



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR:
Complex Chronic Care Management (CPT 99487/99489) allows providers to bill for patients requiring higher-level decision-making and extended care coordination time. With reimbursements up to ~$144 for 99487 and ~$78 for 99489, organizations can unlock incremental revenue while improving compliance and patient outcomes, organizations can unlock incremental revenue while improving compliance and patient outcomes. Success hinges on precise documentation, workflow redesign, and audit-ready processes.
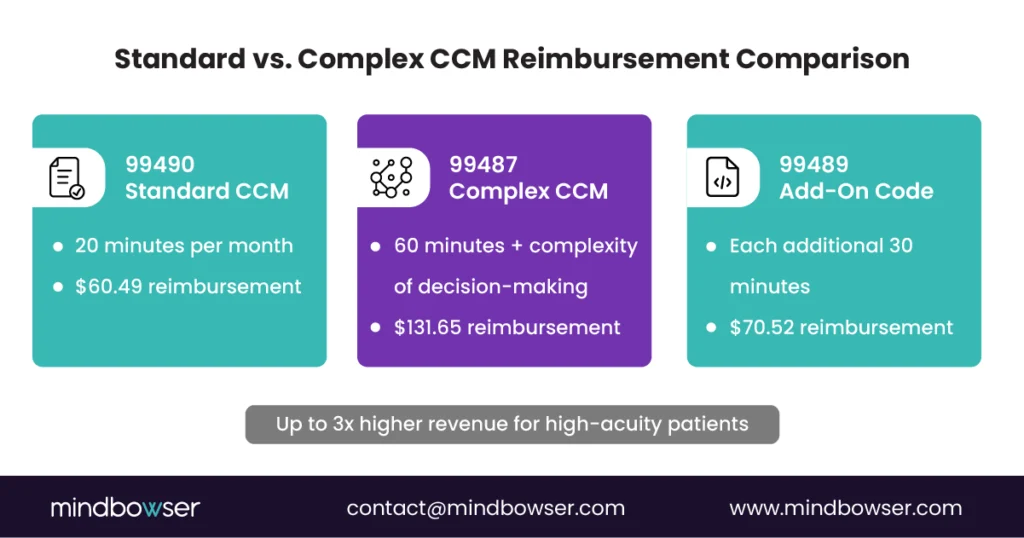
Complex Chronic Care Management (CPT 99487/99489) pays providers for patients who need extended coordination and moderate-to-high complexity medical decision-making. The base complex CCM code, 99487, reimburses $144 for at least 60 minutes per month, compared with $66 for standard CCM (99490). That is a 2.2x revenue multiple for qualifying patients. Additional time is billed using 99489 at $50 for each extra 30-minute increment.
The financial upside is meaningful, but it is not automatic. Organizations must document time, maintain an active care plan, and clearly show clinical complexity in provider notes. CMS audits focus on these elements, and gaps lead to denials or recoupments.
Hospitals and digital health companies that combine disciplined workflows with automation can turn complex CCM into a predictable margin while supporting high-acuity populations.
Rates reflect current PFS national averages.
Are you already doing the work for complex CCM but getting paid as if it were standard care coordination?
That gap shows up every month in hospitals and digital health programs managing high-acuity patients. Care teams spend hours coordinating across specialties, reconciling medications, interpreting remote data, and preventing avoidable escalations. Yet many organizations still bill standard CCM, even when the clinical effort clearly exceeds that threshold.
Complex Chronic Care Management, billed under CPT 99487 and 99489, exists to close that gap. These codes recognize both the time invested and the complexity of medical decision-making required to manage patients with multiple chronic conditions. At current national averages, the base complex CCM code pays $144 for 60 minutes per month, compared with $66 for standard CCM. That difference matters to CFOs watching margins and to operators funding care teams.
The work is already happening. The risk sits in documentation, workflow design, and audit readiness. Organizations that align those pieces capture the revenue. Those who do not leave it on the table.
I. Understanding Complex CCM (99487/99489)
A. Definitions and Criteria
Complex Chronic Care Management is billed when a patient’s needs go beyond routine coordination and require sustained clinical judgment. CPT 99487 applies when clinical staff… For a complete breakdown of CCM CPT variants and when to use each, see our CCM CPT codes guide. Under the direction of a physician or other qualified healthcare professional, spend at least 60 minutes in a calendar month delivering CCM services and the care involves moderate-to-high complexity medical decision-making.
Time alone is not enough. Notes must show active clinical management, such as evaluating competing treatment options, managing polypharmacy, interpreting RPM or lab data, or coordinating across multiple specialists for unstable conditions.
CPT 99489 is an add-on code used when care extends beyond the initial hour. Each unit represents an additional 30 minutes of qualifying clinical staff time in the same month. There is no hard cap, but each increment must meet the same complexity standard as the base code.
Patient eligibility mirrors standard CCM rules. Patients must have two or more chronic conditions expected to last at least 12 months or until death and place them at significant risk of death, acute exacerbation, or functional decline.
B. Key Differentiators from Standard CCM
The clearest distinction between standard and complex CCM is economic. Standard CCM (99490) pays $66 for 20 minutes per month. Complex CCM (99487) pays $144 for 60 minutes plus documented complexity. That is a 2.2x revenue multiple for patients who already consume more care team time.
Operationally, the differentiator is decision-making. Complex CCM requires proof that clinicians are weighing risks, reconciling conflicting data, or managing interactions that materially affect patient outcomes. A simple check-in does not qualify.
For finance leaders, this means complex CCM better matches reimbursement to cost. For technology leaders, it means workflows must capture both time and clinical reasoning in a way that stands up to audit.
C. Why It Matters in 2026
Complex CCM shifts reimbursement toward patient acuity instead of raw minutes. That matters as populations age and comorbidities stack. It allows organizations to fund care managers, pharmacists, and behavioral health coordinators without eroding margins.
It also forces discipline. Programs that treat complex CCM as “longer CCM” fail audits. Programs that treat it as a documented clinical process create sustainable revenue while improving outcomes for the patients who need the most attention.
Get The Downloadable CCM CPT Code & Billing Cheat Sheet To Compare 99487, 99489, And The Full CCM Code Family In One Place
From documentation automation to EHR integration, Mindbowser helps you scale complex CCM with confidence and measurable ROI.
II. Documentation and Compliance Foundations
A. Required Documentation Elements
Complex CCM documentation must prove two things at the same time: that the time threshold was met and that clinical decision-making rose to a moderate or high level. CMS does not accept one without the other.
At a minimum, each billed month must include:
- Comprehensive Care Plan
The care plan must be patient-centered and active. It should list chronic conditions, measurable goals, planned interventions, assigned team roles, and follow-up cadence. Static or copied plans are a red flag. Updates must reflect changes in patient status or treatment direction. - Monthly Time Logs
Providers must document at least 60 minutes of qualifying clinical staff time for CPT 99487. Time can include patient outreach, coordination with specialists, medication reconciliation, RPM review, and care plan updates. Each activity should be timestamped and attributable to the patient. Additional 30-minute increments must be clearly logged to support 99489. - Decision-Making Complexity Evidence
Notes must show moderate-to-high complexity medical decision-making. This includes weighing competing treatment options, managing polypharmacy, interpreting labs or RPM data, or coordinating across multiple clinicians for unstable conditions. A summary without clinical reasoning does not qualify.
If an auditor cannot quickly connect time, complexity, and patient impact, the claim is exposed.
B. Example Notes and Audit Packet
Strong notes make complexity obvious without being long. They explain why decisions were made, not just what was done.
Sample provider note:
Reviewed RPM blood pressure and glucose trends showing increased variability over the past two weeks. Findings suggest possible medication non-adherence versus disease progression.
Coordinated with the RN and pharmacist to review the regimen and assess the interaction risk.
Consulted cardiology regarding beta-blocker adjustment given comorbid heart failure. Provided patient education on monitoring side effects and escalation thresholds.
Complexity: High due to multi-condition management and medication interaction risk.
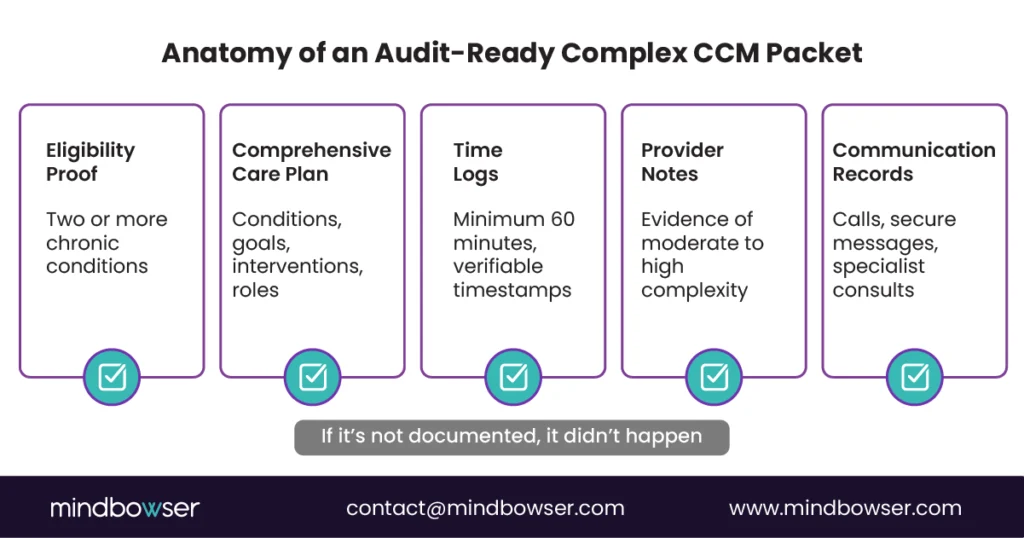
Audit packet structure typically includes:
- Patient eligibility confirmation
- Current care plan with documented updates
- Monthly time log showing =60 minutes
- Provider notes demonstrating complexity
- Communication records with patients and specialists
If any piece is missing, auditors assume the work did not occur.
C. CMS & Compliance Expectations
CMS has consistently identified CCM as an audit focus area, and complex CCM carries higher scrutiny due to higher payments.
Auditors expect:
- Exact adherence to CPT definitions
- Clear linkage between time logs and clinical notes
- Evidence that complexity is ongoing, not episodic
Organizations relying on manual notes and spreadsheets often fail under review. Those using structured templates, automated time capture, and system-generated audit packets reduce risk while protecting revenue.
Get the CCM Audit Readiness Checklist
From documentation automation to EHR integration, Mindbowser helps you scale complex CCM with confidence and measurable ROI.
III. Financial and Operational Impact
A. Incremental Revenue Potential
Complex CCM changes the unit economics of chronic care when applied to the right patients. The math is straightforward, which is why CFOs care about this code set.
- Standard CCM (99490) reimburses $66 for at least 20 minutes per patient, per month.
- Complex CCM base (99487) reimburses $144 for at least 60 minutes plus documented moderate-to-high complexity.
- Add-on time (99489) reimburses $50 for each additional 30-minute increment.
That puts the base complex CCM code at a 2.2x multiple over standard CCM before any add-on time is considered. For patients who routinely exceed 60 minutes of coordination, monthly reimbursement can move well beyond the standard CCM ceiling without adding new patient volume.
At the program level, the impact compounds quickly. A hospital managing 1,000 CCM-eligible patients does not need universal complex CCM adoption to see results. Even shifting a fraction of high-acuity patients into compliant 99487 workflows can fund additional care coordinators, pharmacists, or behavioral health support without tapping operating margin.
For digital health companies, this differential strengthens payer and investor conversations. Revenue tied to documented complexity is more defensible than volume-driven billing alone.
B. ROI Case Study Insights
Case studies consistently show that financial return follows operational discipline.
One digital health program automating intake, documentation, and follow-ups with AI-driven workflows cut documentation time by 70% and shortened follow-up cycles by 60%, while patient interactions rose 50% — freeing care teams to support more complex CCM encounters without added staffing.
A maternal-health build reached 76% automation of manual coordination steps, the kind of structured capture that makes 99487/99489 documentation audit-defensible.
The pattern is consistent. Technology does not create revenue by itself. It enables teams to document the work they already do.
C. Staffing and Workflow Considerations
Higher reimbursement brings higher expectations. Complex CCM requires intentional staffing models.
- Nurse care coordinators carry much of the time documentation and coordination load. They must be trained to surface clinical complexity, not just activity.
- Physicians and advanced practitioners anchor decision-making documentation. Their notes are what ultimately justify complexity under audit.
- Outsourcing vs. in-house decisions hinge on scale and risk tolerance. Mid-market hospitals often outsource to reduce compliance exposure. Startups tend to keep CCM in-house but rely heavily on automation to scale.
Without the right staffing mix and supporting systems, organizations either miss revenue or invite audit risk. There is no middle ground.
IV. Implementation Roadmap for Providers
A. Workflow Redesign Checklist
Complex CCM does not work as an add-on to existing processes. It requires a deliberate workflow that captures eligibility, time, and complexity without adding friction for clinicians.
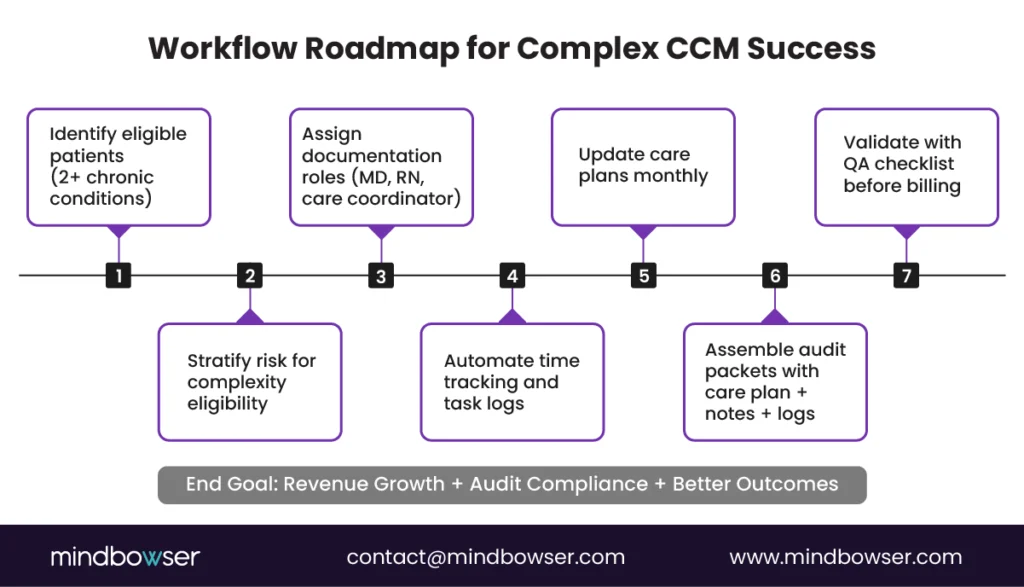
- Patient Identification and Stratification
Start by identifying patients with two or more chronic conditions. Apply risk stratification using utilization history, medication burden, and recent exacerbations to flag patients likely to meet complexity thresholds. - Role-Based Execution
Define responsibilities clearly. Care coordinators and RNs document outreach, monitoring, and coordination time. Physicians or qualified professionals document clinical judgment, treatment trade-offs, and decision rationale. This separation reduces gaps and duplication. - Time Capture Discipline
Every qualifying activity must be captured as it happens. Calls, secure messages, chart reviews, RPM review, and care plan updates all count when tied to active coordination. Missed minutes are lost revenue and audit exposure. - Care Plan Lifecycle Management
Care plans must evolve monthly. Changes in goals, medications, or risk status should trigger updates. Outdated plans undermine both billing and compliance.
Workflows must make the right behavior the easiest behavior.
B. Technology Enablers
Technology determines whether complex CCM scales or stalls.
- AI Medical Summary
Converts unstructured clinical data into structured summaries that support complexity documentation and reduce provider burden. - CarePlan AI
Creates and maintains patient-centered care plans aligned with CPT requirements. Automated prompts ensure plans stay current. - ConnectHealth
Connects directly with major EHRs, including Epic, Cerner, Athena, Healthie, and Canvas. Time logs, care plans, and notes flow into a single audit-ready record.
For CTOs, the test is simple. If documentation lives in multiple systems, audits get harder and revenue leaks.
C. Quality Assurance (QA) Checklist
Quality assurance is the final control point before claims go out the door.
- Complexity Validation
Do notes clearly show moderate-to-high decision-making, such as managing polypharmacy, conflicting data, or unstable conditions? - Time Verification
Is at least 60 minutes logged for 99487, with additional 30-minute increments clearly supporting 99489? - Care Plan Currency
Has the care plan been reviewed and updated in the current month? - Audit Packet Readiness
Can a complete packet be generated on demand, including eligibility, care plan, time logs, and notes? - Pre-Bill Review
Are samples reviewed by a compliance lead before submission?
Programs that pass this checklist consistently are the ones that keep complex CCM revenue.
V. How Mindbowser Enables Complex CCM Success
Mindbowser enables complex CCM programs through custom chronic care management software designed for audit-ready documentation, time capture, and CPT-aligned workflows.
A. Custom Development
Mindbowser designs CCM solutions specifically around CPT 99487 and 99489. That means time capture, care plan updates, and decision-making documentation are not afterthoughts. They are embedded into daily clinical workflows.
- CPT-aware design ensures both the 60-minute threshold and complexity requirements are met without manual policing.
- API-first architecture supports scale for mid-market hospitals and fast-growing digital health companies.
- Client-owned IP ensures long-term flexibility as reimbursement models evolve.
B. Compliance + ROI Automation
Higher reimbursement increases audit exposure. Automation reduces it.
- AI Medical Summary converts unstructured notes, RPM data, and communications into structured documentation aligned to complex CCM requirements.
- CarePlan AI maintains living care plans that reflect current goals, interventions, and assigned roles.
- Audit packet generation assembles eligibility proof, time logs, care plans, and provider notes into CMS-ready packets on demand.
- ROI dashboards give CFOs real-time visibility into revenue from 99487 and 99489, without waiting for lagging reports.
This is not generic CCM software. It is an infrastructure designed to defend revenue under scrutiny.
From Higher Reimbursement to Audit Confidence
Complex Chronic Care Management recognizes what care teams already know. High-acuity patients require more time and deeper clinical judgment. CPT 99487 and 99489 finally pay for that work, with the base code reimbursing $144 compared with $66 for standard CCM.
The upside is meaningful. The bar is high. Organizations that treat complex CCM as “longer CCM” fail audits. Organizations that treat it as a documented clinical process create sustainable revenue and fund better care for their most vulnerable patients.
The path forward is clear. Identify the right patients. Redesign workflows. Automate documentation. Validate every claim before it goes out the door.
Complex Chronic Care Management (CCM) refers to the ongoing coordination of care for patients with two or more chronic conditions that pose significant health risks. CPT codes 99487 and 99489 are used to bill for this service when care involves moderate-to-high complexity medical decision-making and at least 60 minutes of clinical staff time per month, under physician supervision.
The main differences lie in time requirements and decision-making complexity:
Standard CCM (99490) covers 20 minutes of staff time and routine coordination.
Complex CCM (99487) covers 60 minutes and requires moderate-to-high medical decision-making.
Add-on code (99489) covers each additional 30 minutes.
Complex CCM acknowledges the deeper clinical effort needed for high-acuity patients and offers higher reimbursement.
As of 2026, Medicare reimburses approximately:
$144.29 for CPT 99487 (base code for 60 minutes).
$78.16 for CPT 99489 (each additional 30 minutes).
For comparison, standard CCM (99490) reimburses $66.13 — making complex CCM roughly a 2.2x multiple.
To bill 99487 or 99489, providers must document both time spent and decision-making complexity. Required records include:
A comprehensive care plan with diagnoses, goals, and interventions.
Time logs proving 60+ minutes of clinical coordination.
Notes showing moderate-to-high medical decision-making.
Communication records and audit-ready documentation.
Tools like AI Medical Summary and CarePlan AI can automate this process for accuracy and compliance.
Mindbowser builds FHIR-native, API-first CCM platforms tailored for CPT 99487/99489. Our solutions:
Automate documentation and audit packet creation.
Integrate with major EHRs like Epic, Cerner, and Athenahealth.
Use AI-powered workflows (CarePlan AI, AI Medical Summary) to reduce manual work.
Deliver real-time ROI dashboards to track revenue and compliance.
This helps hospitals and digital health companies scale CCM programs that are profitable, compliant, and audit-ready.


