











































TL;DR
Not all clinical decision support system features improve outcomes; many simply add noise. High-performing CDSS drives value by delivering context-aware, actionable guidance within clinical workflows, reducing alert fatigue, and integrating seamlessly with EHR systems. The real impact comes from combining workflow alignment, predictive intelligence, and strong governance, turning CDSS from a compliance tool into a measurable asset under value-based care.
I. Introduction
“What happens when your CDSS fires 300 alerts a day, and clinicians ignore most of them?”
This isn’t edge-case behavior. It’s standard across many health systems.
Clinical decision support is no longer optional. Under value-based care, every missed intervention, delayed diagnosis, or unnecessary admission directly impacts reimbursement, quality scores, and operating margin.
“Up to 90% of clinical alerts are overridden by clinicians.” AHRQ
That stat isn’t about clinician behavior. It’s about system design.
Most organizations still rely on basic clinical decision support software that was built for compliance, not performance:
- Static rules
- Poorly timed alerts
- Minimal personalization
- Weak EHR integration
The result?
Interruptions instead of insights. Noise instead of guidance.
And clinicians respond the only way they can. They override.
Not all CDSS features improve care; many simply increase clicks.
At the same time, expectations have changed.
Modern health systems need advanced clinical decision support that:
- Predicts risk before it escalates
- Recommends next-best actions in real time
- Aligns with clinical workflows, not against them
Because in a VBC model, timing matters. Context matters. Adoption matters.
Now the real question becomes:
- Which clinical decision support system features actually move the needle on outcomes, cost, and clinician efficiency?
- That’s where we start.
Before diving in, it’s important to distinguish between CDSS features, types, and benefits.
- Features define what the system can do (e.g., risk prediction, workflow integration).
- Types describe how the system is built (rule-based, AI-driven, passive vs active).
- Benefits reflect the outcomes achieved (reduced errors, improved quality scores, lower costs).
This guide focuses specifically on the features that directly influence adoption, outcomes, and scalability.
II. Why Clinical Decision Support Must Evolve in a Value-Based Care Era
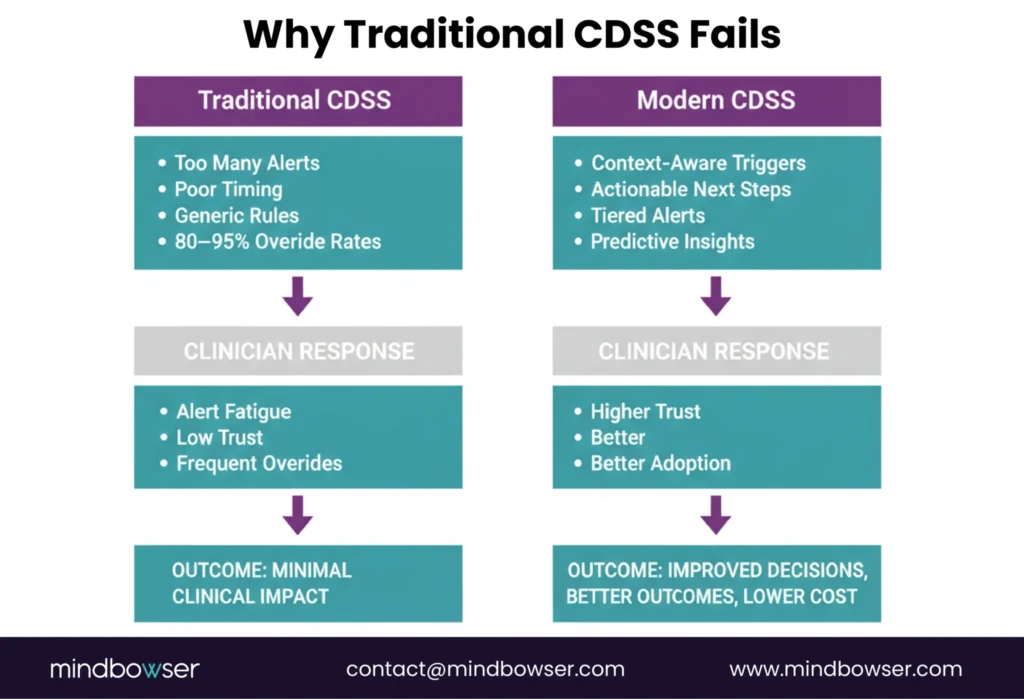
Not all alerts are created equal. Most aren’t even helpful.
So why do they still dominate CDSS design?
Traditional systems were built on rule-based logic. If X happens, trigger Y alert. Simple. Predictable. Easy to implement.
Also, easy to ignore.
This is the core failure.
Not a lack of data. Not a lack of features.
Lack of intelligence at the point of care.
Modern healthcare decision support software must evolve from static alerts to dynamic, context-aware guidance that fits inside clinical workflows.
Let’s break that down.
A. The Shift from Alerts to Intelligence
Why do clinicians ignore the very systems designed to help them?
Most clinical decision support software still behaves like a rule engine rather than a thinking partner.
Legacy CDSS was built on a simple premise: detect an event, fire an alert. Drug interaction? Alert. Abnormal lab? Alert. Missing documentation? Alert.
On paper, that sounds safe.
In practice, it creates overload.
That’s not a usability issue. It’s a design failure.
The problem isn’t alerts. It’s timing, context, and actionability.
Let’s break the gap:
- Basic CDS: Fires alerts after a decision path has started
- Advanced CDS: Intervenes before risk escalates
- Basic CDS: Presents information
- Advanced CDS: Recommends next-best actions
- Basic CDS: Treats all users the same
- Advanced CDS: Adapts to role, specialty, and patient context
One interrupts. The other guides.
Consider a real scenario.
A physician is ordering medications during rounds. A drug interaction alert fires. It’s clinically valid, but not urgent. The physician overrides it. Not out of negligence, but necessity. Time pressure wins.
Now contrast that with advanced clinical decision support:
- Before the order is placed, the system flags a high-risk patient profile, suggests an alternative medication, and aligns with the formulary and the patient’s history. No interruption. Just direction. (Relief replaces friction.)
- This works. Period.
The shift is clear:
- From reactive alerts to proactive intelligence
- From generic rules to context-aware recommendations
- From system-centered design to workflow-centered design
- And this is where outcomes change.
“Effective CDS interventions can reduce medication errors by up to 55%.” Journal of the American Medical Informatics Association
That’s not incremental improvement. That’s operational impact.
If your CDSS only alerts, it’s already outdated. The future belongs to systems that think ahead, act in context, and guide decisions when they still matter.
B. Executive Expectations in 2026
What does a CIO actually expect from clinical decision support today?
Not alerts. Not dashboards. Outcomes.
The conversation has shifted from feature availability to measurable performance across cost, quality, and workflow efficiency.
Each executive stakeholder now evaluates clinical decision support system features through a different lens:
CIOs are asking:
Can this system integrate cleanly with Epic or Cerner?
Will it reduce clinician burden or add to it?
Does it scale across service lines without breaking workflows?
Because for them, CDSS is an infrastructure decision. If it slows systems down, adoption dies.
CMIOs are focused on clinical credibility:
- Are recommendations evidence-based and current?
- Do clinicians trust the system?
- Does it improve adherence without forcing behavior?
Trust is everything here.
No trust, no usage. No usage, no outcomes.
CFOs, on the other hand, are blunt:
Where is the ROI?
- Does CDSS reduce readmissions?
- Can it lower avoidable utilization?
- Does it improve quality scores tied to reimbursement?
Because in a VBC model, CDSS is no longer a clinical tool. It’s a financial lever.
“The difference between CDSS success and failure isn’t deployment, it’s measurable impact.”
Now layer this together.
Executives are no longer impressed by feature lists. They expect:
- Workflow alignment across roles
- Outcome visibility tied to interventions
- Operational efficiency at scale
Three priorities. One system.
Miss one, and the entire investment underperforms.
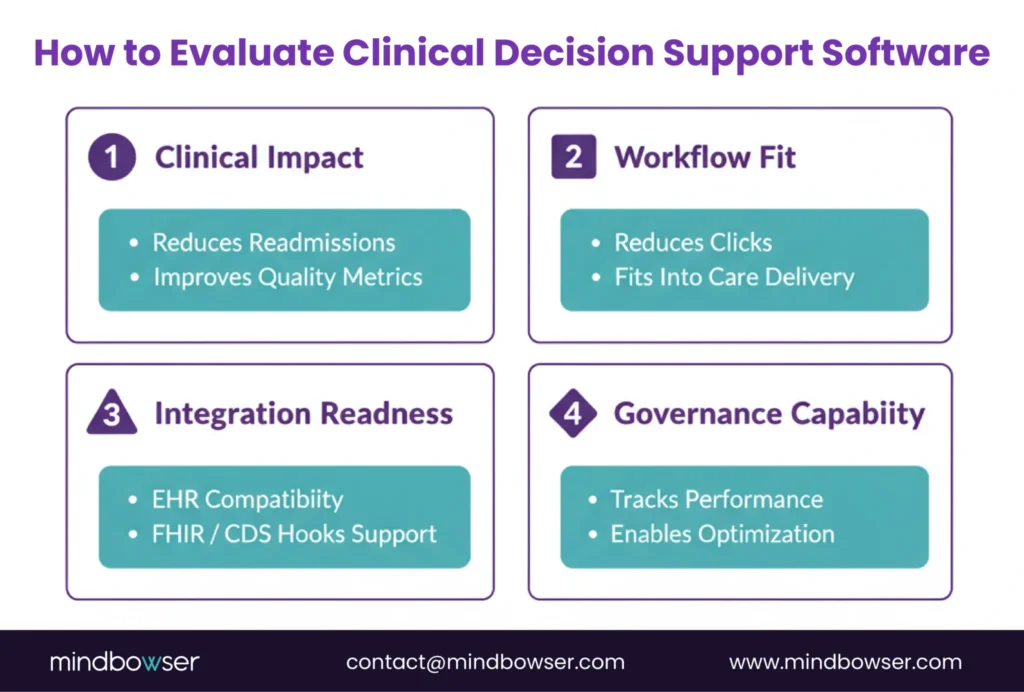
C. What Defines High-Performance Healthcare Decision Support Software
So what actually separates high-performing CDSS from everything else?
It’s not the number of features. It’s how those features behave inside real clinical environments.
Four capabilities define modern, high-impact healthcare decision support software:
1. Workflow Timing
The best systems don’t interrupt. They intervene at the right moment.
- Before orders are placed
- During decision windows
- Within existing clinical flows
Too early, it’s ignored. Too late, it’s irrelevant.
2. Evidence Integrity
Clinicians don’t just want recommendations. They want to know why.
- Source-backed guidelines
- Transparent logic
- Regular updates aligned with clinical standards
Because when evidence is visible, adoption follows.
3. Measurable Outcomes
If you can’t track impact, you can’t justify the system.
High-performing CDSS ties interventions to:
- Reduced readmissions
- Improved guideline adherence
- Lower medication errors
4. Interoperability
This is non-negotiable.
- Seamless EHR integration
- Data liquidity across systems
- Standards like FHIR and CDS Hooks
Without this, even the best advanced clinical decision support system becomes shelfware.
For a deeper dive into how CDSS supports modern healthcare delivery, explore this blog.
High-performance CDSS doesn’t sit on top of workflows. It lives inside them, learns from them, and improves them over time.
III. 10 Clinical Decision Support System Features That Drive Real Outcomes
What separates a CDSS that gets ignored from one that actually changes clinical decisions?
It comes down to how features are layered across adoption, intelligence, and infrastructure.
Not all clinical decision support system features operate at the same level. Some drive usage. Others drive outcomes. A few determine whether the system survives at scale.
The mistake most organizations make is evaluating features in isolation instead of how they perform together.
Let’s break this into three layers that matter in real-world deployments.
A. Workflow-Driven Features (Adoption Layer)
If clinicians don’t use it, nothing else matters.
This is where most CDSS implementations fail. Not because the logic is wrong, but because the experience disrupts care delivery instead of supporting it.
These features determine whether your system gets adopted or overridden.
1. Context-Aware Triggering
When should a CDSS intervene?
Timing is everything.
Basic systems trigger alerts based on static rules. Advanced systems evaluate clinical context in real time:
- Patient condition
- Care setting (ED, inpatient, outpatient)
- Provider role
- Current workflow stage
Instead of firing after an order is placed, the system intervenes during the decision window.
Too early is noise. Too late is useless.
Key insight: Context-aware triggering reduces unnecessary interruptions while increasing relevance.
2. Actionable Next-Best Recommendations
What should the clinician do next?
This is where most clinical decision support software falls short.
Instead of simply flagging an issue, high-performing systems:
- Recommend alternative treatments
- Suggest next diagnostic steps
- Align with clinical guidelines and patient history
No information. Direction.
A system that says “there’s a problem” creates friction.
A system that says “here’s what to do next” creates value.
3. Tiered Alerting and Noise Suppression
Does every alert deserve equal attention?
Clearly not.
High-performing CDSS introduces tiered alerting models:
- High-severity alerts that require immediate action
- Medium-level suggestions that guide decisions
- Low-priority notifications that stay passive
This dramatically reduces alert fatigue, one of the biggest barriers to adoption.
Noise suppression isn’t a nice-to-have. It’s survival.
4. Role-Based Personalization
Should a nurse, physician, and care manager see the same alert?
They shouldn’t.
Advanced CDSS tailors recommendations based on:
- Clinical role
- Specialty
- Experience level
- Care responsibilities
A cardiologist doesn’t need the same prompts as a primary care physician.
Personalization drives relevance. Relevance drives trust. Trust drives adoption.
5. Embedded Clinical Rationale and Transparency
Why should a clinician trust this recommendation?
Because they can see the logic behind it.
High-performing systems embed:
- Guideline references
- Evidence summaries
- Patient-specific reasoning
Not buried in links. Right inside the workflow.
When clinicians understand the “why,” resistance drops.
These workflow-driven features determine whether your CDSS is used or ignored. Get this layer wrong, and nothing else matters.
B. Clinical Intelligence Features (Outcome Layer)
Adoption is step one. But does your CDSS actually improve outcomes?
This is where most systems stall.
They get used. They generate alerts. But they don’t change risk trajectories, reduce utilization, or improve quality scores.
That requires a different class of capability.
Clinical intelligence features move CDSS from reactive support to proactive decision orchestration.
1. Evidence and Guideline Lifecycle Management
How current is your clinical logic?
Outdated guidelines are a silent risk.
High-performing healthcare decision support software continuously manages:
- Clinical guidelines (CMS, USPSTF, specialty bodies)
- Version control and updates
- Local protocol alignment
This ensures recommendations are not just evidence-based, but current and contextually relevant.
Without lifecycle management, even accurate systems drift into irrelevance.
Key insight: Static knowledge degrades. Dynamic evidence sustains trust.
2. Risk Stratification and Predictive Modeling
What if your CDSS could act before a patient deteriorates?
This is the turning point.
Instead of reacting to events, advanced clinical decision support systems:
- Identify high-risk patients early
- Predict readmissions, sepsis, or deterioration
- Prioritize interventions based on risk scores
For example:
- Flagging a patient with rising sepsis risk hours before symptoms escalate
- Identifying patients likely to miss follow-ups or medications
- Stratifying populations for care management outreach
This is where CDSS begins to influence population health outcomes, not just individual encounters.
3. Care Pathway Orchestration and Order Set Integration
What happens after a recommendation is accepted?
In many systems, nothing. The clinician still has to figure out the next steps manually.
That’s friction.
High-performing CDSS connects recommendations directly to care execution:
- Pre-configured order sets
- Evidence-aligned care pathways
- Automated task routing across teams
Instead of stopping at insight, the system guides the entire care journey.
Think about a congestive heart failure patient:
- Risk identified →
- Guideline-based pathway triggered →
- Medications, labs, follow-ups pre-aligned →
- Care team notified
No gaps. No guesswork.
Decision → action → outcome.
For real-world implementations of these capabilities, explore this blog.
Clinical intelligence features don’t just support decisions. They shape outcomes at scale by predicting risk, aligning care, and ensuring every action follows evidence.
C. Enterprise-Grade Infrastructure Features (Scalability Layer)
Even if your CDSS works in one department, can it scale across the enterprise?
This is where many promising implementations fail.
They perform well in pilots. Then break under real-world complexity.
Why?
Because infrastructure determines sustainability.
Without the right foundation, even the best clinical decision support system features won’t survive across service lines, data environments, and regulatory demands.
1. Standards-Based Interoperability
Can your CDSS talk to the rest of your ecosystem, or does it sit in a silo?
Modern healthcare decision support software must integrate seamlessly across:
- EHR systems (Epic, Cerner)
- Data platforms
- Third-party applications
This is where standards matter:
- SMART on FHIR enables embedded apps within EHR workflows
- CDS Hooks allows real-time decision support at clinical trigger points
- Terminology alignment ensures consistency across SNOMED, LOINC, and ICD
Without these, integration becomes brittle. Maintenance costs rise. Adoption drops.
If data doesn’t flow, decisions stall.
Key insight: Interoperability isn’t technical plumbing. It’s what makes real-time decision support possible.
2. Governance, Auditability, and Performance Analytics
Who owns your CDSS logic, and how do you know it’s working?
This is the most overlooked layer.
High-performing systems include built-in governance models that track:
- Alert overrides and acceptance rates
- Clinical outcomes tied to interventions
- Bias and performance drift in predictive models
Because CDSS is not “set it and forget it.”
It evolves.
Governance answers critical questions:
- Which alerts are ignored and why?
- Which pathways improve outcomes?
- Where is the system introducing bias or inefficiency?
This is where CFO and CMIO priorities converge.
Clinical quality meets financial accountability.
One system. Three layers. Real impact.
- Workflow features drive adoption
- Intelligence features drive outcomes
- Infrastructure features drive scale
Miss one layer, and performance collapses.
Enterprise-grade CDSS isn’t just about what the system does. It’s about how reliably it performs across environments, teams, and time.
Ready to Build Clinical Decision Support That Drives Measurable Outcomes?
IV. How Mindbowser Can Help
What does it take to move from CDSS experimentation to measurable enterprise impact?
Not a vendor. A partner who understands clinical workflows, data architecture, and VBC economics all at once.
That’s where Mindbowser operates.
Built on a custom-development-first approach with HIPAA and SOC 2 alignment by design, Mindbowser focuses on turning clinical decision support system features into real-world performance gains, not shelfware.
A. VBC-Aligned CDSS Strategy
Before building anything, do you know which decisions actually drive value?
Most organizations don’t.
Mindbowser starts with workflow and outcome discovery:
- Mapping high-impact clinical decision points
- Aligning CDS interventions to VBC metrics (readmissions, quality scores, utilization)
- Identifying gaps between current workflows and desired outcomes
This ensures CDSS isn’t deployed broadly; it’s deployed where it matters most.
“CDSS without outcome alignment becomes a reporting tool, not a performance engine.”
Key outcome: Every CDS intervention ties back to measurable financial and clinical impact.
B. Engineering and Integration
Can your CDSS actually function inside your existing ecosystem without disruption?
That’s where most implementations break.
Mindbowser builds advanced clinical decision support systems that integrate directly into care delivery environments:
- SMART on FHIR applications embedded within EHR workflows
- CDS Hooks-based triggers for real-time interventions
- Predictive models tailored to patient populations and use cases
No rigid templates. No forced workflows.
Everything is custom-built to fit your clinical and technical environment, ensuring:
- Minimal disruption
- Faster clinician adoption
- Reliable system performance
And because accelerators are pre-built, solutions can launch up to 40% faster while maintaining full customization.
C. Optimization and ROI Instrumentation
How do you prove your CDSS is actually working?
Through continuous measurement and refinement.
Mindbowser implements governance and analytics layers that track:
- Alert acceptance and override rates
- Clinical outcomes tied to CDS interventions
- Workflow efficiency improvements
Then optimizes:
- Reducing unnecessary alerts
- Improving recommendation accuracy
- Adjusting models to prevent drift or bias
This transforms CDSS from a static system into a continuously improving performance engine.
CDSS is not a one-time deployment. It’s a system that learns, adapts, and improves over time.
Mindbowser doesn’t just implement CDSS. It builds systems that clinicians use, executives trust, and CFOs can measure.
From Features to Outcomes: Making CDSS a Strategic Asset
Clinical decision support is no longer about deploying alerts; it’s about driving decisions that improve outcomes, reduce cost, and scale across the enterprise. Health systems that succeed are not the ones with the most features, but the ones with the right clinical decision support system features aligned to workflow, intelligence, and infrastructure. When adoption, predictive insight, and governance work together, CDSS becomes a measurable performance engine across VBC metrics. When they don’t, it becomes noise. For CIOs, CMIOs, and CFOs alike, the mandate is clear: treat CDSS as a strategic asset, not a compliance layer, and invest in features that clinicians trust, systems can support, and finance teams can measure.
The most impactful features are context-aware triggering, actionable recommendations, predictive risk modeling, and interoperability. These directly influence clinician behavior and outcomes, not just alert volume.
Basic systems rely on static alerts, while advanced clinical decision support uses real-time data, predictive analytics, and workflow-aware interventions. The difference is proactive guidance versus reactive notifications.
By using tiered alerting, context-aware triggers, and noise suppression, modern CDSS ensures only high-relevance alerts surface. This reduces unnecessary interruptions and improves clinician trust.
Yes, modern CDSS integrates using FHIR, CDS Hooks, and SMART on FHIR, allowing seamless embedding into EHR workflows without disrupting clinician experience.
ROI is measured through reduced readmissions, improved guideline adherence, lower medication errors, and better utilization management, all tied directly to reimbursement and cost savings.
![5 Types of Clinical Decision Support Systems: Which One Fits Your Hospital? [2026]](https://www.mindbowser.com/wp-content/uploads/2026/03/medical-technology-network-telemedicine-health-insurance-virtual-hospital-healthcare-1024x585.jpg.webp)

