



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
Digital quality measures (dQMs) enable hospitals calculate HEDIS and program performance metrics directly from FHIR data rather than manual abstraction. CMS and NCQA are pushing toward a fully digital ecosystem by 2030, making FHIR readiness, CQL-based engines, and workflow integrations essential. This crash course gives CMIOs a practical mapping template, a 90-day pilot plan, and clear guidance on where AI agents and accelerators fit into real operations.
A CMIO-ready crash course on digital quality measures, FHIR mapping, dQM engines, and a 90-day roadmap to modernize quality reporting for 2030.
If NCQA and CMS walked into your office today and asked, “Can your hospital run digital HEDIS measures on FHIR data this year?”, would you feel confident or exposed?
Quality teams are already stretched by chart chase, abstractors, and manual reconciliations. At the same time, CMS is publishing a dQM Strategic Roadmap and building the Universal Foundation, while NCQA is turning HEDIS into digital content that runs on FHIR and CQL.
In this crash course, we walk through what dQMs really are, why the 2030 timeline matters, what a FHIR-based architecture looks like in an Epic or Cerner environment, and how to de-risk the transition using accelerators like AI Medical Summary, HealthConnect CoPilot, CarePlan AI, RPMCheck AI, and AI Readmission Risk.
I. What exactly are digital quality measures?
Digital quality measures are not just “eCQMs with nicer specs.” CMS defines dQMs as quality measures that use standardized digital data from one or more health information sources, captured and exchanged via interoperable systems, and computed using standards-based measure specs without extra manual effort.
NCQA extends this for HEDIS. Its digital HEDIS content is expressed in Clinical Quality Language (CQL) and Fast Healthcare Interoperability Resources (FHIR).
This lets health plans and providers exchange measure logic and results using the same interoperability stack they are already building for other use cases.
For a CMIO, this means three concrete things:
- Your EHR and data warehouse must expose the right FHIR resources at a usable quality.
- You need a measure engine that understands NCQA dQM content and CMS dQM specs.
- You can stop treating HEDIS and internal quality measures as one-off builds and start treating them as code you can version, test, and automate.
II. Why are CMS and NCQA pushing everyone to dQMs by 2030?
CMS published a Digital Quality Measurement Strategic Roadmap that sets a clear direction. It calls for transitioning all quality measures in CMS programs to dQMs and highlights interoperability and standardized digital data as the foundation for this transition.
In parallel, NCQA is turning HEDIS into digital content. Its Digital Quality Overview and resource directory show how digital measures will leverage FHIR APIs, code packages, and CQL engines to generate scores and submission files.
Industry checklists from organizations like Inovalon and others make the timeline explicit. They describe a transformation where HEDIS measurement becomes fully digital by 2030 and warn that many payers and providers still do not feel ready.
For your value-based programs, this shift is not optional because:
- Medicare Advantage Star Ratings and Medicaid Core Sets are aligning with digital measurement models.
- CMS Universal Foundation measures are meant to span programs, which makes reusable digital content much more attractive than bespoke builds.
III. Where will dQMs show up in your world as a CMIO?
For a CMIO in a mid-market hospital, dQMs will touch at least four domains:
- Regulatory reporting
- Medicare Advantage and commercial contracts that reference HEDIS will increasingly expect digital HEDIS content and FHIR-based feeds.
- Medicaid Child, Adult, and Health Home Core Sets are already introducing electronic clinical data system specifications.
- Value-based care contracts
- Many shared-savings and downside-risk contracts incorporate HEDIS measures or related quality composites.
- As CMS and NCQA modernize the measurement layer, your quality scores and settlement calculations will rely on digital calculations rather than manual abstraction.
- Internal quality and safety programs
- Once you have FHIR-based measures running for external programs, internal measures like sepsis bundles or discharge follow-up can ride the same architecture.
- Data products and AI agents
- dQM logic becomes a reusable service. It can feed AI agents that help nurses close care gaps, risk adjusters validate documentation, and care managers prioritize outreach.
This is where Mindbowser’s accelerators become practical. AI Medical Summary can normalize inconsistent clinical documentation, and HealthConnect CoPilot can surface dQM-driven gaps directly within provider workflows, rather than in a separate portal.
IV. What does a FHIR-based dQM architecture look like?
You can think of a digital HEDIS stack in four layers.
1. Source systems and FHIR layer
- EHR systems such as Epic and Cerner expose FHIR resources, including Patient, Encounter, Condition, Observation, MedicationRequest, and Procedure.
- External data sources, such as labs, HIEs, RPM platforms, and SDOH tools, provide additional FHIR resources and observations.
2. Data quality and normalization
- Data is profiled and cleaned so that the right codes and value sets appear where dQM logic expects them.
- AI Medical Summary can help normalize diagnoses, medications, and histories into structured fields that align with dQM value sets.
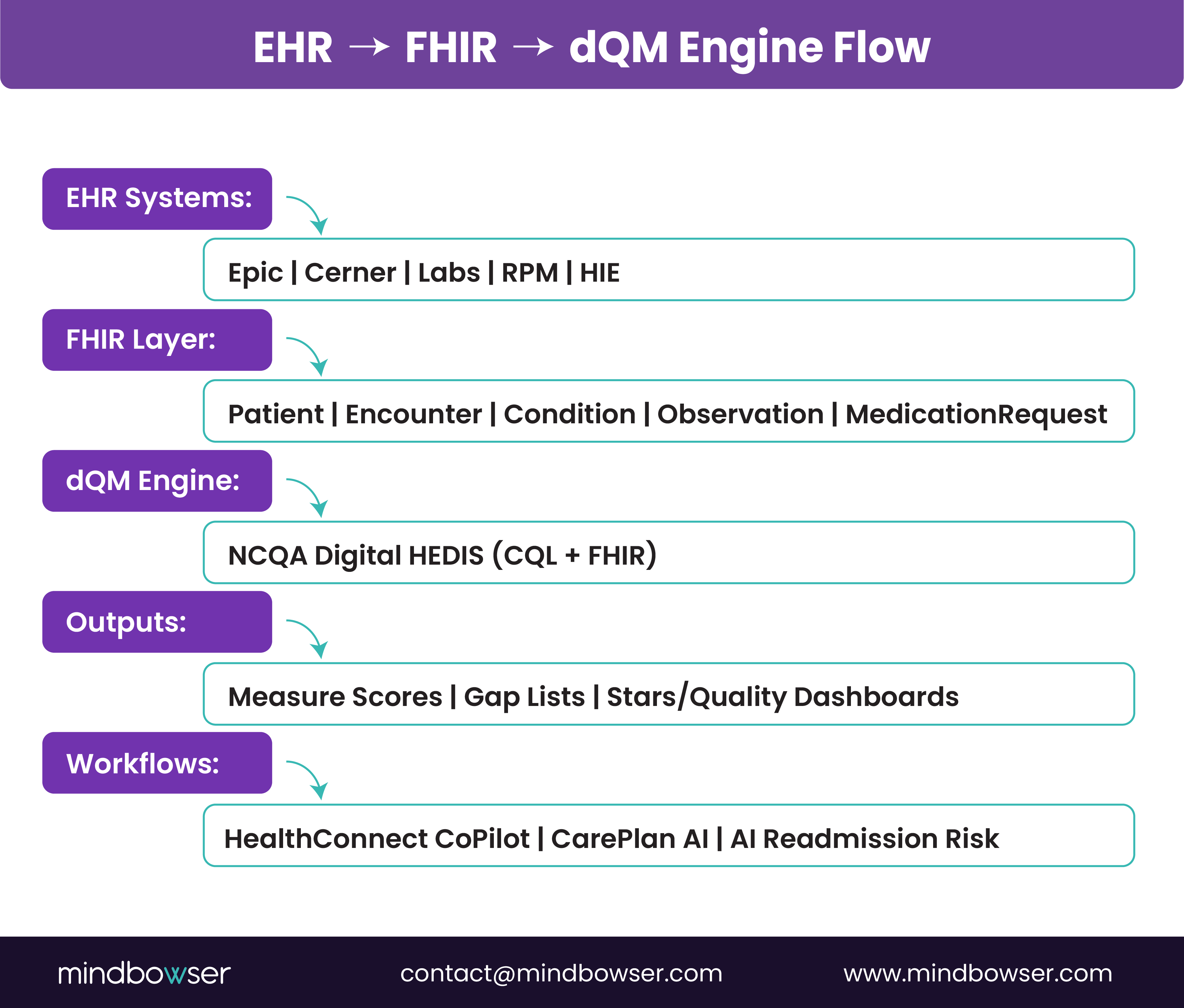
3. dQM engine and content
- NCQA Digital Content Services or similar vendors deliver HEDIS digital content in FHIR CQL format, backed by open source engine requirements.
- A dQM engine runs this content against your FHIR data and produces measure-level results and patient-level gap lists.
4. Clinical and quality workflows
- Quality dashboards and Stars or HEDIS scorecards consume measure results.
- HealthConnect CoPilot, CarePlan AI, and AI Readmission Risk use the same dQM outputs to queue outreach tasks, update care plans, and guide clinicians at the point of care.
Mini FHIR mapping template example
For a blood pressure control measure, your dQM implementation team would map:
- EHR blood pressure flowsheet rows to Observation resources with the right LOINC codes.
- Problem list codes to Condition resources that identify hypertension cohorts.
- Medication lists to MedicationRequest resources that identify appropriate therapies.
You can reuse this template pattern across many measures and contracts.
V. How do you get from eCQMs to dQMs without breaking your reporting year?
Most CMIOs cannot pause quality reporting for a platform rewrite. The safer pattern is a phased transition that runs eCQMs and dQMs in parallel.
A practical 90-day plan, adapted from NCQA and implementation checklists, looks like this.
Days 0 to 30: Assess and align
- Inventory of which external programs you participate in and which measures have digital content available.
- Map those measures to your current eCQM stack and internal definitions.
- Stand up a small FHIR data mart that covers one or two priority measures.
Days 31 to 60: Build and test
- Implement FHIR mappings for a handful of critical resources for your pilot measures.
- Deploy a dQM engine in a non-production environment and load NCQA digital content where applicable.
- Use AI Medical Summary to clean and standardize documentation for the pilot cohort.
Days 61 to 90: Compare and harden
- Run eCQMs and dQMs side by side for the pilot measures.
- Investigate discrepancies with your quality and clinical leaders.
- Use HealthConnect CoPilot and CarePlan AI to test how patient-level gaps will appear inside workflows.
By the end of this cycle, you will have one or two measures running digitally with known variance vs. legacy flows, which will be enough to present a clear roadmap to your CFO and CMO.
Assess Your FHIR Readiness
VI. How do dQMs connect to AI agents and clinical workflows?
Once your measures live as code that runs on FHIR data, they become a powerful trigger surface for AI and automation.
A few concrete patterns:
- Care gap agents
- Use measure gap lists to trigger HealthConnect CoPilot tasks such as scheduling visits, ordering labs, or updating care plans.
- Align outreach sequences to the same logic that drives your Stars or HEDIS scores.
- Risk and readmission agents
- Combine dQM cohort definitions with AI Readmission Risk so that high-risk patients in critical measures receive extra post-discharge support.
- RPM and remote care agents
- Use RPMCheck AI to validate remote vitals and confirm they meet dQM data requirements before they are included in calculations.
Because dQMs run on the same FHIR APIs that your AI workloads use, you do not need to bolt on a separate data pipeline. You can orchestrate quality, risk, and outreach from a single shared source of truth.
VII. Build versus buy: What should your hospital own in the dQM stack?
Most mid-market providers do not want to build their own dQM engine from scratch. At the same time, you cannot outsource everything because you must own your data and quality definitions.
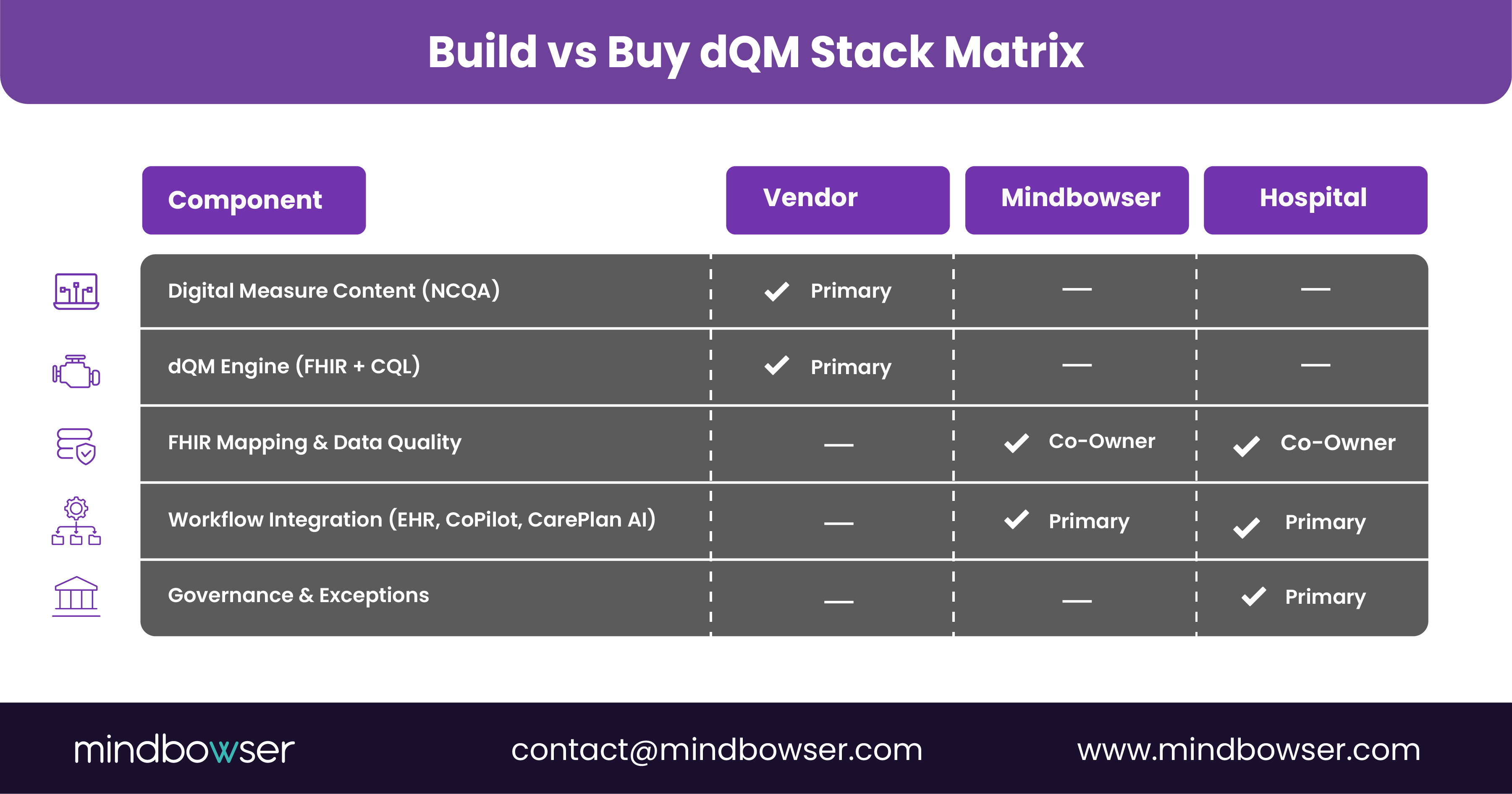
A balanced pattern looks like this:
- Buy or license
- NCQA digital content for HEDIS measures, where available or similar vendor content.
- A dQM engine that supports FHIR, CQL, and NCQA digital content updates.
- Build with a partner
- FHIR mapping and data quality pipelines that are specific to your mix of EHRs, RPM tools, SDOH platforms, and claims feeds.
- Integration of gap lists and measure scores into your existing quality dashboards and EHR workflows, backed by accelerators like HealthConnect CoPilot and AI Medical Summary.
- Own internally
- Governance of measure selection, override rules, and exception handling.
- Clinical review of measure logic and AI assistant behavior.
Mindbowser’s role is to sit on the “build with a partner” line. We connect your source systems to standards-based content and then wire the results into practical, clinician-friendly experiences.
What should you do in the next 90 days?
If you are a CMIO responsible for quality and digital strategy, a realistic 90-day objective is not “go fully digital.” It is “prove that two priority measures can run as dQMs on real FHIR data.”
You can do this by:
- Select two measures that matter for your largest contracts and that have digital content available.
- Standing up a small FHIR-based data mart that includes the resources those measures require.
- Running a dQM engine in parallel with your current eCQM or hybrid process and comparing results.
- Using accelerators like AI Medical Summary, HealthConnect CoPilot, and CarePlan AI to show how gaps surface in daily workflows instead of in spreadsheets.
Once this pilot proves value, you can expand to additional measures and programs and build a multi-year roadmap that aligns with CMS and NCQA timelines.
Digital quality measures are CMS and NCQA-defined measures that run on standardized FHIR data and computable CQL specifications. They replace manual chart review and legacy eCQMs with automated, interoperable calculations using data pulled directly from EHRs and other electronic sources.
eCQMs rely on limited structured data and rigid formats. dQMs use FHIR APIs, value sets, and CQL logic, making them more flexible, multi-source, and easier to automate. CMS and NCQA are transitioning to fully digital measurement to reduce errors and improve timeliness.
CMS’s Digital Quality Measurement Strategic Roadmap and NCQA’s digital HEDIS transition signal that by 2030, most quality programs will require dQMs. Hospitals need FHIR-ready data, a compliant dQM engine, and workflows that can consume digital gap lists to stay aligned with Stars, Medicaid Core Sets, and VBC incentives.
Hospitals need:
- EHR and data-warehouse FHIR APIs;
- Data-quality pipelines aligned to dQM value sets;
- A CQL-aware dQM engine;
- Workflow integrations that surface gaps to clinicians.
This ensures measures run on clean, computable data and feed real-time quality actions.
dQMs calculate quality scores using standardized digital data, enabling more accurate Stars performance, fewer manual abstractions, and faster gap closure. They align multiple contracts around a single digital measure set, improving VBC settlement predictability.
Not always. Many vendors are modernizing to support NCQA’s digital HEDIS content and FHIR inputs. Hospitals mainly need a partner to map EHR data to FHIR and integrate digital measure outputs into clinical workflows. The vendor engine can often remain in place if it supports NCQA digital content updates.


