



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
CMS now requires hospitals to screen all admitted adults for five social risk domains, while NCQA’s SNS-E measure scores plans on both screening and intervention (Social Need Screening and Intervention – NCQA – 2023). Leading systems treat SDOH screening as a data pipeline that drives Z-codes, automated outreach, and measurable reductions in ED use (Ballad Health Reduces ED Visits – Unite Us – 2025) and readmissions (SDOH2Health Emergency Diversion Pilot – SDOH2Health Case Study – 2024). This guide shows how to choose the right screening framework and build an AI-ready, closed-loop SDOH stack for value-based care.
“Are your SDOH workflows ready for the pressure of value-based care?”
If you are responsible for Pop Health, care management, or contracting, you already feel the pressure from CMS, NCQA, and your own utilization data. So here is the question every CIO, CMIO, and VP Pop Health now faces:
“If CMS or a major payer audited your social-needs workflows tomorrow, could you prove that your SDOH screening, coding, and intervention processes are compliant, digital, and driving measurable ROI?”
Most organizations cannot. Not because they lack good intentions, but because SDOH screening is often treated as a form rather than a contract-level performance engine.
Value-based care now demands a different approach. CMS created a five-domain inpatient SDOH screening requirement for all admitted adults.
NCQA formalized social-needs screening and intervention as a scored HEDIS measure. And CFOs now expect proof that closed-loop SDOH workflows reduce avoidable ED visits and readmissions, not just check a box.
This practical guide shows health-system leaders how to choose the right SDOH screening tools, build an AI-ready SDOH tech stack, and operationalize a 12–18 month roadmap that aligns with VBC economics.
I. What SDOH and HRSN mean in Value-based Care operations?
SDOH are societal conditions such as housing, food, transportation, utilities, and safety.
Health-related social needs (HRSN) are individual-level risks that directly affect health.
CMS formalized the operational layer by:
- Publishing the Accountable Health Communities HRSN Screening Tool, a 10-question set across five domains.
- Standardizing Z55–Z65 ICD-10-CM Z-codes for social needs.
- Introducing HCPCS G0136 for SDOH risk assessment, creating a billing pathway for screening.
In VBC, an SDOH program is not a survey. It is a workflow system that captures social risk, codifies it, and ties it to intervention and utilization outcomes.
II. Why is SDOH screening now a compliance requirement?
A. CMS inpatient mandate
Starting January 1, 2024, hospitals must screen all admitted adults for five domains: food, housing, transportation, utilities, and interpersonal safety. This rule is linked to new inpatient SDOH quality measures.
B. NCQA’s SNS-E HEDIS measure
SNS-E requires:
- A valid SDOH screening for selected social needs.
- A documented intervention for members who screen positive.
Forthcoming measure updates incorporate Z-codes and G-codes from claims and electronic sources.
C. VBC implication
Compliance is no longer optional. Paper tools, inconsistent workflows, or missing data will weaken Stars’ performance, contract outcomes, and audit readiness.
III. How to choose the right SDOH screening framework?
Most teams ask, “Should we use PRAPARE or the AHC tool?” Instead, leaders should ask:
“Which screening framework best fits our contracts, EHR, population, and reporting needs?”
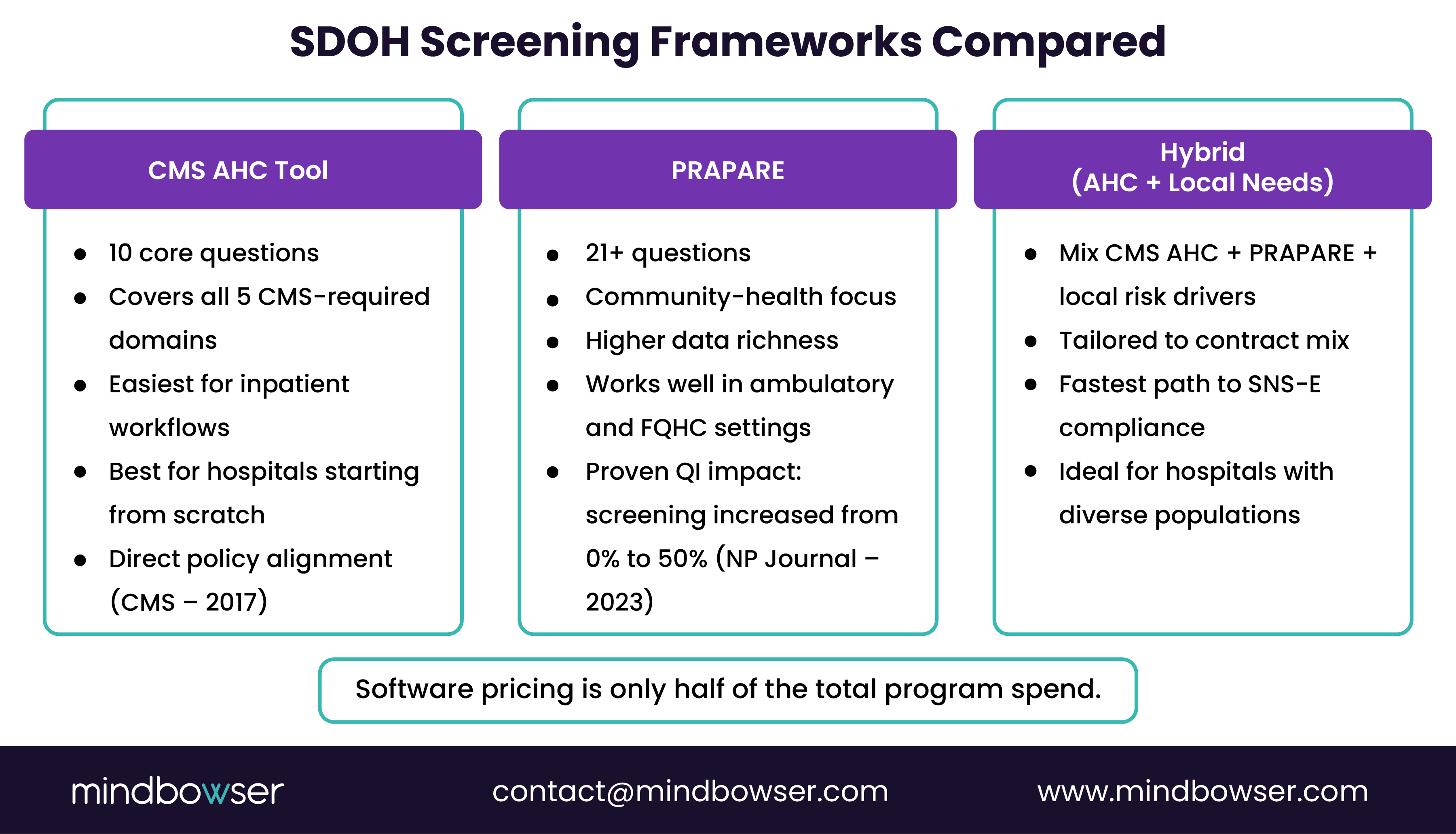
A. Three dominant frameworks
- CMS AHC HRSN Tool
- Simple, validated, aligned with federal policy.
- Covers the five required domains.
- PRAPARE
- Community-health-center-driven, more comprehensive.
- A practice using PRAPARE increased screening from 0% to 50%.
- Local Hybrid Tools
- Mix CMS AHC, PRAPARE, and local needs.
- Recommended when health systems have unique risk mixes.
B. Practical selection criteria
- Regulatory fit for CMS five-domain rule and SNS-E.
- EHR compatibility with Epic, Cerner, or Meditech.
- Population literacy and language mix.
- Burden on front-line staff.
C. How we implement
- Start with the CMS AHC base.
- Add 3–5 local questions.
- Map everything to FHIR and Z-codes.
- Deploy multi-channel screening using HealthConnect CoPilot accelerator.
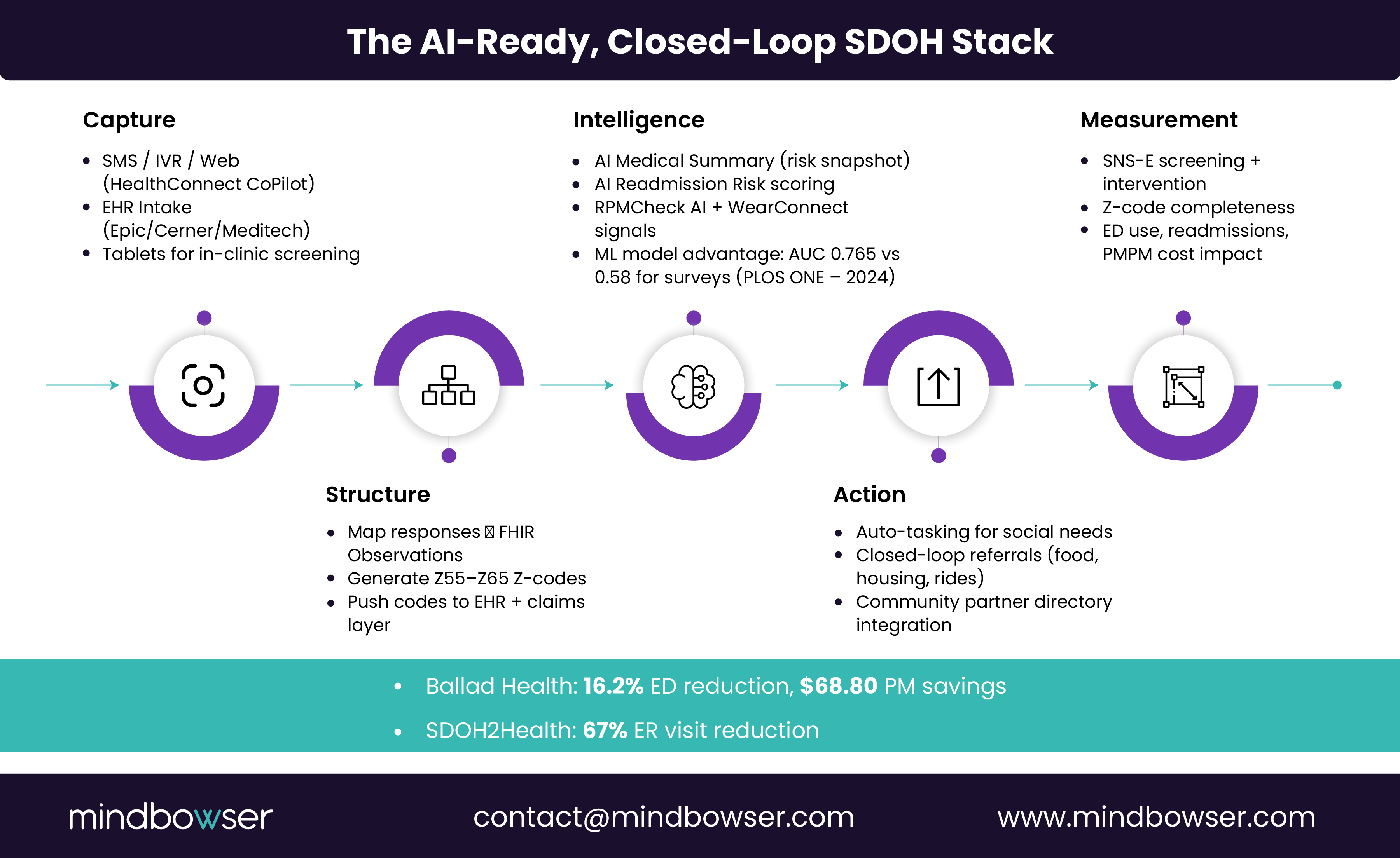
IV. What does an AI-ready SDOH tech stack look like?
The organizations moving the fastest treat SDOH screening as data infrastructure.
A. Capture layer
- EHR intake flows.
- Pre-visit SMS/IVR/web forms via HealthConnect CoPilot.
- Tablet-based in-clinic screens.
B. Structure layer
- Convert question responses to FHIR Observations.
- Trigger ICD-10-CM Z55–Z65 codes.
C. Intelligence layer
- AI Medical Summary generates fast, risk-based narratives for care managers.
- AI Readmission Risk blends social and clinical factors.
- RPMCheck AI and WearConnect enrich data with remote monitoring.
Evidence shows ML models (AUC ~0.765) outperform survey-only models (AUC ~0.58) for identifying HRSN needs.
D. Action layer
- Closed-loop referrals.
- Automated tasking for food, transportation, housing, and safety needs.
- Integration with community networks.
Ballad Health achieved a 16.2 percent overall ED reduction, 24.8 percent reduction for engaged patients, and $68.80 PMPM savings.
Measurement layer
- SNS-E HEDIS performance.
- Z-code completeness.
- Value-based care metrics such as ED rate, readmissions, and PMPM spend.
Rescue broken attribution before it costs you shared savings
V. How closed-loop SDOH programs drive measurable ROI?
Executives will ask: “Does this save money?”
A. Field evidence
- Ballad Health and Unite Us reported $68.80 in PMPM savings, with strong reductions in ED volume.
- SDOH2Health achieved a 67% reduction in ER visits among a targeted cohort.
B. Simple ROI example
If you enroll 1,000 high-risk members and replicate the $68.80 savings:
1,000 × $68.80 × 12 = $825,600 annual avoided spend.
C. Why automation is the force multiplier?
Manual SDOH programs stall under volume. Automated screening and triage ensure interventions are consistent and measurable.
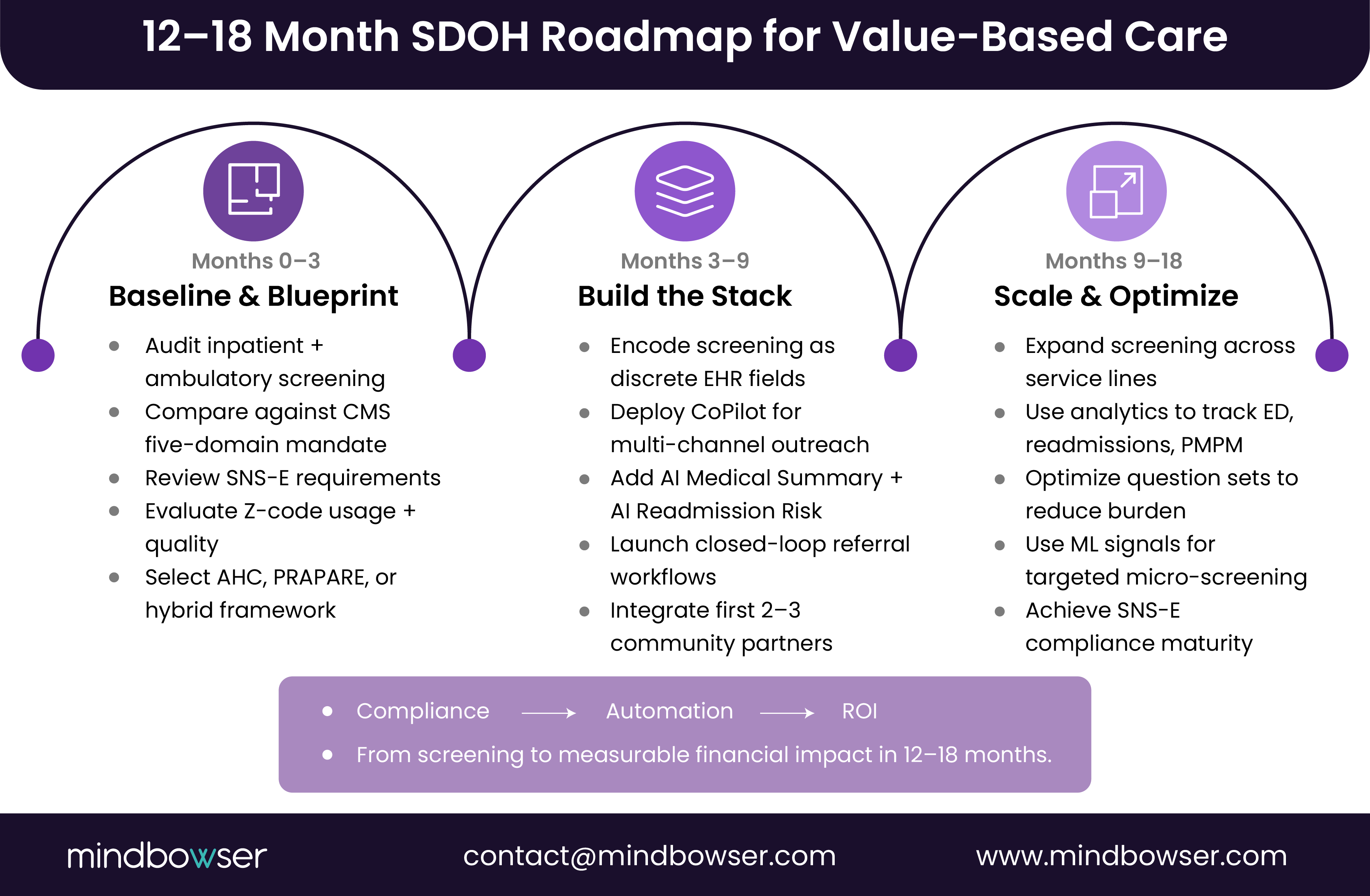
VI. A practical 12–18 month roadmap
A. Months 0–3: Blueprint
- Audit current screening.
- Map to the CMS five-domain rule and SNS-E.
- Select framework.
- Review Z-code quality.
B. Months 3–9: Build
- Encode fields in EHR/CRM.
- Deploy multi-channel screening via HealthConnect CoPilot.
- Add AI Medical Summary and AI Readmission Risk.
- Launch referral workflows.
C. Months 9–18: Scale
- Extend to all inpatient adults.
- Integrate analytics from VBC dashboards.
- Optimize question sets using ML signals.
SDOH is now a Value-based care performance system, not a survey project
The last two years made one fact clear: SDOH has moved from an innovation experiment to a contractual obligation. CMS now requires five-domain inpatient screening, NCQA scores both screening and intervention, and payers are tying real dollars to social-risk documentation and mitigation. The organizations that will lead in 2025–2027 are those that treat SDOH as a data and workflow system, not a form, and build AI-ready, closed-loop infrastructure that reliably reduces avoidable ED visits, lowers readmissions, and improves Stars outcomes.
If your current SDOH process is fragmented, manual, or unmanaged, you are not alone. But the path forward is clear: adopt a validated framework, codify it in your EHR, automate outreach and triage, and measure impact like any other VBC lever. Systems that do this are already showing PMPM savings and real reductions in utilization.
The question now is not whether SDOH matters it is whether your organization can operationalize it fast enough to keep pace with new mandates and contract demands. If you want support building an AI-ready SDOH roadmap, our team can help map your screening, data, and intervention workflows from end to end.
SDOH are broad social conditions; HRSN are actionable individual risks. CMS uses HRSN in the AHC tool and links them to Z-codes.
Most hospitals use CMS AHC, PRAPARE, or a hybrid. Fit to contracts, EHR, and population matters more than brand.
NCQA’s SNS-E measures scores, screening, and interventions. Z-codes and G-codes will play an increasingly important role in measure submission.
AI identifies high-need patients, summarizes charts, and routes interventions. ML models outperform survey-only methods for HRSN prediction.
Yes. Ballad Health achieved a 16.2 percent reduction in ED volume and $68.80 in PMPM savings. SDOH2Health saw a 67% decline in ER visits among a targeted cohort.


