



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
- Cellular devices ($80-150/unit, no phone required) produce the highest patient compliance for 65+ populations. Bluetooth devices ($30-70/unit, widest selection) work best for younger patients who are proficient with smartphones.
- Hub-based gateways connect BLE devices via a single cellular relay for multi-device elderly programs. Cloud API pulls (Dexcom, Withings) cost nothing in device procurement when patients already own the hardware.
- At 500 patients over 65, cellular typically generates approximately $150K typical more annual revenue than Bluetooth, with a modeled range of $94K to $253K, despite costing $20K more in devices, because more patients hit the compliance threshold for CMS billing.
- The per-device price is not the cost that matters. The total cost of ownership, including support burden and lost billing, is.
The first architecture question every CTO asks us when scoping an RPM platform is the same: cellular or Bluetooth?
The answer we give has changed over the past three years. We started by defaulting to Bluetooth. The device selection was wider, the per-unit cost was lower, and every vendor demo looked clean. Then we tracked support costs and compliance rates across six deployed programs, and the data told a different story.
A CTO at a 400-bed system chose BLE to save $50 per device on 500 units. Twenty-five thousand dollars in savings. The BLE pairing support calls cost $38,000 in the first year. The compliance rate for patients over 65 was 58%, meaning 42% of those patients generated zero billable RPM events because their readings never consistently reached the platform. The program switched to cellular for the 65+ cohort in month eight, and compliance jumped to 87% within 60 days.
That story is not unusual. It is the default outcome when BLE devices are deployed to populations they were not designed for.
Why Does the Connectivity Decision Come First?
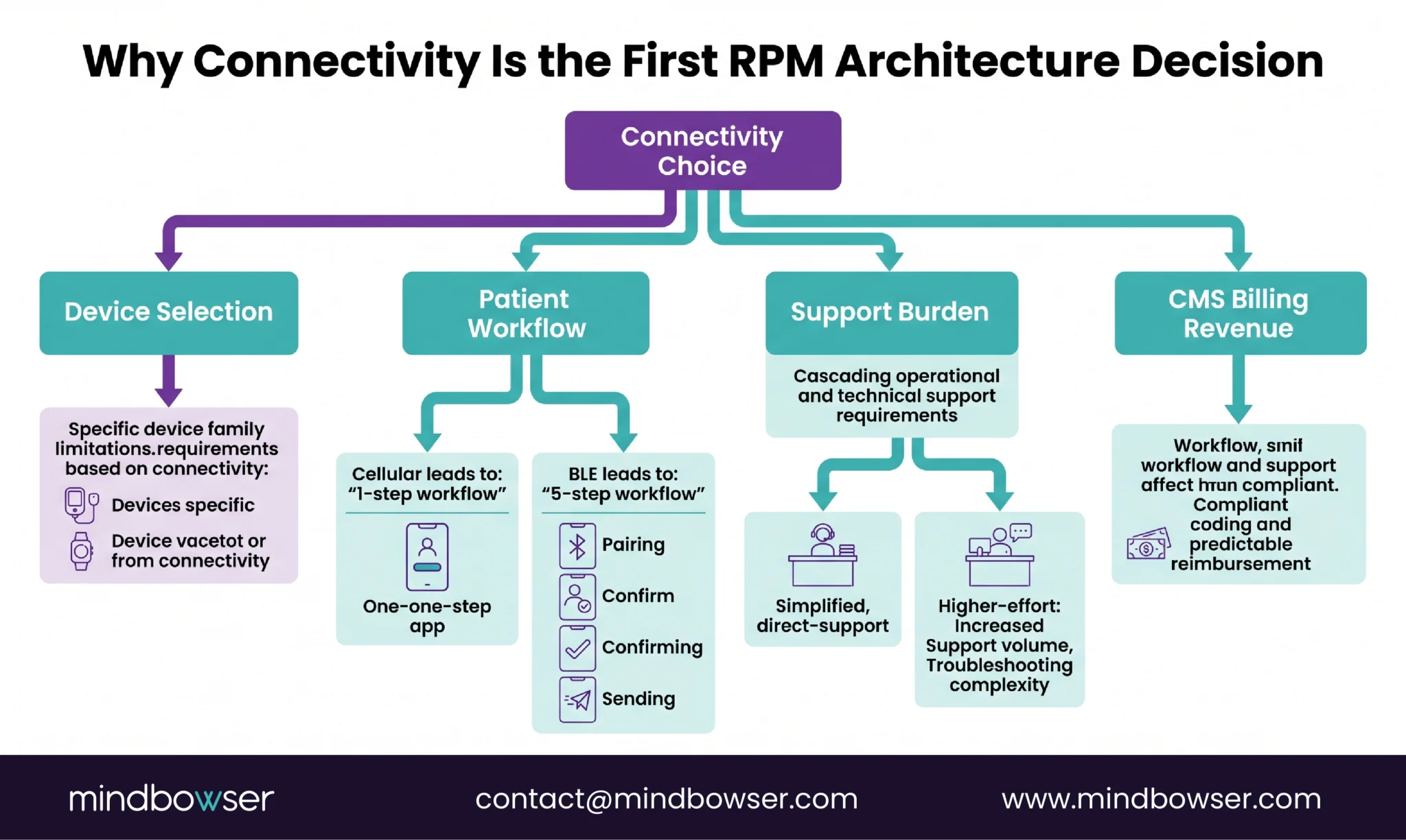
Because it cascades into every other program decision.
- Device selection. Choosing cellular limits you to roughly 40-50 device models across all vital sign categories. Choosing BLE opens 200+. If the specific device your clinical team wants only comes in BLE, that constrains the connectivity decision.
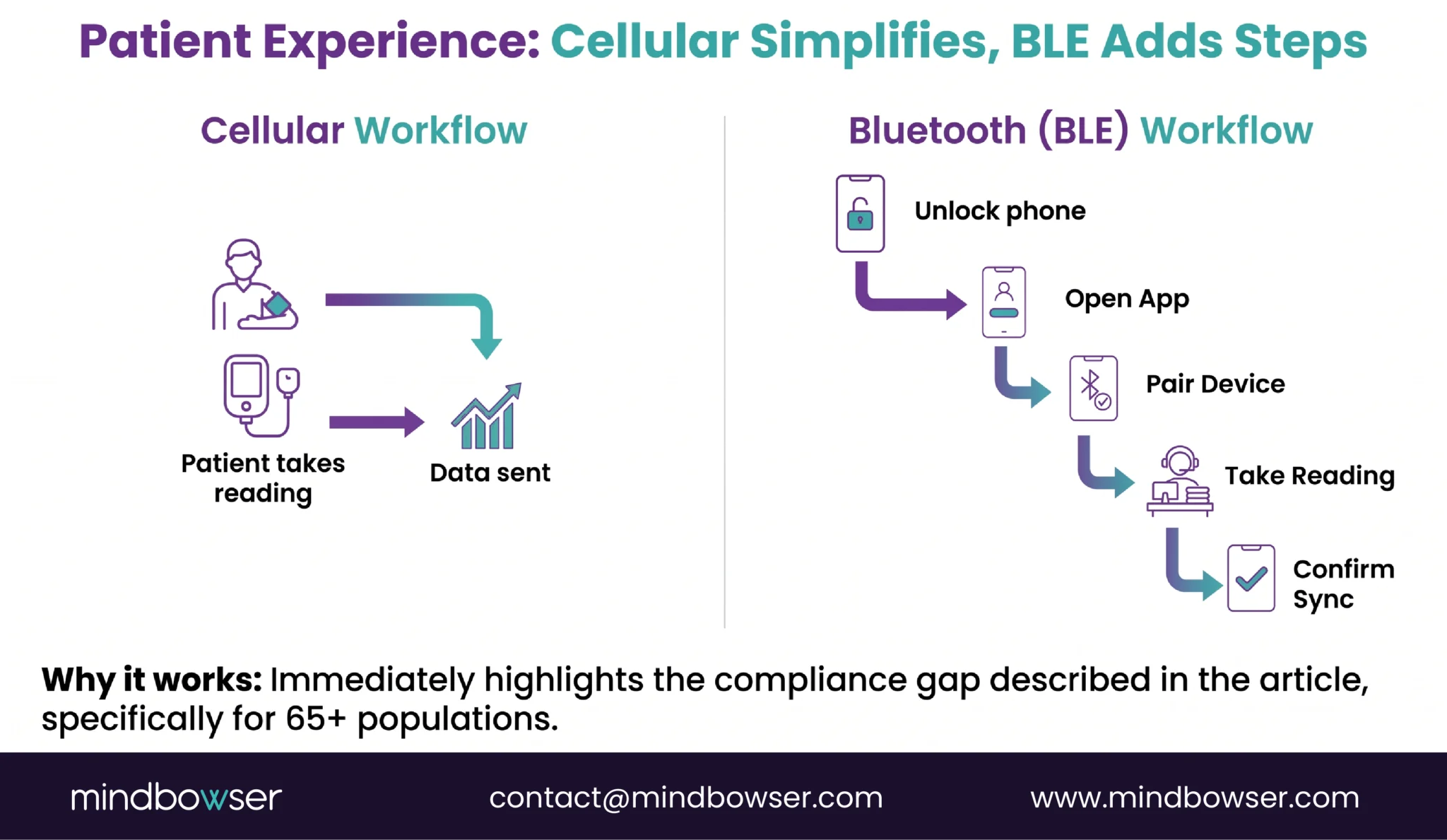
- Patient workflow. Cellular: patient presses button, done. BLE: patient unlocks phone, opens app, waits for pairing, takes reading, confirms sync. Five steps versus one. For patients with cognitive decline, arthritis, or low tech literacy, those four extra steps are the difference between compliance and abandonment.
- Support burden. BLE pairing failure is the #1 support ticket in RPM programs. We have tracked this across every deployment. Typical elderly patient: 2-3 support calls in month one for pairing issues. At $15-25 per call (staff time), that is $30-75 per patient in support cost that never appears on the device spec sheet.
- CMS billing. Revenue depends on data reaching the practitioner’s monitoring system. If readings don’t transmit because the patient couldn’t pair the device, those readings don’t exist for billing purposes. A patient who monitors 20 days but only syncs 11 days of data is billed for zero under the standard 99454 code. Connectivity reliability directly scales revenue.
Cellular: No Phone, Maximum Compliance
Cellular RPM devices have an embedded SIM that transmits readings directly over the carrier network. The patient presses one button. The reading appears on the care team’s dashboard. No smartphone. No app. No Bluetooth pairing. No WiFi password.
Available devices: Tenovi offers seven FDA-cleared cellular-connected RPM devices (BP cuff, scale, pulse oximeter, glucose meter, thermometer, peak flow meter, and a cellular gateway). BodyTrace makes cellular scales and BP cuffs. Omron has cellular-connected models in its clinical line. The device selection is narrower than BLE but covers the core vital sign categories.
Patient experience: one-button operation is not a marketing phrase. We have watched elderly patients use cellular BP cuffs for the first time with zero training. The cuff inflates, measures, deflates, and transmits. The patient sees a number on the small screen. That is the entire interaction. No confirmation needed. No sync status to check.
Compliance data: Tenovi reports a 27% increase in patients eligible for 99454 reimbursement compared to leading BLE devices, specifically because automatic cellular transmission eliminates the sync-failure gap (Tenovi, 2025). Our own data across three programs serving 65+ patients shows compliance rates of 85-95% with cellular versus 55-70% with BLE for the same patient demographics.
Cost: $80-150 per unit, depending on device type. Higher than BLE by $50-80 per device. The embedded SIM includes carrier data for the device’s lifetime in most models (no monthly cellular fee per device for Tenovi and BodyTrace).
Limitations: smaller device selection than BLE, cellular coverage gaps in deep rural areas (rare but real, roughly 0.3% of US population), battery life is 6-18 months for non-rechargeable models, no patient-facing app or data visualization (the patient sees the reading on the device screen only, not trends or history).
Bluetooth (BLE): Lowest Per-Unit Cost, Widest Selection
BLE devices pair with the patient’s smartphone via Bluetooth Low Energy. The phone app receives the reading and transmits it to the RPM platform through the patient’s internet connection (WiFi or cellular data).
- Available devices: hundreds. Every major medical device manufacturer produces BLE-connected models: Omron (BP, ECG), Nonin (pulse oximeter), iHealth (BP, glucose, SpO2), Withings (BP, scale), AliveCor (ECG), plus consumer wearables (Apple Watch, Fitbit, Garmin, Oura). BLE is the default connectivity for the widest device selection.
- Patient experience: requires a compatible smartphone (iOS or Android, specific version requirements vary by device app), app installation from the app store, initial BLE pairing (finding the device in Bluetooth settings, confirming the pairing code), and the phone remaining within 30 feet of the device during measurement. For a 35-year-old with a current iPhone, this is trivial. For a 78-year-old with a 4-year-old Android phone, each step is a potential failure point.
- Cost: $30-70 per unit. The lowest per-device cost in RPM.
- The support reality: BLE pairing is the #1 support ticket in every RPM program we have operated or consulted on. The failure modes are numerous and unpredictable: phone Bluetooth turned off, phone connected to a different BLE device (hearing aids are the most common conflict), app killed by the phone’s battery saver, app update requiring re-pairing, phone OS update breaking BLE compatibility, patient out of Bluetooth range during measurement. Each failure results in a support call. Our data: 2-3 calls per elderly patient in month one, declining to 0.5-1 per month by month six. At $15-25 per call, the year-one support cost for 500 elderly patients is approximately $22,500.
- Where BLE wins: programs that have a patient-facing mobile app (the app is already built, adding BLE device pairing is incremental), younger patient populations (30-55) with current smartphones, multi-device monitoring where the phone serves as the data aggregator for 3+ BLE devices (BP cuff + glucose meter + scale all pairing to one phone), and programs where the specific clinical device only comes in BLE (some spirometers, the Strados RESP Biosensor, AliveCor KardiaMobile).
Evaluate the Right Connectivity Mix for Your Patient Population and Program Scale
Hub-Based Gateway: The Bridge Between BLE Cost and Cellular Reliability
A cellular gateway sits in the patient’s home, plugged into a power outlet. BLE devices pair to the gateway instead of a phone. The gateway aggregates readings from multiple devices and transmits them over the cellular network.
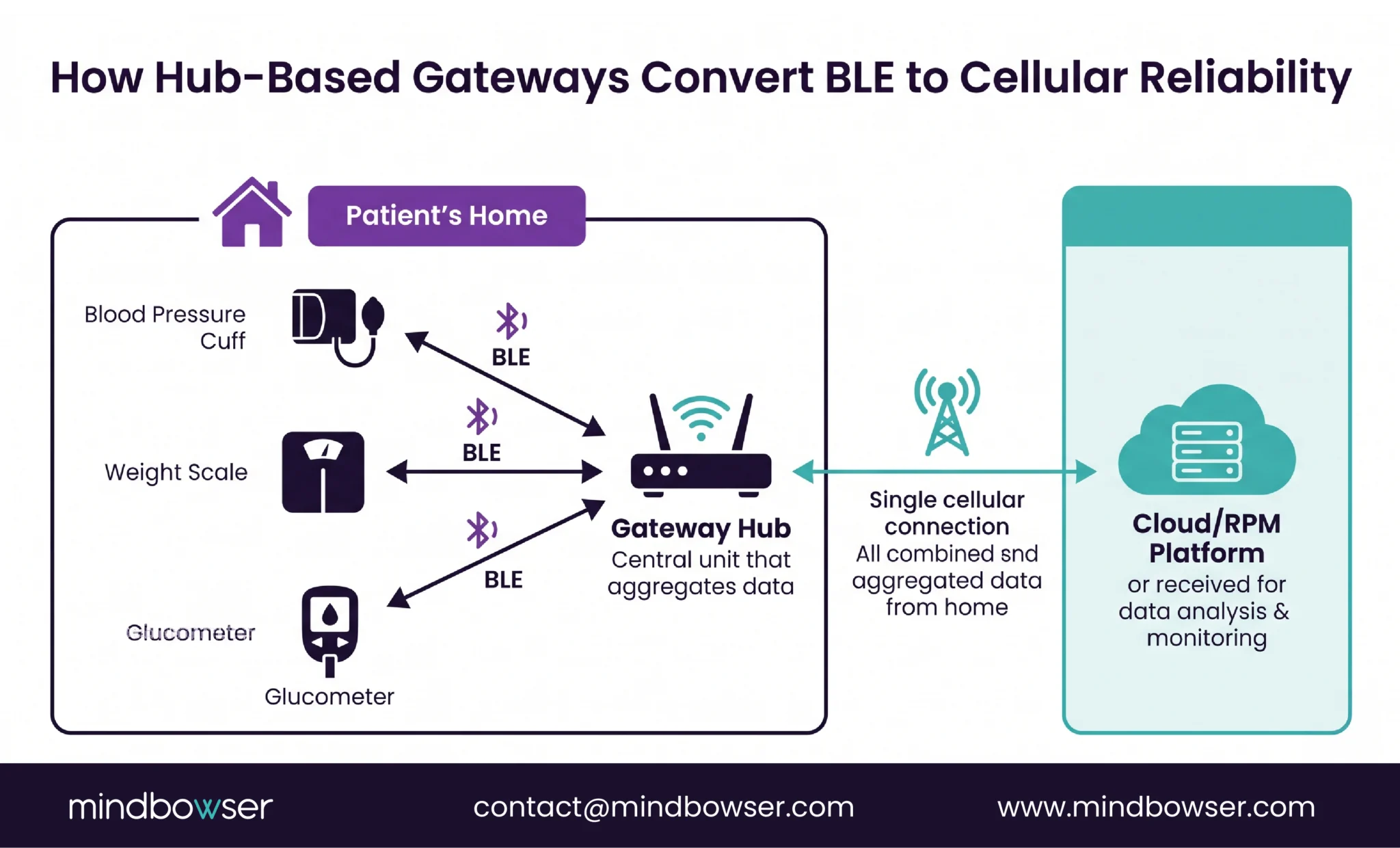
The Tenovi cellular gateway connects multiple BLE devices through one hub. The patient still uses BLE devices (lower per-unit cost), but the gateway eliminates smartphone dependency. The pairing happens once during setup (by the care team or during an in-home visit), and the gateway maintains the connection persistently.
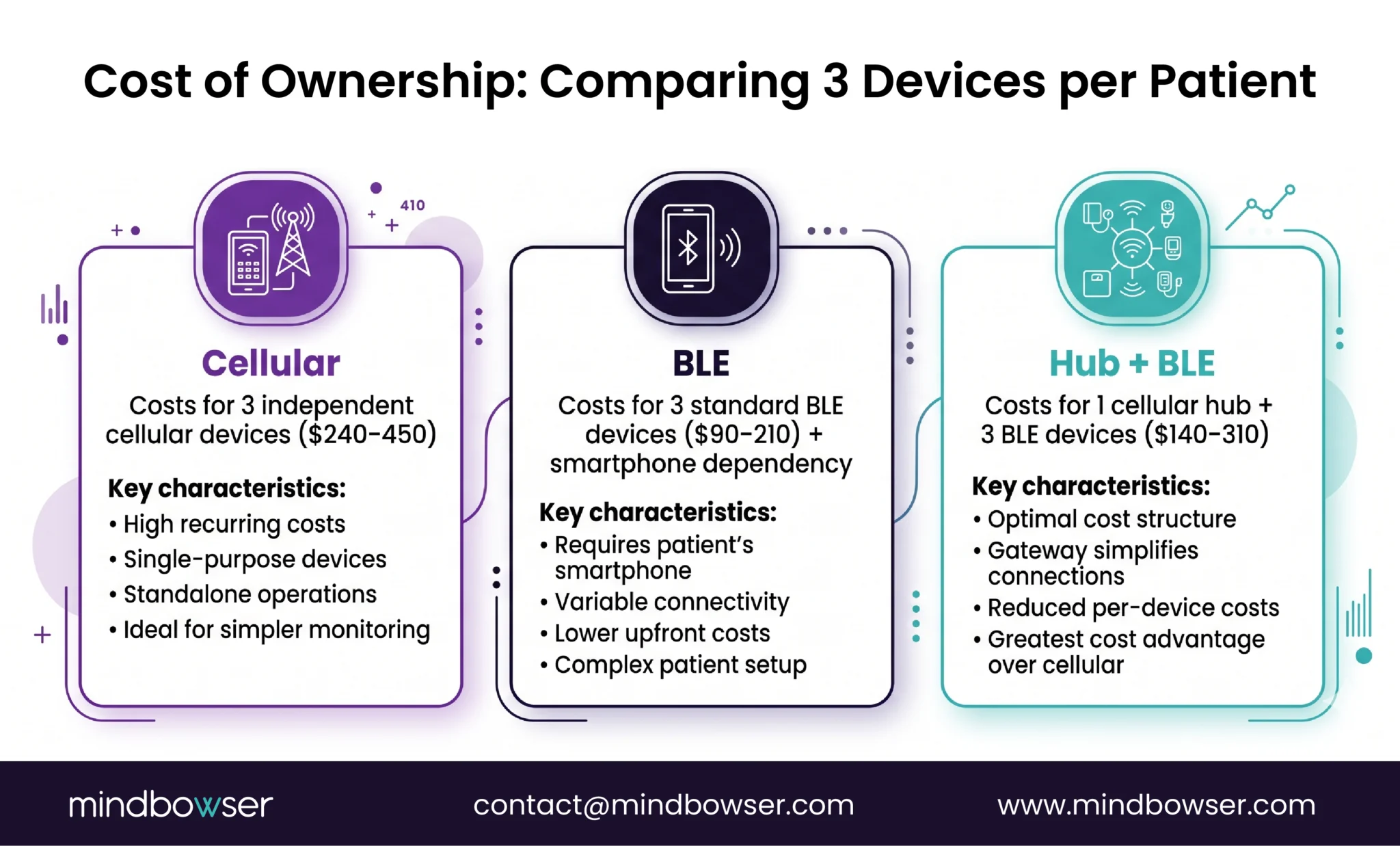
Best for: multi-device elderly programs. A heart failure patient needing a BLE scale, BLE BP cuff, and BLE pulse oximeter would require three separate cellular devices ($240-450) or one gateway ($50-100) plus three BLE devices ($90-210). The gateway model saves $100-250 per patient in device cost while maintaining cellular-level reliability.
Trade-offs: adds hardware to the patient’s home (gateway needs a power outlet and a location within BLE range of where the patient takes readings), requires initial setup (care team configures the gateway and pairs all devices before delivery or during a home visit), gateway failure is a single point of failure for all devices (if the gateway loses power or cellular signal, all device data stops flowing).
The declining relevance: as standalone cellular device prices drop and cellular device selection widens, the gateway model loses its primary cost advantage. A cellular BP cuff that cost $150 three years ago costs $80-100 today. If standalone cellular devices continue this trajectory, gateways become unnecessary for single-device programs. For multi-device programs (3+ devices per patient), gateways remain cost-effective through 2026-2027.
Cloud API: When the Patient Already Has the Device
Cloud API connectivity applies when the patient already owns the device and the data is already flowing to the manufacturer’s cloud. The RPM platform pulls data through the manufacturer’s API instead of integrating with the device directly.
- Common cloud API sources: Dexcom (CGM data via developer API), Abbott (glucose via LibreView), Withings (BP, scale, sleep via Health Mate API), Apple HealthKit (aggregated data from Apple Watch and paired devices), Google Health Connect (Android equivalent), Fitbit/Google (activity, HR, sleep).
- Zero device procurement cost. The patient already bought the device. The RPM program adds monitoring and billing on top of existing device ownership. For diabetes programs where patients are already on Dexcom G7, this eliminates the entire device procurement line from the budget.
- Trade-offs: API latency (readings arrive 5-30 minutes after measurement, not real-time), API rate limits (pulling data for 1,000 patients requires careful request management), dependency on manufacturer uptime (if Dexcom’s cloud has an outage, your RPM data stops), and data completeness (manufacturers may not expose all raw sensor data through their API).
- Best for: diabetes RPM (CGM data already in Dexcom/Abbott cloud), wellness and preventive monitoring (patients with Apple Watch or Fitbit), programs that want to layer RPM billing onto existing consumer device adoption without shipping any hardware.
For a detailed CGM API integration architecture, see our diabetes remote patient monitoring guide.
Cost Comparison at Scale: Total Cost of Ownership
Per-device cost is the metric every vendor leads with. Total cost of ownership, including support burden and billing impact, is the metric that actually determines program economics.
| Factor | Cellular | BLE | Hub + BLE | Cloud API |
|---|---|---|---|---|
| Device cost per unit | $80-150 | $30-70 | $30-70 + $75 hub | $0 |
| 500 patients device cost | $40-75K | $15-35K | $52-110K | $0 |
| Year 1 support cost (500 pts) | ~$2,500 | ~$22,500 | ~$5,000 | ~$3,000 |
| Total year 1 hardware + support | $42-78K | $37-58K | $57-115K | $3K |
| Compliance rate (65+ population) | 85-95% | 55-70% | 80-90% | 70-80% |
| Billable patients (65+, 500 enrolled) | 425-475 | 275-350 | 400-450 | 350-400 |
| Annual RPM revenue (billable pts × $105/mo × 12) | $535-599K | $346-441K | $504-567K | $441-504K |
| Revenue gap vs cellular | — | -$94 to -$253K | -$32 to -$95K | -$95 to -$158K |
The line that changes the conversation: BLE appears cheapest in device cost ($15-35K vs $40-75K). But BLE generates $94K to $253K less annual revenue than cellular for a 500-patient 65+ program because fewer patients hit the compliance threshold for billing.
The $50 per-device savings cost the program $188 to $506 per patient in lost annual revenue.
For younger populations (30-55) where BLE compliance rates match cellular (85%+), the cost comparison favors BLE because the support burden is lower and the compliance gap disappears. The population drives the choice, not the price tag.

Decision Framework: Which Connectivity for Which Program?
Choose cellular when:
- The majority of patients are 65+
- No patient-facing mobile app in the program design
- Data reliability is non-negotiable (cardiac programs, hospital-at-home)
- Single device per condition (one BP cuff, one scale, one pulse ox)
- The program needs the highest possible CMS billing compliance rate
Choose BLE when:
- The patient population is primarily 30-55 with current smartphones
- The program includes a patient-facing mobile app for engagement and education
- Multi-device monitoring where the phone aggregates data from 3+ devices
- The specific clinical device required only comes in BLE
- Per-device budget is the binding constraint (not the total cost of ownership)
Choose hub-based gateway when:
- Elderly patients needing 3+ devices each (gateway cost < 3 cellular devices)
- Patients have reliable home power (for the gateway)
- Program prefers BLE device selection with cellular-level reliability
Choose cloud API when:
- Patients already own and use CGM (Dexcom, Abbott) or consumer wearable (Apple Watch, Fitbit)
- Goal is to layer RPM billing on existing device adoption
- Zero device procurement budget
- Acceptable data latency (5-30 minutes)
Hybrid (the most common model at scale):
Most programs over 200 patients end up hybrid: cellular BP cuffs for elderly hypertension patients, cloud API for diabetic patients already on CGM, BLE wearables for younger multi-condition patients. The RPM platform supports all four connectivity types. Patient segment determines which connectivity each patient uses. This is the architecture ConnectHealth is built for: normalizing data from cellular, BLE, hub, and API sources into a unified patient view.
The Spec Sheet Won’t Tell You This
Device spec sheets compare Bluetooth version, battery life, FDA clearance status, and measurement accuracy. They do not compare support call volume per patient, compliance rates by age group, total cost of ownership including lost billing, or the number of patients who stop using the device in month two because they couldn’t pair it.
The connectivity decision is a business decision disguised as a technology decision. The right choice depends on who your patients are, how many support calls your team can absorb, and whether you are optimizing for per-device cost or total program value.
Early in our RPM work, we defaulted to BLE for everything. The device selection was wider and the per-unit cost was lower. After tracking support costs and compliance rates across six programs serving a combined 2,300 patients, we default to cellular for any program where the majority of patients are over 60. The total cost is lower and the revenue is higher. For programs targeting younger, tech-comfortable populations, BLE remains the right choice. And for multi-condition programs at scale, hybrid (cellular + BLE + cloud API, matched to patient segments) is where most mature programs land. The logistics of managing a hybrid fleet at scale, device inventory, patient segmentation, and return workflows are covered in our RPM scaling guide.
Cellular RPM devices have an embedded SIM and transmit readings directly over the carrier network. No smartphone, app, or Bluetooth pairing required. One-button operation. Cost: $80-150 per unit. Bluetooth (BLE) devices pair with the patient’s smartphone, which transmits data through an app. Wider device selection. Cost: $30-70 per unit. The key difference in practice: cellular achieves 85-95% compliance in 65+ populations versus 55-70% for BLE because cellular eliminates the pairing, app, and phone dependency that cause elderly patient disengagement.
Cellular has the highest compliance for patients over 65 (85-95%), followed by hub-based gateways (80-90%), cloud API (70-80%), and BLE (55-70%) for the same age group. For patients 30-55, BLE compliance rises to 80-90%, closing the gap with cellular. Compliance is measured as the percentage of patients transmitting device data for at least 16 days per 30-day billing period (the threshold for CPT 99454 reimbursement). Tenovi reports a 27% increase in 99454-eligible patients with cellular versus BLE.
Per unit, yes: cellular costs $80-150 versus $30-70 for BLE. But total cost of ownership (device + support + lost revenue) often favors cellular for elderly programs. BLE pairing support calls cost approximately $22,500 per year for 500 elderly patients. Cellular support costs approximately $2,500 for the same panel. And cellular generates $94K-$253K more annual billing revenue because more patients hit compliance thresholds. The $50 per-device savings on BLE costs $188-$506 per patient in lost annual revenue for 65+ programs.
A hub-based gateway is a cellular-connected device that sits in the patient’s home and relays data from multiple BLE devices to the RPM platform. BLE devices pair to the gateway instead of a phone, combining BLE device cost ($30-70 per device) with cellular reliability (no smartphone needed). One gateway ($50-100) can connect 3-5 BLE devices. Best for elderly patients needing multiple devices where buying 3 separate cellular devices would cost more than one gateway plus 3 BLE devices.
Yes, and most programs over 200 patients do. The typical hybrid model: cellular BP cuffs for elderly hypertension patients (highest compliance), cloud API for diabetes patients already on CGM (zero device cost), and BLE wearables for younger multi-condition patients (widest device selection). The RPM platform must support all connectivity types and normalize the data into a unified patient view regardless of how it arrived. This multi-connectivity architecture is what WearConnect is designed to handle.
Cellular. The evidence is consistent across our deployments and published data. Cellular eliminates the three biggest barriers for elderly RPM patients: smartphone dependency, Bluetooth pairing, and app management. One-button operation with automatic data transmission achieves 85-95% compliance in 65+ populations. For elderly patients needing multiple devices, a hub-based cellular gateway with BLE devices is the cost-effective alternative. BLE direct-to-phone should be reserved for elderly patients who have demonstrated smartphone proficiency and have reliable phone support (family member managing the app).


