



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
Care coordination workflows often fail after go-live due to misalignment between planned processes and real-world operations. Challenges include unclear ownership during handoffs, task routing mismatches, manual workarounds, and a lack of escalation paths. EHR integration can expose, rather than solve, these issues by creating alert overload, inconsistent task assignment, and compliance gaps. Over time, adoption drops as workarounds take over, and non-integrated systems create audit and compliance risks.
To fix these issues, focus on re-mapping workflows to reflect actual roles, adding escalation and accountability, and embedding compliance into task flows. Regular reviews and workflow corrections based on real-world feedback prevent small issues from becoming major failures, ensuring care coordination can scale effectively.
Most care coordination programs don’t fail during planning, vendor selection, or pilots. In fact, those phases often look reassuringly clean.
Workflows are mapped.
Roles are defined.
Dashboards show activity.
So why do breakdowns surface only after go-live?
Once a solution is live, care teams no longer operate in idealized workflows. They’re working inside real clinical environments where patient volume fluctuates, roles overlap, alerts compete for attention, and accountability is assumed rather than enforced.
After implementation, coordination is no longer theoretical. It becomes operational.
Care teams are juggling EHR task queues, manual handoffs, informal follow-ups, and compliance requirements that were never fully reconciled during design. What worked during a controlled pilot begins to fray once leadership oversight fades and throughput pressure increases.
For mid-market providers in particular, this gap is amplified by lean staffing models and shared responsibilities. A single care manager may span multiple programs, clinics, or risk cohorts.
Workflows designed around static job titles quickly break under this reality.
This is why care coordination challenges are rarely about choosing the wrong platform. They’re about whether post-go-live workflows align with how care is actually delivered across roles, systems, and time.
In other words, the system may be implemented correctly, but the work is not orchestrated.
I. Where Care Coordination Workflows Break First
Care coordination rarely collapses all at once. It starts breaking at specific pressure points that only become visible after go-live.
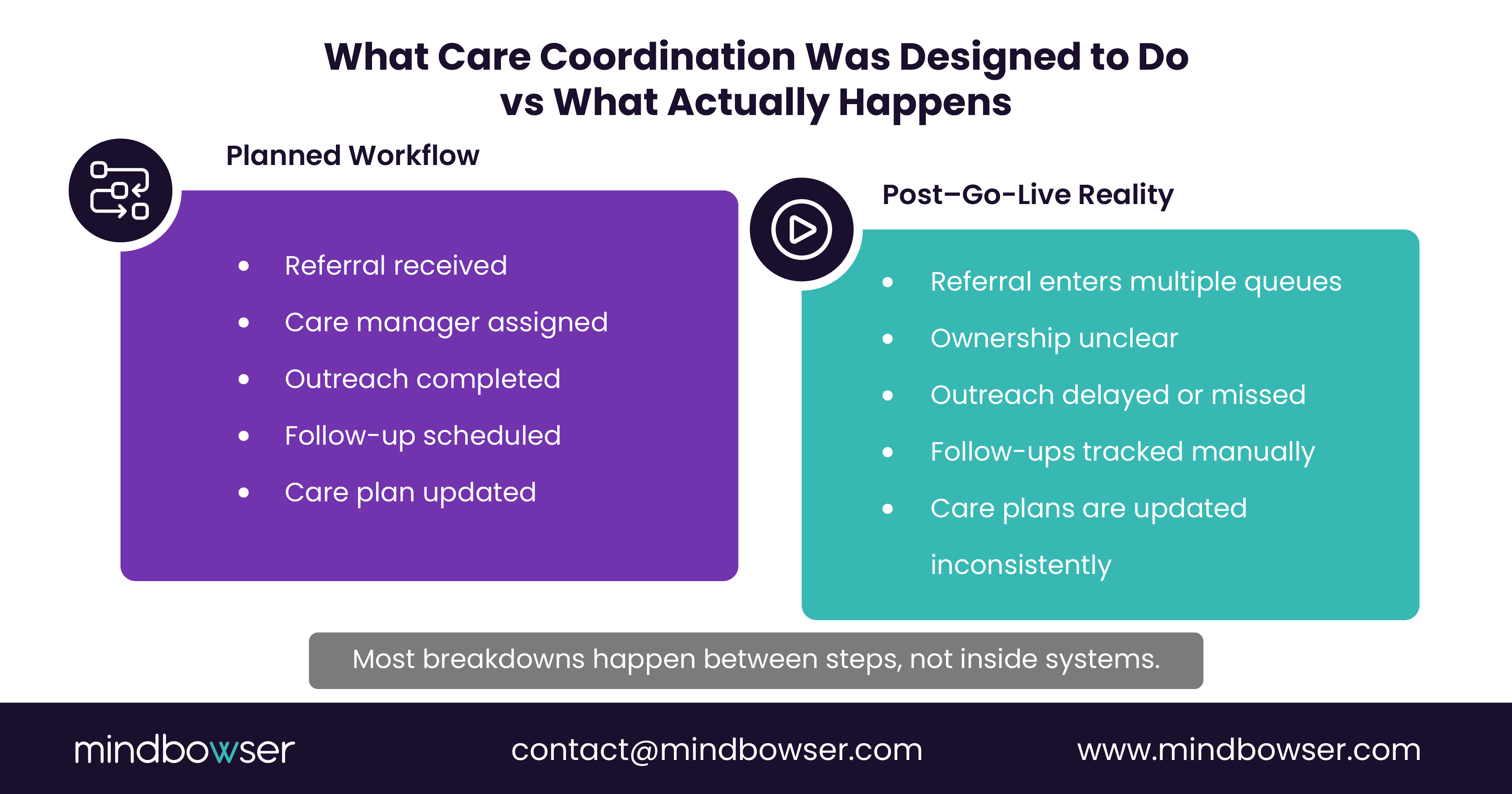
The most common failure is not missing data or system downtime. It is what happens between steps.
1. Handoffs Without Clear Ownership
On paper, ownership appears defined. In practice, it is often implied.
What we consistently see post–go-live:
- Tasks move between roles, but no one is explicitly accountable for the next action
- Alerts are generated, but responsibility is assumed rather than assigned
- Follow-ups rely on individual vigilance instead of system design
When ownership is unclear, tasks do not fail loudly. They simply age in queues until someone notices.
2. Task Routing That Does Not Match Real Roles
Many implementations map workflows based on org charts rather than operational reality.
In mid-market environments:
- Care managers cover multiple programs or clinics
- Roles shift by shift, site, or patient acuity
- Shared inboxes are used to “stay flexible.”
The result:
- Tasks land in inactive or generic queues
- Work is duplicated or silently delayed
- Escalation depends on tribal knowledge instead of rules
Flexibility without structure creates fragility.
3. Manual Handoffs Outside the System
When workflows do not reflect how work actually happens, teams adapt.
Common workarounds include:
- Email or chat messages to move work faster
- Spreadsheets to track follow-ups
- Verbal handoffs during huddles or hallway conversations
The moment this happens, care coordination becomes:
- Invisible to leadership
- Difficult to audit
- Inconsistent across teams
Coordination may still occur, but the system no longer reflects reality.
4. No Escalation When Work Stalls
An incomplete task should trigger action. In many workflows, nothing happens.
Typical gaps:
- No time-based escalation
- No risk-based prioritization
- No secondary owner when the primary role is unavailable
Without escalation, delays go unnoticed until outcomes are affected.
II. Why EHR-Integrated Care Coordination Still Breaks Down in Practice
EHR integration is often treated as the finish line for care coordination. Once tasks, alerts, and documentation live inside the EHR, teams assume coordination will naturally improve.
Post–go-live reality is different.
Integration often exposes workflow flaws rather than fixing them, especially when assumptions made during design do not hold up under real operating conditions.
1. Alert Volume Overwhelms Action
Many care coordination workflows rely heavily on alerts to drive next steps. After go-live, those alerts compete with every other clinical and operational notification in the EHR.
What happens over time:
- High-priority and low-priority alerts look the same
- Care teams scan instead of acting
- Truly urgent follow-ups blend into background noise
This is not a technology failure. It is a prioritization failure. When urgency and risk are not operationalized, alerts lose meaning.
2. Task Routing Mirrors Job Titles, Not Coverage Models
EHR tasking often assumes static roles. Real care delivery rarely works that way.
Common mismatches include:
- One person covering multiple roles across programs
- Tasks assigned to roles that are off-shift or understaffed
- Shared queues are used as a workaround for coverage gaps
When routing does not reflect coverage reality:
- Ownership becomes ambiguous
- Follow-through depends on personal discipline
- Accountability erodes quietly
The workflow functions, but only when people compensate for it.
3. Documentation Feels Like Extra Work, Not Care Delivery
Post–go-live, care teams are asked to document coordination activities to support reporting, audits, and quality programs.
When documentation is detached from action:
- Notes are completed late or inconsistently
- Care plans lose accuracy over time
- Compliance gaps accumulate without clear signals
Documentation works best when it is a natural outcome of task progression, not a separate step added at the end.
4. Integration Without Governance Creates Fragility
An EHR-integrated workflow still needs rules.
Without:
- Defined escalation paths
- Time-bound expectations
- Role-based accountability
Integration simply digitizes existing chaos.
This is why care coordination challenges persist even in technically sound EHR environments. The system is integrated, but the workflow is not governed.
III. Why Adoption Drops After Go-Live and Workarounds Take Over
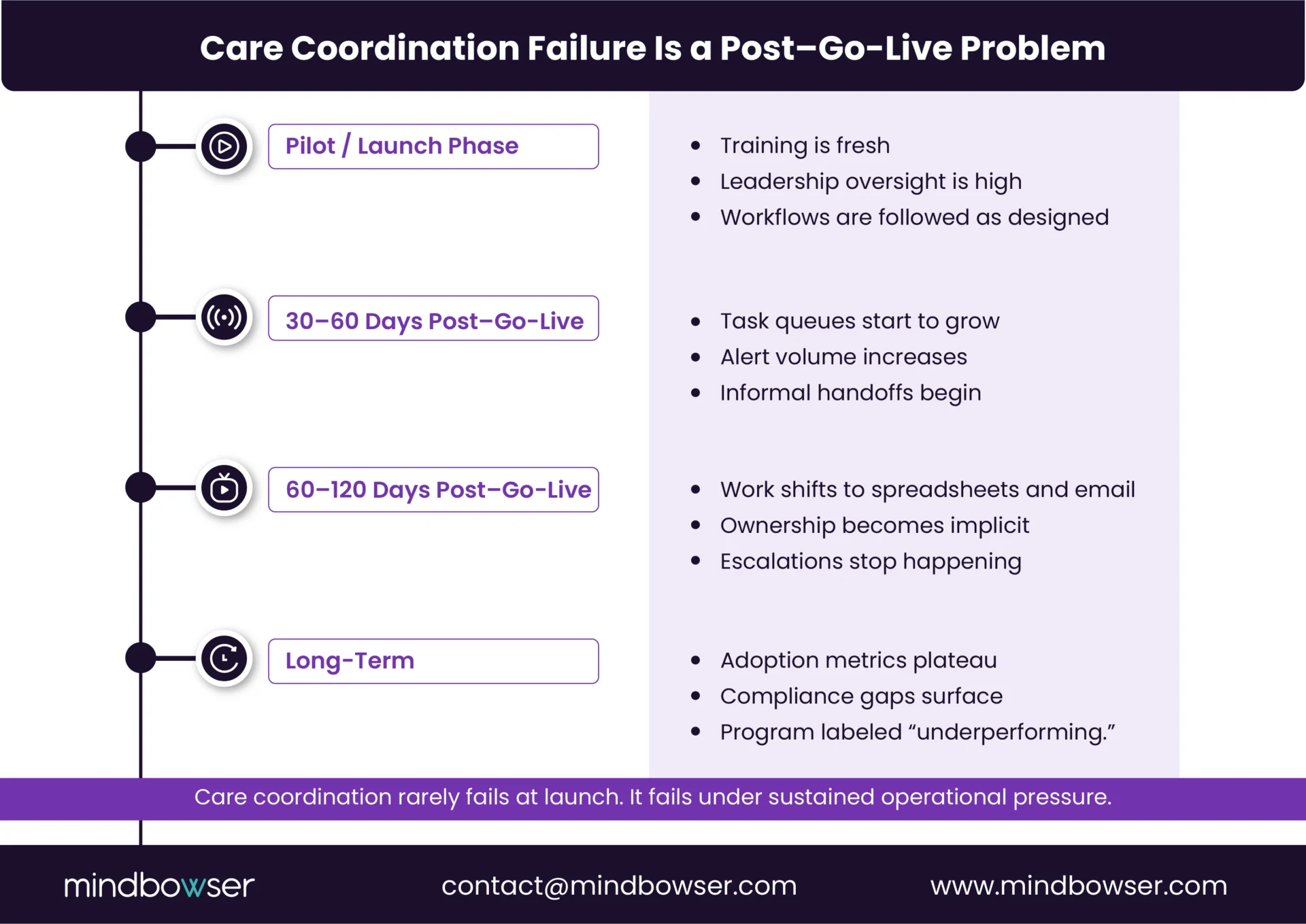
Care coordination tools rarely fail immediately. Adoption erosion happens quietly, usually within the first few months after go-live.
At launch, workflows are followed. Training is fresh. Leadership is watching.
Then operational pressure sets in.
Patient volume increases. Staffing flexes. Competing priorities surface. The workflow is tested in ways no pilot ever reveals.
1. Workflow Friction Creates Silent Resistance
When a workflow adds steps without removing others, care teams adapt to protect patient care.
Common patterns we see:
- Tasks are completed later in the day instead of in real time
- Follow-ups are tracked in personal notes or spreadsheets
- Informal verbal handoffs replace system-based ones
These are not signs of disengagement. They are signals that the workflow slows teams down.
2. Behavior Change Without Guardrails Does Not Scale
Post–go-live workflows often depend on people remembering to do the right thing.
Examples include:
- Closing tasks in a specific order
- Using structured fields consistently
- Updating care plans at precise moments
Without built-in enforcement:
- Consistency erodes
- Adoption metrics plateau
- Variability increases across teams
Over time, the workflow becomes optional instead of authoritative.
3. Dashboards Mask Frontline Reality
Leadership often relies on surface-level indicators such as:
- Task completion rates
- Login frequency
- Number of notes entered
These metrics can look healthy even when real coordination is happening elsewhere.
By the time outcome gaps appear, the workflow has already fractured into parallel processes.
4. Adoption Failure Is a Workflow Signal
When teams stop using a care coordination workflow as designed, it is rarely because the tool lacks features.
It usually means:
- Ownership is unclear
- Prioritization is manual
- The workflow does not respect time and role constraints
Retraining does not fix this. Redesign does.
Fix Workflow Gaps in Care Coordination and Restore Execution Confidence
IV. The Compliance and Risk Gaps That Emerge When Care Coordination Breaks Down
When care coordination workflows degrade, the first impact is operational. The longer-term impact is risk.
Post–go-live workarounds create compliance exposure that rarely shows up in dashboards. It surfaces later, during audits, payer reviews, or incident investigations.
1. Informal Coordination Breaks Auditability
As coordination moves outside structured workflows, it becomes harder to reconstruct what actually happened.
Typical gaps include:
- Missing evidence of task completion
- Inconsistent follow-up documentation
- Unclear timing of outreach or escalation
Emails, spreadsheets, and verbal handoffs do not create defensible audit trails. Even when care is delivered, organizations struggle to prove it.
2. Access Controls Weakened Through Workarounds
When systems slow teams down, access boundaries tend to loosen.
Over time, this leads to:
- Shared inboxes or credentials
- Proxy documentation by unauthorized roles
- Excessive permissions granted to “keep work moving.”
These shortcuts introduce HIPAA and least-privilege violations that accumulate quietly, especially in environments with rotating staff or external partners.
3. Compliance Is Treated as a Reporting Layer
Many implementations address compliance after workflows are designed.
This usually means:
- Adding checkboxes or required fields
- Relying on reports to flag gaps
- Asking teams to reconcile care delivery and documentation separately
The result is predictable. Documentation lags behind action. Timestamps are inconsistent. Remediation effort increases.
Compliance holds up best when it is embedded in task flows, escalation logic, and role assignments.
4. Risk Accumulates Post-Implementation
Care coordination breakdowns rarely trigger immediate failures.
Instead, small inconsistencies build over time:
- Missed follow-ups
- Delayed interventions
- Incomplete records
Eventually, these surface as quality penalties, denials, or legal exposure.
This is why post–go-live workflow reviews matter. They reveal risks that no pre-implementation checklist can catch.
5. What Actually Fixes Care Coordination After Implementation
Fixing care coordination after go-live does not start with new tools. It starts with acknowledging how work is actually getting done.
Organizations that recover from post-implementation breakdowns focus on workflow correction, not feature expansion.
Re-map Workflows Around Real Roles
The first step is to observe execution, not to review diagrams.
Effective redesigns focus on:
- Who performs each task in practice, not in policy
- How responsibilities shift by shift, site, or patient risk
- What happens when the primary owner is unavailable
Ownership is assigned to operational roles as they exist today, not as they were imagined during planning.
This alone reduces dropped handoffs without adding documentation burden.
Build Escalation Into the Workflow
A task that sits incomplete should never fail silently.
Strong escalation design includes:
- Time-based triggers tied to task type
- Risk-based prioritization for high-acuity patients
- Clearly defined secondary owners
Escalation removes the need for manual policing and ensures delays are visible before outcomes are affected.
Remove Steps Before Adding Structure
Post–go-live reviews often uncover steps added to satisfy edge cases or reporting needs.
High-performing teams:
- Eliminate low-value documentation
- Collapse redundant handoffs
- Reduce clicks before enforcing structure
Adoption improves when workflows make work easier, not heavier.
Embed Compliance Into Action
Compliance works best when it is enforced by workflow progression.
This means:
- Required fields triggered by task completion
- Automatic timestamps tied to actions
- Access controls aligned with role-based ownership
When compliance is part of execution, audit readiness becomes a byproduct instead of a separate effort.
Treat Post–Go-Live as a Design Phase
Teams that scale successfully treat go-live as the start of learning.
They plan for:
- Frontline feedback
- Usage pattern analysis
- Iterative workflow correction
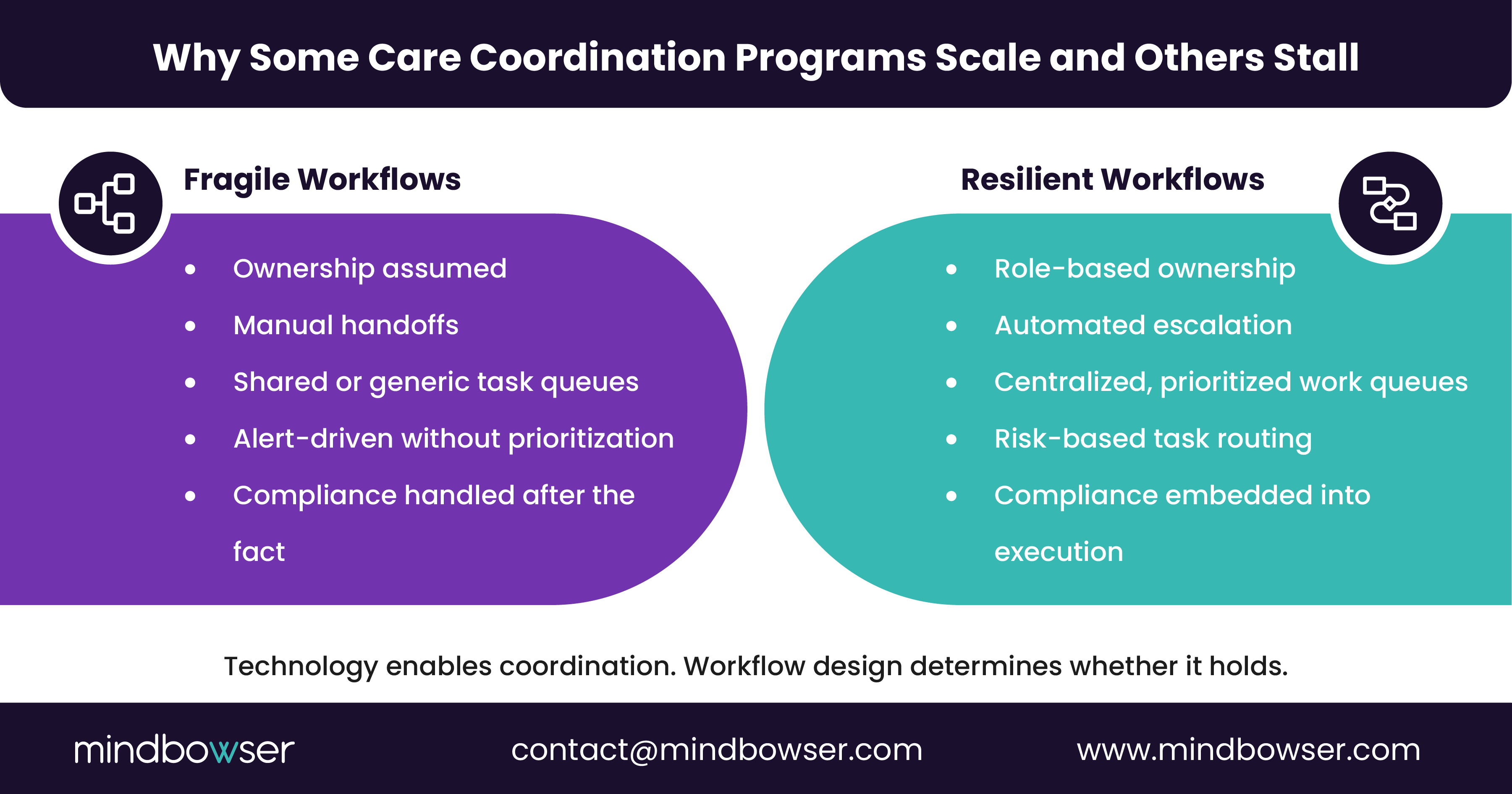
This mindset shift often determines whether care coordination remains fragile or becomes resilient.
Care Coordination Breaks When Workflows Are Treated as Static
Care coordination does not fail because teams lack commitment or because technology is insufficient. It fails when workflows are designed for launch rather than sustained execution.
Post-implementation reality introduces variability that no demo can capture:
- Staffing changes
- Shifting patient acuity
- Competing clinical and operational priorities
When workflows are not built to absorb this variability, small cracks form.
Over time:
- Handoffs lose clarity
- Ownership becomes implicit
- Work drifts outside the system
- Compliance gaps accumulate quietly
The response is often more training or more features. Neither addresses the root cause.
Care coordination stabilizes only when workflows are continuously shaped by how care is delivered in practice after go-live. Ownership is explicit. Escalation is automatic. Compliance is enforced by design.
For mid-market providers and scaling healthtech platforms, this is an inflection point.
Programs that correct workflow breakdowns early:
- Protect outcomes
- Reduce operational and compliance risk
- Preserve frontline trust
Those who do not often label care coordination as “underperforming” when the real issue is that the workflow was never designed to hold under pressure.
V. Next Step: Assess Before You Rebuild
If adoption has declined or workarounds have become the norm, the fastest path forward is a focused post–go-live workflow assessment.
A targeted review can quickly surface:
- Where handoffs are failing
- Which roles are overloaded
- Where escalation and compliance gaps exist
From there, workflows can be corrected without replacing systems or disrupting care delivery.
Care coordination works when workflows are designed to survive real-world pressure. That work begins after implementation, not before.
Post–go-live ownership should sit with operational clinical leadership, not IT or vendors. IT plays a critical support role, but care coordination breaks down when no one is accountable for day-to-day execution decisions, such as task prioritization, escalation rules, and role-coverage changes. Successful programs assign a single operational owner with authority to modify workflows as conditions change.
High-performing programs treat workflows as living systems. A practical cadence is:
- A structured review at 30, 60, and 90 days post–go-live
- Quarterly reviews once workflows stabilize
These reviews focus on task aging, escalation performance, and frontline friction rather than feature usage.
Yes, but only if workflows are designed with program-aware orchestration. Without this, care managers are forced to context-switch among different rules, queues, and documentation standards. Effective designs centralize work while allowing program-specific prioritization and escalation logic.
Rigidity usually comes from hard-coded rules that do not account for coverage variability or patient complexity. The solution is controlled flexibility:
- Role-based ownership with fallback paths
- Risk-based prioritization instead of static queues
- Escalation rules that adapt to time and acuity
This allows workflows to flex without losing accountability.
Beyond outcome measures, leaders should track execution health indicators, including:
- Time to first outreach
- Task aging by role
- Escalation trigger frequency
- Workload distribution across care managers
These metrics surface breakdowns early, before patient outcomes or financial performance decline.
External care managers, community partners, or outsourced services introduce additional handoff risk. Workflows must explicitly define:
- Where responsibility transfers
- How follow-ups are confirmed
- What documentation is required for auditability
Without this, accountability dissolves across organizational boundaries.
The most common mistake is layering fixes on top of broken workflows, such as adding dashboards, alerts, or retraining sessions. These increase noise without improving execution. Durable fixes always start with workflow simplification and ownership clarity.


