



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
- Care team workflow is the limiting factor behind many stalled digital health and operational initiatives.
- Most healthcare organizations digitize tasks without redesigning how work moves across teams, creating hidden friction.
- Fragmented workflows force clinicians and care teams to rely on manual coordination, workarounds, and parallel systems.
- As programs scale, these inefficiencies compound, impacting adoption, cost, and clinical reliability.
- Workflow-first design enables digital initiatives to move from pilots to sustainable operations.
Why does care team workflow break down in healthcare organizations?
Because most healthcare organizations digitize tasks, not workflows.
Over the past decade, health systems and digital health teams have invested heavily in EHRs, point solutions, and automation tools. Yet care teams still coordinate work through inboxes, meetings, and manual follow-ups. The technology exists, but the way work moves across people, systems, and decisions remains fragmented.
Care team workflow breaks down when responsibility is distributed across roles without a shared operational model. Tasks get completed, but handoffs fail. Context is lost between systems. Coordination becomes dependent on individual effort rather than on system design.
As organizations scale digital initiatives, these cracks widen. What works for a small team or pilot begins to stall under real clinical volume, not because teams resist change, but because workflows were never designed to absorb complexity.
This is why care team workflow isn’t an operational detail.
It’s the structural layer that determines whether digital health initiatives scale quietly or plateau.
I. How Fragmented Care Team Workflows Limit Scale and Adoption
Fragmented workflows don’t fail loudly. They fail gradually by adding friction at every handoff.
In most healthcare organizations, care teams span clinicians, care managers, coordinators, and operational staff. Each role may be supported by technology, but the workflow across roles is rarely designed end-to-end. As a result, coordination depends on memory, messaging, and manual tracking.
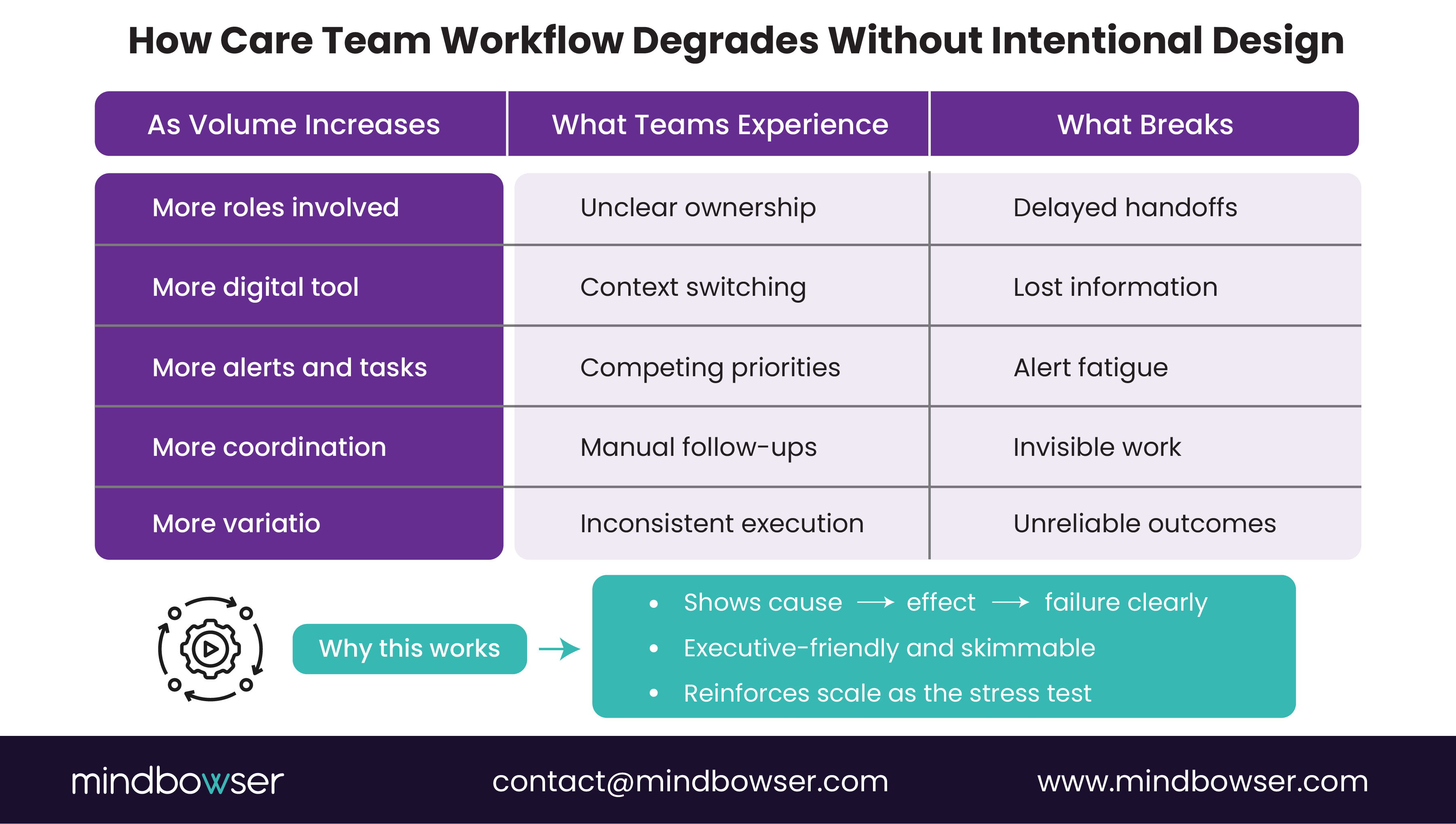
Where Fragmentation Shows Up First
Workflow fragmentation typically surfaces in a few predictable ways:
- Unclear ownership at handoffs
Tasks are often moved between teams without clear ownership or timelines, resulting in increased delays and rework. - Parallel systems of record
Care teams document in multiple tools, forcing manual reconciliation and context switching. - Invisible work
Follow-ups, coordination, and exception handling happen outside formal systems, making effort hard to measure or improve. - Inconsistent execution across teams
Similar care scenarios are handled differently depending on who is involved, reducing reliability.
These issues don’t prevent work from getting done, but they make it harder to repeat consistently.
Why Scale Amplifies Workflow Gaps
At low volume, teams compensate by drawing on experience and extra effort. At scale, those same gaps turn into bottlenecks:
- More coordination overhead per patient
- Slower response times and missed follow-ups.
- Lower adoption of new tools as complexity increases
- Leadership blind spots around where time and effort are actually spent
Digital initiatives stall not because teams lack tools, but because workflows weren’t designed to scale across people and systems.
Transform Disconnected Tasks into Structured, Accountable Care Team Workflows
II. Why Digitizing Tasks Doesn’t Fix the Care Team Workflow
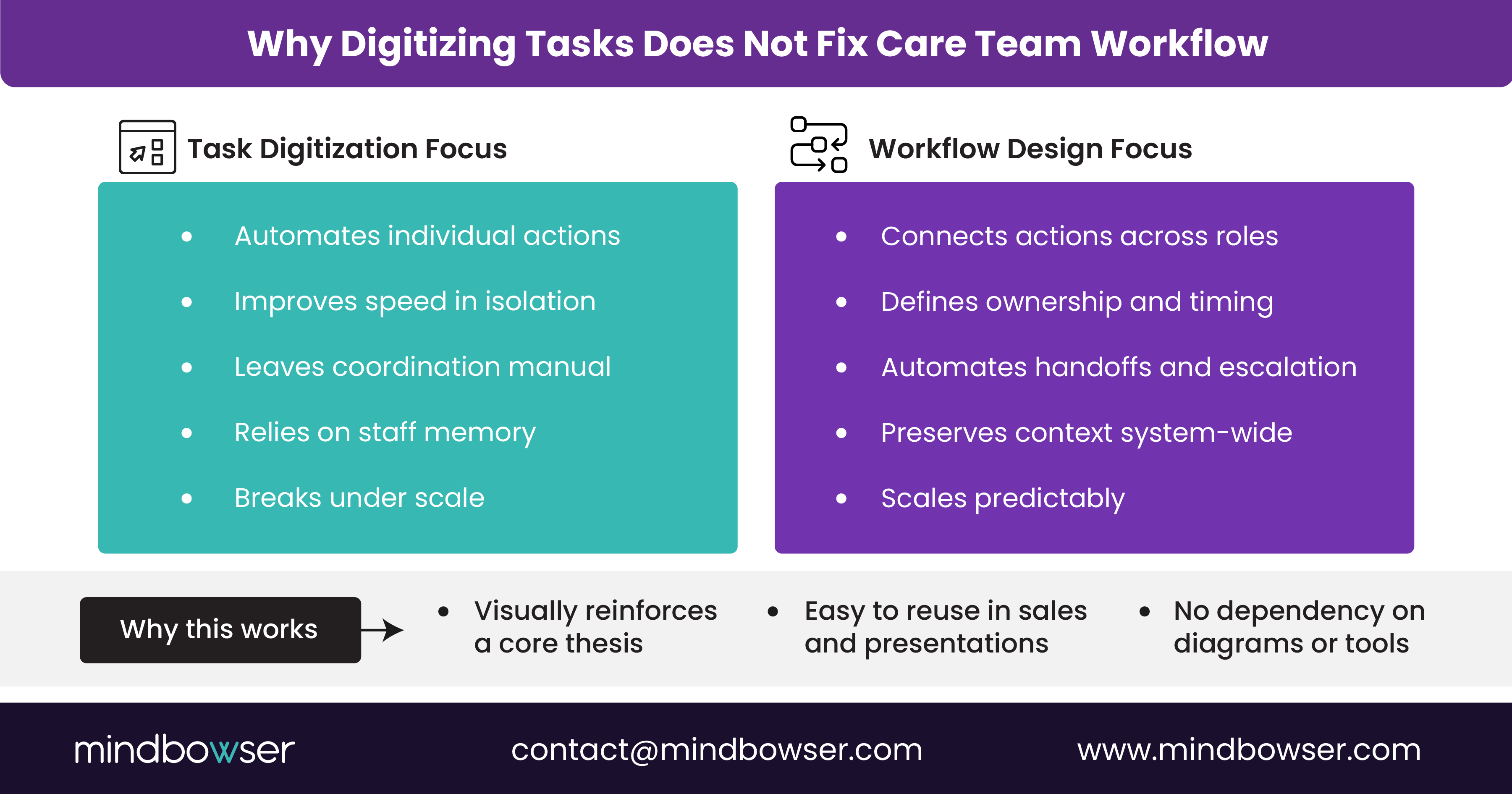
Digitization is often mistaken for workflow design.
Many healthcare organizations deploy tools that streamline individual tasks, such as documenting notes, sending messages, and generating alerts. But when a shared workflow doesn’t connect those tasks, teams still rely on manual coordination to move work forward.
Task Efficiency Vs Workflow Effectiveness
Task-level improvements answer questions like:
- How fast can a note be written?
- How quickly can a message be sent?
- How easily can data be viewed?
Workflow effectiveness answers different questions:
- Who owns the next action?
- What triggers escalation?
- How is context preserved across handoffs?
- When should a human intervene versus the system?
Without those answers embedded in the system, care teams are left to decide in real time every time.
The Hidden Cost of “Tool-first” Design
When tools are layered without workflow logic:
- Alerts compete for attention without prioritization
- Messages lack a clinical or operational context
- Care coordination shifts to side channels
- Teams create personal workarounds to stay afloat
Over time, this increases cognitive load and reduces trust in digital systems. Adoption suffers not because tools are poorly built, but because they don’t reflect how care actually moves.
What Actually Changes Outcomes
Organizations that see sustained impact treat workflow as a first-class design problem. They define how work should flow across roles before selecting or configuring technology. Tools then reinforce the workflow rather than replace it.
This distinction is what separates digitized care from coordinated care.
III. What An Effective Care Team Workflow Looks Like at Scale
Effective care team workflows don’t eliminate complexity. They contain it.
At scale, healthcare delivery involves multiple roles, systems, and decisions. High-performing organizations design workflows that absorb this complexity without pushing it back onto individuals.
Characteristics of Scalable Care Team Workflows
Across mature healthcare operations, effective workflows share common traits:
- Clear ownership at every step
Each action has a defined owner, timing, and expected outcome, reducing ambiguity at handoffs. - System-driven coordination
Work progresses based on rules and triggers, not on memory or manual follow-up. - Context preserved across roles
Clinical and operational context travels with the task, minimizing rework and miscommunication. - Exception-based intervention
Teams focus on outliers and risk, while the system handles routine coordination. - Consistent execution across teams
Similar scenarios are handled the same way, regardless of who is on shift.
These workflows don’t feel rigid to care teams. They feel reliable.
Why Consistency Matters More Than Speed
Speed gains matter, but consistency is what enables scale. When workflows behave predictably:
- New staff onboard faster
- Adoption improves because expectations are clear
- Leadership gains visibility into effort and bottlenecks
- Improvements can be made systematically instead of anecdotally
Effective care team workflow becomes an organizational asset, not a dependency on individual expertise.
IV. Care Team Workflow Is the Foundation for Scalable Care
Care team workflow is not an operational afterthought. It is the structure that determines whether digital initiatives translate into real, repeatable outcomes.
When workflows are unclear, teams compensate with effort. When workflows are well designed, systems absorb complexity and teams focus on judgment, not coordination. This difference becomes more pronounced as organizations grow, add programs, or introduce new technologies.
Healthcare leaders often ask which tool, platform, or solution will unlock scale. In practice, scale is unlocked when care team workflows are explicitly designed around ownership, handoffs, escalation, and context sharing. Technology then reinforces those workflows instead of working against them.
Organizations that treat workflow as a foundational design decision gain more than efficiency.
They gain predictability, consistency, and the ability to improve operations systematically over time.
Before expanding initiatives or investing in additional tools, it is worth stepping back and examining how work actually moves across care teams today. That clarity enables digital health efforts to move beyond pilots and become part of how care is reliably delivered.
Care team workflow defines how work moves across roles, systems, and decisions inside an organization. Care coordination focuses on aligning activities around the patient. Coordination depends on workflow, but workflow determines whether coordination is repeatable and scalable.
Poorly designed workflows shift coordination work onto clinicians and care staff. This increases cognitive load, interruptions, and context switching. Clear workflows reduce unnecessary decisions and allow clinicians to focus on clinical judgment rather than operational tasks.
Yes. Workflow standardization applies to handoffs, ownership, and escalation, not clinical decision-making. Standardizing how work moves creates consistency while preserving clinical autonomy where it matters.
Workflow redesign is most effective before scaling new initiatives, adding tools, or expanding patient volume. Redesigning early prevents manual workarounds from becoming embedded in daily operations.
Digital tools rely on workflows to be effective. If workflows are fragmented, tools add complexity rather than value. When workflows are clear and system-driven, digital investments support adoption, visibility, and long-term operational improvement.


