



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
- Pediatric telehealth urgent care is shifting from a convenience feature to a core care delivery model, driven by rising demand, ER overload, and caregiver preference for instant access.
- Platforms that succeed are built around pediatric-specific workflows, real-time triage, deep EHR integrations, and compliance by design, not generic telemedicine layers.
- The real advantage comes from custom architecture that enables safe scaling, faster decision-making, and measurable ROI across the care continuum.
What if the first touchpoint in pediatric care didn’t start in the ER but on a screen?
Parents today expect immediate answers, not long wait times.
At the same time, health systems are under pressure to reduce unnecessary emergency visits and improve access. This is where pediatric telehealth urgent care is reshaping care delivery.
The real question is not whether to adopt it but how to build it right for scale, safety, and long-term value.
I. Why Pediatric Telehealth Urgent Care Is Becoming a Core Digital Health Opportunity
What if your fastest-growing patient segment is also your most underserved?
That’s the paradox in pediatric care today.
Health systems are seeing steady pediatric demand, yet access remains fragmented. Parents don’t think in care settings. They think in urgency. Fever at 9 PM. Rash before school. Breathing issues on the weekend.
And when access fails, they default to the emergency room.
“Pediatric urgent care demand isn’t increasing. It’s being redirected often inefficiently.”
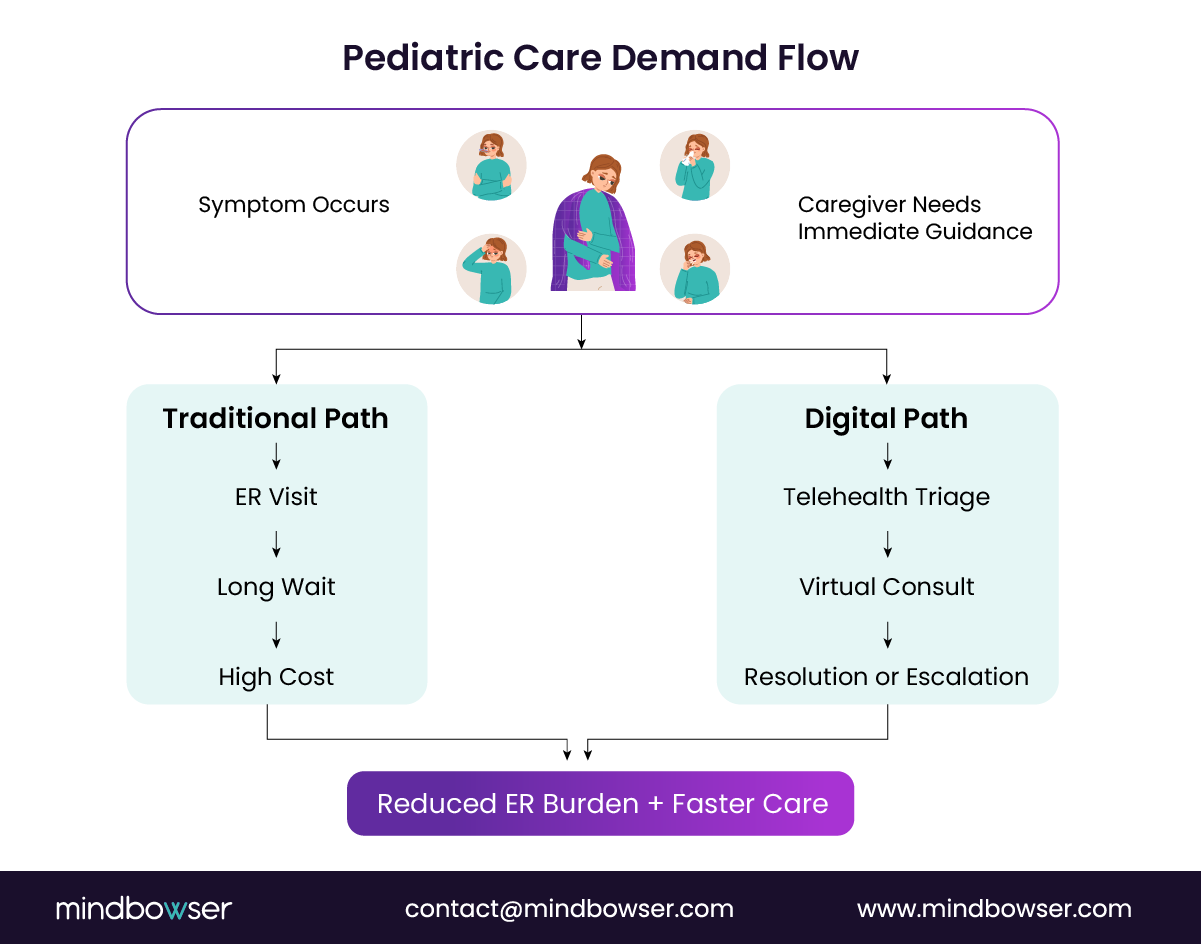
The numbers make the case. The CDC reports that over 25% of pediatric emergency department visits are non-urgent, meaning they could be treated in lower-acuity settings such as telehealth. At the same time, McKinsey notes that telehealth utilization remains ~38x higher than pre-pandemic levels, with sustained demand across family care segments.
This creates a clear product signal.
- Demand is real and recurring
- Access points are misaligned
- Digital channels are now trusted
So the opportunity isn’t to digitize urgent care. It’s to redefine how pediatric urgent care is accessed, triaged, and delivered.
For product and technology leaders, this is where strategy shifts.
Are you building a feature inside a broader platform?
Or are you building a pediatric telehealth urgent care system that becomes the front door to care?
Because those are two different plays.
The first adds convenience.
The second captures demand, drives retention, and reduces downstream costs.
And here’s the nuance most teams miss.
Pediatric care is not just “telehealth for smaller patients.” It introduces:
- Caregiver-led interactions
- Age-specific clinical protocols
- Higher sensitivity to safety and escalation
Which means generic telehealth platforms struggle to adapt.
Pediatric telehealth urgent care is emerging as a distinct product category rather than a feature layer. The teams that treat it that way will move faster and scale cleaner.
Let’s break down the forces driving this shift.
A. Why traditional urgent care models struggle with pediatric demand
Walk into a pediatric ER during peak hours. You’ll see a pattern.
Fever. Ear pain. Mild respiratory symptoms. Skin rashes.
High volume. Low acuity. Long wait times.
This isn’t accidental. It’s structural.
Emergency departments are designed for critical care. Pediatric demand, however, is episodic, unpredictable, and often non-emergent. That mismatch creates operational strain.
A Deloitte analysis shows that non-emergency ER visits can cost up to 2-5 times as much as urgent or virtual care alternatives. Yet families still choose ERs. Why?
Access.
- Pediatricians are not always available on the same day
- Urgent care centers may lack pediatric specialists
- Parents prioritize immediacy over setting
So the system absorbs avoidable load.
Now layer in workforce constraints.
Not every urgent care facility has pediatric-trained clinicians. That increases diagnostic variability, raises escalation rates, and slows throughput.
The result is a three-part failure:
- Capacity mismatch during demand spikes
- Cost inefficiency across care settings
- Inconsistent pediatric expertise
And for health systems, this translates directly into margin leakage and poor patient experience.
Traditional urgent care models react to pediatric demand. They don’t absorb or redistribute it efficiently.
B. Why telehealth is uniquely suited for pediatric urgent care
Why do parents reach for their phone before anything else?
Because in pediatric care, speed beats location.
A child spikes a fever at night. A rash appears before school. A cough worsens over hours, not days. These are not scheduled events. They are moment-of-need decisions, and traditional care models are not built for that cadence.
Telehealth is.
“Convenience isn’t the value. Immediate clinical reassurance is.”
Here’s what makes pediatric telehealth urgent care structurally aligned with demand:
First, most pediatric urgent cases are visually diagnosable or symptom-driven. Conditions like rashes, mild respiratory issues, conjunctivitis, and ear pain can often be assessed through guided virtual exams and caregiver input.
Second, caregiver presence is already built into the interaction. Unlike adult care, pediatric visits always involve a parent or guardian. That makes virtual consultations not just viable, but often more efficient.
Third, the economics work.
A study published in Health Affairs found that telehealth visits can reduce care costs by up to 50% compared to in-person urgent care or ER visits, particularly for low-acuity conditions. For payers and providers, that’s immediate ROI. For product leaders, that’s a scalable business model.
Now layer in a behavioral shift.
Parents have crossed the trust barrier. During and after the pandemic, virtual pediatric visits became normalized. What started as a necessity is now a preference.
So the model flips.
- Instead of “go somewhere for care.”
- It becomes “access care instantly.”
And that shift matters.
Because once telehealth becomes the first touchpoint, it can:
- Filter unnecessary ER visits
- Route high-risk cases appropriately
- Capture longitudinal patient data early
That’s not just convenience. That’s system-level efficiency.
Here’s the strategic insight most teams underestimate.
Telehealth is not replacing urgent care. It’s absorbing the front layer of demand and redistributing it intelligently across the care continuum.
Pediatric telehealth urgent care works because it matches how demand actually shows up: unplanned, urgent, and caregiver-driven.
C. Why digital health startups are investing
If the demand is obvious, why isn’t every platform winning here?
Because execution is harder than it looks.
The surface opportunity in pediatric telehealth urgent care is clear. High volume. Repeat usage. Strong payer interest. But underneath, it requires tight alignment between clinical workflows, product design, and infrastructure.
That’s exactly where startups see an opening.
“Pediatric urgent care is one of the few segments where better product design directly reduces the cost of care.”
Here’s what’s driving investment.
First, sustained telehealth adoption is no longer speculative. According to McKinsey, up to 76% of consumers are interested in using telehealth going forward, with family care and pediatrics among the highest intent categories. This is not a pandemic spike. It’s a behavioral reset.
Second, health systems are actively looking for demand redistribution models.
Hospitals don’t want more ER visits. They want:
- Lower-cost care settings
- Better triage before admission
- Higher patient retention within their network
Pediatric telehealth urgent care platforms solve all three.
Third, specialized networks create defensibility.
Generic telehealth platforms compete on access. Pediatric-focused platforms compete on clinical depth, caregiver experience, and outcomes. That difference matters when you’re selling to health systems or scaling across markets.
Now consider the product advantage.
Legacy systems do not constrain startups. They can:
- Design pediatric-first triage engines from day one
- Build API-first integrations with EHRs and pharmacies
- Embed clinical decision support tailored to age groups
That leads to faster iteration and tighter feedback loops.
But here’s the real reason capital is flowing.
Recurring use.
Pediatric urgent care is not episodic in the same way adult specialty care is. Families return. Conditions repeat. Trust compounds.
That creates:
- Higher lifetime value per user
- Lower acquisition cost over time
- Stronger platform stickiness
And investors notice patterns like that.
Digital health startups are investing in pediatric telehealth urgent care because it combines high demand, repeat usage, and clear ROI when built correctly.
The catch?
It only works if the platform is designed for pediatric care from the ground up.
III. What Clinical Workflows Must Pediatric Telehealth Urgent Care Platforms Support?
What breaks first when you scale pediatric telehealth?
Not infrastructure. Not a video.
Workflows.
Because pediatric urgent care isn’t just about connecting a clinician to a patient, it’s about making the right decision, fast, with incomplete information and a caregiver in the loop.
“Bad workflows don’t just slow care. They increase clinical risk.”
This is where many platforms fail. They replicate adult telehealth flows and expect pediatric care to fit inside them. It doesn’t.
To build a scalable pediatric telehealth urgent care platform, workflows must be:
- Symptom-driven, not appointment-driven
- Risk-aware, not first-come-first-served
- Caregiver-guided, not patient-led
And most importantly, they must support real-time triage and escalation.
Let’s break down what that actually means.
A. How pediatric triage works
How do you decide in under 60 seconds whether a child needs ER care or a virtual consult?
That’s the core challenge of pediatric triage.
Unlike adult care, pediatric triage depends heavily on age, symptom progression, and caregiver-reported context. A mild fever in a 10-year-old is routine. The same symptom in a 3-month-old can be critical.
So the workflow must start with structured symptom intake rather than free-form input.
1. Symptom-based triage
The system captures:
- Primary symptom (fever, cough, rash, injury)
- Duration and severity
- Age-specific modifiers (infant vs toddler vs adolescent)
This isn’t just data collection. It feeds into clinical decision logic that determines the next step.
Think of it as a decision tree, not a form.
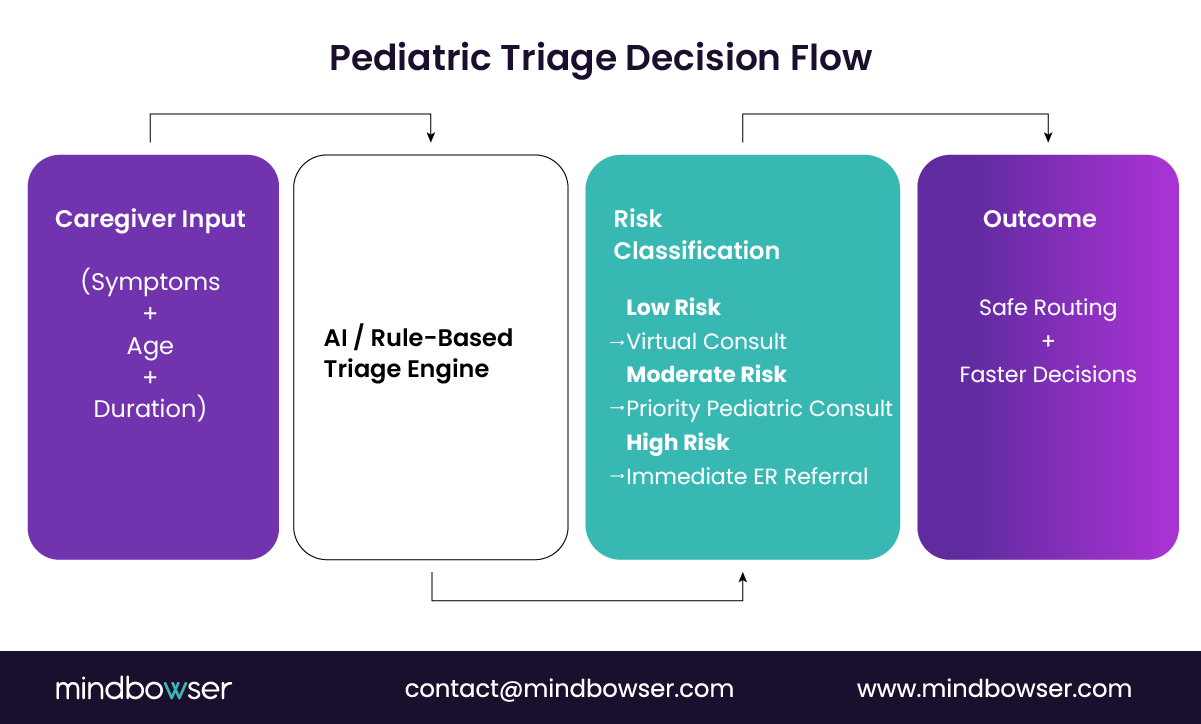
2. Risk stratification
Once inputs are captured, the platform must classify risk:
- Low risk: route to virtual consult
- Moderate risk: prioritized consult with pediatric clinician
- High risk: immediate ER referral or escalation
Here’s where product design meets clinical safety.
A study in Pediatrics highlights that structured triage protocols significantly reduce inappropriate care routing and improve outcomes in urgent pediatric settings. That’s not optional at scale. That’s foundational.
3. Escalation workflows
This is where most systems fall short.
If a case cannot be safely handled virtually, the platform must:
- Trigger real-time escalation alerts
- Provide clear caregiver instructions
- Route data to downstream care settings (ER, in-person clinic)
No ambiguity. No delay.
Because in pediatric care, hesitation creates risk.
Here’s the strategic takeaway.
Triage is not a feature. It is the control layer of your entire pediatric telehealth urgent care platform.
Get it right, and you reduce unnecessary visits, improve outcomes, and scale safely.
Get it wrong, and everything downstream breaks.
Pediatric triage workflows must be structured, dynamic, and tightly integrated with escalation logic.
B. Conditions treated
What actually gets resolved in a pediatric telehealth urgent care visit?
This is where skepticism often shows up.
Can virtual care really handle pediatric urgency?
The answer is yes, but only if the platform is designed around the right set of conditions and clinical pathways.
“Pediatric telehealth doesn’t replace all urgent care. It absorbs the right 60-70%.”
That’s the sweet spot.
Most pediatric urgent cases fall into low-to-moderate acuity categories that are highly protocol-driven and visually assessable. When triage is done correctly, these cases can be resolved safely without in-person visits.
Here’s how that breaks down.
1. Fever management
Fever is one of the most common pediatric complaints.
The workflow focuses on:
- Age-specific thresholds (infants vs older children)
- Associated symptoms (lethargy, rash, dehydration)
- Duration and response to medication
For most cases, clinicians can guide caregivers on home management. High-risk cases are escalated immediately.
2. Skin conditions
Rashes, allergic reactions, insect bites, and mild infections.
These are ideal for telehealth because they are visually diagnosable. High-resolution video and image uploads allow clinicians to assess patterns quickly.
A study published in JAMA Dermatology found that tele-dermatology achieves diagnostic concordance rates above 80% compared to in-person visits. That’s strong clinical confidence for pediatric use cases.
3. Respiratory issues
Cough, cold, mild asthma symptoms, and upper respiratory infections.
Through guided questioning and observation, clinicians assess:
- Breathing patterns
- Severity markers (retractions, wheezing)
- Risk factors based on age and history
Low-risk cases are managed virtually. Red flags trigger escalation.
4. Ear infections
Ear pain is a frequent driver of urgent visits.
While physical examination has limits, a structured symptom assessment combined with caregiver-reported indicators allows clinicians to:
- Initiate treatment when appropriate
- Recommend follow-up if needed
This reduces unnecessary clinic visits while maintaining the quality of care.
5. Minor injuries
Cuts, bruises, mild sprains.
Telehealth enables:
- Visual assessment
- First-aid guidance
- Decision on whether imaging or in-person care is needed
This prevents overutilization of ER services for low-risk injuries.
So what’s the boundary?
High-acuity conditions. Severe trauma. Complex diagnostics.
Those still belong in physical care settings.
But here’s the operational insight.
When platforms are designed around the right mix of conditions, they can safely handle most pediatric urgent demand while filtering out high-risk cases early.
Pediatric telehealth urgent care succeeds by focusing on high-volume, protocol-driven conditions that can be safely triaged and managed virtually.
C. How pediatric care differs
Why do standard telehealth workflows break the moment a child enters the equation?
Because pediatric care is never a one-user interaction.
It’s a three-layer interaction:
- Child (patient)
- Caregiver (decision-maker)
- Clinician (diagnostic authority)
Miss that, and your product creates friction fast.
“Pediatric care is not delivered to the patient alone. It is mediated through the caregiver.”
That single shift changes everything.
1. Caregiver-led interactions
In adult telehealth, the patient directly describes symptoms.
In pediatrics, caregivers interpret and report them.
That introduces:
- Subjectivity in symptom reporting
- Variability in accuracy
- Emotional bias under stress
So your platform must guide the caregiver.
Not just collect input. Guide it.
That means:
- Structured prompts (“Is the child responsive?” vs open text)
- Visual aids (rash examples, breathing patterns)
- Real-time clarification during intake
This reduces ambiguity and improves the quality of clinical decisions.
2. Pediatric-specific clinical protocols
Here’s where generic platforms fail quietly.
Pediatric care is age-sensitive at every step:
- Medication dosing varies by weight and age
- Symptom severity thresholds change across age groups
- Risk tolerance is lower, especially for infants
A fever is not just a fever.
In a newborn, it’s an emergency signal. In a 12-year-old, it may be routine.
That means your system must embed:
- Age-aware triage logic
- Pediatric dosing safeguards
- Condition-specific care pathways
According to the American Academy of Pediatrics, clinical decision-making in children must account for developmental stage and age-specific risk factors, reinforcing the need for tailored workflows.
3. Consent and compliance complexity
Now layer in regulatory friction.
Pediatric telehealth introduces additional compliance requirements:
- Verified caregiver identity
- Consent for treatment
- State-specific telehealth regulations for minors
And this is where scaling often slows down.
If consent workflows are manual or inconsistent, you create:
- Legal exposure
- Delayed consultations
- Poor user experience
The solution is not more forms. It’s embedded compliance workflows.
- Pre-visit digital consent capture
- Identity verification tied to caregiver accounts
- Audit-ready documentation trails
Built once. Enforced every time.
Here’s the strategic insight.
Most telehealth platforms are built for a single user journey. Pediatric care requires multi-actor orchestration with higher clinical sensitivity.
That’s not a UI tweak. That’s a system design decision.
Pediatric telehealth urgent care platforms must be caregiver-centric, protocol-driven, and compliance-aware by design.
IV. What Core Features Power Scalable Pediatric Telehealth Urgent Care Solutions?
What separates a pilot telehealth product from a platform that actually scales?
Not a video. Not UI polish.
It’s the depth of clinical, caregiver, and operational features working together as a system.
Because once demand increases, gaps show up fast. Missed context. Delayed routing. Incomplete documentation. And suddenly, your “telehealth solution” becomes a bottleneck.
“Features don’t scale platforms. Integrated capabilities do.”
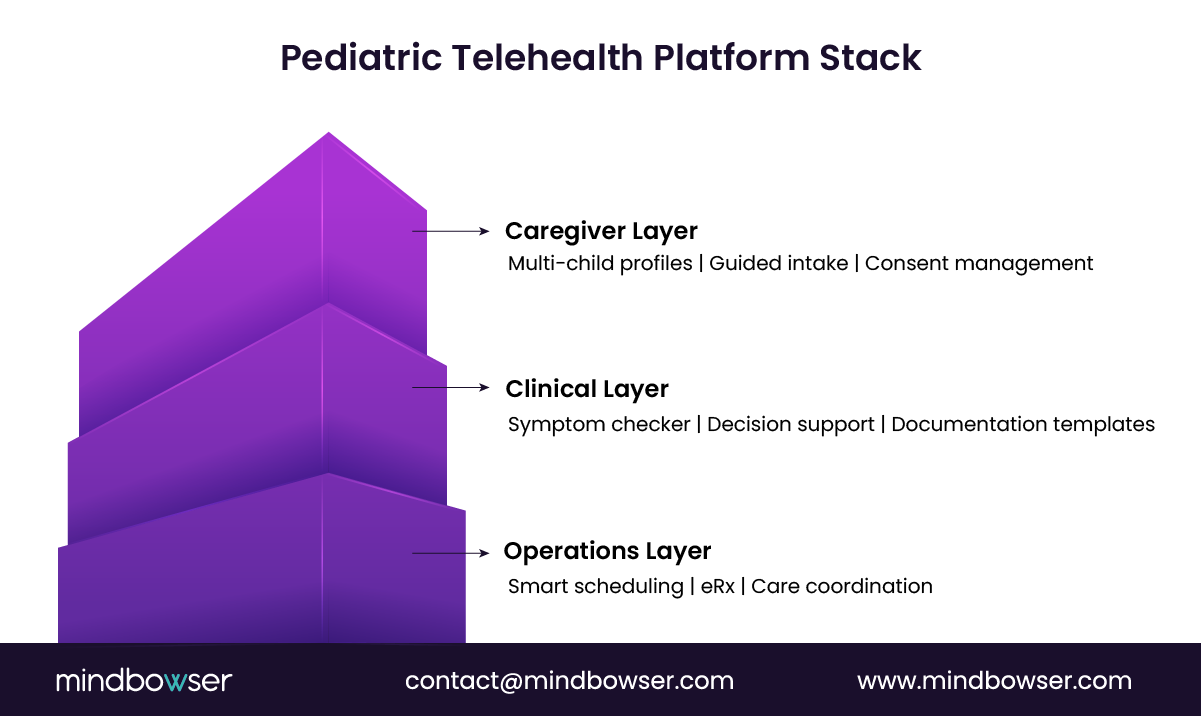
For pediatric telehealth urgent care, those capabilities must align across three layers:
- Patient and caregiver experience
- Clinical decision support
- Operational execution
Let’s break them down.
A. Platform capabilities
If the front door is digital, what must it handle from day one?
Everything the caregiver needs to start, continue, and trust the care journey.
1. Video consultation built for pediatric care
This isn’t a generic video.
Pediatric consults require:
- Multi-participant support (parent + child + clinician)
- High-quality visuals for skin, throat, and behavioral cues
- Low-latency performance for real-time assessment
A laggy call isn’t just frustrating. It impacts diagnosis.
2. Pediatric patient profiles
Every interaction should build context.
That means structured profiles capturing:
- Age, weight, and developmental stage
- Vaccination history
- Allergies and chronic conditions
Why does it matter?
Because pediatric care decisions are context-heavy, without this data, clinicians rely on fragmented input, increasing risk.
3. Caregiver accounts and controls
Remember the three-layer interaction.
Caregivers must be able to:
- Manage multiple children under one account
- Provide consent seamlessly
- Access visit history and care plans
This is not a UX nice-to-have. It’s foundational.
A confusing caregiver experience leads to drop-offs before the consult even begins.
Here’s the product insight.
The platform layer is not just about access. It’s about reducing friction before clinical interaction begins.
Get this right, and you increase:
- Visit completion rates
- Care continuity
- Patient retention
Platform capabilities must be designed around caregiver-led access and pediatric context, not generic telehealth flows.
B. Clinical tools
What ensures clinical quality doesn’t drop as volume increases?
Not more clinicians.
Better tools.
Because in pediatric telehealth urgent care, clinicians are making decisions fast, often with limited physical examination. The platform must augment clinical judgment, not slow it down.
Clinical speed without decision support increases risk. Clinical speed with the right tools increases throughput.
Here’s what that looks like in practice.
1. Pediatric symptom checkers
This is where every visit begins.
But most symptom checkers are built for adults. That’s a problem.
Pediatric symptom checkers must be:
- Age-aware (infant vs toddler vs adolescent)
- Structured for caregiver input
- Designed to surface red flags early
Instead of asking, “What are you feeling?”, the system asks:
- “Is the child feeding normally?”
- “Any difficulty breathing?”
- “How long has the fever lasted?”
This creates clinically usable input, not vague descriptions.
And it feeds directly into triage logic.
2. Clinical decision support (CDS)
This is the backbone of safe scaling.
CDS systems guide clinicians with:
- Evidence-based pediatric protocols
- Risk alerts based on symptoms and age
- Recommended next steps (treat, monitor, escalate)
According to research published in BMJ Quality & Safety, clinical decision support systems can improve adherence to care guidelines by up to 30%, especially in high-variability environments like urgent care.
That’s not just quality improvement. That’s consistency at scale.
3. Pediatric documentation templates
Documentation is where speed usually breaks.
Free-text notes slow clinicians down and create inconsistency. In pediatric care, that risk is amplified due to:
- Consent requirements
- Weight-based dosing
- Detailed symptom history
Structured templates solve this.
They enable:
- Faster charting during or post-consult
- Standardized clinical records
- Audit-ready documentation for compliance
And here’s the hidden ROI.
Better documentation reduces:
- Claim denials
- Legal exposure
- Rework across care teams
Here’s the strategic takeaway.
Clinical tools are not back-office features. They are real-time enablers of safe, efficient care delivery.
Without them, scaling means adding more clinicians.
With them, scaling means increasing throughput per clinician without compromising safety.
Pediatric telehealth urgent care platforms must embed symptom intelligence, decision support, and structured documentation into every consult.
C. Operational features
What keeps the system moving when demand spikes at 7 PM on a weekday?
Operations.
Because even the best clinical workflows fail when patients can’t be routed, prescriptions are delayed, or follow-ups fall through.
“Operational gaps don’t show up in demos. They show up in drop-offs, delays, and lost revenue.”
For pediatric telehealth urgent care, operational features must ensure speed, continuity, and coordination across the care journey.
1. Smart scheduling and queue management
Pediatric urgent care is not appointment-first. It’s demand-first.
That means your system must handle:
- On-demand consults
- Dynamic queue prioritization based on triage severity
- Load balancing across available pediatric clinicians
This is where many platforms break.
If every case enters a flat queue, high-risk patients wait longer than they should. That’s a clinical and operational failure.
A better approach?
- Triage-driven routing
- Priority-based queues
- Real-time clinician availability mapping
This reduces wait times while improving care quality.
2. ePrescription (eRx) workflows
A consult without closure creates friction.
For pediatric care, prescriptions must be:
- Weight and age-adjusted
- Sent to the caregiver’s preferred pharmacy instantly
- Logged with clear dosage instructions
Delays here lead to:
- Care gaps
- Increased follow-up calls
- Poor patient experience
According to the American Medical Association, e-prescribing improves medication adherence and reduces errors compared to handwritten prescriptions, especially in outpatient settings.
In pediatric urgent care, that’s critical.
3. Care coordination and follow-ups
What happens after the consult?
This is where long-term value is created.
Platforms must enable:
- Automated visit summaries for caregivers
- Follow-up reminders (especially for unresolved symptoms)
- Escalation tracking if symptoms worsen
And importantly:
- Data handoff to primary care providers or EHR systems
Without this, telehealth becomes a silo.
With it, telehealth becomes part of the longitudinal care journey.
Here’s the operational insight.
Speed gets patients in. Coordination keeps them in your system.
When operational features are tightly integrated, you:
- Reduce no-shows and drop-offs
- Improve treatment adherence
- Increase repeat usage
That’s where ROI compounds.
Operational features must ensure real-time access, seamless prescription flow, and continuous care beyond the virtual visit.
Ready to Build a Pediatric Telehealth Platform That Scales Safely?
V. What Technology Architecture Enables Pediatric Telehealth Platforms to Scale?
What breaks when your pediatric telehealth urgent care platform goes from 50 visits a day to 5,000 visits a day?
Not demand. Not even clinicians.
Architecture.
Because scaling pediatric telehealth urgent care isn’t just about handling more users. It’s about handling more complexity per interaction: triage logic, caregiver workflows, clinical safety checks, and real-time integrations.
“Scaling telehealth is easy. Scaling safe pediatric telehealth is not.”
This is where many Series B+ teams hit a wall. Early MVP architectures, often stitched together with third-party tools, start failing under:
- Latency during peak hours
- Fragmented data across systems
- Compliance gaps under audit pressure
So the shift becomes inevitable.
From feature-based builds to platform-grade architecture
Let’s break down what that requires.
A. Infrastructure
Can your platform handle peak pediatric demand without degrading care quality?
That’s the bar.
1. Cloud-native foundation
Pediatric urgent care demand is unpredictable.
Evenings. Weekends. Seasonal spikes (think flu season).
A cloud-native setup allows you to:
- Auto-scale compute during demand surges
- Maintain performance across geographies
- Deploy updates without downtime
This ensures availability when it matters most.
2. High-availability video infrastructure
Video is not just a feature. It’s a diagnostic tool.
So your architecture must support:
- Low-latency, high-resolution streaming
- Failover mechanisms (fallback to audio or reconnect flows)
- Multi-party sessions (caregiver + child + clinician)
A dropped call in pediatric care isn’t just inconvenient. It disrupts clinical continuity.
3. Secure data architecture
Pediatric data is sensitive. More stakeholders. More compliance layers.
Your system must ensure:
- End-to-end encryption (in transit and at rest)
- Role-based access controls (caregiver vs clinician vs admin)
- Audit trails for every interaction
HIPAA compliance is table stakes. The real challenge is maintaining it at scale without slowing the system down.
Here’s the architecture insight.
Infrastructure is not just about uptime. It’s about ensuring clinical reliability under load.
If performance drops, decision-making slows. If security gaps appear, scaling stops.
Pediatric telehealth urgent care platforms must be cloud-native, video-resilient, and security-first from day one.
B. Interoperability
What happens after the consult ends? Does your data move or does it stall?
This is where most pediatric telehealth urgent care platforms quietly fail.
Without interoperability, telehealth becomes a dead-end interaction rather than part of the care continuum.
Disconnected telehealth creates convenience. Connected telehealth creates clinical value.
For product and technology leaders, interoperability is not a compliance checkbox. It’s a lever for growth and retention.
1. EHR integration
Every pediatric interaction generates critical data:
- Symptoms and triage decisions
- Diagnoses and prescriptions
- Follow-up recommendations
If this data doesn’t flow into the EHR, you create:
- Fragmented patient records
- Duplicate documentation work
- Poor continuity of care
A report from HIMSS highlights that interoperability gaps remain a top barrier to effective care coordination, directly affecting outcomes and operational efficiency.
So what’s required?
- Bi-directional data exchange
- Real-time updates during or immediately after consults
- Support for major EHR systems (Epic, Cerner, Athenahealth)
This ensures that virtual care is not isolated. It’s embedded.
2. FHIR-based data exchange
Here’s where architecture meets speed.
FHIR (Fast Healthcare Interoperability Resources) enables:
- Standardized data formats
- Faster integrations across systems
- Modular expansion as your platform grows
Instead of building one-off integrations, you create a plug-and-play ecosystem.
For scaling teams, this matters.
Every new partnership, hospital, payer, and pharmacy should not require months of custom work.
FHIR reduces that friction.
3. Pharmacy and insurance integrations
The care journey doesn’t end with diagnosis.
It continues through:
- Medication fulfillment
- Coverage validation
- Claims processing
Without integration, caregivers face delays. Clinicians face rework. Platforms lose trust.
So your system must connect with:
- Pharmacy networks for real-time eRx delivery
- Insurance systems for eligibility checks and billing workflows
This enables:
- Faster treatment initiation
- Reduced administrative burden
- Cleaner revenue cycles
Here’s the strategic insight.
Interoperability is not about moving data. It’s about making every interaction part of a larger care system.
When done right, it:
- Improves clinical outcomes
- Reduces operational waste
- Strengthens partnerships with health systems and payers
Scalable pediatric telehealth urgent care platforms must be API-first, FHIR-enabled, and deeply integrated across the healthcare ecosystem.
C. AI and automation
If triage, routing, and documentation are manual, can you really scale?
Not for long.
Because pediatric telehealth urgent care isn’t just volume-heavy, it’s decision-heavy. Every interaction requires triage, risk assessment, documentation, and routing. Doing that manually slows throughput and increases variability.
“Automation doesn’t replace clinicians. It removes the friction around them.”
Here’s where AI and automation become essential.
1. AI-driven triage and intake
Instead of static forms, AI-enabled intake systems can:
- Dynamically adjust questions based on prior responses
- Flag high-risk symptoms in real time
- Pre-classify cases before clinician review
This reduces clinician cognitive load and shortens time-to-decision.
In high-volume pediatric settings, even a 30-40% reduction in intake time can significantly increase daily consult capacity.
2. Automated clinical documentation
Documentation is one of the biggest hidden bottlenecks.
AI-powered tools can:
- Convert consult conversations into structured notes
- Auto-fill pediatric templates
- Generate summaries for both EHRs and caregivers
This doesn’t just save time. It improves consistency.
And consistency is what enables safe scale.
3. Intelligent routing and load balancing
Not every case should go to the next available clinician.
AI-driven routing can:
- Match cases based on severity and clinician expertise
- Prioritize high-risk pediatric cases
- Distribute load across the network in real time
This ensures:
- Faster response times
- Better clinical outcomes
- Higher clinician efficiency
Here’s the architecture takeaway.
Infrastructure handles scale.
Interoperability connects systems.
AI makes the system intelligent under pressure.
Without automation, scaling means hiring more clinicians.
With it, scaling means doing more with the same clinical capacity.
AI and automation are the force multipliers that make pediatric telehealth urgent care platforms operationally and clinically scalable.
VI. What Compliance and Safety Challenges Must Pediatric Telehealth Platforms Address?
What slows scaling more than technology?
Compliance.
And in pediatric telehealth urgent care, the bar is higher.
Because you’re not just managing patient data. You’re managing minor patients, caregiver authority, and clinical risk in real time.
Compliance is not a blocker. It’s the foundation of trust and scale.
The challenge is this.
Most teams treat compliance as a post-build layer. But in pediatric care, that approach creates:
- Delays in go-live
- Rework in workflows
- Exposure during audits
The smarter approach is different.
Build compliance into workflows, architecture, and clinical decision-making from day one.
A. Compliance requirements
Who is consenting? Who is verified? Who is accountable?
These questions define pediatric telehealth.
Platforms must ensure:
- HIPAA-compliant data handling across video, messaging, and storage
- Caregiver identity verification before any consultation begins
- Digital consent capture aligned with state-specific minor care laws
Here’s the friction point.
If identity and consent are handled manually, you introduce delays and risk. If they’re embedded into the intake flow, they become invisible and repeatable.
That’s how you scale safely.
B. Clinical guidelines
Are your workflows aligned with pediatric standards, or are they just adapted from adult care?
That distinction matters.
Pediatric telehealth must align with:
- American Academy of Pediatrics (AAP) care guidelines
- Age-specific prescribing rules
- Documentation standards for minor care
Why?
Because clinical variability increases risk.
Structured adherence reduces it.
When guidelines are embedded into:
- Triage logic
- Decision support systems
- Documentation templates
You move from individual clinician judgment to system-supported consistency.
That’s what regulators and health systems expect.
C. Risk mitigation
What happens when a case is misclassified or deteriorates after the consult?
This is where safety systems must take over.
Effective platforms include:
- Clinical decision support alerts for high-risk scenarios
- Clear escalation protocols (ER referral, urgent follow-up)
- Physician oversight layers for edge cases
Patient safety research shows that standardized escalation protocols improve response times and reduce variability in urgent care decision-making, critical in pediatric cases where symptoms can evolve rapidly.
So the goal isn’t to eliminate risk. That’s not realistic.
The goal is to detect, route, and respond to risk faster than traditional care models.
Here’s the strategic takeaway.
Compliance and safety are not constraints. They are system design requirements.
When built correctly, they:
- Reduce legal exposure
- Increase partner trust (health systems, payers)
- Enable faster scaling across regions
Pediatric telehealth urgent care platforms must embed compliance, clinical standards, and risk controls directly into workflows, not bolt them on later.
VII. How Mindbowser Can Help Build Pediatric Telehealth Urgent Care Solutions
Why do so many pediatric telehealth platforms stall after MVP?
Because what works at 100 visits a week breaks at 1,000.
Generic tools get you to demo. They rarely get you to scale.
“Pediatric telehealth isn’t a feature you plug in. It’s a system you design.”
This is where a custom-build approach changes the trajectory.
A. Why custom development matters
Can a white-label telehealth platform support pediatric triage, caregiver workflows, and compliance at scale?
In most cases, no.
Here’s why:
- They are built for general telemedicine, not pediatric-specific workflows
- Triage logic is often static, not age-aware, or risk-adaptive
- Integration layers are limited, slowing EHR and pharmacy connectivity
So teams end up layering patches.
More tools. More workarounds. More friction.
Custom development flips this.
It allows you to:
- Build pediatric-first workflows from intake to escalation
- Embed clinical protocols directly into the system
- Design a scalable architecture aligned with your growth roadmap
And most importantly, you own the IP and control the roadmap.
That’s not just technical flexibility. That’s strategic leverage.
B. Capabilities
What does it take to build a production-grade pediatric telehealth urgent care platform?
Execution across three layers.
1. End-to-end telemedicine platform development
From caregiver onboarding to clinician workflows, platforms must support:
- Pediatric-specific intake and triage
- High-quality, multi-party video consults
- Structured clinical documentation
Built as one system. Not stitched together.
2. EHR and FHIR-based integrations
Continuity of care depends on connectivity.
Mindbowser enables:
- Bi-directional EHR integrations (Epic, Cerner, Athenahealth)
- FHIR-based APIs for faster interoperability
- Real-time data exchange across care systems
This ensures telehealth is not siloed. It’s embedded.
3. HIPAA-compliant, security-first architecture
Compliance is built into the foundation:
- Secure data handling across all touchpoints
- Role-based access and audit trails
- Scalable infrastructure aligned with HIPAA and SOC 2 requirements
So you don’t slow down when audits or partnerships scale.
C. Innovations
Where does differentiation come from once the basics are in place?
From intelligence and care orchestration.
1. AI-powered clinical documentation
Reduce clinician burden with:
- Automated note generation from consults
- Structured summaries for EHR and caregivers
- Consistent, audit-ready records
This increases throughput without increasing workload.
2. Remote patient monitoring (RPM) integration
Extend care beyond the visit.
For chronic or recurring pediatric conditions:
- Track symptoms over time
- Trigger alerts for deterioration
- Enable proactive interventions
This shifts care from reactive to continuous.
3. Care coordination platforms
Connect the full ecosystem:
- Primary care providers
- Specialists
- Caregivers
With shared data and communication flows.
This reduces fragmentation and improves outcomes.
Here’s the strategic takeaway.
The winners in pediatric telehealth urgent care will not be the fastest to launch.
They will be the ones who:
- Build custom, workflow-aligned systems
- Integrate deeply across the care ecosystem
- Use AI to increase clinical and operational efficiency
Custom-built pediatric telehealth platforms create long-term competitive advantage by aligning clinical safety, scalability, and product differentiation.
Why Pediatric Telehealth Urgent Care Is a Defining Bet for Digital Health Leaders
What if your next growth lever isn’t adding services but redesigning access? Pediatric telehealth urgent care is quickly becoming that lever. Demand is consistent, caregiver-driven, and increasingly digital-first. Health systems are looking for ways to reduce unnecessary ER utilization.
Startups are looking for repeatable, high-retention use cases. The intersection is clear. Platforms that align pediatric workflows, triage intelligence, and deep integrations don’t just improve access; they reshape how care enters the system. The difference comes down to architecture and intent. Build it as a feature, and you’ll compete on convenience.
Build it as a care delivery layer, and you’ll own the front door, improve outcomes, and create measurable ROI across the care continuum. Pediatric telehealth urgent care is not an extension of telehealth; it’s becoming the operating model for first-touch pediatric care.
Pediatric telehealth urgent care is a virtual care model that enables real-time diagnosis, triage, and treatment of non-emergency pediatric conditions through video consultations, supported by clinical workflows and decision systems.
It typically covers fever, respiratory infections, skin conditions, ear pain, minor injuries, and other low- to moderate-acuity issues that can be assessed virtually.
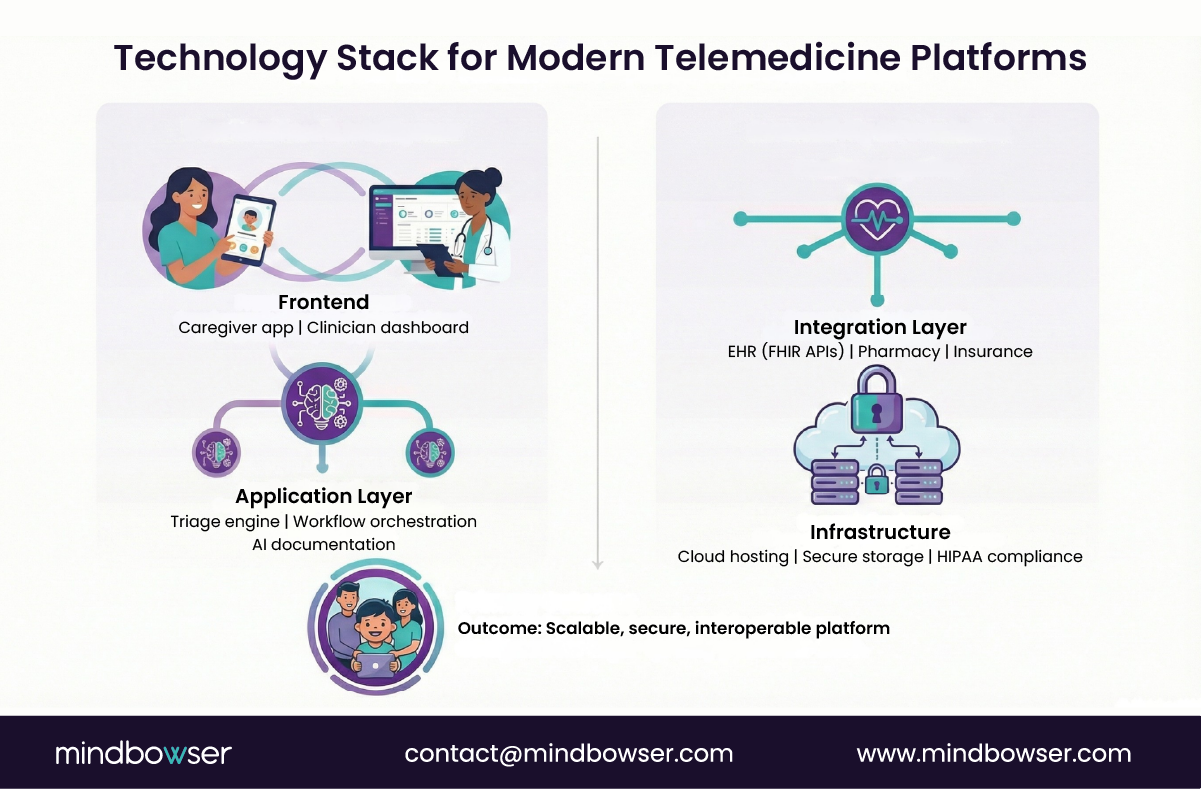
Most scalable platforms are built using custom architecture with pediatric-specific workflows, API-first integrations (EHR, pharmacy), and embedded compliance and clinical decision support systems.
Yes, when designed correctly. Safety depends on structured triage, adherence to pediatric guidelines, and strong escalation protocols for high-risk cases.
Core components include cloud-native infrastructure, secure video systems, FHIR-based interoperability, AI-driven triage and documentation, and compliance-ready data architecture.
Costs vary based on scope, integrations, and compliance requirements, but typically range from MVP builds to full-scale platforms depending on feature depth and scalability needs.


