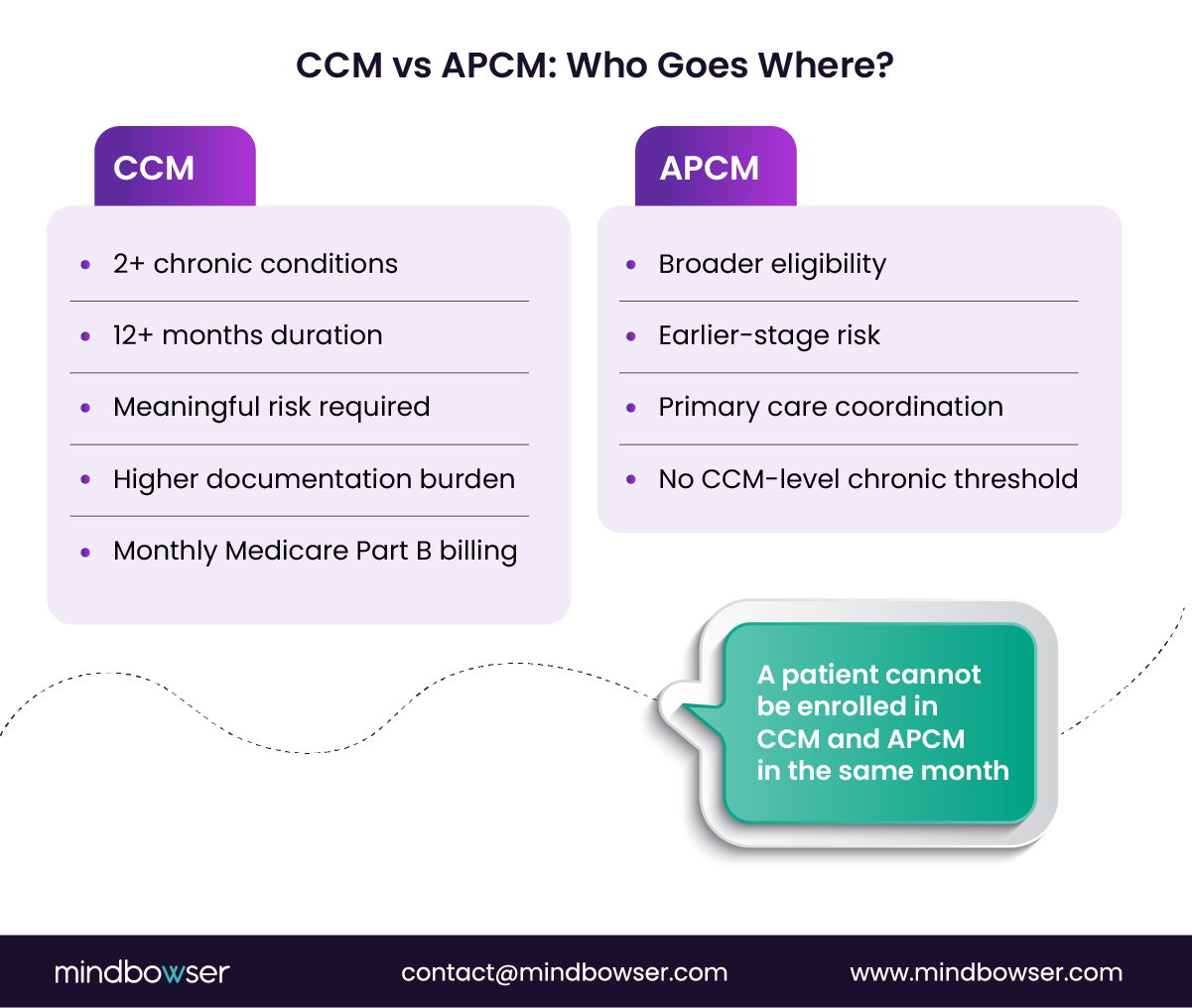
CCM
- Requires two or more chronic conditions
- Conditions must last 12 months or longer
- Must demonstrate meaningful clinical risk
- Highly compliance-driven and audit-sensitive
- Monthly reimbursement tied to documented time and care plans
APCM
- Broader eligibility
- Can include patients with fewer or lower-risk conditions
- Focuses on access, coordination, and team-based primary care
- Designed to extend structured care across a wider panel
CCM is precise. APCM is expensive. They serve different jobs.
Why Running Only CCM Creates Gaps?
Systems that deploy CCM alone run into three predictable problems:
- Patients who need support but fall just short of CCM criteria receive none
- Care teams spend time debating eligibility instead of acting
- Patients deteriorate until they finally qualify, often through avoidable utilization
APCM prevents these gaps by catching patients earlier.
Parallel Enrollment Logic That Scales
High-performing hospitals use routing logic, not manual decisions:
- Patients with 2+ chronic conditions and risk signals -> CCM
- Patients with emerging or lower risk -> APCM
Patients are reassessed monthly and can move between programs as risk changes. This creates a clean funnel in which APCM patients “graduate” into CCM rather than being rediscovered months later.
A patient cannot be enrolled in both programs in the same month. This is enforced through EHR logic and billing checks.
Patient Communication Without Confusion
Patients often ask why their neighbor is in CCM while they are not.
What works:
- Simple explanation: “CCM is for patients with two or more long-term conditions. APCM supports patients earlier.”
- Clear reassurance that neither program replaces the primary care physician
- Staff scripts that explain eligibility rather than apologize for it
Programs that script this conversation see higher trust and fewer opt-outs.
APCM does not compete with CCM. It protects and feeds it.
Together, they enable hospitals to manage risk across the full panel while remaining CCM-compliant, focused, and financially durable.
V. EHR and FHIR Playbook
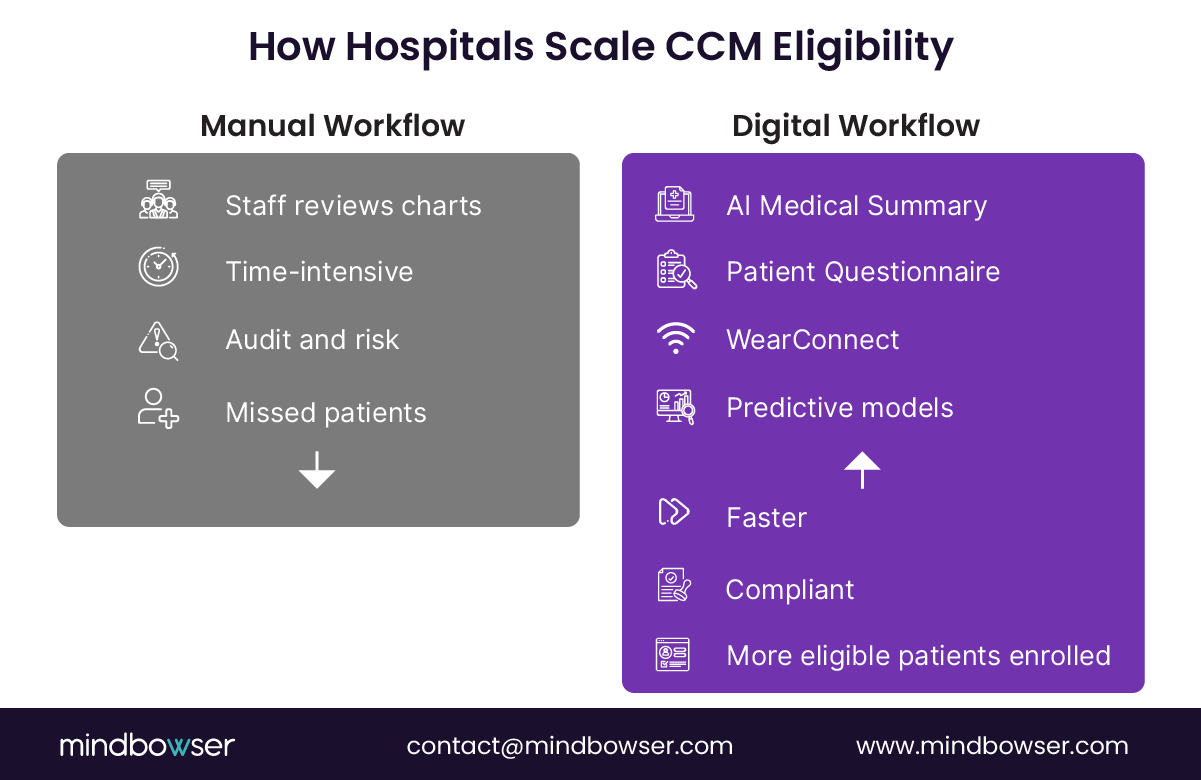
Eligibility definitions are simple. Finding the right patients every month inside your EHR is not. Programs scale only when IT, care management, and compliance align on one repeatable workflow supported by custom chronic care management software that integrates eligibility, care plans, and audit workflows into the EHR.
The Four EHR Data Surfaces That Matter
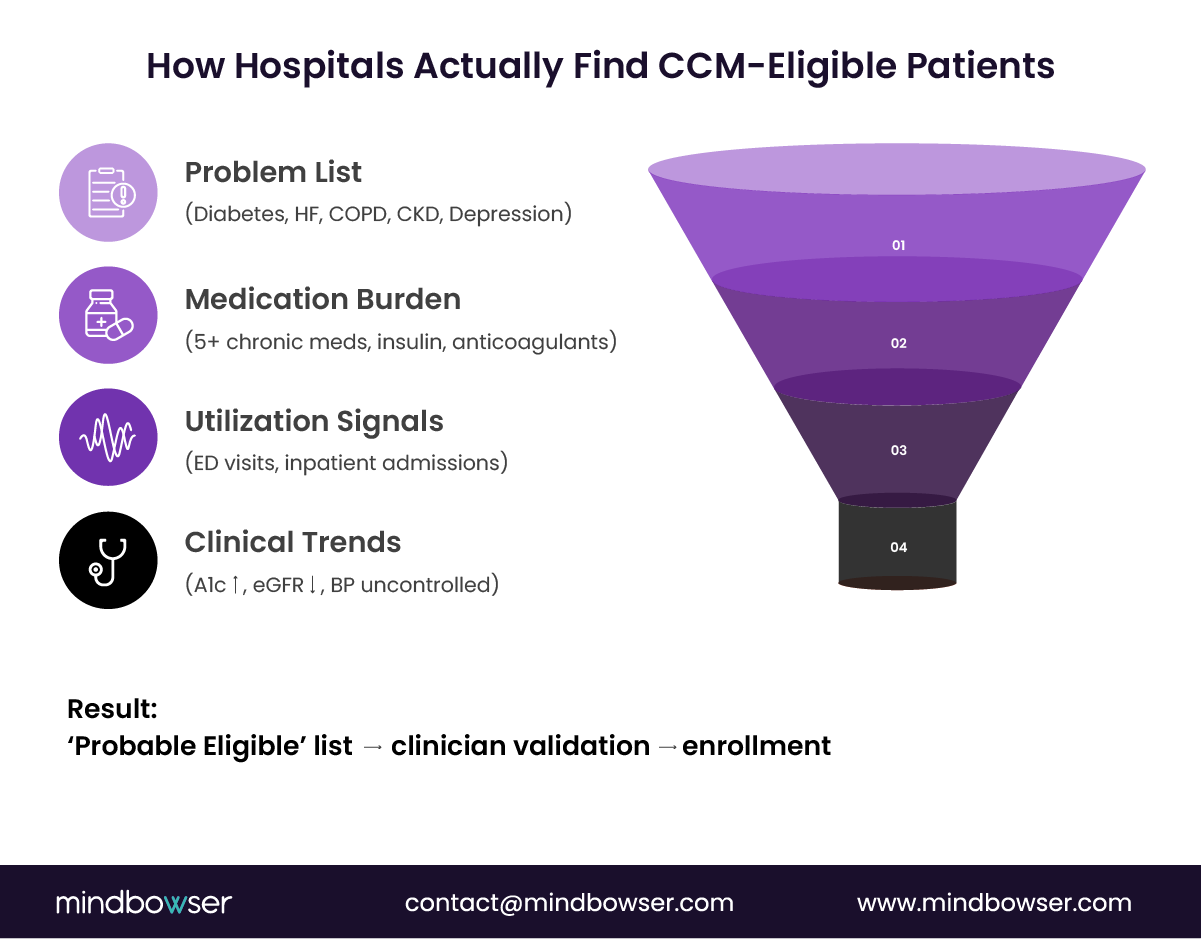
High-performing CCM programs never rely solely on diagnosis. They combine four signals to build an audit-safe eligibility funnel.
- Chronic condition groupings (problem list)
Anchor on condition families, not single codes. Diabetes, heart failure, COPD, CKD, and depression are common starting points—flag patients with two or more chronic domains, not two unrelated diagnoses. - Medication burden
Polypharmacy is one of the strongest predictors of CCM eligibility.
- Five or more chronic medications
- Long-term insulin, anticoagulants, inhaled steroids, biologics
This signal often confirms risk when utilization data is incomplete.
- Utilization signals
Recent use converts “stable on paper” patients into defensible CCM candidates.
- ED visits in the last 6 months
- Inpatient admissions tied to chronic disease
Utilization is where many missed patients surface.
- Clinical observations
Lab and vital trends strengthen the risk narrative.
- Rising A1c
- Declining eGFR
- Poor BP control
- Abnormal spirometry
Practical Query Patterns by EHR
Epic (Epic Cogito / Epic SlicerDicer)
Common logic:
- =2 chronic condition domains
- AND =1 ED visit in the last 6 months
Output is sent to a “probable eligible” workqueue for nurse or clinician review, not for auto-enrollment.
Cerner (by Oracle Health)
Typical pattern:
- CKD stage 3–5
- AND diabetes or hypertension
- PLUS medication count =5
This approach earns trust across primary care and specialty teams.
Athenahealth, Meditech, Canvas
When utilization data is thinner:
- Use condition + medication logic
- Supplement with claims or billing feeds
- Refresh monthly for consistency
Perfection is not required. Consistency is.
FHIR Object Map for Audit Defense
As programs mature, FHIR becomes the backbone of eligibility and audits.
Key objects:
- Condition: chronic diagnoses
- MedicationRequest / MedicationStatement: long-term therapy
- Encounter: ED and inpatient utilization
- Observation: labs and vitals
- CarePlan / Goal: proof of CCM activation
Mindbowser’s HealthConnect CoPilot packages these objects into standardized eligibility pulls and export-ready artifacts, eliminating the need for custom integration cycles.
The “Probable Eligible” Model
The most defensible programs do not auto-enroll from queries.
They:
- Flag probable eligibility
- Route for clinical validation
- Document the risk rationale
- Enroll with confidence
This single step reduces false positives, protects the margin, and satisfies auditors.
Eligibility logic should not live in people’s heads.
When EHR queries are standardized and paired with clinical validation, CCM becomes predictable, scalable, and defensible.
In practice, most high-performing systems operationalize eligibility using a three-layer workflow:
- Automated EHR queries to generate an initial eligible population
- Structured intake or data capture (forms, RPM, patient-reported inputs)
- Clinical validation by care managers to confirm CMS-aligned risk and duration
This layered approach ensures scalability without sacrificing audit defensibility.
VI. Documentation and Audit Readiness (Where CCM Programs Are Won or Lost)
Billing CCM is straightforward. Defending it in an audit is not. In 2026, documentation is the control plane that protects both revenue and credibility.
The Four CMS Documentation Requirements
Every CCM patient must have all four elements present and retrievable. Missing one can invalidate the entire month.
- Patient consent
Consent may be verbal or written, but it must be:
- Documented in the chart
- Clear about CCM services, cost sharing, and the right to revoke
Executive risk: consent buried in free text or scanned PDFs that cannot be easily exported.
- Comprehensive care plan
The care plan must reflect:
- Active problems
- Patient-centered goals
- Planned interventions
- Assigned care team members
Static or outdated plans are a common denial trigger. This is where automation matters. Mindbowser’s CarePlan AI generates CMS-aligned plans directly from EHR data, cutting documentation time by roughly 40% while maintaining audit-safe language.
- 24×7 access to the care team
Auditors expect evidence that patients know how to reach support after hours. This is usually satisfied through:
- After-hours instructions embedded in the care plan
- Nurse triage workflows tied to CCM patients
- Continuity and accountability
One practitioner must be accountable for ongoing management. Ambiguity here creates audit risk.
Time Tracking and Concurrency Controls
Time documentation is binary. Either it is defensible, or it is not.
Monthly time thresholds
- General CCM: 20+ minutes
- Complex CCM: 60+ minutes
Best practice:
- Log activities by date, duration, and activity type
- Tie work to care plan goals, not generic “care coordination.”
Concurrency rules that matter
- CCM cannot overlap with TCM in the same month
- CCM may run with RPM and BHI if workstreams are distinct
- CCM and APCM cannot overlap monthly
Embedding a concurrency matrix in enrollment and billing workflows prevents repeat errors.
The Monthly Export Pack (Your Audit Insurance)
High-performing programs generate a standardized export pack for each CCM patient, each month:
- Consent record
- Current care plan
- Time log summary
- Care team communications
- Concurrency verification
When audits occur, these teams export and submit rather than scramble.
If documentation feels like a tax on your team, the system is broken.
When documentation is automated, structured, and exportable, CCM becomes predictable, scalable, and audit-proof.
VII. ROI and Operations (What CFOs Actually Approve)
Once eligibility and documentation are solid, CCM becomes a financial conversation. This is where CFOs decide whether the program stays small or scales.
The Revenue Waterfall
The math is consistent across mid-market health systems.
- A 50,000-life Medicare panel typically includes ~20,000 CCM-eligible patients (2+ chronic conditions with risk).
- A realistic first-year enrollment rate of 15–20% yields 3,000–4,000 active CCM patients.
- General CCM reimbursement averages ~$64 per patient per month, with complex CCM paying more.
At 3,500 enrolled patients, that equates to ~$2.7M in annual CCM revenue before adjustments. This is why CCM keeps resurfacing in margin and quality discussions.
What CFOs consistently find is that CCM revenue leakage is rarely due to reimbursement rates—it is driven by under-identification of eligible patients. Even a 10–15% gap in eligibility capture can translate into seven-figure missed revenue annually in mid-sized systems.
Cost Structure That Holds Up in Practice
Staffing
- Care manager cost: ~$80K–$100K per FTE
- Sustainable panel: 250–300 patients per care manager
- 3,500 patients = ~12–14 FTEs
Technology
- Eligibility logic, care plan automation, time tracking, and audit exports
- Typically $8–$12 PMPM, depending on build vs buy
Program overhead
- Training, compliance, QA, and governance
- Commonly $100–$150K in year one
Break-Even and Payback
- Break-even: ~1,800–2,000 enrolled patients
- Payback period: 9–12 months in most systems
The swing factor is not reimbursement. It is efficiency. Teams using automated care plans and export packs support larger panels with the same staff, accelerating payback.
The Silent Margin Killer: Denials
A 5% denial rate at scale can erase six figures annually. That is why high-performing programs treat eligibility logic, documentation, and concurrency checks as financial controls rather than clerical tasks.
Operations: From Eligible to Enrolled
Eligibility lists do not create revenue. Consent does.
What works
- Nurse-led calls using plain-language scripts
- Outreach tied to clinical moments (post-discharge, Annual Wellness Visits)
Programs that align outreach this way routinely lift consent rates from ~22% to ~41% within a quarter.
First-30-day activation checklist
- Medication reconciliation completed
- Baseline labs reviewed
- Care goals established
- The care manager was introduced by name
Early engagement reduces drop-off and stabilizes monthly time capture.
CCM ROI is not theoretical. The math works.
The difference between a break-even program and a seven-figure contributor is operational discipline.
VIII. How Hospitals Actually Identify CCM-Eligible Patients (Simplified View)
For executive alignment, eligibility can be simplified into a repeatable decision stack:
- Step 1: Does the patient have 2+ chronic conditions?
- Step 2: Are those conditions expected to last ≥12 months?
- Step 3: Is there documented risk (utilization, labs, function, meds)?
- Step 4: Can that risk be clearly defended in the chart?
If all four are true, the patient is not just clinically eligible—they are audit-ready.

VIII. CCM Eligibility in 2026: What Actually Matters
In 2026, CCM eligibility is no longer about knowing the rule. Every hospital leader knows it by heart: two or more chronic conditions, 12 months, meaningful risk. The real differentiator is whether your organization can apply that rule consistently, defensibly, and at scale.
The systems that win do not chase diagnosis lists. They operationalize eligibility through EHR logic, utilization signals, and documented clinical judgment. They treat eligibility as a monthly workflow rather than a one-time decision. That is how they avoid denials, expand enrollment, and turn CCM into a reliable lever for revenue and quality.
The takeaway from this guide is simple: in 2026, CCM eligibility is not a compliance hurdle. It is a design choice. Build it deliberately, and everything downstream works better.
Medicare CCM requires two or more chronic conditions expected to last at least 12 months or until death. The conditions must also create a meaningful risk of death, acute exacerbation or decompensation, or functional decline.
Yes, diabetes can qualify for CCM when it is paired with at least one other chronic condition and creates ongoing management needs or measurable risk. Diabetes often qualifies alongside hypertension, CKD, heart failure, or depression.
Yes, COPD can qualify for CCM when it is paired with another chronic condition and requires ongoing care management. COPD is commonly used in CCM eligibility when supported by utilization history, medication burden, or documented exacerbation risk.
No. CMS does not publish a finite list. The rule is for two or more chronic conditions that have lasted at least 12 months and pose a real risk. Common categories include diabetes, heart failure, COPD, CKD, depression, and cancer. Clinical judgment is key.
APCM is broader and can include patients who do not meet strict CCM criteria. A patient cannot be enrolled in both CCM and APCM in the same month. Many hospitals run them in parallel with routing logic in their EHR.
At minimum: patient consent, a comprehensive care plan, time tracking for monthly activities, and a concurrency review. Many hospitals also export lab values, medication lists, and utilization notes to strengthen the audit file.
CCM is a Medicare Part B service, so patients usually pay a copay unless they have supplemental coverage. Consent can be verbal or written, but must be documented in the EHR. It does not need to be re-collected monthly unless circumstances change.
Yes. Major depressive disorder, bipolar disorder, anxiety disorders, and substance use disorder can all qualify if they are chronic, recurring, and impair function. Documentation must clearly show long-term risk and management needs.


