



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
- 419 hospitals across 147 systems and 39 states are approved for CMS’s Acute Hospital Care at Home program, serving over 31,000 patients (CMS, September 2025). Congress extended the waiver to 2030.
- Episodes cost 32% less than inpatient care ($5,081 vs $7,480), readmissions run lower (7% vs 23% in RCT data), and patient satisfaction exceeds 90% (AHRQ PSNet).
- But hospital-at-home is not chronic RPM with the volume turned up. It requires continuous monitoring every 5-15 minutes, 24/7 command centers, video visit capability, and DRG-based reimbursement that pays $5,000-15,000+ per episode.
- The technology architecture is the barrier to entry, and the systems that build it now have a four-year runway before the waiver expires.
In November 2020, CMS issued the Acute Hospital Care at Home waiver as a pandemic measure. Nobody expected 419 hospitals across 39 states to still be running it five years later, or that Congress would extend it to 2030.
What started as “we need beds during COVID” became something different. Health systems discovered that certain patients, those with heart failure exacerbations, COPD flare-ups, pneumonia, cellulitis, did as well or better at home as they did in a hospital bed. The outcomes data confirmed it. The cost data made the CFOs pay attention. And by the time the pandemic emergency ended, the waiver had become too valuable to let expire.
The technology story here is worth understanding because it explains why hospital-at-home is not simply an extension of existing chronic RPM programs. The monitoring requirements, the staffing model, the reimbursement structure, and the system architecture are fundamentally different. We will walk through each of those differences, because the health systems that understand this distinction will build the infrastructure that defines acute care for the next decade.
How Did a Pandemic Waiver Become a Permanent Program?
The trajectory tells the story.
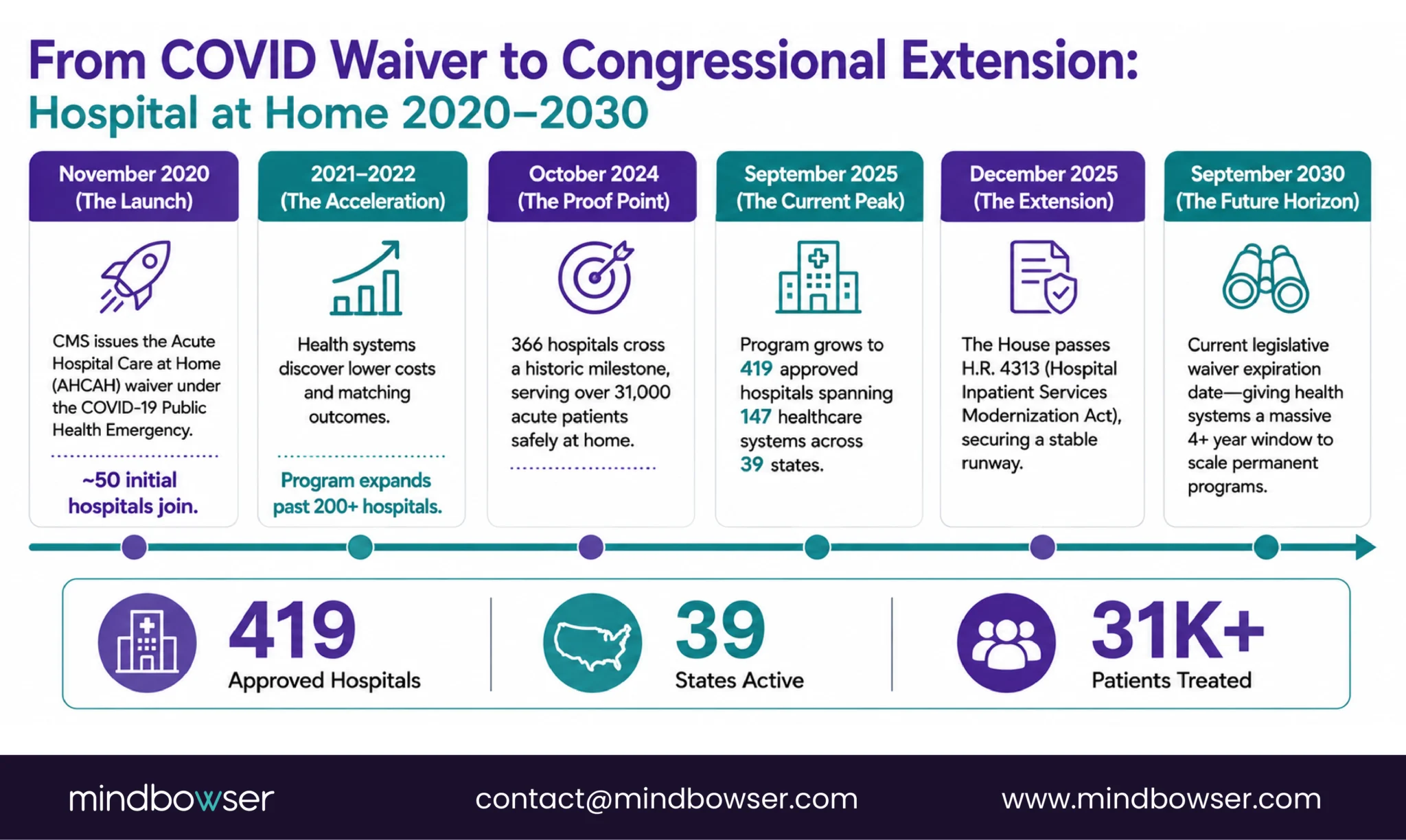
- November 2020: CMS issues the AHCAH waiver under the COVID-19 Public Health Emergency. Initial participating hospitals: roughly 50. The rationale was simple: hospitals needed bed capacity. Sending stable acute patients home with monitoring freed beds for sicker patients.
- 2021-2022: Adoption accelerated beyond the bed-capacity rationale. Health systems running AHCAH programs noticed something the CMS actuaries would later confirm: these episodes cost less, produced comparable outcomes, and patients overwhelmingly preferred them. Participating hospitals grew past 200.
- October 2024: 366 hospitals had served over 31,000 patients under the waiver. A JAMA article analyzed participation patterns and found broad adoption across system sizes and geographies (JAMA, 2024).
- December 1, 2025: The House passed H.R. 4313, the Hospital Inpatient Services Modernization Act, extending the waiver through September 2030 (Newsweek, 2025). This was not a temporary patch. Congress looked at the data and decided hospital-at-home deserved a runway.
- September 2025: 419 hospitals across 147 systems and 39 states approved. CMS announced a second public data release for March 17, 2026, covering April 2023 through September 2025. Two and a half years of patient outcome data about to become public.
- January 2026: A STAT News piece by the architect of the original CMS waiver argued that Congress needs to go further, moving hospital-at-home from waiver status to permanent program with updated requirements (STAT News, 2026).
The arc from emergency measure to Congressional extension happened because the data kept saying the same thing: comparable clinical outcomes at 32% lower cost with 90%+ patient satisfaction. That combination is rare enough in healthcare to sustain political support across five years of shifting priorities.
The timeline below shows how hospital-at-home evolved from a COVID emergency waiver into a multi-state care delivery model extended through 2030.
What Do the Outcomes Actually Show?
The evidence base is now substantial enough to draw conclusions with confidence.
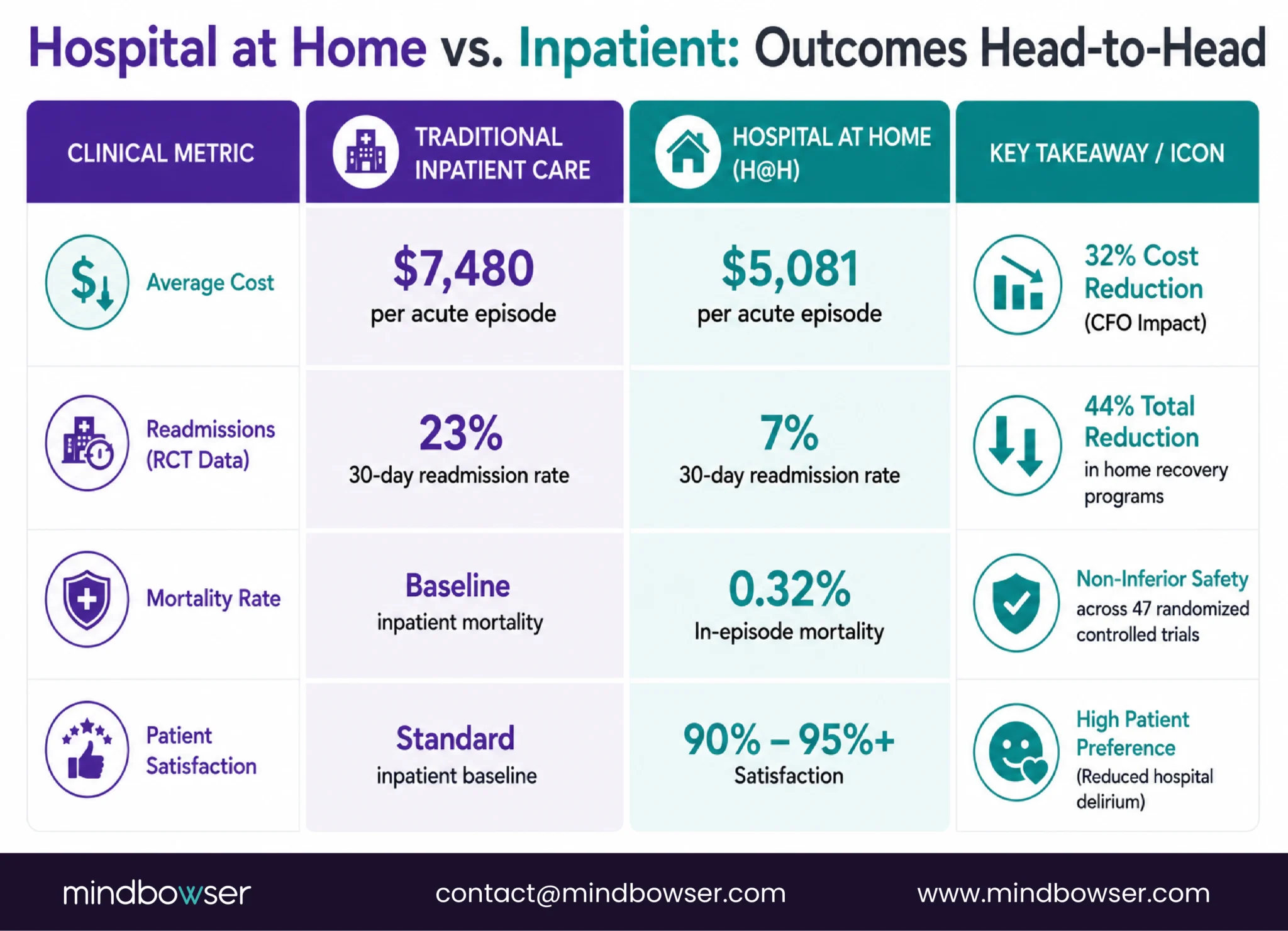
- Cost: AHRQ data shows hospital-at-home episodes average $5,081 compared to $7,480 for equivalent inpatient episodes. A 32% cost reduction per episode. CMS’s own report confirmed lower Medicare spending in the 30-day post-discharge period for more than half of the top 25 MS-DRGs compared to traditional inpatient stays (AMA, 2025).
- Readmissions: An early randomized trial of 91 elderly patients admitted through the ED with infection, heart failure exacerbation, COPD, or asthma found 30-day readmission rates of 7% for hospital-at-home patients versus 23% for hospital inpatients. A separate home recovery program reported a 44% reduction in readmission rates (AMA, 2024).
- Safety: A 2024 study reported an in-episode mortality rate of 0.32% and a 30-day mortality rate of 4.35%, comparable to conventional inpatient care. A large 2024 meta-analysis of 47 RCTs covering 9,749 participants demonstrated non-inferiority to hospital care, with no statistically significant differences in mortality, readmission, emergency attendance, or patient satisfaction.
- Patient satisfaction: Consistently above 90-95% across studies. Patients report greater comfort, more autonomy, reduced infection exposure, and less hospital-induced delirium (a significant issue for elderly inpatients). UK virtual wards integrated into the NHS reported satisfaction above 95% with a clear preference for home care.
One point of honesty: the 2024 meta-analysis shows non-inferiority, not superiority. Hospital-at-home matches hospital outcomes at lower cost. It does not universally beat them. For specific conditions and populations (elderly, heart failure, COPD exacerbation), the data tilts toward better outcomes at home. For complex surgical recovery or patients without adequate home support, traditional inpatient care remains appropriate.
Recent studies show hospital-at-home programs can match inpatient outcomes while reducing cost and readmissions.
How Is Hospital-at-Home RPM Different from Chronic RPM?
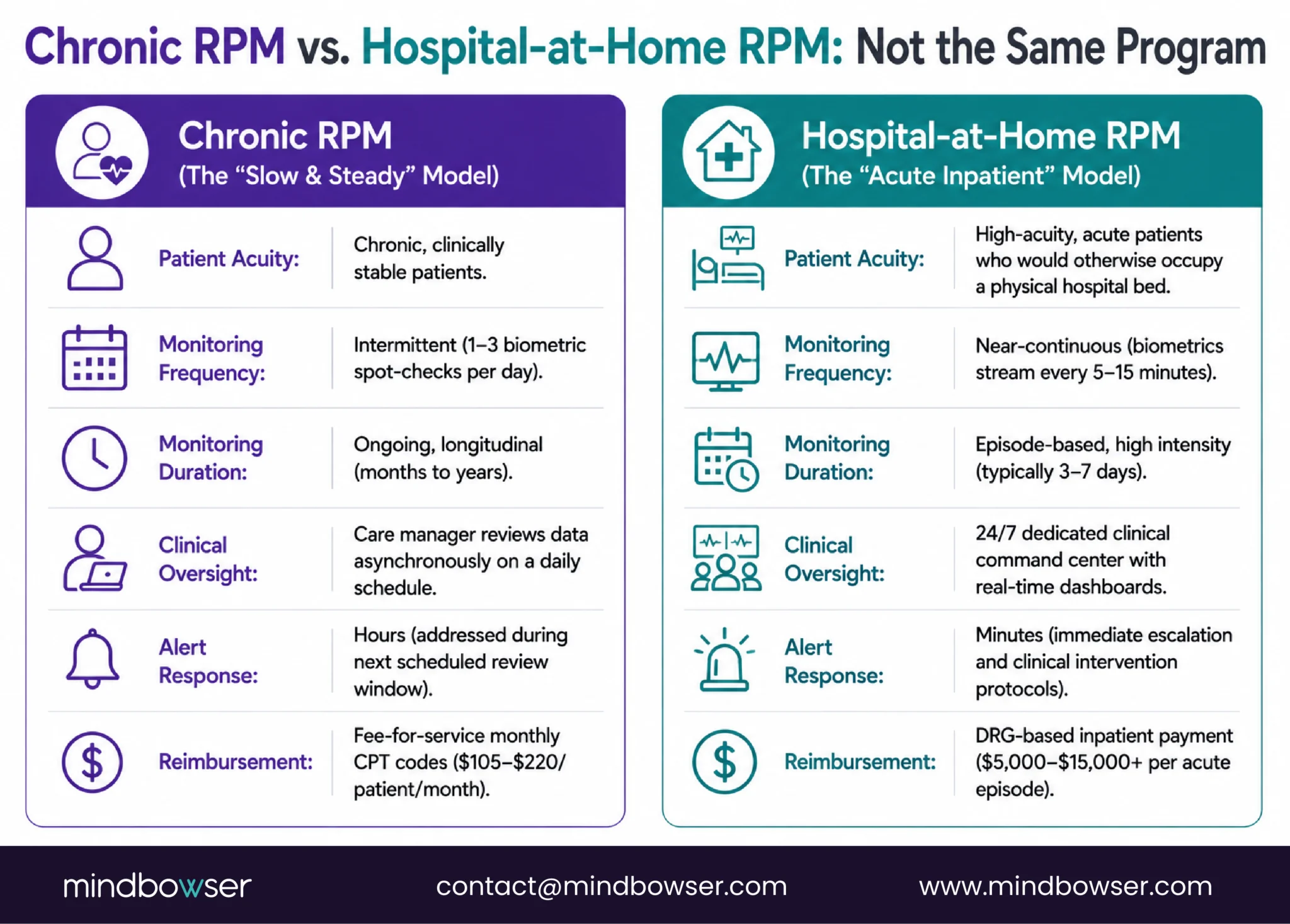
This is the distinction most people miss, and it explains why chronic RPM vendors cannot simply extend their platforms to hospital-at-home.
A PMC analysis from 2023 identified three monitoring modalities essential for hospital-at-home: vital sign monitoring (continuous), continuous single-lead ECG (cardiac patients), and fall monitoring (PMC, 2023). These are not the once-daily spot checks of chronic RPM. They are continuous data streams requiring real-time clinical interpretation.
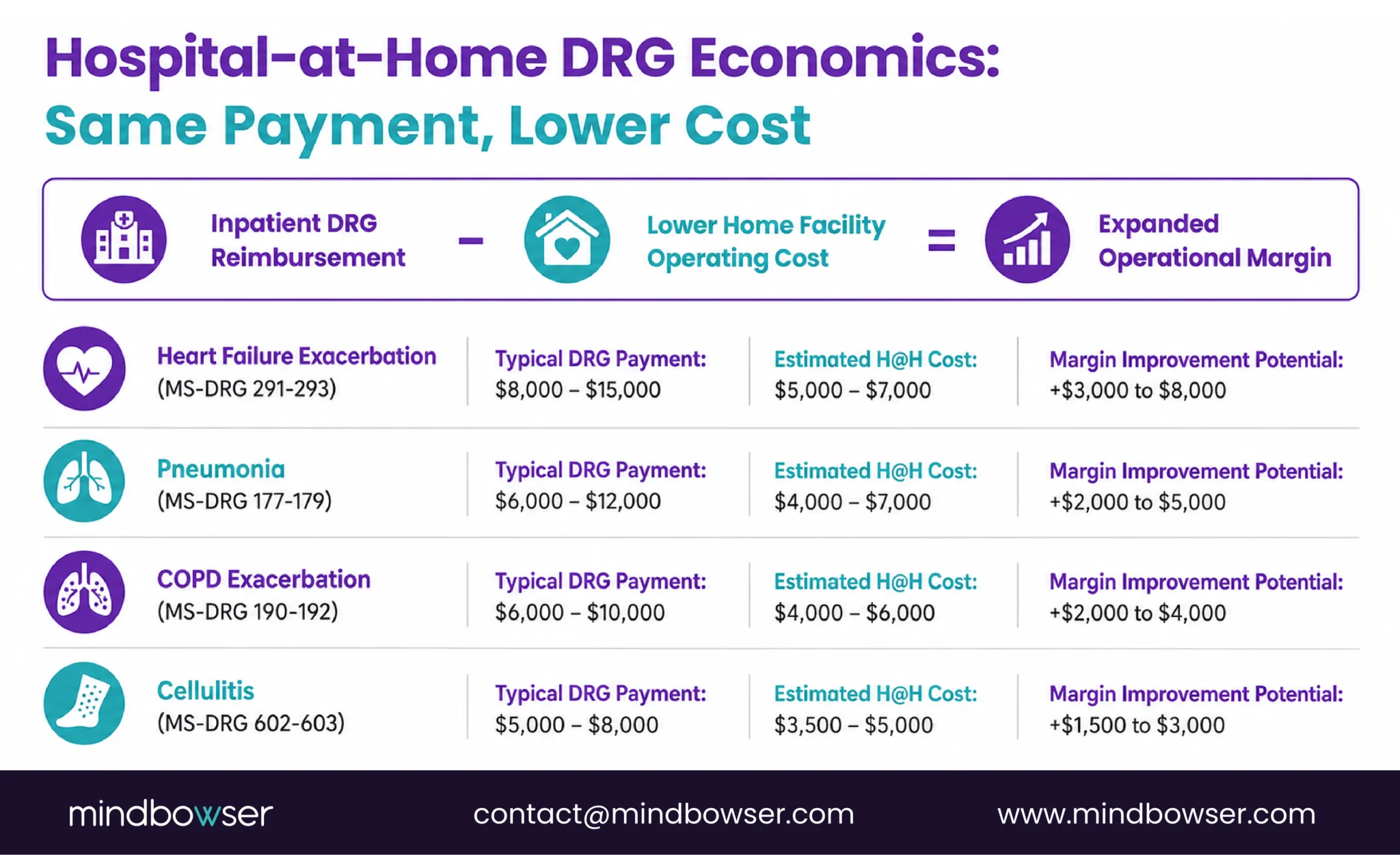
The reimbursement difference is equally fundamental. Chronic RPM generates $105-220 per patient per month through CPT codes. Hospital-at-home generates DRG-based payment, the same reimbursement the hospital would receive for an inpatient stay. For a heart failure exacerbation (MS-DRG 291-293), that can be $8,000-15,000 per episode. For pneumonia (MS-DRG 177-179), $6,000-12,000. The revenue per patient is an order of magnitude higher than chronic RPM.
This reimbursement structure is why hospital-at-home is the highest-revenue RPM use case by far, and why the technology investment to support it is correspondingly higher.
What Technology Does a Hospital-at-Home Program Require?
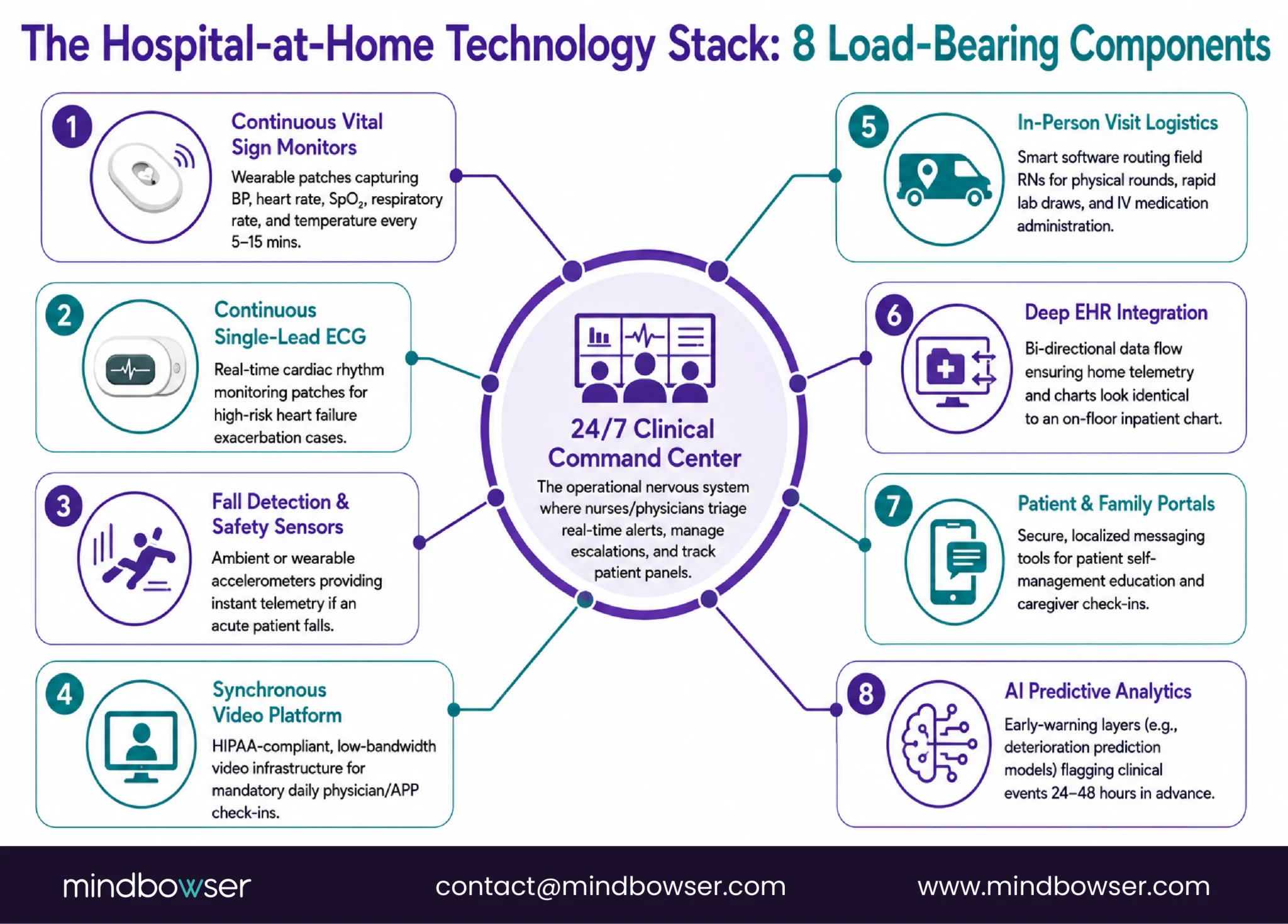
Eight technology components. Each one is load-bearing. Remove any one and the program either fails CMS requirements or puts patients at risk.
- Continuous vital sign monitoring. Blood pressure, heart rate, SpO2, respiratory rate, and temperature measured every 5-15 minutes. Bio-beat and similar continuous monitoring platforms are designed for this use case (Bio-beat, 2025). This is not a BP cuff used twice daily. It is wearable or bedside monitors capturing data at ICU-adjacent frequency in a living room.
- Continuous single-lead ECG. For cardiac patients (heart failure exacerbation is one of the most common H@H conditions), continuous rhythm monitoring is essential. Wearable ECG patches (Zio, Hexoskin, BioTelemetry) or chest-strap monitors providing real-time ECG data to the command center.
- Fall detection and safety monitoring. Acute patients at home face fall risk, especially elderly patients on new medications. Wearable accelerometers (Apple Watch fall detection, dedicated medical fall sensors) or ambient room sensors. Falls in H@H patients require immediate clinical response, not a next-day review.
- Video visit capability. CMS requires at least two physician or APP check-ins per day for AHCAH patients. At least one must be synchronous (video or in-person). The video platform must be HIPAA-compliant, reliable on the patient’s home internet, and accessible from the command center dashboard.
- 24/7 clinical command center. This is the operational backbone. Nurses and physicians monitoring patient panels continuously, reviewing vital sign trends in real time, conducting video check-ins, coordinating in-person visits, and managing escalations. The command center sees every patient’s continuous data on a single dashboard, receives prioritized alerts, and responds within minutes.
- In-person visit logistics. Daily RN visits for physical assessment, lab draws, IV medication administration, wound care. This requires visit scheduling, route optimization (multiple patients in a geography), supply chain management (medications, lab kits, equipment), and documentation that flows back to the command center and EHR.
- EHR integration. All monitoring data, video visit notes, in-person visit documentation, lab results, and medication administration records must flow into the hospital’s EHR. The patient’s chart must look as complete as an inpatient chart. This is a CMS requirement and a clinical necessity: the care team needs a single source of truth.
- Patient and family communication. Secure messaging for non-urgent questions. Education delivery for condition self-management. Caregiver alerts for patients with family members involved in care. Discharge planning communication as the episode concludes.
Here is what this architecture means in practice: a hospital-at-home program is not a chronic RPM platform with more frequent readings. It is a hospital monitoring infrastructure, the kind of system that runs an ICU step-down unit, deployed in a patient’s home. The command center is the nursing station. The video platform is the bedside interaction. The continuous monitors are the telemetry. The in-person visits are the rounds. Everything that happens on a hospital floor happens here, just distributed across homes instead of rooms.
Discuss hospital-at-home technology architecture and build strategy for your health system
What Does the Reimbursement Look Like?
Hospital-at-home is reimbursed under DRGs, not CPT codes. This is the single most important financial distinction from chronic RPM.
When a patient is admitted to an AHCAH program, the hospital receives the same MS-DRG payment it would receive for an inpatient admission for that condition. The patient is technically an inpatient. They just happen to be in their home instead of a hospital bed.
The 32% cost savings documented by AHRQ applies across qualifying DRGs because hospital-at-home eliminates the facility cost (the bed, the room, the 24/7 on-site infrastructure) while maintaining clinical services through the command center and visit model.
CMS’s own data confirmed that AHCAH episodes were associated with lower Medicare spending in the 30-day post-discharge period for more than half of the top 25 MS-DRGs. The savings extend beyond the episode itself.
Not every condition qualifies. AHCAH is specifically for patients who would otherwise require inpatient admission. The patient must be assessed in an ED or clinic, meet inpatient admission criteria, and then be offered the option to receive the care at home instead. Elective procedures, surgical recovery requiring inpatient-level nursing, and patients without adequate home environments do not qualify.
The 2030 waiver extension provides a four-year runway to build, scale, and demonstrate outcomes that support eventual permanent program status.
Who Is Building Hospital-at-Home Platforms?
The competitive market has consolidated around a few major players, each with a different model.
- Current Health (Best Buy Health). Acquired by Best Buy in 2021 for $400M. Enterprise H@H platform with continuous monitoring hardware, 24/7 clinical services, and health system integration. The largest dedicated H@H technology company. Best Buy’s retail logistics infrastructure provides a home-setup advantage no healthcare company can easily replicate.
- Biofourmis. AI-powered H@H with the Biovitals engine analyzing 120+ biomarkers for personalized baselines. The most technically sophisticated monitoring layer in the market. FDA-cleared for certain predictive algorithms. Raised $300M+ in funding.
- Medically Home. Partnership model where Medically Home provides the technology and command center infrastructure and the health system provides the clinical staff. Joint ventures with Tufts Medicine, Mayo Clinic, and others.
- Contessa Health (now part of Optum). Acquired by Amedisys in 2021, then rolled into Optum through the UnitedHealth/Amedisys acquisition. Hybrid model integrating H@H with home health services. The Optum acquisition gives Contessa access to UHC’s patient population and payer data.
- Accuhealth. H@H software platform targeting health systems that want to run their own programs without outsourcing clinical services.
The pattern across all five: they are vendor platforms. The health system subscribes, pays per-patient fees, and operates within the vendor’s technology and workflow constraints. For systems running 10-20 concurrent H@H patients, this model works. For systems scaling to 50-100+ concurrent patients, the per-patient fees compound and the lack of customization becomes a constraint.
This is where the build-vs-buy question becomes material.
Planning a hospital-at-home program?
Use Our Technology Checklist to Audit Your RPM Devices, Connectivity, Alert Workflows, and EHR Integrations in One Pass
Why Would a Health System Build Custom vs Buy a Platform?
The decision depends on scale, control requirements, and how central hospital-at-home is to the system’s strategy.
Buy (vendor platform) when:
- Running fewer than 50 concurrent H@H patients
- Testing the model before committing capital
- Need the vendor’s 24/7 command center staffing (don’t have internal capacity)
- Want a proven workflow without development time
- Timeline: 2-4 months to launch
Build custom when:
- Scaling to 50-100+ concurrent patients (per-patient vendor fees exceed build cost)
- Hospital-at-home is a strategic priority, not a pilot
- Need native EHR integration (Epic/Cerner) where H@H data is indistinguishable from inpatient data in the chart
- Want to own the command center technology and customize alert logic, escalation pathways, and reporting
- Need to integrate H@H with existing chronic RPM programs (same patient monitored continuously during acute episode, then transitions to chronic RPM post-discharge)
- Timeline: 4-8 months with accelerator-based build
The transition from acute H@H monitoring to chronic RPM post-discharge is an architecture challenge no vendor platform handles well. A patient admitted for heart failure exacerbation receives continuous monitoring during the H@H episode (DRG billing). Upon discharge from the H@H episode, they transition to chronic RPM (CPT billing) with daily weight, BP, and SpO2 monitoring. The platform needs to handle both monitoring modes, both reimbursement models, and the clinical handoff between them.
WearConnect handles the device integration layer across both acute continuous monitoring and chronic intermittent monitoring. PatientWatch provides the real-time command center dashboard architecture. HealthConnect CoPilot manages the EHR integration where H@H documentation meets the same standards as inpatient charting.
What Does a 2026 H@H Launch Look Like?
A 12-month trajectory from waiver application to scaled program.
Phase 1: Foundation (Months 1-3)
- Submit AHCAH waiver application to CMS (or confirm existing waiver is active post-extension)
- Select or build technology platform (continuous monitoring, video, command center)
- Design command center staffing model (internal vs outsourced, 24/7 coverage)
- Identify first qualifying conditions (heart failure and COPD exacerbation are the most common starting points)
- Recruit and train H@H clinical team (command center nurses, visiting RNs, physician oversight)
- First 5-10 patients: carefully selected, close to hospital (30-minute transfer radius), adequate home environment, caregiver available
Phase 2: Calibration (Months 4-6)
- Scale to 20-30 concurrent patients
- Refine in-person visit logistics: route optimization, supply chain, lab specimen handling
- Calibrate continuous monitoring alert thresholds (expect high false alarm rates initially, same pattern as chronic RPM but higher stakes)
- Measure outcomes versus inpatient baseline for same DRGs
- Build the CMS reporting infrastructure (AHCAH data submissions required)
Phase 3: Scale (Months 7-12)
- Scale to 50+ concurrent patients
- Optimize DRG mix: which conditions produce the best margin improvement?
- Build the acute-to-chronic transition pathway (H@H episode → chronic RPM post-discharge, single platform)
- Develop outcomes database for CMS March 2026 data release participation
- Decision point: build or buy the command center? At 50+ patients, internal command center often becomes more cost-effective than outsourced
The waiver runs to 2030. That provides a four-year-plus runway from a 2026 launch to build, iterate, scale, and produce the outcome data that positions the system for whatever permanent H@H program CMS eventually establishes.
The Next Decade of Acute Care Is Being Built Right Now
Four hundred nineteen hospitals across 39 states. Congressional extension to 2030. Thirty-two percent cost savings confirmed by CMS. Non-inferior clinical outcomes across 47 randomized controlled trials. Patient satisfaction above 90%. The data is not ambiguous.
The question for health systems in 2026 is not whether hospital-at-home will become a permanent part of acute care delivery. The question is whether your system builds the technology infrastructure or rents it. Vendor platforms get you started. Owned infrastructure gives you control as the program scales to 50, 100, 200 concurrent patients.
Sandra Elliott’s BRI 2026 finding on AI-powered deterioration prediction (24-48 hours of advance warning before clinical events) is more relevant for hospital-at-home than for any other RPM application. Catching deterioration in a patient at home, not in a hospital bed with a nurse down the hall, requires earlier detection with higher confidence. The AI prediction layer is not optional for hospital-at-home. It is the safety architecture.
The first time someone described hospital-at-home to me, I thought it was a COVID workaround that would disappear when beds reopened. Five years, 419 hospitals, 31,000 patients, and a Congressional extension later, that assumption is thoroughly updated. The waiver is not an experiment anymore. It is a four-year runway to build what comes next.
If your leadership team is evaluating hospital-at-home and the technology architecture conversation hasn’t started yet, that is the first conversation to have. The clinical model, the staffing model, and the financial model all depend on what the technology can support.
The AHCAH waiver, issued by CMS in November 2020, allows hospitals to provide acute inpatient-level care in patients’ homes instead of hospital beds. Patients must meet inpatient admission criteria and be offered the home option. The waiver requires continuous monitoring, 24/7 clinical availability, daily in-person visits, and at least two physician or APP check-ins per day. Congress extended the waiver to September 2030 through H.R. 4313, passed December 2025.
As of September 2025, 419 hospitals across 147 health systems in 39 states are approved for AHCAH. Over 31,000 patients have been served since the program launched. CMS will release detailed outcome data (April 2023 through September 2025) on March 17, 2026. Participation has grown from roughly 50 hospitals in 2020 to 419 in 2025, a trajectory that shows sustained institutional commitment beyond the original pandemic rationale.
Hospital-at-home is reimbursed under MS-DRGs (Diagnosis-Related Groups), the same payment model as traditional inpatient stays. The hospital receives DRG payment for the episode ($5,000-15,000+ depending on condition), not CPT-based monthly RPM billing ($105-220/month). This makes H@H the highest-revenue RPM-adjacent use case by a significant margin. The cost per episode averages $5,081 versus $7,480 for inpatient (32% savings), so the margin improvement per episode can range from $1,000 to $8,000 depending on the DRG.
Eight components: (1) continuous vital sign monitoring every 5-15 minutes, (2) continuous single-lead ECG for cardiac patients, (3) fall detection, (4) HIPAA-compliant video visit platform, (5) 24/7 clinical command center with real-time dashboard, (6) in-person visit logistics (scheduling, supply chain, lab specimen handling), (7) EHR integration where H@H documentation meets inpatient charting standards, (8) patient and family communication platform. This is not a chronic RPM stack with more frequent readings. It is hospital monitoring infrastructure deployed in a home.
A 2024 meta-analysis of 47 RCTs (9,749 patients) showed non-inferiority to hospital care with no significant differences in mortality, readmission, or patient satisfaction. AHRQ data shows 32% cost savings per episode. An early RCT found 7% readmission for H@H versus 23% for inpatient. Patient satisfaction consistently exceeds 90-95% with preference for home care. CMS confirmed lower 30-day Medicare spending for more than half of the top 25 MS-DRGs. The evidence shows H@H matches hospital outcomes at lower cost for qualifying conditions.
AHCAH covers patients who meet inpatient admission criteria and can safely receive care at home. The most common qualifying conditions: heart failure exacerbation, COPD exacerbation, pneumonia, cellulitis, urinary tract infection, and asthma exacerbation. Patients must have an adequate home environment, and the hospital must be able to transfer the patient to inpatient within a safe timeframe if clinical escalation is needed. Elective procedures and complex surgical recovery do not qualify.
Congress extended the AHCAH waiver to September 2030 through H.R. 4313, passed by the House on December 1, 2025. This provides a four-year-plus runway from 2026 for health systems to build, scale, and demonstrate outcomes. CMS has signaled interest in making H@H a permanent program pending sufficient outcome data, and the March 2026 data release covering 2.5 years of patient outcomes will inform that decision.


