



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
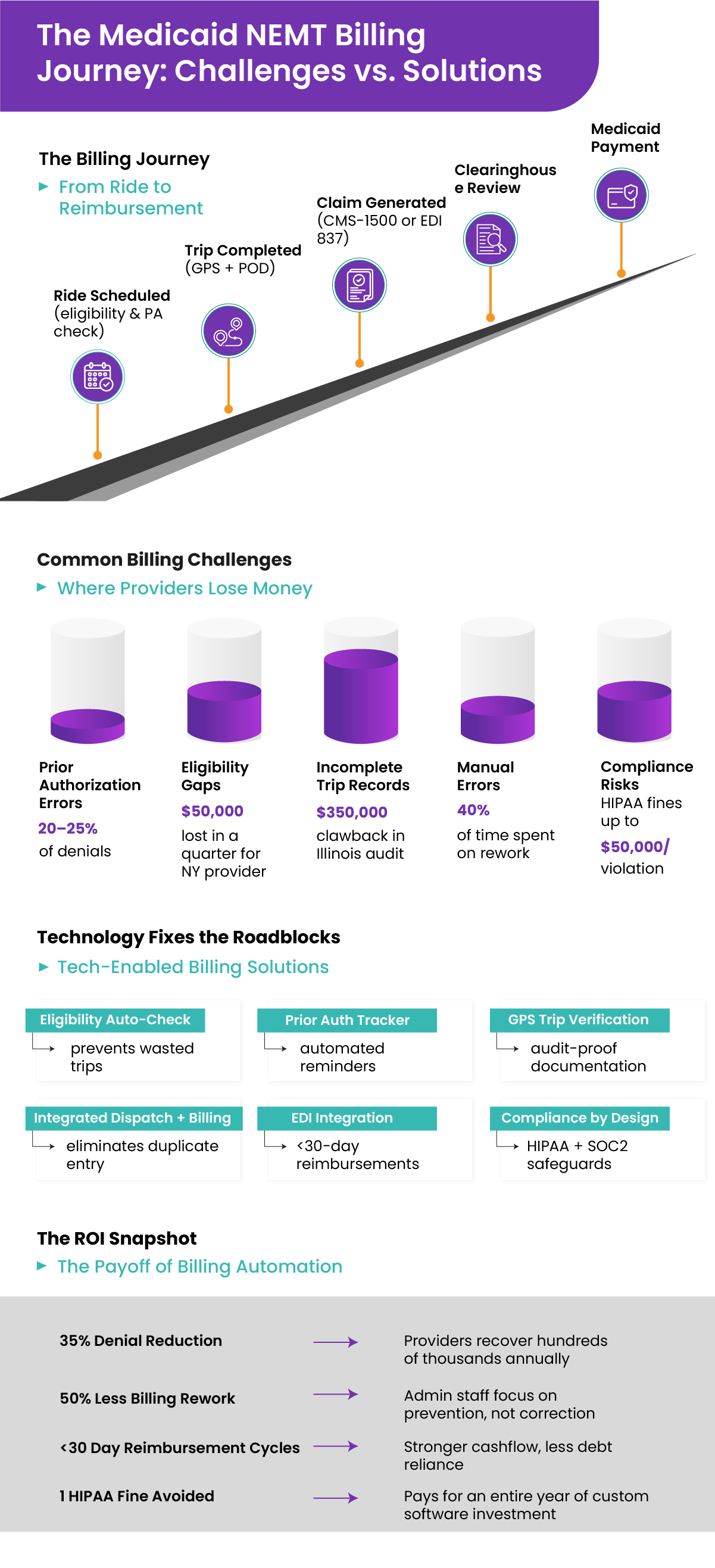
Medicaid promises patients a ride to care, but for providers, those rides don’t always get paid. With 10–20% of NEMT claims being denied on first submission, operators face cash flow crunches, and patients face disruptions in care. Billing isn’t back-office housekeeping. It’s the financial engine of every transportation program. If it fails, the whole system feels the impact.
If these costs sound familiar, you’re not alone!
it’s a systemic challenge across NEMT. The good news? Modern technology can stop the leaks before they drain your business. See how Mindbowser helps providers recover revenue and rebuild trust.
III. Common Medicaid NEMT Billing Challenges
If Medicaid billing were straightforward, providers wouldn’t lose thousands of dollars each month due to preventable denials. The reality is that billing workflows are fragile, highly regulated, and prone to errors at multiple touchpoints. Below are the most persistent challenges NEMT operators face.
A. Prior Authorization Issues
- Missed Requests
Providers sometimes transport a patient before authorization is fully approved. Even if the trip was medically necessary, Medicaid will automatically deny reimbursement. - Incorrect Details
When authorization data doesn’t match the billed HCPCS code, mileage, or service type, the claim is flagged for rejection. - Shifting State Rules
Some states require prior authorization for every trip. Others allow recurring approvals for treatments like dialysis. Still others rely on broker-mediated workflows.
Case in Point: A Midwest operator saw denial rates spike to 17% when a dialysis patient’s standing prior authorization expired mid-month. Without an automated tracker, dispatchers continued to schedule rides, unaware that the PA window had closed. Every one of those trips was later denied. Revenue was unrecoverable.
Bottom line: Without airtight authorization tracking, providers risk denials they cannot appeal.
B. Eligibility Verification Gaps
- Lapsed Coverage
Medicaid coverage changes monthly. Manual checks often miss patients who lose eligibility during the cycle. - Broker vs. State Mismatches
Brokers may show a patient as eligible while the state Medicaid system lags in updates. Providers get caught in the middle. - Batch Processing Delays
Some providers rely on nightly eligibility checks. That creates a gap during the day when ineligible rides may still be dispatched.
Case Insight: A New York provider lost $50,000 in a single quarter when batch verification failed to flag 200 ineligible rides. Every claim was denied outright.
Bottom line: Eligibility must be verified in real time, not overnight.
C. Incomplete Trip Records
Medicaid requires proof that the ride occurred exactly as billed. Missing even one detail can trigger denials or even fraud investigations.
- Required data fields include:
- Pickup and drop-off timestamps
- Driver and vehicle ID
- Odometer readings and mileage
- Proof of Delivery (electronic signature, PIN, or GPS verification)
- If documentation is missing, Medicaid may reject the claim. In audits, incomplete records can even result in the repayment of funds already received.
Audit Example: In Illinois, a provider faced $350,000 in clawbacks when auditors found 1,200 trips lacked GPS-stamped proof of delivery. The rides happened, but without compliant documentation, Medicaid demanded repayment.
Bottom line: Documentation gaps turn completed rides into financial liabilities.
D. Manual Data Entry Errors
Billing teams still manually enter trip data, which creates endless opportunities for errors.
- Common errors:
- Duplicate claim submissions
- Incorrect HCPCS or mileage codes
- Mismatched patient IDs
- Typographical errors in dates of service
- Because Medicaid systems are rigid, even tiny mistakes cause denials. Each error delays payment by 30 to 90 days.
Bottom line: Manual data entry is too brittle for high-volume, compliance-heavy billing.
E. Late Submissions
Every state enforces strict timelines for claim submission—often 90 or 180 days. If the deadline is missed, the claim is permanently non-payable.
- Providers relying on paper logs or manual workflows are at the highest risk.
- Multi-state operators juggling different timelines multiply that risk.
Bottom line: Late submissions equal guaranteed revenue loss.
F. Compliance Risks (HIPAA & CMS)
Billing systems must comply with HIPAA, CMS, and state regulations. Risks arise when:
- PHI is sent through unsecured email or stored in spreadsheets.
- Systems lack encryption at rest or in transit.
- No audit trail exists for staff access to PHI.
Fines can reach $50,000 per violation. Repeat offenses can jeopardize a provider’s Medicaid contract.
Bottom line: Billing errors don’t just cost money. They can put the entire business relationship at risk.
G. Fraud Flags and False Positives
Even legitimate claims are sometimes flagged as fraudulent if documentation trails are weak.
- Red flags include:
- Multiple rides for the same patient on the same day without matching prior authorization
- Mileage discrepancies (billing 25 miles for a 12-mile trip)
- Lack of verifiable proof of service
- Providers without strong trip verification often face unnecessary denials or lengthy audits.
Real-World Insight: A behavioral health transport provider in Florida had 10% of claims frozen during a fraud investigation because logs lacked GPS validation. Rides were real, but missing proof caused months of delayed reimbursement.
Bottom line: Weak documentation creates unnecessary exposure to fraud audits.
The Bigger Picture
Every denial is more than an inconvenience. It’s lost revenue, wasted staff time, and erosion of payer trust. Studies show that up to 40% of NEMT billing staff hours are spent reworking denied claims. The problem isn’t a a lack of effort—it’s outdated, manual processes that can’t keep pace with the complexity of Medicaid.
IV. The Real Cost of Billing Problems
Billing errors in Medicaid NEMT don’t exist in a vacuum. They ripple across operations, finances, compliance, and even patient care. While individual denials may seem minor, their cumulative impact can destabilize entire transportation programs.
A. Cashflow Crunch
For most NEMT operators, Medicaid is the primary source of revenue. When 10–20% of claims are denied or delayed, cash flow becomes unpredictable.
- Delayed Reimbursements – Denials typically extend payment cycles by 30–90 days as staff resubmit and wait for adjudication.
- Payroll Stress – Providers often struggle to cover driver wages, fuel, and maintenance while waiting on reimbursements.
- Credit Dependency – Some mid-sized operators resort to lines of credit or factoring services to cover shortfalls, which eats into margins.
Case Example: A 40-vehicle fleet in Texas reported that reimbursement delays forced them to use a $250,000 credit line just to cover fuel bills. The interest expense alone costs them $25,000 annually — money that could have been invested in expansion or compliance upgrades.
B. Revenue Loss (Denials = Unrecoverable Income)
Not all denied claims can be salvaged. Many Medicaid denials — especially those tied to missed prior authorization or late submissions — are non-appealable.
- Providers may write off 5–10% of total billed revenue annually due to denials that cannot be corrected.
- At an average reimbursement of $65 per trip, even losing 500 trips a month equals nearly $390,000 in unrecoverable income annually.
Data Point: CMS estimates that 10–20% of Medicaid claims are denied on first submission. Even if half are recovered through resubmissions, the remaining losses are significant.
C. Administrative Overload
Behind every denial is a mountain of paperwork. Billing teams spend excessive hours on rework, slowing down other functions.
- Resubmission Cycles – Each denial requires claim correction, re-verification, and resubmission of the claim.
- Staff Burnout – Billing staff often spend 30–40% of their time fixing errors, leaving little bandwidth for proactive compliance or analytics.
- Hidden Labor Costs – What appears to be “back-office work” often equates to tens of thousands of dollars in wasted salary hours annually.
Scenario: A behavioral health transport service employing four full-time billing clerks discovered that three of them spent most of their week resolving denials. According to their own calculations, $120,000/year in labor costs was allocated to rework alone.
D. Compliance Fines & Contract Risk
Billing errors don’t just cost money — they can trigger compliance investigations. Medicaid and CMS program integrity units actively monitor claims for irregularities.
- HIPAA Violations – If PHI is mishandled (e.g., transmitted insecurely via email or stored on non-encrypted systems), fines can reach $50,000 per violation.
- State Medicaid Audits – Missing trip verification logs or incomplete audit trails can lead to clawbacks of previously paid claims.
- Contract Jeopardy – Repeated compliance failures erode trust with state agencies and brokers, risking loss of future contracts.
Revenue.
The Larger Picture
Billing problems in Medicaid NEMT are not merely clerical errors; they are often indicative of more significant issues. They represent a systemic risk to financial stability, compliance integrity, and patient access to care. For providers operating on tight margins, even modest denial rates can mean the difference between growth and closure.
Audit Example: An Illinois operator was forced to repay $350,000 after a Medicaid audit found gaps in GPS trip verification. The rides had occurred, but without compliant proof, the payments were clawed back.
E. Reputation Damage
In Medicaid NEMT, trust is currency. Hospitals, brokers, and state agencies must believe that providers deliver reliable and compliant services. Billing errors undermine that trust.
- Hospitals may hesitate to refer patients if billing issues disrupt the continuity of transport.
- Brokers may shift contracts to more reliable providers.
- Patients lose confidence when providers cut back services due to financial stress.
Industry Insight: One regional fleet in the Midwest lost its contract with a major Medicaid broker after repeated claim delays flagged them as “high-risk.” Despite strong on-time performance, their billing inefficiency cost them the relationship — and millions in annual revenue.
V. How Technology Solves Medicaid Billing Challenges
Manual billing and outdated systems leave providers vulnerable to denials, cash flow delays, and compliance risks. Purpose-built technology flips the equation. Instead of reacting to denials after they occur, providers can prevent errors upfront, streamline workflows, and protect revenue. Here’s how.
A. Eligibility Auto-Check (Real-Time Verification)
- The Problem
Medicaid eligibility changes monthly, sometimes mid-cycle. Manual checks often miss these shifts, resulting in claims being filed for patients who are no longer eligible for coverage. - The Solution
Automated eligibility checks validate coverage before a trip is dispatched. Integrations with Medicaid APIs (X12 270/271 transactions) confirm in real time whether the patient is eligible on the exact date of service. - The Outcome
If the patient isn’t eligible, the system blocks the trip before it happens, saving providers from unreimbursable rides.
Case Example: A New York provider cut denial rates from 18 percent to under 5 percent within 90 days by implementing pre-trip eligibility verification.
Bottom line: Real-time eligibility checks prevent wasted trips and protect cash flow.
B. Prior Authorization Tracker
- The Problem
Expired or mismatched authorizations remain one of the top causes of automatic claim denials. - The Solution
Software tracks prior authorization windows, required documentation, and state-specific rules. Automated alerts notify dispatchers when an authorization is about to expire, preventing unsanctioned trips. Authorization records are attached directly to the claim file, creating a complete audit trail. - The Outcome
Operators drastically reduce unrecoverable denials tied to missing or expired PAs.
Scenario: A Midwest dialysis transport operator reduced PA-related denials by 70 percent after adopting automated reminders integrated with dispatch.
Bottom line: Automated PA management closes one of the largest gaps in Medicaid billing denial.
C. Trip Verification and Proof of Delivery
- The Problem
Missing or incomplete trip records—such as absent GPS stamps or unsigned proof of delivery—lead to denials or clawbacks during audits. - The Solution
GPS-based trip tracking automatically records pickup and drop-off coordinates, while digital proof of delivery (e-signatures, PINs, or photo verification) is tied directly to billing records. Immutable audit logs ensure every mile is defensible. - The Outcome
Audits become routine instead of high-stakes battles.
Audit Example: An Illinois provider avoided $200,000 in clawbacks after switching to GPS trip verification and digital signatures, satisfying state auditors with thorough and accurate records.
Bottom line: Verified trips mean fewer denials and stronger audit defense.
D. Integrated Dispatch and Billing
- The Problem
In many systems, dispatchers log trip data in one platform while billing clerks re-enter it in another. Every re-entry multiplies the chance of errors. - The Solution
An integrated system connects scheduling, dispatch, and billing in a single workflow. Trip details—such as mileage, patient ID, and timestamps—automatically flow into claims generation. - The Outcome
Fewer duplicate entries, fewer mismatches, faster claim submission.
Efficiency Insight: One behavioral health transport provider cut billing administration time by half after moving from manual entry to an integrated platform.
Bottom line: Unified workflows eliminate the swivel-chair problem that drives denials.
E. EDI Integration with Clearinghouses (837/835)
- The Problem
Paper claims and manual uploads create bottlenecks, while formatting errors often result in rejections. - The Solution
Systems that generate CMS-1500 or EDI 837 claims feed directly into clearinghouses. Built-in rules validate claims against Medicaid standards before submission. Automated remittance posting (EDI 835) eliminates the need for manual reconciliation. - The Outcome
Providers accelerate reimbursement and shorten Days Sales Outstanding (DSO).
Financial Impact: A regional operator reduced average DSO from 60 days to 28 days by adopting EDI 837/835 workflows.
Bottom line: Direct EDI integration streamlines payments and minimizes the risk of rejection.
F. Fraud Prevention and Audit Readiness
- The Problem
Even legitimate claims can trigger fraud flags if data trails are incomplete. Providers without verifiable proof face unnecessary denials or prolonged audits. - The Solution
Audit logs capture GPS path, timestamps, driver ID, and patient signatures in tamper-proof records. Role-based permissions restrict access to PHI to authorized staff only. Built-in anomaly detection flags suspicious billing patterns before submission. - The Outcome
Providers pass audits confidently and prevent fraud flags from delaying reimbursement.
Outcome: A Florida behavioral health provider avoided a fraud investigation when their system automatically produced verifiable logs for every trip billed.
Bottom line: Strong verification safeguards revenue while protecting reputation.
G. Compliance by Design (HIPAA, SOC 2, CMS)
- The Problem
Off-the-shelf tools often lack compliance safeguards, putting providers at risk of fines and contract loss. - The Solution
Custom systems embed HIPAA-grade encryption, SOC 2 Type II safeguards, and CMS audit-ready workflows. Immutable audit trails protect PHI and meet regulatory requirements. - The Outcome
Providers stay compliant without scrambling for last-minute fixes when audits arrive.
Regulatory Note: With HIPAA fines reaching $50,000 per violation, compliance built into the foundation is not optional—it’s a matter of survival.
Bottom line: Compliance baked into workflows ensures long-term security and payer trust.
The Big Picture
Technology does more than reduce denials. It rewrites the billing equation entirely. By embedding eligibility checks, prior authorization tracking, trip verification, and compliance into daily workflows, providers shift from reactive firefighting to proactive revenue protection.
The result is straightforward:
- Higher first-pass acceptance rates
- Shorter reimbursement cycles
- Lower compliance risk
- More predictable cashflow
VI. Why Off‑the‑Shelf Billing Systems Fail
Generic healthcare billing and transportation tools look tempting. Quick setup, lower sticker price, familiar screens. In Medicaid NEMT, that promise breaks under real rules, real volumes, and real audits. The result is higher denial rates, hidden costs, and blind spots providers cannot afford.
A. One‑Size‑Fits‑All Codes and Templates
- The problem
Medicaid rules are not uniform. Each state sets its own mix of HCPCS codes, modifiers, mileage logic, and prior authorization workflows. Generic systems assume one template fits all. - The impact
When templates fail to capture state-specific quirks, claims are rejected for the basics: incorrect modifier, missing attestation, or bundled miles billed separately. Denials climb, cash stalls. - Example
A Pennsylvania provider using a generic platform saw a 22 percent denial rate because the software could not support the state’s wheelchair lift modifiers out of the box. Staff resorted to manual edits, which introduced new errors.
Bottom line: Templates that ignore state rules convert routine trips into avoidable denials.
B. Poor Integration with Dispatch Systems
- The problem
Dispatch in one system, billing in another. Data is re‑typed, re‑mapped, and re‑checked. Every swivel of the chair invites error. - The impact
Duplicate claims, mismatched mileage, and missing timestamps. Clearinghouses reject on format. Payers deny the content. Staff spend hours reconciling the same trip in two places. - Example
A Midwest operator logged trips in a dispatch app and then entered them into a billing portal. Thirty extra hours a week were spent on duplicate entry, resulting in a measurable increase in mismatched HCPCS codes.
Bottom line: If dispatch and billing do not share a source of truth, denial risk compounds at volume.
C. Limited Reporting and Analytics
- The problem
Many off‑the‑shelf systems show totals only. Claims in, claims out. No drill‑down by payer, code, broker, or denial reason. - The impact
Leaders cannot identify patterns, forecast cash flow, or address payer-specific issues. Revenue leakage hides in plain sight. - Example
A 50-vehicle fleet discovered, after a year, that one broker had rejected 80 percent of trips due to PA mismatches. Their billing tool lacked denial reason trendlines, so the signal surfaced months late. Lost revenue exceeded $500,000.
Bottom line: Without denial analytics, teams fight fires, not causes.
D. Vendor Lock‑In and Escalating Costs
- The problem
Subscription tools control the roadmap. Providers wait for updates when Medicaid rules shift. Pricing ratchets up with volume. - The impact
As you grow, you pay more, yet critical updates can lag for quarters. Meanwhile, staff build manual workarounds. Cost rises on both fronts. - Example
A regional operator started at $1,200 per month. Three years later, the fee increased to $3,500 per month, plus integration charges, and the system still lacked support for a new state Medicaid API. Growth without control.
Bottom line: When you do not own the capability, you rent your future.
E. Compliance Gaps
- The problem
Generic tools often treat HIPAA, CMS program integrity, and audit logs as add‑ons. PHI encryption, access controls, and immutable trip‑to‑claim trails are incomplete or absent. - The impact
Exposure grows. A single incident can result in fines of up to $50,000 per violation, as well as potential contract risks with brokers and state agencies. - Example
A Texas operator faced a HIPAA penalty after driver app logs exposed PHI without encryption at rest. The vendor disclaimed responsibility because the product was not designed to meet HIPAA-grade controls.
Bottom line: Compliance cannot be bolted on. It must be baked in.
F. Inflexibility in Multi‑State Operations
- The problem
Expanding across counties or states introduces new rules for EVV, rural mileage thresholds, PA cadence, and filing windows. Many off‑the‑shelf systems lack configurable rules engines. - The impact
Teams run parallel workflows per state, then reconcile by hand. Scale stalls. Errors climb. Morale dips. - Example
A provider serving Ohio and Kentucky ran two billing processes because their tool could not support both states’ rules in one environment. Extra staffing cost: roughly $80,000 per year.
Bottom line: If the software cannot adapt to state variations, expansion becomes a cost center, not a growth lever.
The Bottom Line
Not more tools. Better workflows. Off‑the‑shelf billing solves for averages, but Medicaid NEMT lives in specifics. Rules vary, auditors scrutinize, and cash flow depends on clean first-pass claims. If your system cannot integrate with dispatch, adapt to state policy, expose denial patterns, and meet HIPAA requirements by design, you will pay in denials, labor, and risk. Why gamble revenue on templates that were never built for your routes, your payers, your rules?
VII. The Case for Custom Billing Software
For years, many NEMT providers have relied on broker portals or generic billing platforms. That patchwork may work for a handful of trips in a single state. But when volumes scale, rules diverge, and audits intensify, the cracks become unsustainable. Custom billing software flips the script. Instead of forcing your operation to conform to rigid templates, it adapts to your contracts, workflows, and compliance environment.
A. Tailored to Payer and State Medicaid Rules
- The problem with generic tools
They assume one set of rules across the board. In reality, each state and payer has its own specific requirements, including HCPCS modifiers, round-trip bundling, rural mileage thresholds, and EVV mandates. - The custom advantage
A configurable rules engine encodes each payer’s requirements directly into the billing system. Updates are immediate, not dependent on a vendor’s next release cycle. - The outcome
Claims align with state and payer rules during the initial review, drastically reducing denials.
Scenario: A multi-state Midwest provider reduced denials by 35 percent after deploying a custom rules-based engine integrated with state Medicaid APIs.
Bottom line: Custom rules engines turn state variability from a liability into a strength.
B. Seamless Integration with Dispatch and Scheduling
- The problem with siloed systems
Dispatchers and billing clerks often duplicate effort. Trip data logged once must be keyed again into a billing portal. Every re-entry creates opportunities for mismatches. - The custom advantage
Dispatch and billing operate as one. Trip mileage, timestamps, vehicle IDs, and proof-of-delivery flow directly into claim generation. - The outcome
Duplicate entry disappears. Denials tied to mismatched trip data plummet.
Efficiency gain: A behavioral health operator cut billing admin time by 50 percent after adopting a dispatch-to-billing integration built for their workflows.
Bottom line: Unified data capture means faster billing, fewer denials, less rework.
C. Custom Reporting Dashboards
- The problem with generic reports
Totals hide trends. Providers see how much was submitted and paid, but not why claims failed or which payers are underperforming. - The custom advantage
Dashboards flag denial reasons by code, payer, and broker. Leaders gain insight into where revenue is leaking and which contracts create the most risk. - The outcome
Providers shift from reactive denial fixing to proactive revenue protection.
Leadership value: A 50-vehicle fleet built denial heatmaps into its dashboard. The tool revealed that one broker was responsible for 70 percent of the delays. They used the data to renegotiate terms, recovering $200,000 annually.
Bottom line: Custom reporting turns billing data into business intelligence.
D. Scalable for Multi-Payer Environments
- The problem with growth
Medicaid may be the starting point, but providers often expand into Medicare Advantage, managed care, and commercial contracts. Off-the-shelf systems choke on this mix. - The custom advantage
Custom platforms support multi-payer workflows under one roof. Medicaid, Medicare, and private-pay claims all run through the same system. - The outcome
Providers scale seamlessly without layering redundant systems or staff.
Expansion example: A regional fleet expanded from Medicaid-only to a mixed payer model (Medicaid, Medicare Advantage, and commercial). Their custom platform handled the transition without adding a second billing tool.
Bottom line: Growth requires flexibility, not parallel workarounds.
E. Ownership of Intellectual Property (IP)
- The problem with vendor lock-in
SaaS vendors own the codebase. Providers are dependent on vendor timelines for updates and price increases. - The custom advantage
With custom development, providers own the code, data models, and workflows. They control updates, integrations, and scaling decisions. - The outcome
Cost savings over time, independence from vendor roadmaps, and resilience as Medicaid evolves.
Strategic control: One large operator avoided $300,000 per year in subscription fees by building a custom platform they owned outright.
Bottom line: Owning the system means owning your future.
F. Compliance by Design
- The problem with bolt-on compliance
Many vendors add HIPAA safeguards as patches, rather than as foundational elements. Logs, encryption, and access controls are incomplete. - The custom advantage
Compliance is architected from the ground up, featuring HIPAA encryption at rest and in transit, SOC 2 Type II standards, audit-ready trip logs, and PHI access controls. - The outcome
Providers walk into Medicaid audits with confidence, not fear.
Compliance win: A New York operator passed a Medicaid audit with zero findings after adopting custom billing software that tied every billed trip to GPS and electronic proof-of-delivery.
Bottom line: Compliance by design eliminates surprises and protects contracts.
The Bigger Picture
Custom billing software is more than just a technical upgrade. It is a strategic asset. Providers that invest in tailored systems see measurable gains in:
- Revenue protection: Denials drop, reimbursements accelerate.
- Operational efficiency: Manual re-entry is minimized, allowing staff to focus on prevention.
- Compliance confidence: Audits become routine, not existential.
- Scalability: Systems adapt to new states, payers, and contracts.
Margins in NEMT are thin. Compliance risk is high. The difference between growth and closure often lies in whether billing is treated as generic admin or strategic infrastructure.
See how NEMT Data Dashboards Improve ROI
VIII. Real-World Impact (Use Cases)
Custom billing systems for Medicaid NEMT aren’t theory. Providers across the U.S. are already using them to recover revenue, cut administrative costs, and pass compliance audits with confidence. The following cases highlight measurable results.
A. Multi-State Provider Reduces Denials by 35%
- The Challenge
A large operator serving multiple states struggled with chronic denials, averaging nearly 20 percent of claims each month. Each state imposed different Medicaid rules, prior authorization requirements, and clearinghouse pathways. Billing staff were drowning in rework, and the provider lost more than $100,000 per quarter in unrecoverable revenue. - The Solution
They implemented a custom billing engine integrated directly with state Medicaid APIs. Key features included:- Real-time Medicaid eligibility checks before dispatch (270/271 transactions).
- Automated prior authorization tracking with alerts for expiring approvals.
- GPS-verified trip completion tied directly to claim line items.
- The Outcome
Within six months:- Denial rates dropped from 20 percent to under 7 percent.
- Average reimbursement time improved by 15 days.
- Annual revenue recovery exceeded $400,000.
Bottom line: Custom billing stabilized cash flow and gave leadership confidence to expand into new counties.
B. Behavioral Health Transport Cuts Billing Admin Hours by 50%
- The Challenge
A behavioral health transport provider managed more than 10,000 trips per month. Billing clerks manually keyed trip data from dispatch logs into a separate billing portal. Errors and duplicates were constant, and most of the billing team’s week was spent fixing denials. - The Solution
The provider deployed an integrated dispatch + billing system with:- One-click EDI 837 claim submission.
- Auto-matching of Medicaid remittances (835) with trip records.
- Dashboards showing denial reasons by payer and code.
- The Outcome
- Billing rework fell by 50 percent.
- Payroll savings equaled two FTE billing clerks, about $90,000 annually.
- Denials tied to mismatched trip data dropped by 65 percent.
Bottom line: Integrated systems converted a denial factory into a streamlined billing engine.
C. Regional Fleet Accelerates Reimbursements from 60 Days to Less Than 30
- The Challenge
A 30-vehicle fleet in the Midwest faced chronic cash flow problems. Medicaid reimbursements took 60–75 days due to slow claim submission, lack of real-time tracking, and manual reconciliation of payments. - The Solution
They adopted an EDI-integrated billing platform with:- Automated claim validation before submission, catching format errors early.
- Real-time claim status updates (276/277 transactions).
- Automated remittance posting linked directly to dispatch records.
- The Outcome
- Days Sales Outstanding (DSO) dropped from 63 days to 28 days.
- Improved cash floww allowed the fleet to expand into two new counties withoutincurringn debt.
- A major broker flagged them as a “preferred partner,” leading to new contracts.
Bottom line: Faster reimbursement turned cashflow from a liability into a growth driver.
D. Small Operator Strengthens Audit Defense
- ThebChallenge
A small Illinois provider nearly lost its Medicaid contract after an audit flagged missing proof-of-delivery records for 15 percent of trips. The rides occurred, but without compliant documentation, payments were at risk of being clawed back. - The Solution
The operator implemented a trip verification and audit log module with:- GPS-stamped pickup and drop-off coordinates.
- Patient e-signatures are tied directly to claims.
- Immutable logs showing driver ID, timestamps, and mileage.
- The Outcome
- At the next audit, the provider produced a full trip-to-claim report in under 30 minutes.
- Audit risk was neutralized, preserving a Medicaid contract worth $2 million annually.
- The system also reduced patient no-shows by 18 percent through automated reminders.
Bottom line: Compliance-ready documentation turned a near-miss into a long-term contract win.
The Takeaway
Across these cases, three themes stand out:
- Denials shrink when eligibility, prior authorization, and trip verification are automated.
- Admin costs drop when dispatch and billing share a single workflow.
- Cash flow improves when EDI automates claim submission, tracking, and posting.
Whether a provider runs 30 vehicles or 300, custom billing systems transform Medicaid NEMT from fragile and reactive to predictable and growth-ready.
IX. Quick Stats
Numbers often cut through complexity faster than narrative. Medicaid NEMT billing is riddled with inefficiencies, denials, and compliance risks that providers cannot afford to overlook. The following statistics highlight just how big the stakes are—and how much providers stand to gain by modernizing their systems.
1. Claim Denials Are Widespread
- Between 10% and 20% of Medicaid claims are denied on their first submission (CMS).
- In certain states, denial rates exceed 25 percent, often tied to prior authorization mismatches or eligibility gaps.
- Even when denials are corrected and appealed, providers typically lose 5 to 10 percent of total revenue permanently.
What this means: Every tenth trip—or more—is at risk of going unpaid without intervention.
2. Rework consumes Staff Time
- Up to 40 percent of billing staff time is spent fixing denied claims.
- Each denial can take 30 to 60 minutes to identify, correct, and resubmit.
- A provider processing 5,000 trips per month wastes hundreds of staff hours on denial corrections alone.
- 40 percent = reworking denials
- 35 percent = claim submission
- 25 percent = denial prevention and analytics
What this means: Providers are paying for labor that doesn’t advance the business—it just patches holes.
3. Delayed Reimbursements Strain Cashflow
- Denied or corrected claims can take 60 to 90 days—or longer—to process.
- Even “clean” claims often take 30–45 days to be reimbursed.
- Providers that automate EDI 837/835 claim workflows routinely cut reimbursement cycles to under 30 days.
- Manual or paper claims = 60–90 days
- Automated EDI claims = fewer than 30 days.
What this means: Faster cash flow directly reduces reliance on credit lines, often saving providers $20,000 to $50,000 annually in financing costs.
4. HIPAA Compliance Risks Carry Heavy Penalties
- HIPAA fines can reach $50,000 per violation, with repeat violations capped at $1.5 million annually.
- Many generic billing tools lack encryption at rest, audit logs, or SOC 2 readiness.
- Compliance failures not only trigger fines, they can also jeopardize state Medicaid contracts.
What this means: Compliance gaps don’t just create financial risk—they threaten the survival of the contract itself.
5. Financial Stakes Are Massive
- Missed medical appointments cost the U.S. more than $150 billion annually (NIH).
- Reliable NEMT directly reduces preventable ER visits and readmissions by ensuring patients receive timely care.
- For providers, even a 5% improvement in claim acceptance can mean hundreds of thousands of dollars in annual revenue recovery.
- Fleet size
- Trips per month
- Average reimbursement per trip
Outputs would estimate:
- Denials avoided
- Staff hours saved
- Revenue recovered
What this means: The return on billing automation often pays for itself within 9 to 12 months.
The Bottom Line
The data is clear:
- Denials are common.
- Staff are overburdened.
- Cash flow is fragile.
- Compliance risks are expensive.
Technology isn’t a luxury add-on. It is the only way providers can remain solvent, compliant, and competitive in the Medicaid NEMT market.
X. How Mindbowser Helps
Solving Medicaid NEMT billing challenges is not about installing off-the-shelf software. It requires a structured approach that blends technology, compliance expertise, and a deep understanding of provider workflows. Over the past decade, Mindbowser has partnered with NEMT operators, brokers, and healthcare organizations to re-engineer billing operations, reduce denials, and accelerate reimbursements. Here is how the process works.
A. Discovery: Mapping Workflows and State Medicaid Rules
- Capturing the as-is state
The first step is to understand how billing works today. Mindbowser interviews billing teams, dispatchers, and drivers to document the real process from trip scheduling to claim submission. - Identifying denial hotspots
Historical claim data is analyzed to uncover patterns in denial reasons. Prior authorization errors, eligibility mismatches, and incomplete trip records often emerge as root causes. - Documenting state-specific requirements
Since every Medicaid program operates differently, Mindbowser creates a payer-by-payer rulebook covering authorization workflows, coding standards, documentation formats, and submission timelines.
Consultant’s note: Providers often underestimate hidden rules such as rural mileage thresholds or trip bundling. Capturing these rules early prevents expensive rework later.
Bottom line: Discovery ensures that the solution is tailored to the provider’s environment, not a generic template.
B. Prototype: Building the Billing Dashboard and Integration Workflows
- Wireframing the solution
Visual mockups show how eligibility checks, authorization trackers, and claim workflows will look in practice. - Creating reporting previews
Sample dashboards highlight denial trends, payer performance, and cash flow insights. Leadership gets an early view of how data will drive decision-making. - Mapping integrations
Workflow diagrams illustrate how dispatch data will flow into billing, then to clearinghouses and payers.
This step enables stakeholders to preview the future system before its full rollout, fostering alignment and reducing resistance.
Bottom line: Prototyping builds confidence that the system will solve real-world problems before development begins.
C. Agile Build: Phased Delivery with Compliance Built In
- Sprint-based approach
Development happens in phases, each delivering measurable value. Typical sprint sequence:- Sprint 1: Eligibility auto-check and prior authorization tracker.
- Sprint 2: Trip verification with GPS, e-signature, and proof-of-delivery logs.
- Sprint 3: Integrated claim generation with EDI 837/835 submission.
- Sprint 4: Analytics dashboards for denial prevention and cashflow monitoring.
- Compliance from day one
Every sprint undergoes HIPAA safeguard review, PHI audit logging, and SOC 2 readiness checks. Compliance is part of the foundation, not a late-stage patch.
Result: A behavioral health operator saw denial rates fall by 12 percent after the very first sprint—eligibility checks—was deployed.
Bottom line: Agile delivery means faster wins for providers while building a fully compliant, long-term solution.
D. Support: SLA-Based Claim Monitoring and Compliance Updates
- Ongoing claim monitoring
After go-live, Mindbowser provides 24/7 support for issues like claim submission errors, EDI transaction failures, or broker integration updates. - Staying current with Medicaid rules
State Medicaid rules evolve constantly. Mindbowser ensures providers stay compliant by releasing timely updates for new prior authorization formats, EVV mandates, and submission protocols. - Quarterly performance reviews
Every quarter, providers receive an ROI report showing reductions in denial rates, shortened DSO, and administrative hours saved.
Real-world example: When New York Medicaid rolled out a new prior authorization submission API, a provider on Mindbowser’s platform adapted in two weeks. Competitors relying on SaaS vendors waited nearly eight months for vendor updates.
Bottom line: Continuous support protects revenue long after deployment.
E. Why Mindbowser? Domain Expertise Matters
- Healthcare-first approach
Mindbowser combines 10+ years of healthcare technology experience with expertise in HIPAA, HL7/FHIR, and CMS program integrity. - Direct NEMT experience
The team has built platforms for operators in New York, Illinois, and the Midwest. This means workflows are grounded in field-tested realities. - Code ownership policy
Providers retain full ownership of their custom systems. No vendor lock-in, no rising subscription fees. - Future-ready capabilities
Beyond billing, Mindbowser builds predictive scheduling, AI-driven denial prevention, and EHR integrations into platforms, preparing providers for growth.
The consultant’s takeaway: Providers don’t need another generic billing tool. They need a partner who understands Medicaid’s complexity and designs technology that reduces denials, protects compliance, and scales with growth. That is the role Mindbowser plays.
Net Result
Mindbowser’s process—discovery, prototype, agile build, and ongoing support—turns Medicaid billing from a fragile, manual process into a strategic asset. Providers using these systems consistently see:
- Lower denial rates.
- Faster reimbursements.
- Reduced administrative burden.
- Audit readiness at all times.
In a market where margins are razor-thin and compliance risk is constant, the right partner makes billing predictable, defensible, and growth-ready.
XI. Summary
Billing is the lifeline of NEMT operations. Vehicles, drivers, and dispatchers may keep the service running day to day, but without clean Medicaid claims, providers do not get paid. And when cash flow stalls, the impact spreads quickly to patients, hospitals, and payers alike.
A. Medicaid NEMT Billing Is Both Critical and Fragile
- Every trip must prove medical necessity, prior authorization, and completion with documentation.
- Between 10% and 20% of Medicaid claims are denied on their first submission.
- State-by-state rule variations add complexity that overwhelms even experienced billing teams.
Bottom line: Billing is not back-office clerical work. It is mission-critical infrastructure.
B. The Real Cost of Errors Goes Beyond Lost Revenue
- Denials delay reimbursement cycles by 30 to 90 days.
- Many denials—like expired prior authorizations or late submissions—are unrecoverable, costing providers hundreds of thousands annually.
- Compliance failures can result in HIPAA fines of up to $50,000 per violation and jeopardize contracts.
- Repeated billing failures erode trust with brokers, hospitals, and patients.
Bottom line: Errors cost money, time, reputation, and contracts.
C. Technology Changes the Equation
- Eligibility auto-checks prevent wasted rides before they happen.
- Prior authorization trackers close one of the largest denial gaps.
- GPS trip verification and electronic proof of delivery make audits more defensible.
- EDI integrations accelerate reimbursements and reduce rework.
- Fraud prevention and HIPAA compliance are seamlessly integrated into workflows.
Bottom line: Automation shifts providers from reactive denial-fighting to proactive revenue protection.
D. Off-the-Shelf Tools Will Not Cut It
- Generic billing platforms struggle with state-specific Medicaid rules.
- They fail to integrate dispatch and billing seamlessly.
- Reporting is limited to surface-level information and overlooks trends of denial.
- Subscription costs rise as volume grows, while compliance remains patchy.
Bottom line: What looks inexpensive up front often creates higher costs in denials, staff hours, and risk.
E. The Case for Custom Billing Software Is Clear
- Tailored rules engines reduce denials by aligning with payer-specific requirements.
- Integrated dispatch-to-claim workflows eliminate duplicate data entry, streamlining the process.
- Dashboards surface denial reasons and cashflow bottlenecks.
- Systems scale across payers and states without duplication.
- Providers own the platform, avoiding vendor lock-in and unpredictable pricing.
Real-world outcomes:
- Denials reduced by 35 percent.
- Billing rework cut by half.
- Reimbursement cycles shortened by more than 30 days.
Bottom line: Custom systems protect revenue, strengthen compliance, and support growth.
The Final Word
Medicaid billing is both the most fragile and the most important function in NEMT. Providers relying on manual processes or generic tools will continue to face denial cycles, compliance investigations, and unstable cash flow. Providers who modernize with custom-built software can ensure accuracy, accelerate payments, and maintain trust with payers.
This is not about fixing clerical errors. It is about reimagining billing as a strategic driver of financial stability and patient access to care. The providers who invest in custom, compliance-ready billing will not only survive Medicaid’s complexity. They will thrive in it.
The most common denial drivers include:
- Missing or expired prior authorizations.
- Eligibility mismatches where a patient is not covered on the date of service.
- Incomplete trip records such as missing timestamps, GPS logs, or proof-of-delivery.
- Incorrect HCPCS or mileage codes.
- Duplicate or late submissions.
Executive insight: Most of these issues are preventable with automated eligibility checks, prior authorization tracking, and trip verification tools. Providers that automate these steps cut denial rates by more than half.
- Clean claims usually take 30 to 60 days for reimbursement.
- Denied or corrected claims can stretch payment cycles to 60 to 90 days or longer.
- Providers using EDI 837/835 automation often reduce turnaround to under 30 days.
Executive insight: Track Days Sales Outstanding (DSO) as a core KPI. Anything consistently above 45 days signals process inefficiencies.
Yes, and it should. Integration is not a feature; it is a requirement.
- Dispatch data (trip times, mileage, patient ID) should flow directly into claims.
- Integrated workflows ensure the same record drives scheduling, trip verification, and billing.
- This eliminates duplicate data entry and reduces mismatched claim errors.
Executive insight: When evaluating a platform, ask if dispatch data auto-populates into claims. If staff still re-enter information, denial risk remains high.
Fraud prevention depends on audit-ready data trails. Custom systems embed these protections into daily workflows.
- GPS-stamped trip logs tied to each claim.
- Electronic proof-of-delivery (signature, PIN, or photo).
- Immutable audit trails showing driver ID, timestamps, and odometer readings.
- Rules engines that flag suspicious patterns like duplicate trips or excessive mileage.
Executive insight: Strong audit logs not only protect against fraud but also prevent legitimate claims from being frozen during investigations.
Yes. The ROI is clear and often fast.
- Denial reduction alone (from 20 percent down to under 5 percent) usually delivers payback in 6 to 12 months.
- Faster reimbursements improve cashflow, reducing reliance on credit lines.
- Compliance readiness prevents fines and preserves Medicaid contracts.
- Long term, custom platforms scale across states and payers without recurring vendor fees.
Executive insight: Run a denial-prevention ROI model. Take your current denial percentage, apply it to monthly billing volume, and calculate potential revenue recovered if denials are cut in half. For most operators, the savings cover the system within a year.


