



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
Most value-based care programs do not fail because the contract is bad.
They fail because claims and clinical data never align in a way a contract, an auditor, or a nurse can trust. Only 36 percent of hospitals have the IT stack to support population health, HIE, and VBC analytics, meaning most CIOs are flying half-blind.
This blog walks through three failure modes (claims-only views, broken attribution, and quality-measure drift), then shows a practical FHIR quick-start and “attribution rescue” pattern that we implement with clients using workflows like AI Medical Summary and HealthConnect CoPilot.
“Are you confident that your value-based care performance reports reflect what is actually happening in your clinics?”
Most CIOs and CTOs quietly say no. The problem is rarely the contract. The real problem is that claims and clinical data describe different versions of the same patient. Finance teams work with claims that are complete but delayed. Care teams work with charts that are rich but inconsistent.
Only 36 percent of hospitals have the integrated analytics, HIE, and population health systems needed to unify these sources for value-based care.
When the data behind risk scores, attribution lists, and quality measures do not agree, value-based programs stall. This guide explains the three failure patterns that cause that breakdown and shows a practical path forward using FHIR, attribution rescue workflows, and accelerators like AI Medical Summary and HealthConnect CoPilot.
I. Why do claims and clinical data tell different stories?
CIOs and CTOs often report that financial dashboards do not align with what clinicians see at the point of care. The disconnect is structural.
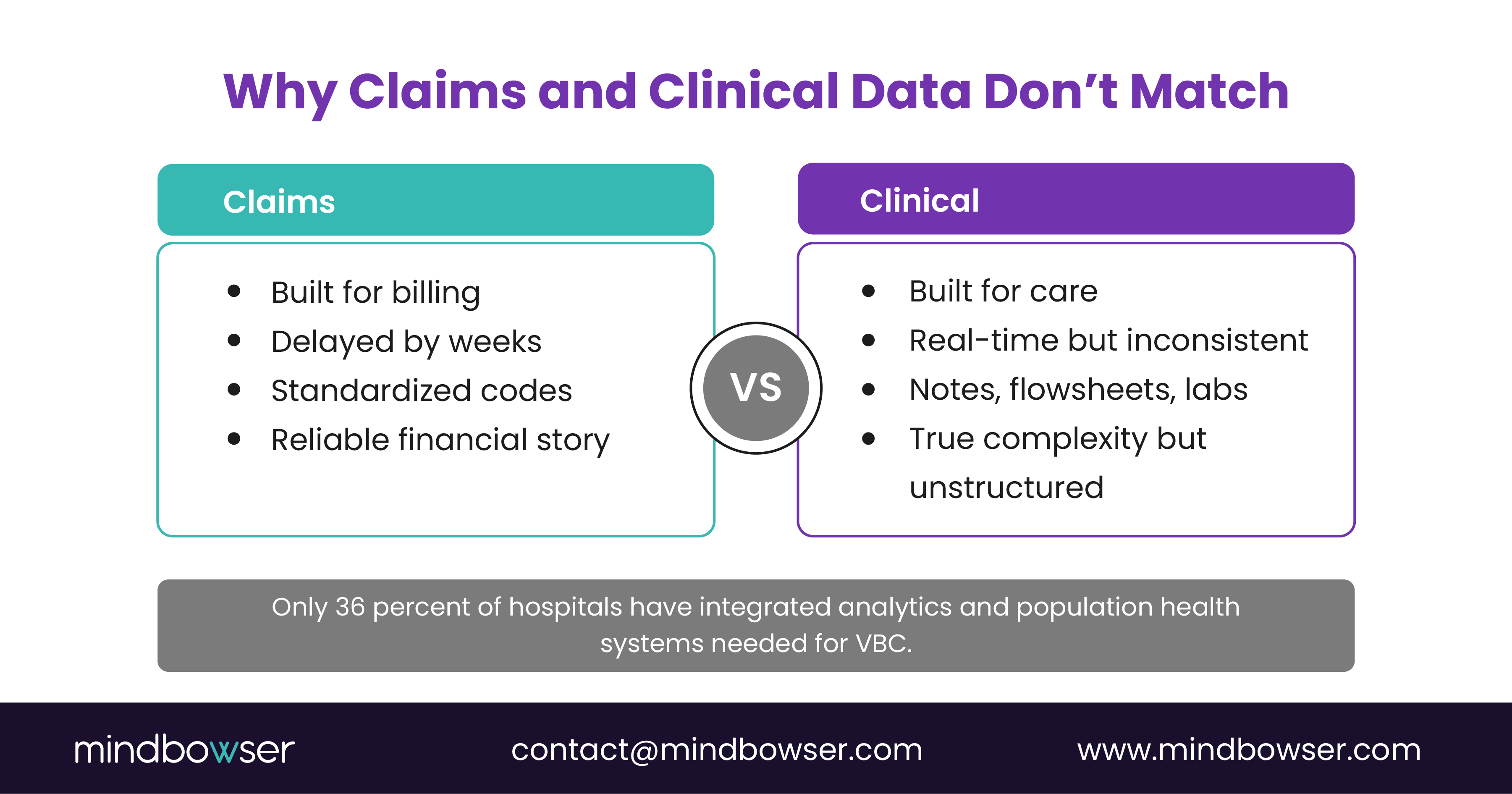
- Claims are built for payment and arrive weeks after the encounter.
- Clinical data is built for care and sits inside notes, problem lists, flowsheets, and lab feeds.
- Only 36 percent of hospitals have the IT infrastructure needed to integrate both views for VBC analytics, leaving most organizations working with an incomplete truth.
When the two systems disagree, every value-based contract becomes unreliable.
Finance sees low risk and high cost.
Clinicians see complex panels and closed gaps that never show up in reports.
II. What do we actually mean by claims vs clinical data?
To fix the issue, we need to define the sources clearly.
A. Claims data
- From payer adjudication systems
- Uses HCPCS, CPT, ICD, and revenue codes
- Complete financial story
- Lacks clinical context and arrives late
B. Clinical data
- From EHRs, labs, RPM, and pharmacy systems
- Contains diagnoses, vitals, labs, medications, and notes
- Rich view of complexity
- Inconsistent structure and coding
Value-based care depends on aligning both data types across:
- Attribution
- Risk adjustment
- Quality measures
- Utilization patterns
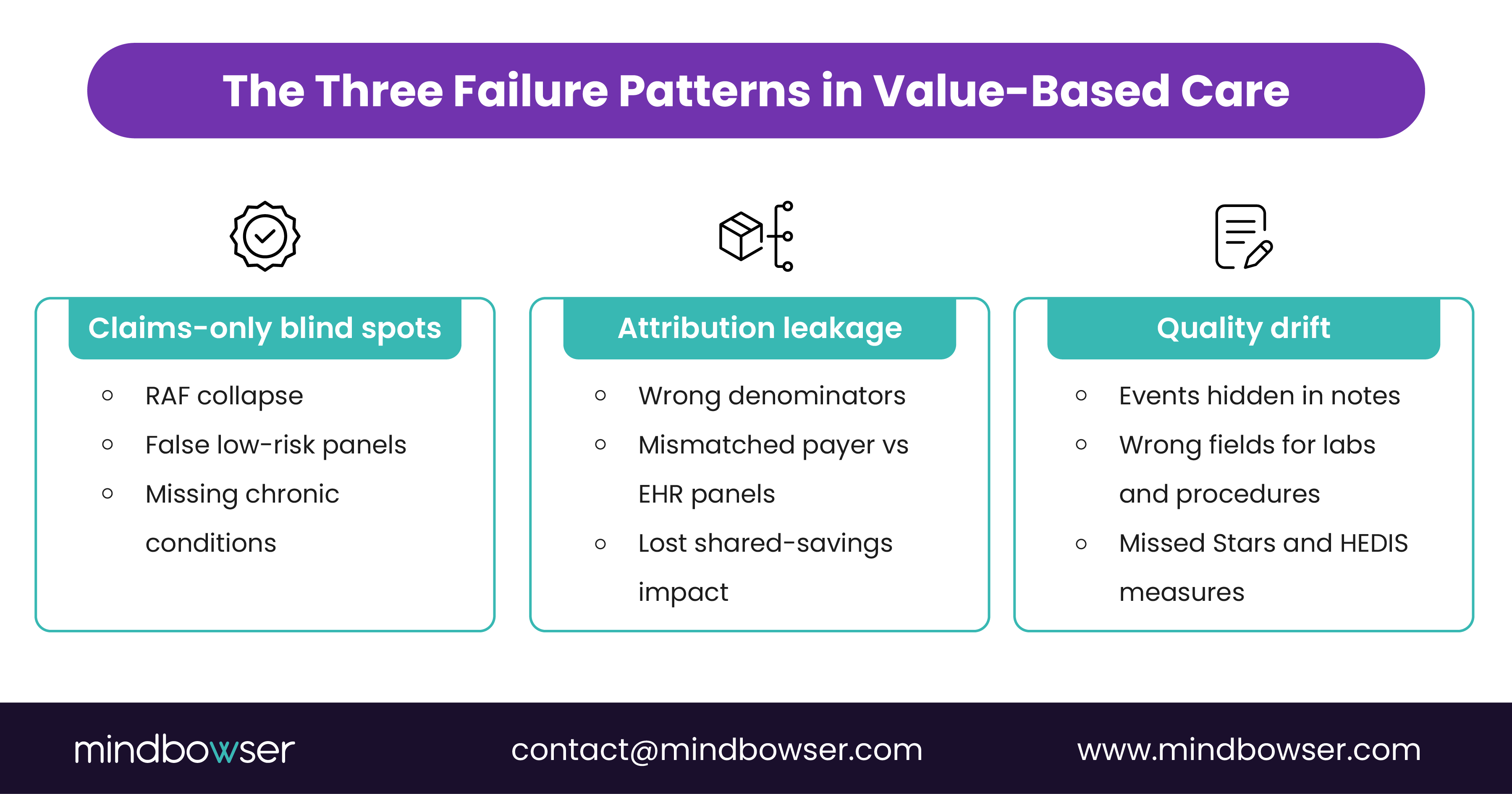
III. Failure pattern 1: Claims-only views hide real risk and care gaps
Many VBC teams start with a claims-only warehouse because it appears simpler. It also guarantees errors later.
A. Typical symptoms
- RAF scores that spike early, then collapse
- Panels that look low risk on paper
- Gaps-in-care lists that contradict what nurses see in charts
During ChartBiopsy work, we repeatedly see high-complexity conditions in notes that never surface in claims. Records often sit in PDFs or CCDs without structured fields.
B. How do we fix it
- Use AI Medical Summary to extract diagnoses, medications, labs, and risk factors from narrative notes and external records.
- Map findings into FHIR resources like Condition, MedicationStatement, Observation, and Encounter.
- Feed enriched FHIR data into risk adjustment and quality logic instead of relying on billing fields.
The goal is simple: risk scores and care gaps should reflect the true clinical story.
IV. Failure pattern 2: Broken attribution and denominator errors
Attribution errors undermine VBC programs even when coding is strong.
Common issues:
- Patient exists in the payer panel but not in the EHR panel.
- Patient assigned to the wrong PCP in one system.
- Patient moves locations, and the contract view is never updated.
This becomes more urgent as more members adopt accountable care models. The Medicare Shared Savings Program generated more than 2.1 billion dollars in net savings in 2023.
Organizations that cannot clean their attribution lose access to these opportunities.
A. Our attribution rescue pattern using HealthConnect CoPilot
- Ingest payer attribution files, eligibility files, and claims.
- Match against EHR panels and the master patient index.
- Surface mismatches for operations teams to resolve.
- Publish a clean attribution registry as FHIR Group or CareTeam resources.
Once that is done, gap lists and clinician views finally align.
V. Failure pattern 3: Quality measures built on the wrong fields
Quality programs continue to expand and rely on standard measures.
- NCQA Health Plan Ratings include HEDIS, CAHPS, and HOS measures.
- CMS quality ratings for marketplace and Medicare plans depend on clean and complete clinical data.
Common mapping failures include:
- Colonoscopies are stored as free text instead of coded procedures
- Blood pressure values in custom flowsheets
- Pharmacy fills stored in external vendor tables with poor member matching
How to fix it
- Use AI Medical Summary to identify and measure events hidden in narrative notes.
- Use CarePlan AI to generate next-step tasks linked to measure definitions.
- Build a FHIR-based quality layer that standardizes Observations, Procedures, and Medications.
This reduces quality drift and improves Stars and HEDIS performance.
Rescue broken attribution before it costs you shared savings
VI. How a 90-day FHIR quick-start fixes value-based care data challenges?
The CMS Interoperability and Patient Access Final Rule established a baseline expectation that payers and providers use FHIR APIs for key datasets.Most mid-sized organizations benefit from a narrow, focused rollout.
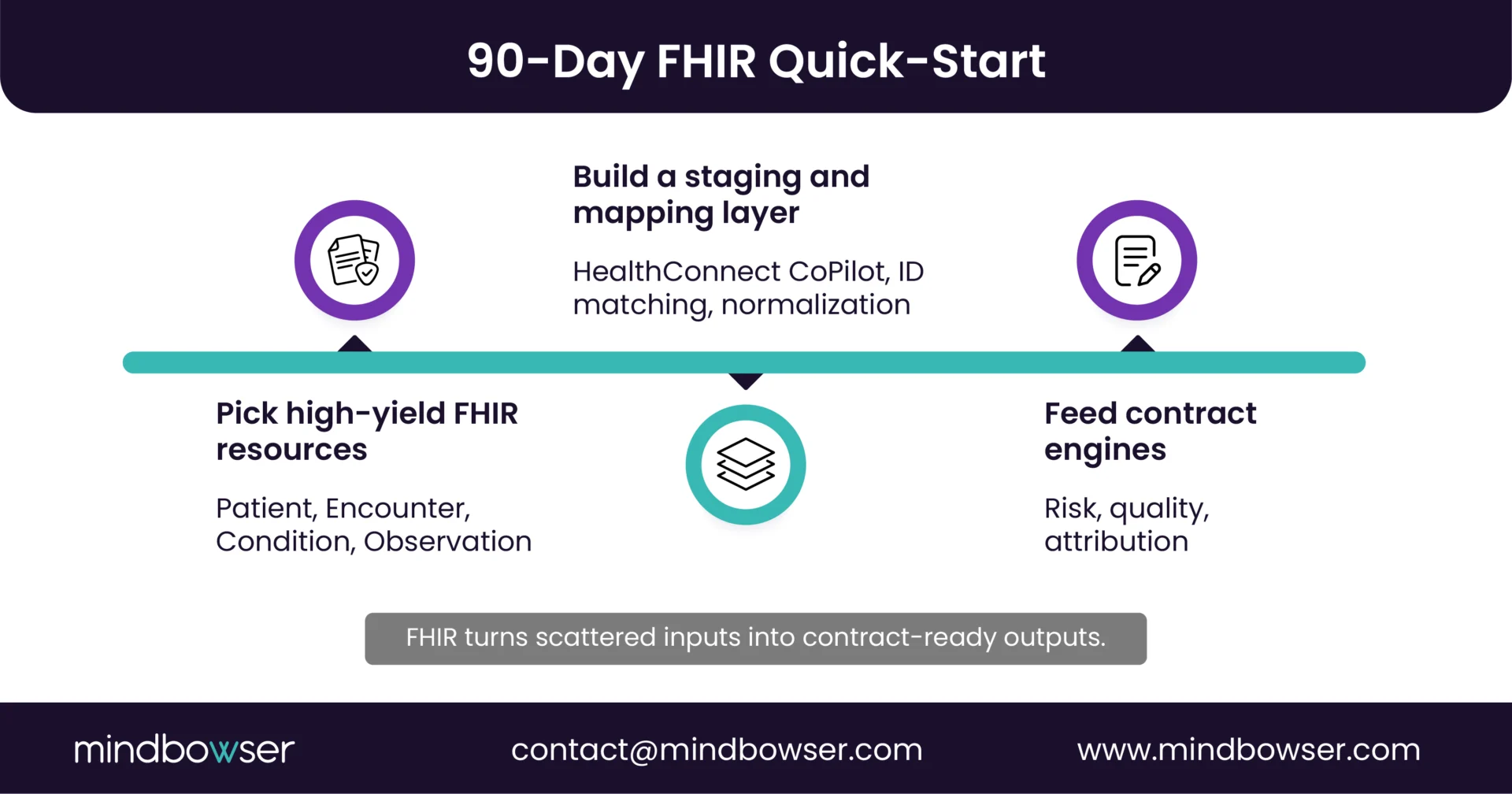
A. Step 1: Select high-yield FHIR resources
- Patient
- Practitioner
- Encounter
- Condition
- Procedure
- Observation
- MedicationRequest or MedicationDispense
B. Step 2: Build a claims and clinical staging layer
- Ingest claims, EHR extracts, labs, RPM, and pharmacy data
- Use HealthConnect CoPilot to normalize, match, and map
- Add provenance tags for audit readiness
C. Step 3: Wire FHIR into risk, quality, and attribution
- Feed Condition and Encounter data to risk engines
- Feed Observations and Procedures to quality engines
- Use FHIR APIs for payer and partner data exchange
This turns fragmented data into a contract-grade foundation.
VII. How does an attribution rescue work in practice?
Once the FHIR layer is in place, attribution cleanup becomes predictable.
A. Workflow
- Gather payer panels, rosters, and eligibility files.
- Compare with EHR PCP assignments using HealthConnect CoPilot.
- Flag mismatches for operations staff.
- Save the final attribution list in the FHIR Group or CareTeam resources.
- Use this registry for gap closure, Stars, outreach, and reporting.
Even small organizations can recover thousands of “lost” patients across contracts.
VIII. What “good” looks like for a CIO
A successful VBC program does not need a large analytics platform. It requires reliable, contract-grade data.
A. Checklist
- One source of truth for risk, quality, and attribution
- Traceable provenance for every important field
- Aligned definitions across finance, clinical, and analytics teams
- Ability to explain measure denominators in under five minutes
- Compliance with CMS and NCQA definitions and rules
The Medicare Shared Savings Program shows the upside. When data and operations align, collective savings exceed billions each year.
IX. What This All Means for Your Next Contract Year?
Value-based care does not reward organizations that document more. It rewards organizations that align the financial story in claims with the clinical story in charts. When that alignment happens, RAF scores stabilize, attribution becomes predictable, and quality measures finally match what nurses and physicians see every day; when it does not, even strong clinical programs underperform.
Your path forward does not require a new platform. It requires contract-grade data plumbing that reconciles claims and clinical inputs, standardizes them through a FHIR layer, and supports audit-ready attribution and quality logic.
Organizations that make this shift position themselves to benefit from the broader VBC landscape, including the more than 2.1 billion dollars in shared savings delivered by the Medicare Shared Savings Program in 2023.
If your top three value-based contracts produce numbers your clinical and analytics teams cannot defend in five minutes, it is time to rebuild the foundation. We can help you design a blueprint, run a 90-day FHIR quick-start, and implement attribution and quality workflows that produce reliable results for every reporting cycle.
How does Mindbowser help?
We work with organizations that have data but lack contract-grade alignment. Our focus is on the plumbing under VBC programs.
What we build:
- Value-based care data blueprint
- FHIR and integration quick-start (CMS-9115-F compliant)
- Clinical workflow automation with AI Medical Summary and CarePlan AI
- Attribution rescue via HealthConnect CoPilot
- Quality and risk mapping governance
We do not sell an off-the-shelf VBC platform.
We build custom data pipelines and AI helpers that make existing systems perform like a VBC-ready stack.


