



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
The five-year extension of the Acute Hospital Care at Home (AHCAH) waiver through September 30, 2030 under Section 6210 of the Consolidated Appropriations Act, 2026, P.L. 119-75, gives health systems regulatory certainty they did not have when they were making 12-month pilot decisions. The operational bar, however, did not move: 24/7 RN call coverage, two daily visits, EMS coordination, clinical AI for selection and documentation, and ongoing CMS reporting all remain. State Rural Health Transformation Program (RHTP) plans signed in December 2025 now layer state dollars on top of the federal AHCAH framework in multiple states, turning build-vs-wait from a regulatory question into a capacity question.
The five-year extension of the Acute Hospital Care at Home waiver through September 30, 2030 changes the build-vs-wait calculus for every health system that has been hesitating, but it does not change the operational requirements CMS imposes on participating hospitals. When I sit down with a CMIO or VP of Innovation evaluating whether to apply, the conversation has changed in the last year. After Section 6210 of the Consolidated Appropriations Act, 2026, P.L. 119-75, the planning horizon extends through September 30, 2030. After Section 6210 of the Consolidated Appropriations Act, 2026, P.L. 119-75, the planning horizon extends through September 30, 2030.
This is a regulatory pathway guide written for the CMIO at a 350-700 bed regional health system whose CEO has said, “I want to know if we should apply for the AHCAH waiver before next year’s budget cycle.” The CFO will read it next, and ask harder questions about the payment mechanism. If your state is one of the dozen-plus that included Hospital at Home expansion in its RHTP plan, your State RHTP Project Director will read it after that, and the conversation moves into procurement.
What Is the AHCAH Waiver, and What Did It Originally Allow?
The Acute Hospital Care at Home (AHCAH) waiver is a CMS regulatory mechanism, originally launched in November 2020 under the COVID-19 Public Health Emergency, that lets approved Medicare-participating hospitals deliver inpatient-level acute care to traditional Medicare beneficiaries in the patient’s home rather than in a hospital bed. Hospitals must apply, demonstrate operational infrastructure, and meet ongoing CMS reporting requirements. The waiver suspends specific Conditions of Participation in 42 CFR Part 482, most notably the requirement for 24/7 nursing on the physical hospital premises and the physical-environment requirements that assume care happens inside the four walls.
The original 2020 program was a PHE response. It was extended through 2024 in the Consolidated Appropriations Act of 2023, then renewed again under various continuing resolutions. The program then lapsed on September 30, 2025 during the government shutdown, creating a 43-day disruption for participating hospitals, patients, and administrators. Congress extended AHCAH waivers and flexibilities through September 30, 2030 under Section 6210 of the Consolidated Appropriations Act, 2026, P.L. 119-75. CMS participation data showed hundreds of approved hospitals across dozens of states before the 2025 lapse, reflecting meaningful growth from earlier 2024 participation levels.
What the waiver actually provides is straightforward: a hospital that is already a Medicare-participating provider, that demonstrates the operational capacity to deliver acute inpatient-level care safely in the patient’s home, and that meets CMS’s ongoing reporting requirements, can bill traditional Medicare for AHCAH services at the standard inpatient DRG rate. The patient’s home becomes, for billing purposes, the inpatient bed.
What it does not provide, and this is where the misunderstandings start, is a payment differential. Medicare reimburses the AHCAH stay at the same DRG rate as the equivalent inpatient stay. There is no premium for the operational complexity of running care in 50 different homes instead of in one wing of a hospital. That math drives much of the strategic conversation in H2 #6.
What Did the 5-Year Extension Through 2030 Actually Change?
For three years before PL 119-75 was signed, every health system board considering AHCAH had the same problem. The capital request to build the program (clinical AI for patient selection, FHIR-grade EHR integration, RPM device fleet, 24/7 nursing coverage capacity, EMS coordination protocols, quality reporting infrastructure) had a payback window of 18 to 36 months. The waiver had a regulatory horizon of 12 months at a time. The math did not work, and dozens of health system boards I have walked through this with chose to wait.
Section 6210 of the Consolidated Appropriations Act, 2026, P.L. 119-75, extended AHCAH waivers and flexibilities through September 30, 2030. Congress allowed the prior authorization to expire on September 30, 2025 during a broader shutdown. The lapse created real disruption for patients mid-episode, for hospitals with capitalized infrastructure, and for state RHTP plans that assumed waiver continuity. That is a real five-year planning horizon going forward, but the lapse is the policy risk health systems should price into any build-vs-wait decision. Capital requests submitted to a health system finance committee in 2026 now have a regulatory backdrop that extends past the typical 36-month payback. Modern Healthcare, Becker’s Hospital Review, and the Bipartisan Policy Center covered both the lapse and reinstatement as a turning point for institutional commitment to H@H programs.
What the extension does NOT change is also worth naming clearly:
- Payment mechanism unchanged. Medicare still pays the inpatient DRG. There is no AHCAH-specific payment differential.
- Operational requirements unchanged. The 24/7 RN call coverage, two-daily-visit standard, EMS coordination protocol, and ongoing CMS reporting all remain.
- Patient eligibility unchanged. The clinical and social criteria CMS established are the same.
- Application path unchanged. Existing Medicare participation is still a prerequisite. Operational infrastructure must still be demonstrated. Ongoing reporting cadence is the same.
- Quality + safety obligations unchanged. What you were going to have to report in 2024 is what you will still have to report in 2026, 2028, and 2030.
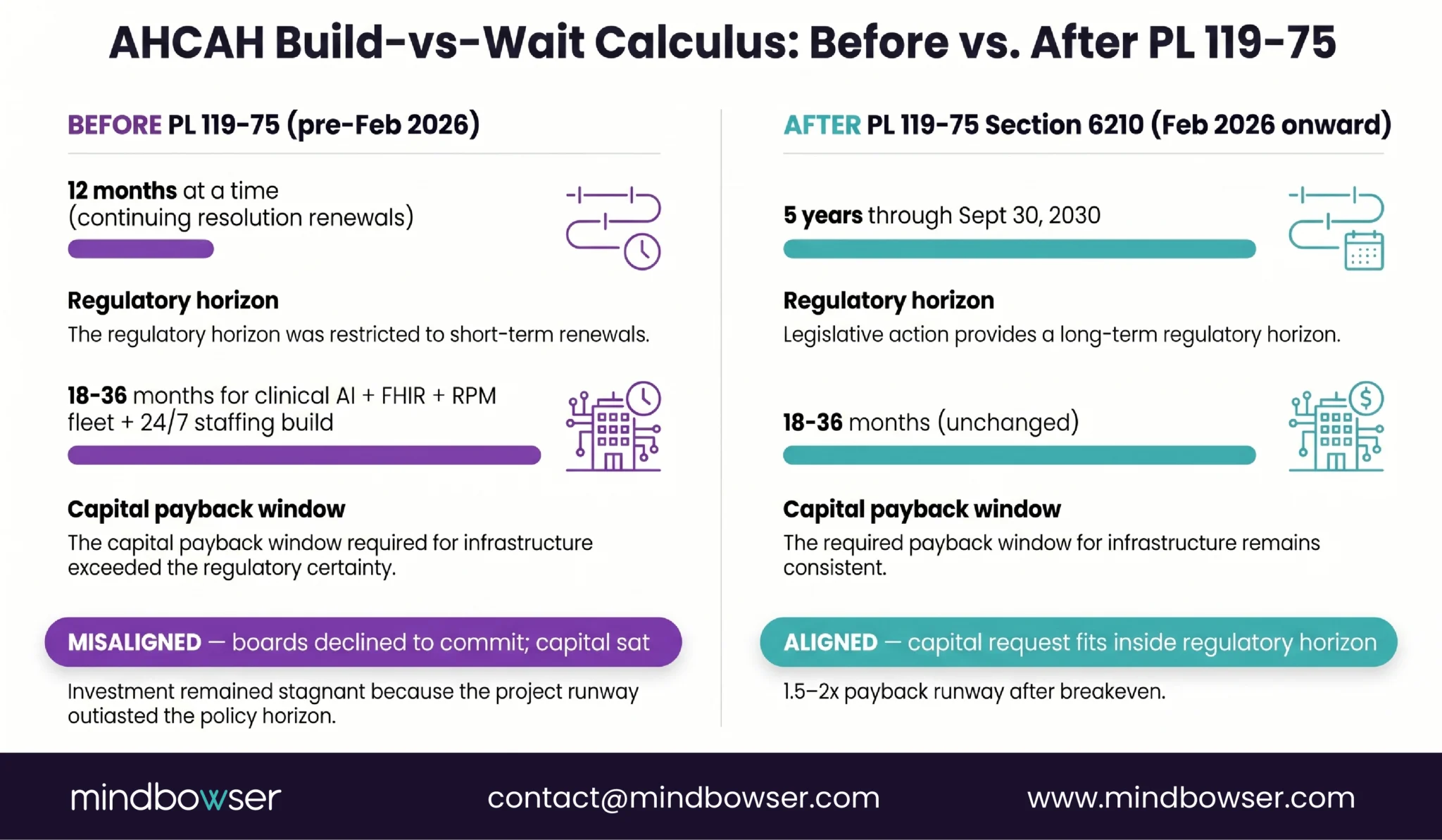
The extension is a regulatory horizon shift, not a regulatory simplification. That is the right frame for the build-vs-wait conversation.
Which Patients Actually Qualify for AHCAH?
It is 3:47 a.m. The ED hospitalist at a 480-bed regional hospital is looking at a 68-year-old patient with cellulitis of the left lower extremity, mild dehydration, controlled type 2 diabetes, and stable vitals. The patient lives 14 miles from the hospital, in a single-story home, with an adult daughter present overnight. Does this patient qualify for AHCAH enrollment, or does the hospitalist admit to the inpatient med-surg floor?
That is the actual decision point. Patient selection is the most clinically consequential step in the AHCAH workflow, because the wrong selection (a patient who decompensates faster than the home model can respond to) creates safety incidents that drive regulatory scrutiny and erode the program’s quality reporting. Mass General Brigham Home Hospital’s published operational data, which has been one of the most-cited references in the field, documents extensive patient-selection criteria they refined over multiple program-years.
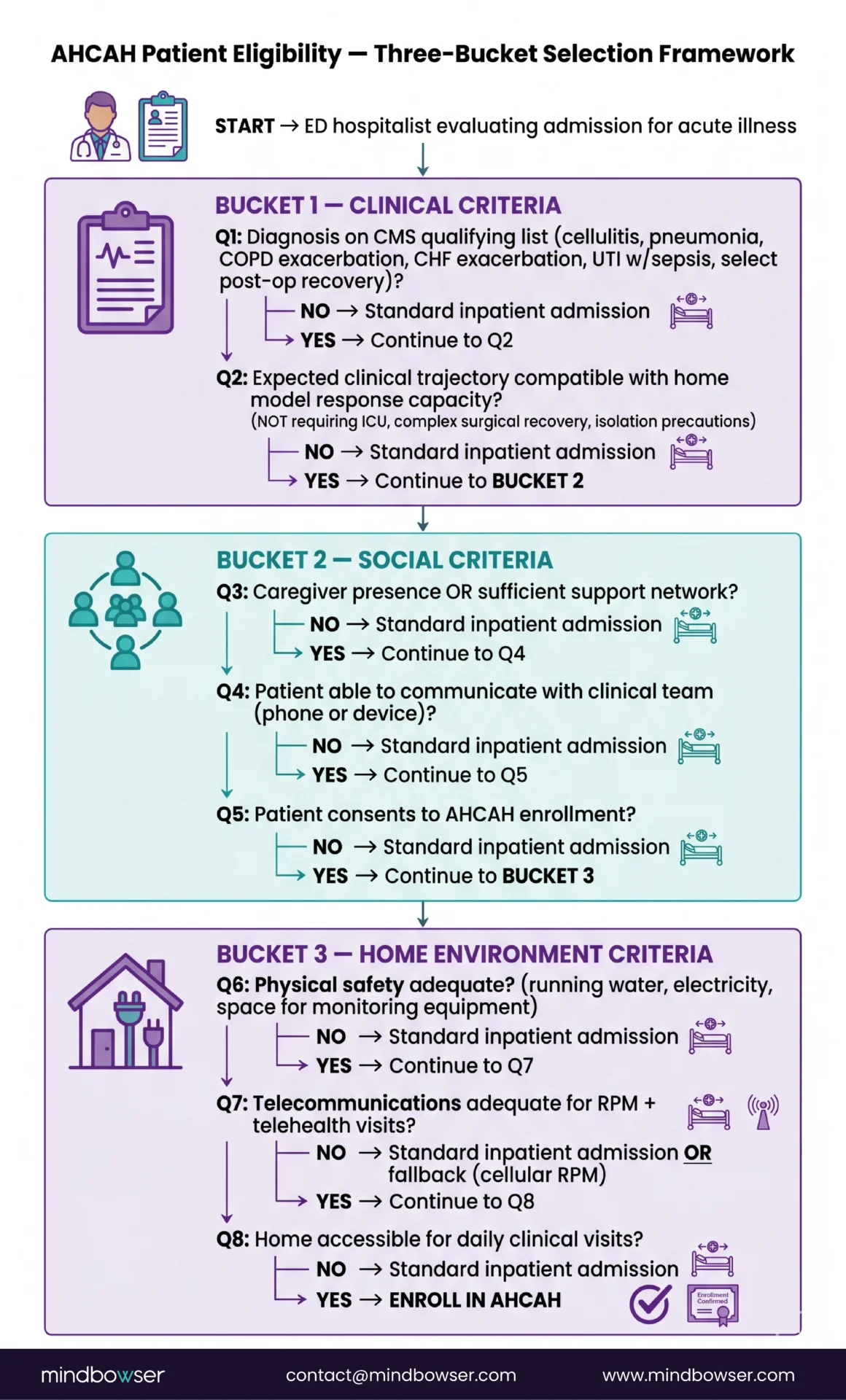
The CMS framework establishes three buckets of selection criteria:
- Clinical criteria. Acute illness or exacerbation requiring inpatient-level care. CMS publishes a list of qualifying diagnoses, including but not limited to cellulitis, pneumonia, COPD exacerbation, congestive heart failure exacerbation, urinary tract infection with sepsis, and select post-operative recoveries. The clinical team must judge that the patient’s expected clinical trajectory is compatible with the home model’s response capacity.
- Social criteria. A caregiver presence or sufficient support, an ability to communicate with the clinical team (phone or device), patient consent, and an acceptable level of patient acuity for the home setting.
- Home environment criteria. Physical safety (running water, electricity, sufficient space for monitoring equipment), telecommunications infrastructure adequate for the RPM and telehealth components, and accessibility for the daily clinical visits.
Patients excluded from AHCAH enrollment include those whose expected trajectory requires intensive care, complex surgical recovery, isolation precautions incompatible with home setting, or who lack the social and home environment supports.
The published programs that have shared their patient-selection refinements (Mass General Brigham, Mayo Clinic Advanced Care at Home, Atrium Health Hospital at Home) all converge on the observation that selection rigor in the first 90 days of a program is what determines safety reporting in years two and three. Programs that loosen selection criteria to drive enrollment volume see safety incidents rise, and CMS reporting starts asking harder questions.
How Does a Hospital Actually Apply for the Waiver?
The single biggest application failure mode I have seen is hospitals submitting before they have the operational infrastructure documented. CMS does not approve applications based on intent. They approve based on demonstrated capacity. A hospital that submits a one-page narrative attestation gets a return-for-additional-information letter, and the clock resets.
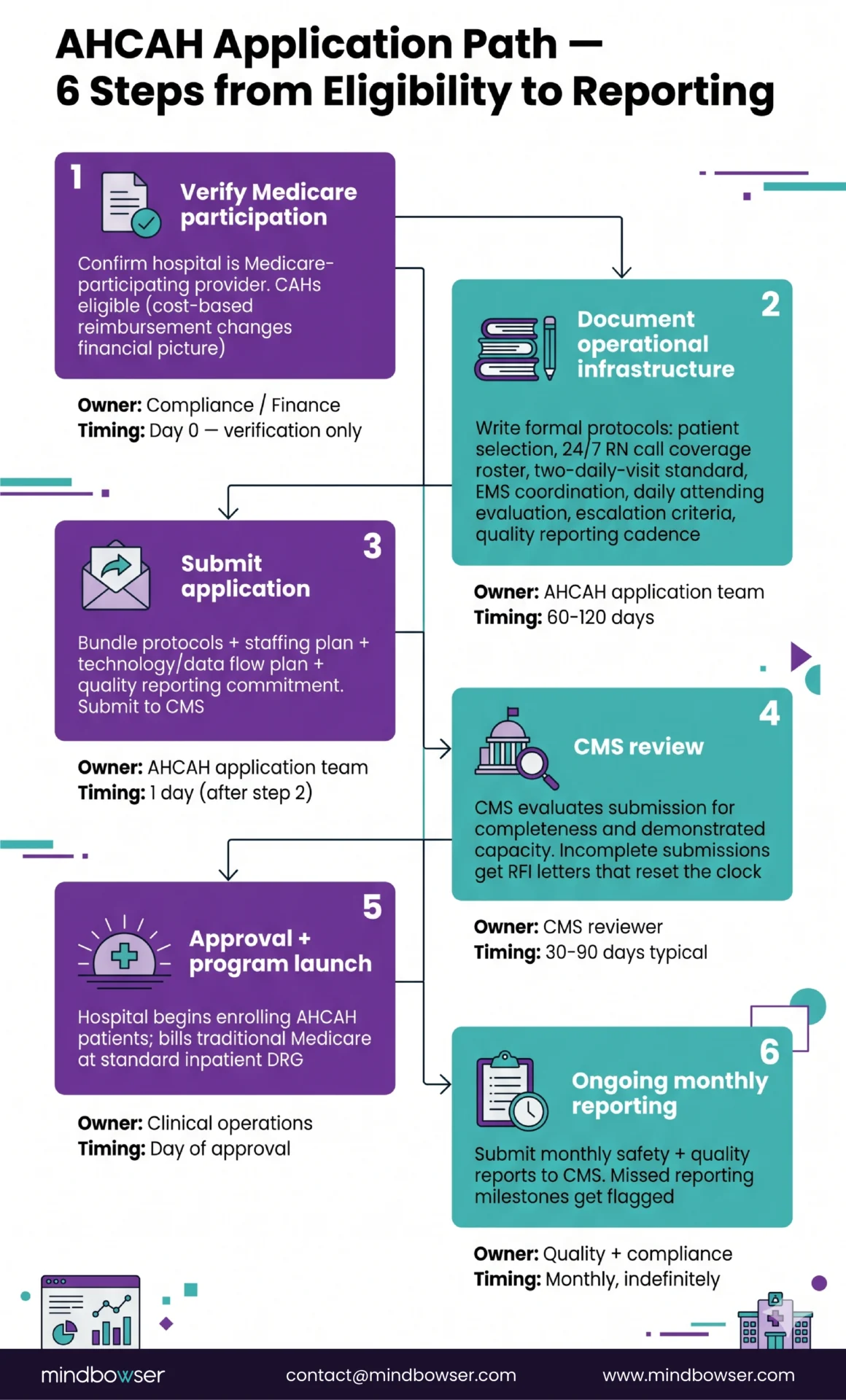
The application path follows a recognizable sequence:
- Verify Medicare participation status. Only Medicare-participating hospitals are eligible. Critical Access Hospitals can apply, though the CAH cost-based reimbursement structure changes the financial picture (we cover that in the rural H@H launch playbook).
- Demonstrate H@H program capability. This is the operational documentation step. CMS expects formal protocols covering patient selection, the 24/7 RN call coverage roster, the two-daily-visit standard (or one in-person plus one telehealth, per CMS guidance), the EMS coordination protocol with named local EMS providers, the daily attending physician evaluation workflow, the escalation criteria (when an AHCAH patient gets transferred to standard inpatient care), and the quality and safety reporting cadence.
- Submit the application. The submission includes the protocols, the staffing plan, the technology plan (CMS expects to see how patient data flows from home back to the EHR), and the quality reporting commitment.
- CMS review. Typical review timelines have been in the 30-90 day range, though they vary based on application completeness.
- Approval and program launch. Approved hospitals can begin enrolling AHCAH patients and billing traditional Medicare at the inpatient DRG.
- Ongoing reporting. CMS requires monthly safety and quality reporting. The reporting cadence does not stop. Programs that miss reporting milestones get flagged.
The operational infrastructure documentation is where most application work actually lives. The application itself is operational and regulatory work. There is no software product that writes the protocols for you. That said, the underlying technology stack the protocols describe (the FHIR data flows, the RPM integration, the clinical documentation, the patient-selection decision support) is where pre-built tools save months of build time. We come back to that in the technology stack section.
What Operational Requirements Survive the Extension?
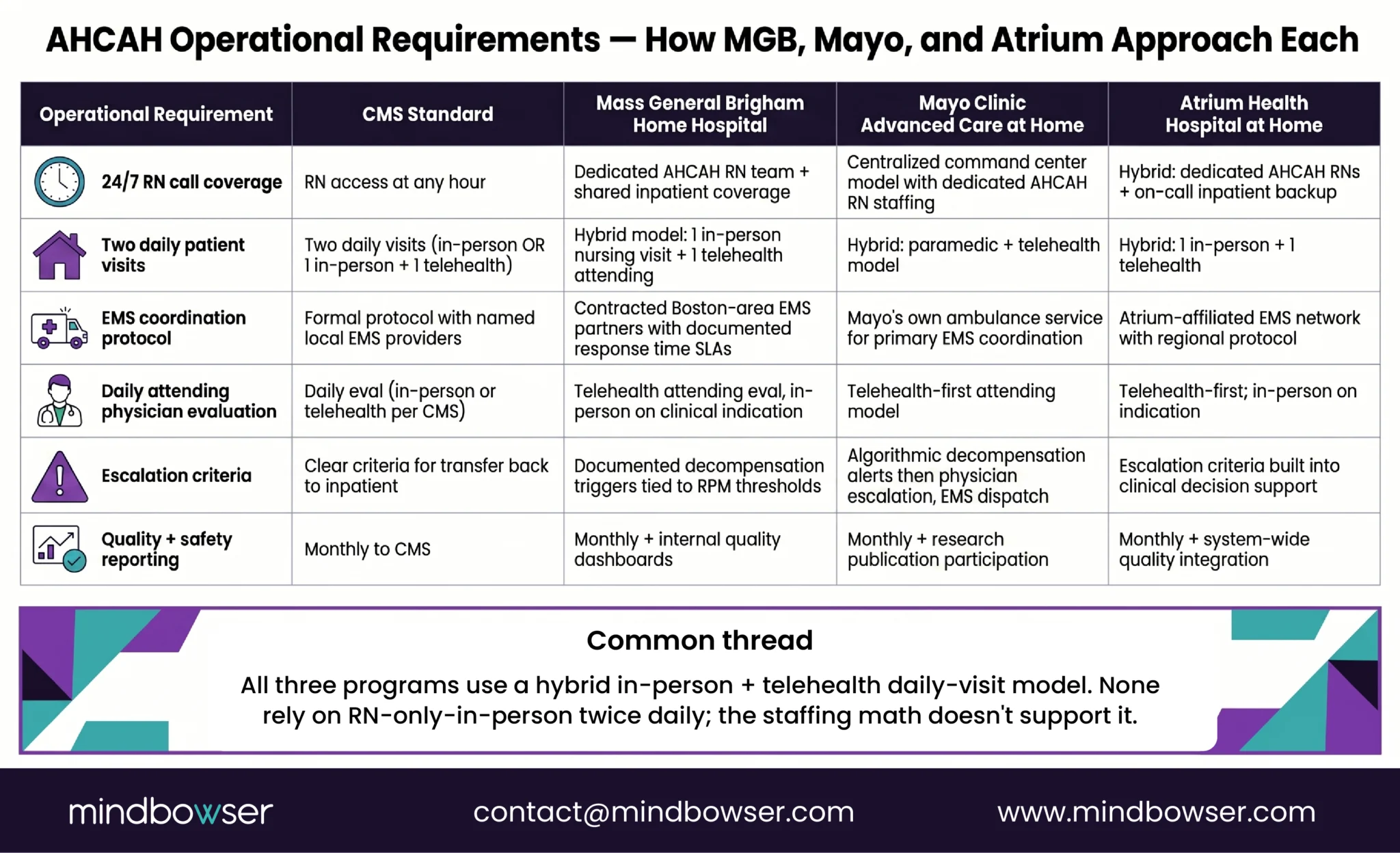
The gap between “we have a pilot” and “CMS will let us bill for it” is operational. The extension did not change that gap. The operational bar a hospital has to clear to participate in AHCAH includes:
- 24/7 registered nurse call coverage: A patient enrolled in an AHCAH program must have access to a registered nurse at any hour. This is staffing, not software. A hospital that does not have the headcount to cover 24/7 RN call lines should not apply. Most published programs handle this through a combination of dedicated AHCAH RN staffing and shared coverage with other inpatient services.
- Two daily visits per patient: CMS expects two daily visits to each enrolled patient. This can be two in-person visits or one in-person plus one telehealth visit, per published CMS guidance. Published AHCAH programs commonly use a hybrid model.
- EMS coordination protocol: AHCAH programs must have a formal protocol with local EMS providers covering escalation events. If an AHCAH patient deteriorates, the EMS response time and protocol matters.
- Daily attending physician evaluation: A physician must evaluate the patient daily. This can be in-person or telehealth, per CMS guidance.
- Escalation criteria. The program must have clear criteria for when an AHCAH patient is transferred back to standard inpatient care. This is both a clinical safety requirement and a CMS reporting expectation.
- Quality and safety reporting to CMS: Monthly. Including patient outcomes, adverse events, escalation events, and safety incidents.
Across published AHCAH programs, the operating model usually combines 24/7 RN call coverage, daily physician review, hybrid in-person and telehealth visits, RPM-supported monitoring, EMS escalation protocols, and monthly CMS quality reporting. The exact workflow varies by hospital, staffing model, geography, and local EMS capacity.
The 24/7 RN call coverage requirement is the single biggest staffing question. It is a capacity question, not a technology question. A 350-bed health system with thin RN coverage on the inpatient floors is not in a position to layer AHCAH coverage on top. That is one of the legitimate “wait” conditions in the build-vs-wait framework.
Ready to Turn the CMS Hospital at Home Extension Into a Competitive Advantage?
What MedPAC Said in June 2024 – and What That Means for Renewal Risk
The five-year extension is regulatory certainty for now. It is not regulatory permanence. Before September 30, 2030, Congress will have to decide whether to renew, sunset, or restructure the AHCAH program. MedPAC has already started raising the questions that will shape that debate.
The MedPAC June 2024 Report to Congress dedicated Chapter 6 to a review of the AHCAH program. The findings, paraphrased from the chapter:
Medicare pays AHCAH stays at the standard inpatient DRG without any payment differential, despite the fact that AHCAH program operational costs are different (and in some cases higher per-encounter) than equivalent inpatient stays. The lack of payment differential creates uneven incentives and may not be sustainable as a long-term Medicare payment policy.
Quality measurement for AHCAH programs is in early development. CMS has limited validated quality metrics specifically calibrated to the home setting, and the existing inpatient quality framework does not translate cleanly. Until quality measurement matures, MedPAC has limited ability to compare AHCAH outcomes to equivalent inpatient outcomes at policy-relevant scale.
AHCAH program enrollment is concentrated in well-resourced, predominantly urban and suburban health systems. Program access for rural Medicare beneficiaries, Medicaid-eligible patients, and underserved populations remains limited. Equity considerations will be central to any future renewal debate.
The Commonwealth Fund’s 2024 H@H reporting reinforced the access concentration finding, documenting that the majority of AHCAH-enrolled patients to date have been concentrated in a relatively small number of large health systems. The American Hospital Association’s 2024 H@H fact sheet, while advocating for permanent extension, acknowledged the same equity gap.
What this means for renewal risk: the 2030 renewal debate will probably hinge on three questions. (1) Can CMS develop AHCAH-specific quality measures that hold up at scale? (2) Can Medicare introduce a payment differential that aligns reimbursement to operational reality? (3) Can the program demonstrate equitable access growth, including penetration into rural and underserved populations? Health systems building AHCAH programs in 2026-2030 should be planning to participate in the data and outcomes evidence base that will inform that 2030 debate, not just running their programs in isolation.
This is also where state RHTP funding becomes strategically important.
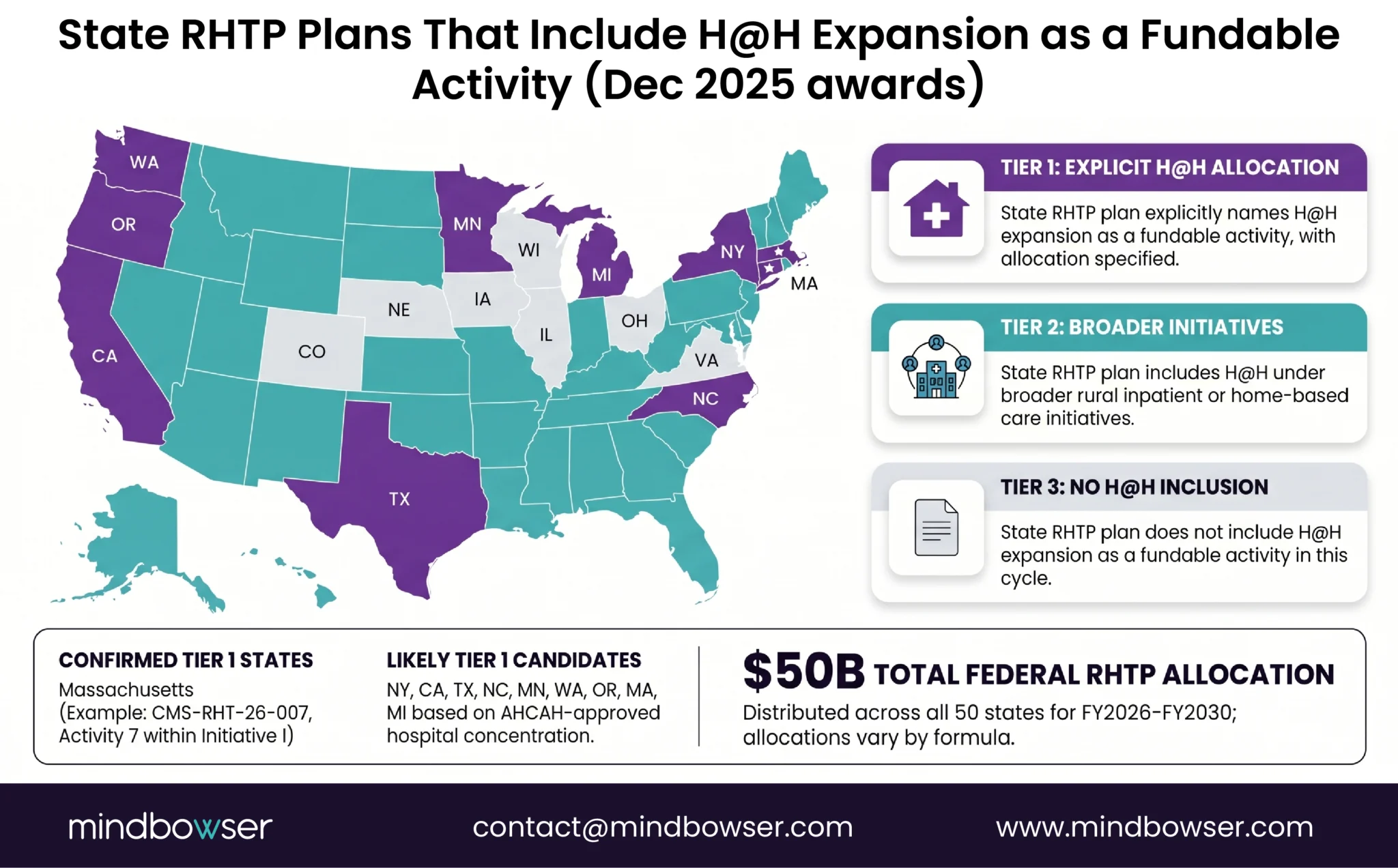
How Does State RHTP Funding Stack on Top of the AHCAH Waiver?
The Rural Health Transformation Program ($50B over FY2026-2030, all 50 states awarded December 2025) changes the H@H build math in states whose RHTP plans include H@H expansion as a fundable activity. The Massachusetts RHTP Application (CMS-RHT-26-007) lists Hospital at Home expansion as Activity 7 within Initiative I. Multiple other states’ applications include similar H@H expansion language.
State RHTP funding addresses what the federal AHCAH waiver alone does not address. The federal waiver gives a hospital the regulatory permission to bill Medicare. The state RHTP funding can help finance the capital build (the FHIR plumbing, the RPM device fleet, the clinical AI), the staffing capacity (the 24/7 RN coverage), and the operational scaling (the EMS coordination buildout). It can also help close the equity gap MedPAC flagged, by funding rural and underserved-population H@H deployments that the standalone DRG payment cannot finance.
The state procurement window is Q3 2026 through Q1 2027 in most states. State RHTP Project Directors are scoping their vendor selections in this window. Health systems planning AHCAH applications in that same window should be checking whether their state’s RHTP plan includes H@H expansion, and if so, what the eligibility and matching requirements look like for state RHTP H@H funding.
For a CMIO at a regional health system, the state RHTP overlay can shift a marginal build-vs-wait decision into a clear “build now” decision. For a State RHTP Project Director, the AHCAH waiver creates the federal regulatory framework that state RHTP-funded H@H expansion can run inside. The two programs are designed to be additive, and the timing is convergent.
What Technology Stack Does AHCAH Actually Require?
In every CMIO conversation I have, the technology question comes up early. What data flows does CMS oversight require? What clinical AI does the patient-selection decision lean on? What does the in-home device fleet look like? What integration depth does the EHR need?
Before any product enters the conversation, the capability list is worth naming clearly. An AHCAH program needs:
- Real-time vitals and symptom data flow from the patient’s home to the clinical team, including blood pressure, oxygen saturation, heart rate, weight, glucose where applicable, and patient-reported symptom data
- FHIR-grade EHR integration so the in-home work documents into the same inpatient record the daily attending uses, and so the discharge transition flows cleanly into outpatient follow-up
- Daily attending physician documentation infrastructure that handles both the in-person and telehealth visit components without doubling the documentation burden
- Care plan generation and patient-facing communication that the patient and caregiver can actually use (not a clinician-facing dashboard repurposed for the home)
- PHI compliance for in-home device data, which adds the home network and caregiver-access dimensions on top of standard hospital HIPAA compliance
- Readmission and decompensation risk decision support to inform patient selection at the front door and to flag deterioration trajectories during the AHCAH stay
- Post-AHCAH transition follow-up for the 30-day window where readmission risk is highest and the AHCAH-to-outpatient handoff has historically been a weak point
For most of these capabilities, pre-built tools are already running in production deployments and shorten the build timeline considerably. HealthConnect CoPilot is one of the tools doing the FHIR plumbing in production across health system deployments, with EHR integrations that connect Epic, Cerner, Athenahealth and the in-home device data into a single FHIR layer. Tools like WearConnect handle the 300+ wearable and RPM device integrations the continuous-monitoring requirement leans on, which removes most of the device-fleet integration work that AHCAH programs would otherwise do from scratch. AI Medical Summary is already running clinical summarization in production, with deployment data showing -50% documentation time and +45% accuracy, which addresses the daily attending documentation burden the operational requirements section flagged.
Patient selection decision support is a more focused use case. AI Patient Readmission Risk supports patient-selection decision-making at 8% prediction accuracy in production deployments and -25% 30-day readmissions, which gives the ED hospitalist in the H2 #3 scene a decision-support layer for the AHCAH-vs-standard-inpatient question. PHISecure handles the PHI de-identification layer for in-home device data and research-sharing scenarios that AHCAH programs increasingly need to participate in the quality evidence base MedPAC flagged. DischargeFollow AI covers the post-AHCAH transition follow-up where production deployments report -38% 30-day readmissions and -40% manual follow-up volume.
There are also workflow steps where no packaged accelerator exists, and naming them honestly matters. The CMS quality and safety reporting itself is custom build per program, not a packaged accelerator. The 24/7 RN call line is staffing, not software. The EMS coordination protocol is operational and relational work, not a product. The AHCAH application protocols themselves are operational and regulatory work that the application team writes, with the technology stack documented inside them. State Medicaid coverage parity, where it applies, is policy advocacy work. Programs that try to plug a product into every step lose credibility. Programs that name the human-required and custom-build steps clearly hold their credibility.
The pre-built tools shorten the from-scratch build by 6-9 months in most of the AHCAH technology categories. They do not replace the operational, staffing, and regulatory work that lives outside them.
Hospital at Home Platform Requirements Checklist: Validate your AHCAH platform readiness before you build or apply.
How Should a CMIO Decide: Build Now, or Wait?
Given the 5-year regulatory horizon, the unchanged operational bar, the MedPAC concerns shaping the 2030 renewal debate, and the state RHTP overlay, the build-vs-wait decision comes down to four questions a health system should be honest about:
- Do you have FHIR-grade EHR plumbing in place, or a credible plan to build it on a 6-12 month horizon? If yes, the data integration work that AHCAH requires is additive, not foundational. If no, the FHIR plumbing has to come first.
- Do you have 24/7 RN call coverage capacity, or a staffing plan that can credibly add it? This is the hardest question. RN supply is constrained nationally. A health system with thin inpatient RN coverage cannot layer AHCAH coverage on top.
- Does your state’s RHTP plan include H@H expansion, and if so, what is the eligibility and matching profile? The state overlay can shift the capital math significantly. Worth checking before the 2026-2027 budget cycle.
- Do you have quality and safety reporting capacity that can sustain monthly CMS reporting cadence indefinitely? Programs that miss reporting get flagged. Reporting capacity is what sustains the program past the launch year.
The 4-quadrant decision matrix:
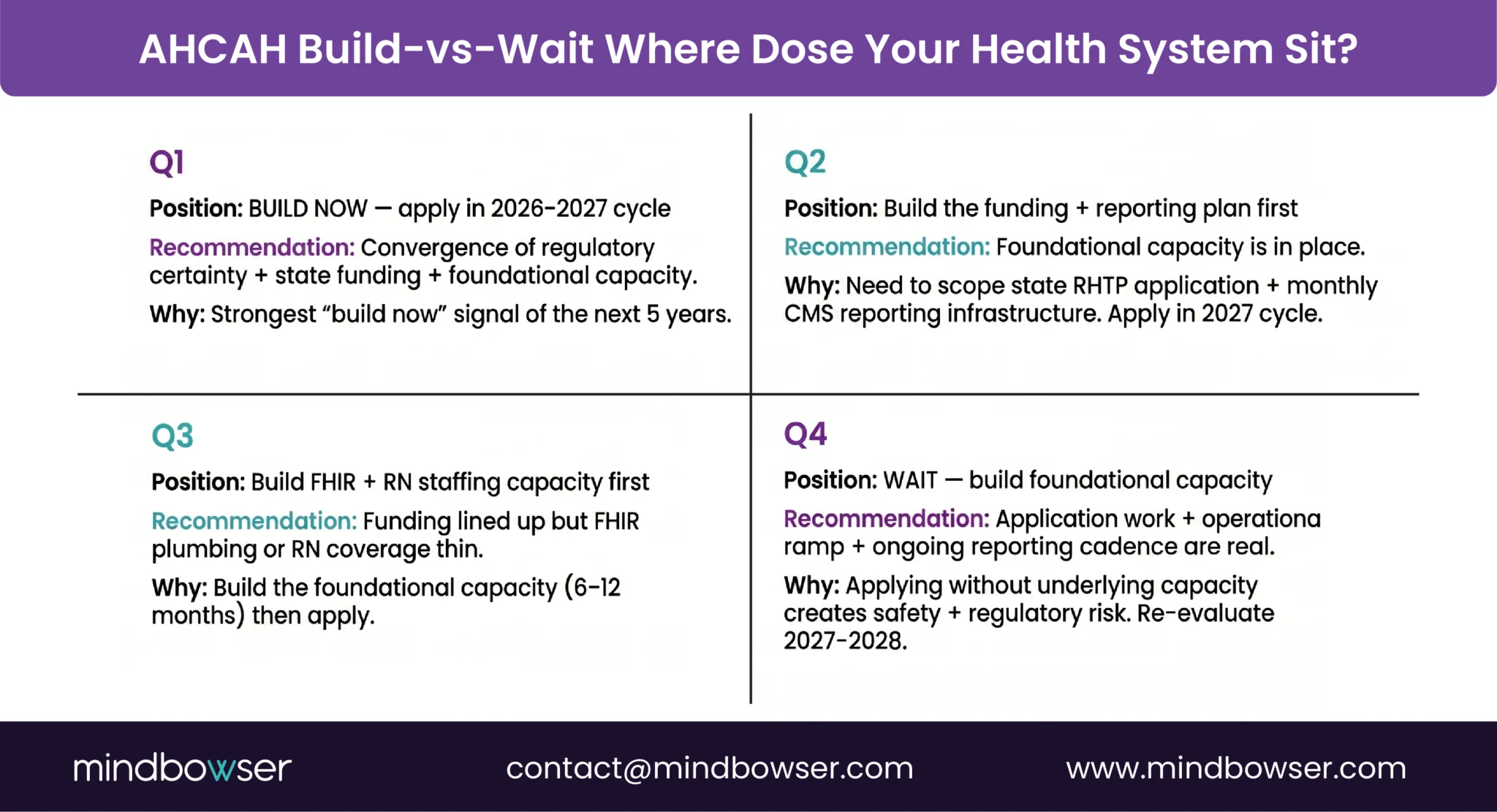
The honest “wait” conditions are worth naming explicitly. A health system in Quadrant 4 should not apply for AHCAH in the 2026-2027 cycle. The application work, the operational ramp, and the ongoing reporting cadence are real, and applying without the underlying capacity creates safety and regulatory risk. The five-year extension means there is a real planning runway. Wait, build the foundational capacity, and re-evaluate in 2027-2028.
A health system in Quadrant 1 should be applying in the 2026-2027 window, particularly if their state’s RHTP plan includes H@H expansion funding. The convergence of regulatory certainty + state funding + foundational capacity is the strongest “build now” signal of the next five years.
The two off-diagonal quadrants are the conversations that take the longest. Most health systems I work with land in one of those two, and the right answer is to name the gap (FHIR plumbing OR funding+reporting capacity) and build it before applying.
How Mindbowser Helps Health Systems Build AHCAH-Compliant H@H Programs
AHCAH compliance is a workflow redesign, not a product purchase. The capability layers an AHCAH program needs (FHIR data flows from home to EHR, RPM device fleet integration, clinical AI for patient selection and documentation, in-home PHI compliance, readmission decision support, post-discharge transition follow-up) all exist in production today. The Mindbowser engagement maps the workflow first, then plugs in the pre-built components that already cover most of those capability layers, then custom-builds the program-specific layer (state-specific reporting, payer-contract configuration, AHCAH protocol documentation, 24/7 coverage workflow design).
Health systems starting from this stack skip 6-9 months of from-scratch FHIR + RPM + clinical AI build and reach AHCAH application-readiness in roughly half the timeline of a from-scratch effort. The accelerator components named in the technology stack section (HealthConnect CoPilot, WearConnect, AI Medical Summary, AI Patient Readmission Risk, PHISecure, DischargeFollow AI) are already running in production. The custom layer on top is where each program’s distinctiveness lives.
AHCAH authority note: Originally extended by CAA 2023 Section 4140 through December 31, 2024; reinstated and extended through September 30, 2030 by PL 119-75 Section 6210, signed February 2026. The waiver allows qualified hospitals to deliver inpatient-level care at home by waiving selected hospital Conditions of Participation requirements, including the 24/7 on-site nursing requirement under 42 CFR Section 482.23(b).
The CMS Acute Hospital Care at Home (AHCAH) waiver is a Medicare regulatory mechanism, originally launched in November 2020, that allows approved Medicare-participating hospitals to deliver inpatient-level acute care to traditional Medicare beneficiaries in the patient’s home. It suspends specific Conditions of Participation in 42 CFR Part 482 (most notably the 24/7 on-premises nursing requirement) for participating hospitals. PL 119-75 Section 6210 extended the waiver through September 30, 2030.
The current AHCAH waiver, as extended by PL 119-75 Section 6210, signed February 2026, runs through September 30, 2030. Before that date, Congress will have to decide whether to renew, sunset, or restructure the program. MedPAC’s June 2024 Report to Congress raised three policy questions (payment differential, quality measurement, and equitable access) that will likely shape the renewal debate.
A hospital must (1) verify Medicare participation status, (2) document its operational infrastructure (24/7 RN coverage, two-daily-visit standard, EMS coordination, daily attending evaluation, escalation criteria, technology and data flow, quality reporting cadence), (3) submit the application with formal protocols, (4) complete CMS review (typically 30-90 days), and (5) maintain monthly safety and quality reporting to CMS after approval.
CMS organizes patient eligibility into three buckets: (1) clinical criteria (acute illness requiring inpatient-level care, qualifying diagnosis, expected trajectory compatible with home model), (2) social criteria (caregiver presence or sufficient support, communication ability, patient consent), and (3) home environment criteria (physical safety, telecommunications adequate for RPM and telehealth, accessibility for daily clinical visits). Patients requiring intensive care, complex surgical recovery, or isolation precautions are excluded.
No. Medicare reimburses AHCAH stays at the standard inpatient DRG rate, with no payment differential for the operational complexity of running care across multiple home settings. MedPAC’s June 2024 Report to Congress identified the lack of payment differential as a sustainability concern, and the question is likely to be central to the 2030 renewal debate.
