



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
Rural telehealth marketing assumes broadband that the FCC’s 2024 Section 706 Broadband Deployment Report shows a meaningful share of rural Americans still do not have , roughly 16.9 percent lack access to the older 25/3 Mbps threshold, and approximately 28 percent lack access to the current 100/20 Mbps standard that modern telehealth workloads increasingly assume. The deployments that actually work in these rural service areas use low-bandwidth video codecs, store-and-forward asynchronous workflows, hub-and-spoke specialist networks, and cellular fallback. Reimbursement parity is uneven and commercial payer coverage is narrower than CMS coverage. FCC Rural Health Care Program subsidies and USDA Distance Learning and Telemedicine grants pay for the broadband infrastructure that closes the gap. RHTP funding now layers on top of both for the hospitals that apply.
Opening: What Rural Telehealth Marketing Quietly Ignores
Telehealth has been pitched as the answer to rural healthcare access for fifteen years. Conference keynotes, vendor decks, and policy briefs converge on the same narrative: video visits eliminate distance, specialty consults flow through screens, and the rural access gap closes itself.
The narrative is half true. Telehealth has expanded rural access in measurable ways. It has also accumulated more marketing claims than verified outcomes, and the gap between the pitch and what works in a 25-bed Critical Access Hospital with 6 Mbps upload speed is wider than most decks acknowledge.
Three things rural telehealth marketing routinely ignores:
- Rural broadband gaps remain substantial at modern benchmarks. The FCC’s 2024 Section 706 Broadband Deployment Report finds roughly 16.9 percent of rural Americans lack access at the older 25/3 Mbps threshold and approximately 28 percent lack access at the current 100/20 Mbps standard. Video codecs that work in suburban primary care do not work at 3 Mbps upload with 200 ms jitter, and they degrade visibly below 100/20.
- Specialist supply is the constraint, not patient demand. A telehealth platform without a specialist on the other end is a webcam pointed at an empty room.
- Commercial reimbursement parity is uneven. CMS covers more than most state Medicaid programs, and commercial payers cover less than CMS.
The hospitals that have deployed working rural telehealth in 2026 worked around all three constraints. The ones that bought platforms without solving for them are still paying license fees on systems clinicians stopped using in month four.
This piece walks through what actually works, what reliably fails, and where Rural Health Transformation Program (RHTP) funding now changes the math.
Can Rural Telehealth Actually Work Without Reliable Broadband?
Yes, but not the way most platforms market it.
Rural telehealth works without reliable broadband when the architecture matches the constraint. That means low-bandwidth video codecs (H.265/HEVC at 384-512 kbps), audio-only fallback for billing-eligible visits, store-and-forward asynchronous workflows for specialty consults, and cellular bonded connections where wired broadband is intermittent. It does not mean a 1080p video visit on a 3 Mbps connection. That fails predictably.
The hospitals that have deployed working rural telehealth in low-broadband counties accept three architectural choices upfront:
- Synchronous video is the exception, not the default. Most rural telehealth volume runs as audio-only follow-ups, store-and-forward derm/wound/radiology consults, and remote patient monitoring data review. Synchronous video is reserved for tele-stroke, tele-psych intakes, and acute consultations where real-time interaction is medically necessary.
- Bandwidth is engineered, not assumed. QoS marking, jitter buffers, codec selection, and bonded cellular fallback are configured into the network before clinicians touch the platform.
- Hub-and-spoke beats point-to-point. A rural hospital does not contract with 14 individual specialists. It contracts with one academic medical center hub that fields the consultations across services.
The platforms that work in rural deployments support all three. The ones that don’t get returned.
What Rural Telehealth Marketing Gets Wrong
Five claims show up repeatedly in rural telehealth pitches that do not survive contact with a 25-bed hospital’s actual operating environment.
- Claim 1: “Telehealth solves rural specialist access.” Telehealth does not create specialists. It connects existing specialists to patients more efficiently. If the regional academic medical center has a 14-week wait for tele-neurology, the rural hospital has a 14-week wait for tele-neurology. The platform did not change supply.
- Claim 2: “Our platform works on any connection.” Every platform works on a sales demo. Rural deployment exposes the difference between “works” and “remains usable when 6 of 12 concurrent visits drop to 2 Mbps because the school district is streaming end-of-day announcements.” Vendors that cannot answer detailed questions about codec behavior under packet loss have not deployed in rural environments.
- Claim 3: “Reimbursement parity is settled.” Reimbursement parity is settled for Medicare on a state-by-state and code-by-code basis with continuing CMS rule changes. Medicaid parity varies by state. Commercial parity varies by payer and plan. Hospitals deploying telehealth based on “parity is settled” assumptions discover the gaps in month three of revenue cycle review.
- Claim 4: “Patients adopt easily.” Rural patient median age is 72. Digital literacy varies. The hospitals running successful rural telehealth invest substantial care coordinator time in patient onboarding, device support, and family caregiver training. The platforms that pretend onboarding is friction-free have not measured it.
- Claim 5: “It pays for itself in year one.” Some specific use cases (tele-stroke, tele-psych) pay for themselves quickly through avoided transfers and shortened length of stay. Most rural telehealth use cases reach breakeven in year two or three after enrollment ramps, infrastructure depreciates, and reimbursement workflows stabilize. Year-one ROI claims are usually ROI on a pilot, not on production operations.
We have seen all five claims fail in deployment. We have also seen rural telehealth produce real clinical and financial outcomes when the architecture, specialist contracts, and reimbursement workflows are designed for the constraint instead of around it.
Low-Bandwidth Architecture for Rural Telehealth
A working low-bandwidth telehealth architecture has six components.
- 1. Codec selection. H.265/HEVC at 384-512 kbps for video, Opus at 24 kbps for audio. The codec is the single largest determinant of whether the call holds at low bandwidth. Older H.264 platforms require 1-2 Mbps for usable quality and degrade rapidly below that.
- 2. Adaptive bitrate. The platform must downshift video quality (and ultimately drop to audio-only) when bandwidth drops, without requiring clinician intervention. A platform that freezes the call instead of downshifting is unusable in rural environments.
- 3. Bonded cellular fallback. A bonded cellular connection (LTE or 5G aggregating 2-3 carrier links) provides the backup when wired broadband fails. Costs $200-400 per month per site but eliminates the most common failure mode in rural telehealth: wired connection drop mid-visit.
- 4. QoS marking on the LAN. Telehealth packets are DSCP-marked at the endpoint and prioritized through the LAN and WAN. Hospitals that skip QoS configuration discover the EHR backup job killing the tele-stroke consult on Tuesday morning.
- 5. Jitter buffer tuning. Default jitter buffers assume sub-100 ms latency. Rural connections frequently run 150-300 ms with bursty jitter. Buffer tuning at the endpoint reduces audio dropouts and lip-sync drift.
- 6. Endpoint hardware. Carts, peripherals, and stethoscopes need to be telehealth-grade rather than consumer webcams. Rural deployments that try to save capex on endpoint hardware compromise diagnostic quality and create clinician adoption resistance.
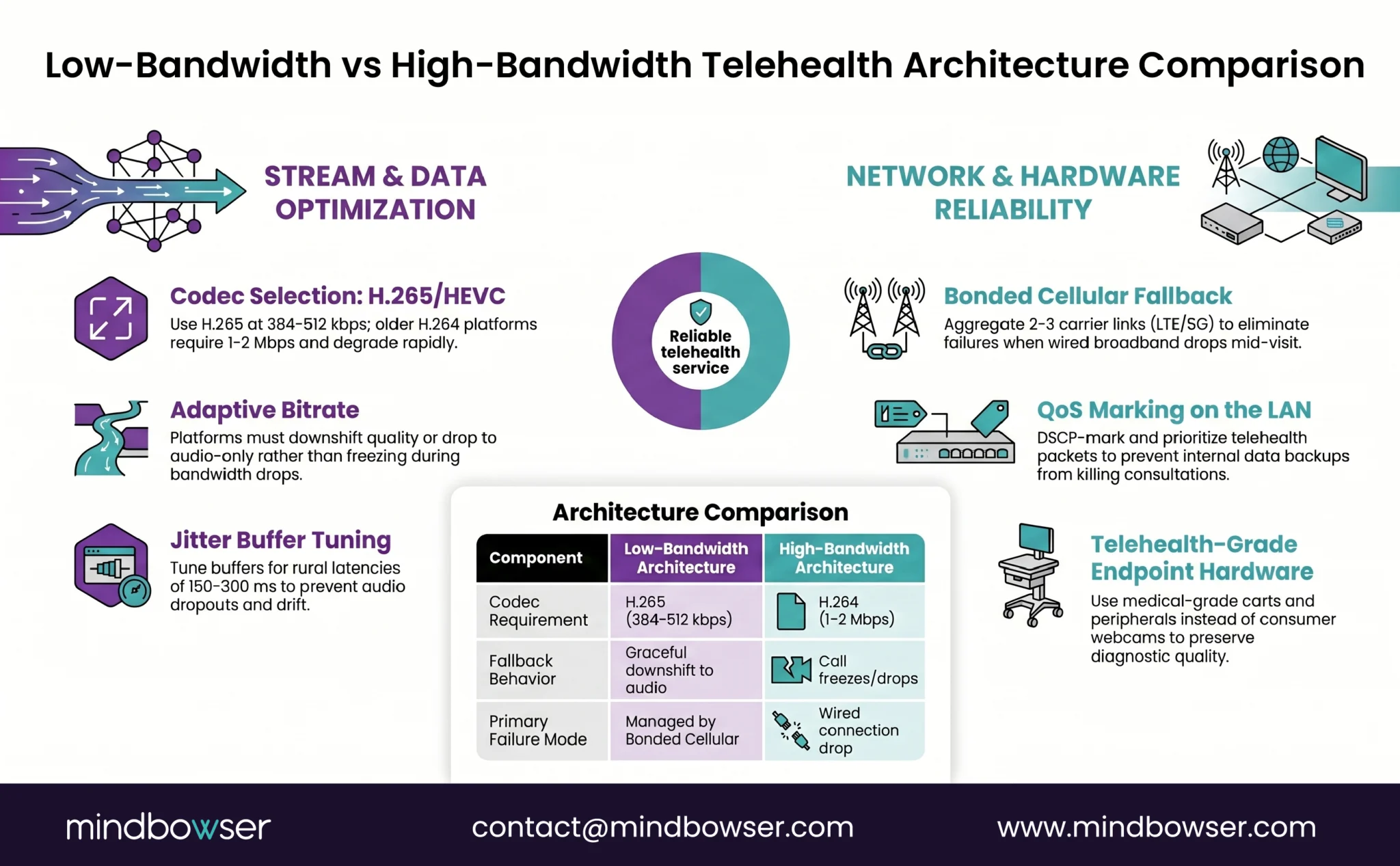
When all six components are in place, telehealth runs reliably at 1.5-2 Mbps with degradation graceful enough to preserve clinical workflow. When any one is missing, the deployment fails in ways the help desk struggles to diagnose.
Hub-and-Spoke Specialty Access: The Model That Works
The hub-and-spoke model is the rural telehealth pattern with the longest track record of measurable outcomes. It works because it solves the supply-side problem rather than pretending the problem is technology.
- The structure. A rural hospital (spoke) contracts with an academic medical center or large health system (hub) for specialty consultation services across multiple specialties under one agreement. The hub commits to coverage windows (often 24/7 for tele-stroke and tele-ICU, business-hours for tele-psych and tele-derm). The spoke routes consultation requests through the hub’s intake workflow rather than calling individual specialists.
- Why it works. Rural hospitals cannot recruit a neurologist, psychiatrist, intensivist, dermatologist, and infectious disease specialist. Hubs already employ them. The hub-and-spoke contract converts the rural hospital’s specialist access problem from a recruiting problem (impossible) into a contracting problem (solvable).
- The economics. Hubs charge per-consultation fees ($150-400 for routine consults, higher for tele-stroke), retainer fees ($5,000-15,000 per month for guaranteed coverage), or hybrid models. The spoke captures the avoided transfer revenue, the shortened length of stay, and the patient retention. The hub captures the consultation fee and a referral pipeline for tertiary cases that genuinely need transfer.
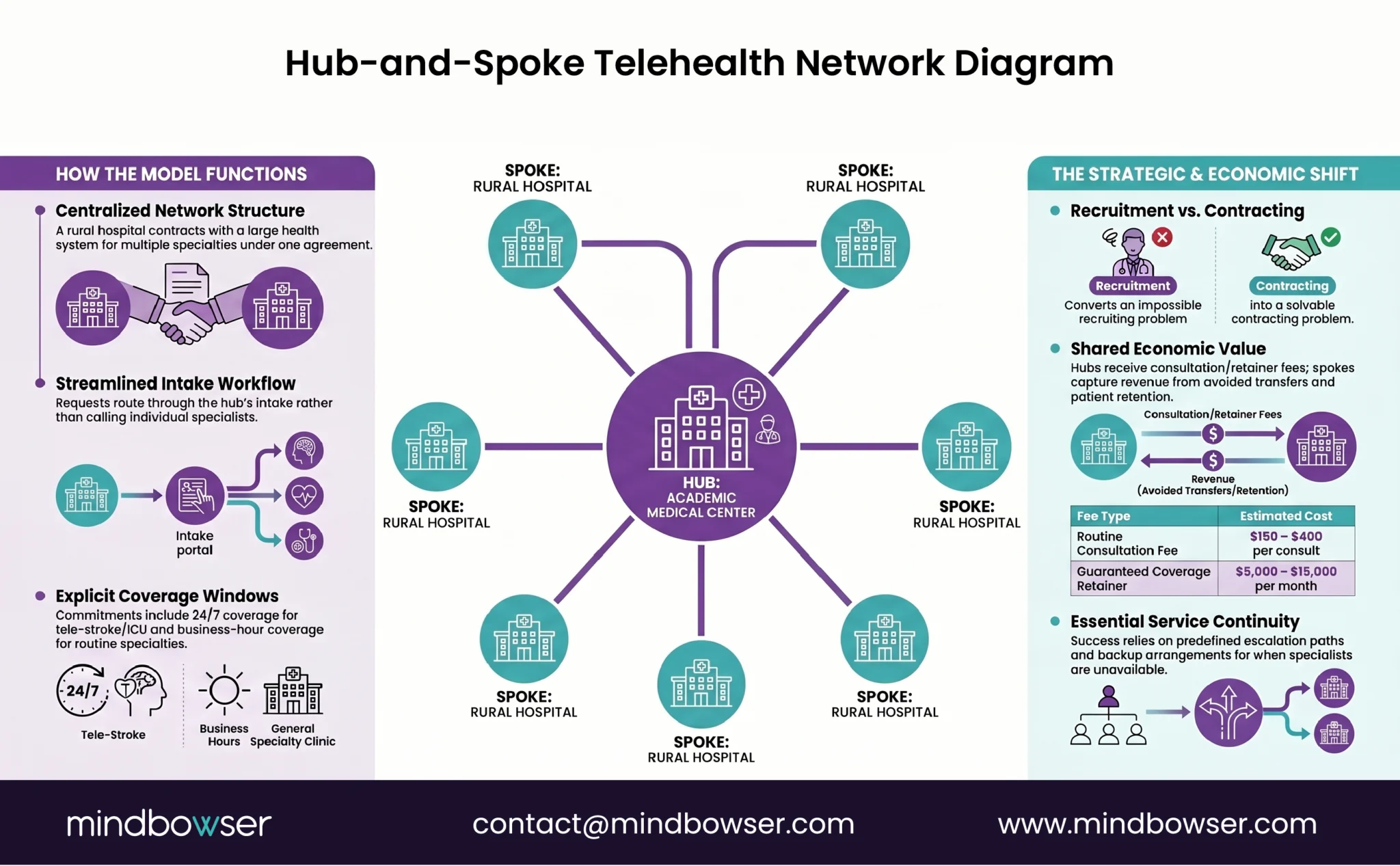
The hub-and-spoke contracts that work get the coverage definitions right. Coverage windows are explicit. Escalation paths are documented. Backup arrangements when the hub specialist is in surgery are pre-defined. The contracts that fail leave coverage as “best effort” and discover during a 2 a.m. tele-stroke consult that “best effort” means voicemail.
Tele-Stroke, Tele-Psych, Tele-ICU: Which Specialties Work in Rural Settings
Not every specialty translates equally to telehealth. Five specialty lines have demonstrated measurable rural outcomes; three remain difficult.
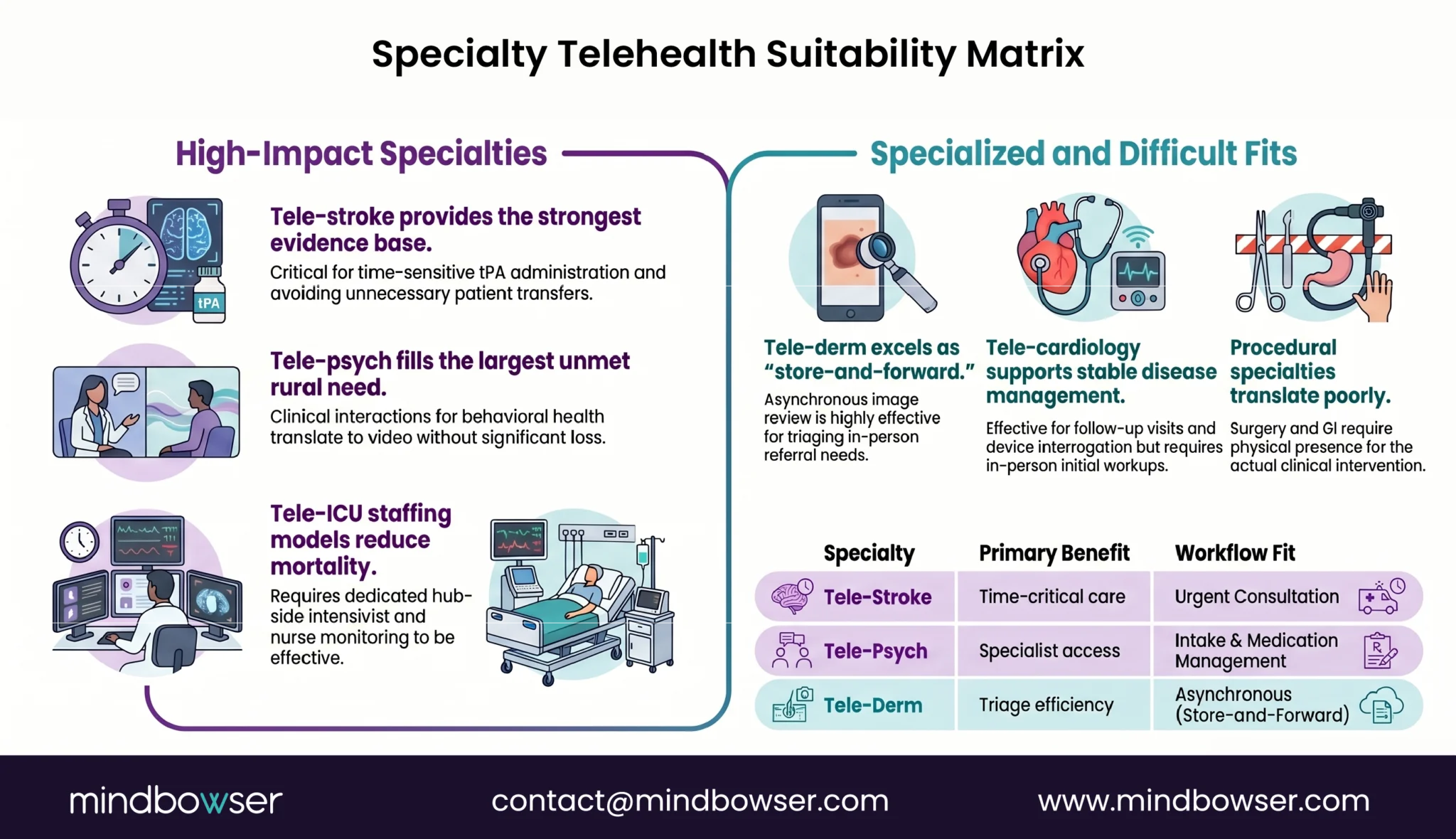
- Tele-stroke. Strongest evidence base. tPA administration windows are time-critical, neurologist availability in rural hospitals is near-zero, and the consult workflow (CT image review + bedside neuro exam via video) translates well to telehealth. Avoided transfers and improved tPA rates are well-documented. Coverage requires 24/7 hub commitment.
- Tele-psych. Strong evidence base, large unmet need. Behavioral health specialist supply is the binding constraint in most rural counties. Tele-psych intakes work well via video; medication management visits work well via audio-only. The clinical interaction translates without significant loss.
- Tele-ICU. Works where the hub has dedicated tele-ICU staffing (intensivist + critical care nurse monitoring multiple spokes). Reduces mortality in studies but requires hub investment in the staffing model. Not viable as a side activity for the hub’s daytime intensivists.
- Tele-derm. Works well as store-and-forward (patient or PCP submits images, dermatologist reads asynchronously). Triages in-person referral need. Synchronous tele-derm video is rarely necessary.
- Tele-cardiology. Works for follow-up visits, device interrogation review, and stable disease management. Initial workup and acute presentations still need in-person evaluation.
- Difficult specialties. Surgery, GI, and most procedural specialties translate poorly. Pre-op consultation can be telehealth, but the intervention itself requires presence. Pediatric subspecialty access is constrained by family logistics more than telehealth platform capability.
Hospitals that pick the right specialty mix for telehealth investment generate measurable outcomes. The ones that try to telehealth-enable every specialty equally dilute their investment and discover that surgery does not happen over video.
We help rural healthcare organizations implement reliable low-bandwidth telehealth and hub-and-spoke specialty access models.
Store-and-Forward and Asynchronous Telehealth for Rural Reality
Synchronous video gets the marketing attention. Asynchronous workflows produce more rural telehealth volume with fewer infrastructure requirements.
Store-and-forward means the originating site captures clinical data (images, video clips, measurements, history) and submits it to the consulting specialist for review at a later time. The specialist reviews and responds within a defined turnaround window (typically 24-72 hours). No live interaction. No bandwidth requirement during the consultation itself.
Where it works:
- Dermatology: images and history submitted, dermatologist reads, returns recommendation
- Radiology: routine reads to remote radiologists
- Wound care: serial images submitted, wound specialist tracks progression
- Ophthalmology: retinal screening images for diabetic retinopathy
- Pathology: digital slide review
Why it fits rural: asynchronous workflows tolerate intermittent connectivity, do not require scheduling alignment between rural patient and tertiary specialist, and reduce specialist no-show rates to zero (the specialist reads when available, not when scheduled).
Reimbursement. CMS reimburses store-and-forward in specific clinical contexts (primarily teledermatology and teleophthalmology) and continues to expand coverage. State Medicaid coverage varies. Commercial coverage is narrower than synchronous.
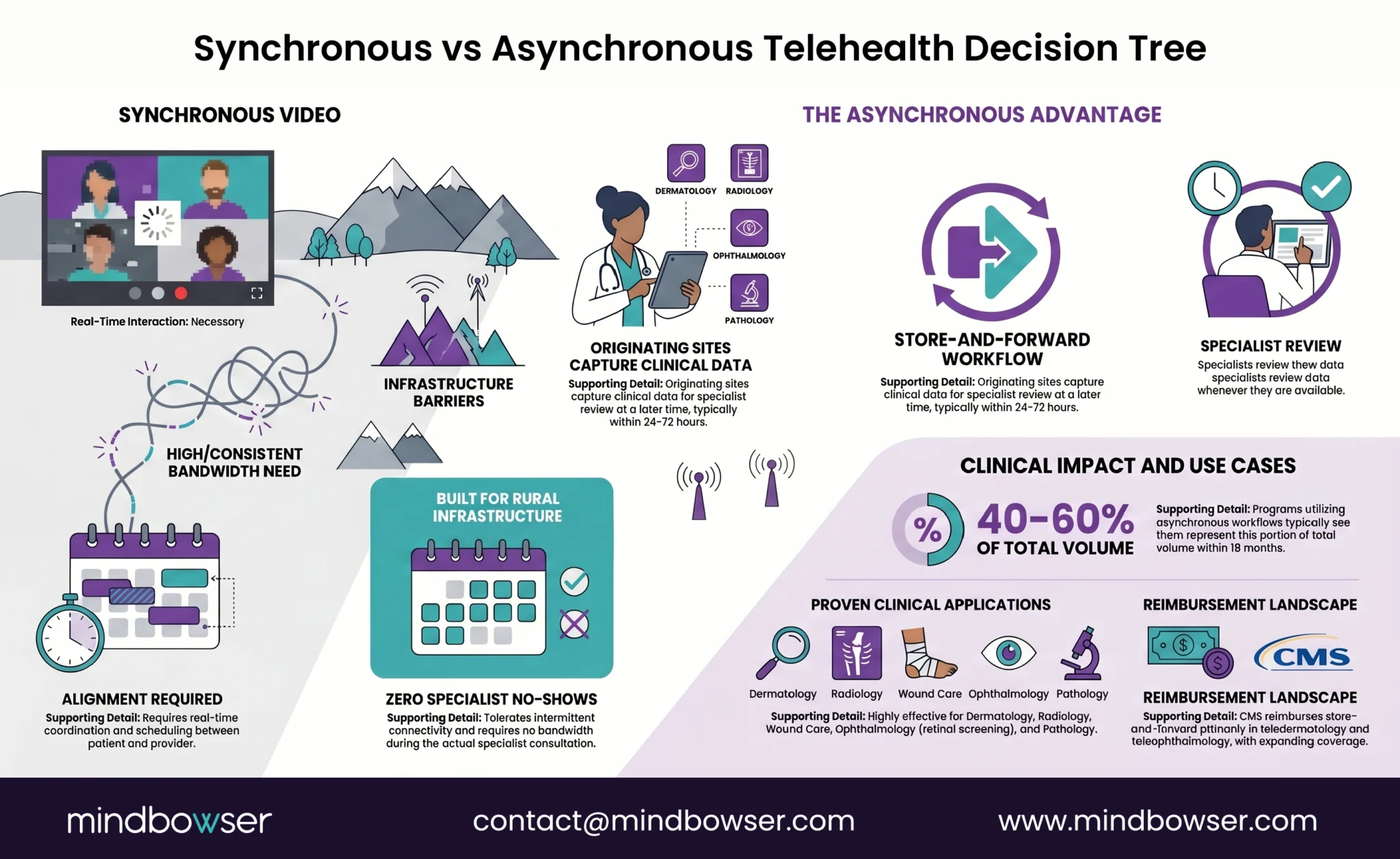
Rural telehealth programs that build asynchronous workflows alongside synchronous video typically see asynchronous represent 40-60 percent of total telehealth volume within 18 months. The programs that focus exclusively on synchronous video underutilize their telehealth investment.
Rural Telehealth Reimbursement: What CMS Covers and What Commercial Payers Don’t
Reimbursement is where rural telehealth deployments most often miscalculate revenue. Three payer categories operate by different rules.
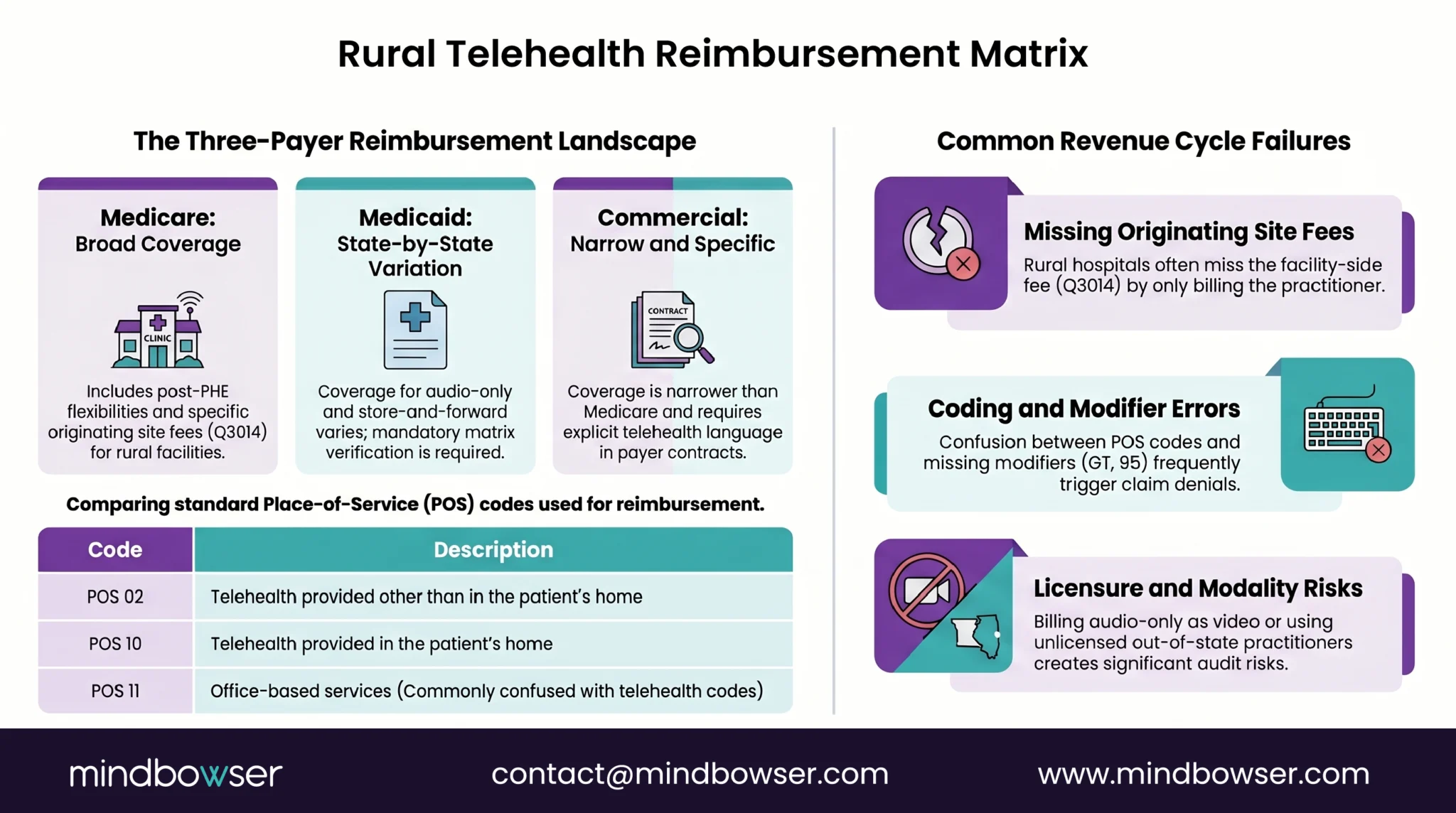
- Medicare. Broad coverage of telehealth services post-PHE flexibilities, with continuing CMS Physician Fee Schedule updates. Originating site fee (Q3014) covers the rural facility. Distant site fee covers the practitioner. POS 02 (telehealth provided other than in patient’s home) and POS 10 (telehealth provided in patient’s home) are the standard place-of-service codes. Audio-only is reimbursable for specific codes. Federally Qualified Health Centers and Rural Health Clinics have separate reimbursement structures with their own rules.
- Medicaid. Coverage varies by state. Most state Medicaid programs cover synchronous video; fewer cover audio-only; fewer still cover store-and-forward. Parity laws require equivalent reimbursement to in-person visits in some states, allow lower telehealth rates in others. State-by-state reimbursement matrix verification is mandatory before deployment, not optional.
- Commercial. Coverage is narrower than Medicare. Parity laws apply in most states but include exceptions, scope limits, and cost-sharing variations. Commercial payer contracts need explicit telehealth language; default contract terms often exclude or limit telehealth.
Common revenue cycle failures:
- Wrong place-of-service code. POS 02 vs POS 10 vs POS 11 confusion creates denials.
- Missing modifiers. GT (synchronous telehealth via interactive audio/video) and 95 (synchronous telehealth) requirements vary by payer.
- Originating site fee not billed. Rural hospitals frequently bill the practitioner side and miss the facility-side originating site fee.
- Audio-only billed as video. Triggers audit risk and post-payment recoupment.
- State licensure mismatch. Distant site practitioner not licensed in patient’s state. Telehealth does not waive state licensure requirements except under specific compact arrangements.
Hospitals that deploy telehealth without revenue cycle scoping discover the reimbursement gaps in month three. The gaps are knowable in advance with payer-by-payer contract review and CMS guidance walkthrough.
FCC Rural Health Care Program and USDA Grants: Broadband Infrastructure Funding
The constraint that rural telehealth most often hits is the broadband connection itself. Two federal programs subsidize the infrastructure.
FCC Rural Health Care Program (RHCP). Provides discounts on telecommunications and broadband services for eligible rural healthcare providers. Two sub-programs:
- Healthcare Connect Fund. 65 percent discount on broadband services for rural healthcare providers participating in a consortium.
- Telecommunications Program. Discount that brings rural rates to urban-equivalent rates for telecommunications services used for healthcare.
Eligible providers include rural public or non-profit hospitals, rural health clinics, Critical Access Hospitals, community mental health centers, and others. Application is annual through USAC. Funding is uncapped but subject to FCC budget adjustments.
USDA Distance Learning and Telemedicine (DLT) Grants. Capital grants for telecommunications-enabled equipment and infrastructure. Funds telehealth carts, peripherals, video endpoints, and the network infrastructure connecting rural sites to specialist hubs. Grant range typically $50,000-$1,000,000. Requires matching funds (15 percent for most applicants).
Stacking with RHTP. RHTP funds can pay for telehealth program operations, clinical staffing, training, and software platforms. FCC RHCP pays for the broadband connection. USDA DLT pays for the equipment. The three programs stack legitimately when scoped correctly. The stacking is rarely used because few rural hospitals have grant capacity or technology partner support to pursue all three concurrently.
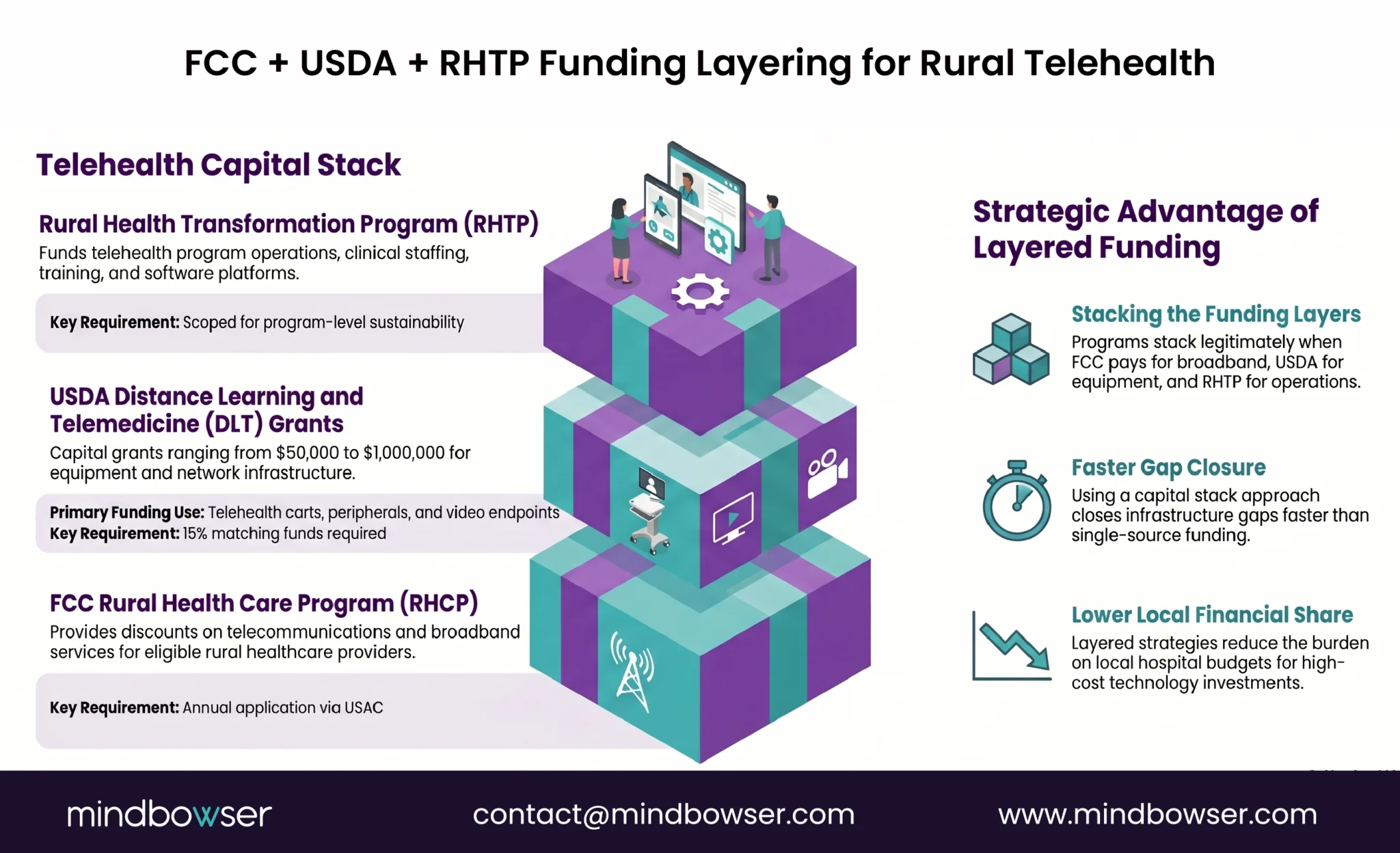
The hospitals that build their rural telehealth funding strategy as a layered capital stack rather than a single funding source close their broadband and equipment gaps faster and at lower local share.
Where Rural Telehealth Deployments Fail (and How to Avoid It)
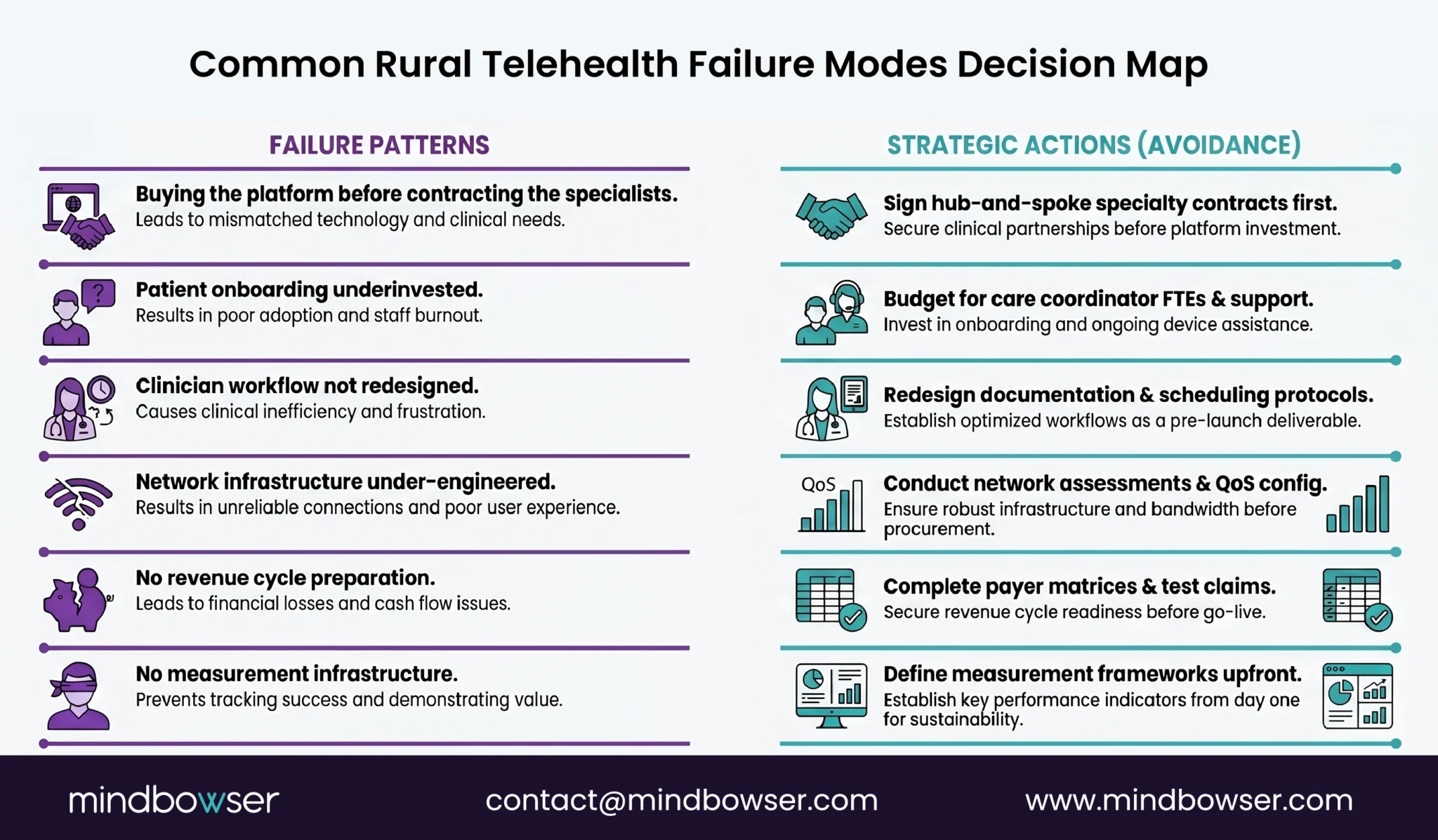
Six failure patterns recur across rural telehealth deployments we have seen.
- Failure 1: Buying the platform before contracting the specialists. The platform is licensed, deployed, and trained on. There is no specialist on the other end. The platform sits unused while the contract auto-renews.
- Avoidance: Sign hub-and-spoke specialty contracts before signing the platform contract. The platform should be selected based on the hub’s preferred infrastructure where possible.
- Failure 2: Network infrastructure under-engineered. The deployment assumes the existing internet circuit will carry telehealth traffic. The first multi-concurrent-visit afternoon proves otherwise.
- Avoidance: Network assessment before procurement. Bandwidth headroom, QoS configuration, jitter measurement, cellular fallback architecture all designed before clinicians use the platform.
- Failure 3: No revenue cycle preparation. Charge capture, code selection, modifier application, and payer contract terms are figured out after the first claims start denying.
- Avoidance: Revenue cycle workflow design and payer-by-payer reimbursement matrix completed in parallel with platform selection. Test claims before go-live.
- Failure 4: Patient onboarding underinvested. The platform assumes patients self-onboard. Rural patient demographics and digital literacy do not support that assumption. Adoption stalls.
- Avoidance: Care coordinator FTE allocation for patient onboarding, family caregiver training, and ongoing device support. Budget the staffing as part of the program, not as overhead.
- Failure 5: Clinician workflow not redesigned. Telehealth visits are bolted onto existing in-person workflows. Clinicians do double documentation, scheduling becomes chaotic, and adoption resistance builds.
- Avoidance: Clinical workflow redesign as a project deliverable. Documentation templates, scheduling protocols, intake processes, and follow-up workflows all redesigned for telehealth before launch.
- Failure 6: No measurement infrastructure. The deployment runs for 18 months without reliable utilization, clinical outcome, or financial performance data. Renewal decisions are made on anecdote.
- Avoidance: Measurement framework defined upfront. Visit volume, completion rates, no-show rates, clinical outcomes by specialty line, revenue per visit, and avoided transfer counts tracked from day one.
The hospitals that have functioning rural telehealth programs in 2026 worked through all six failure modes during planning. The ones that bought platforms first and figured out the rest later are the case studies vendors do not feature.
How RHTP Funding Changes Rural Telehealth Economics
The Rural Health Transformation Program ($50 billion across 50 states, FY2026-FY2030) is the largest rural healthcare capital injection in a generation. Telehealth is a named or implicitly funded activity in most state RHTP plans we have reviewed.
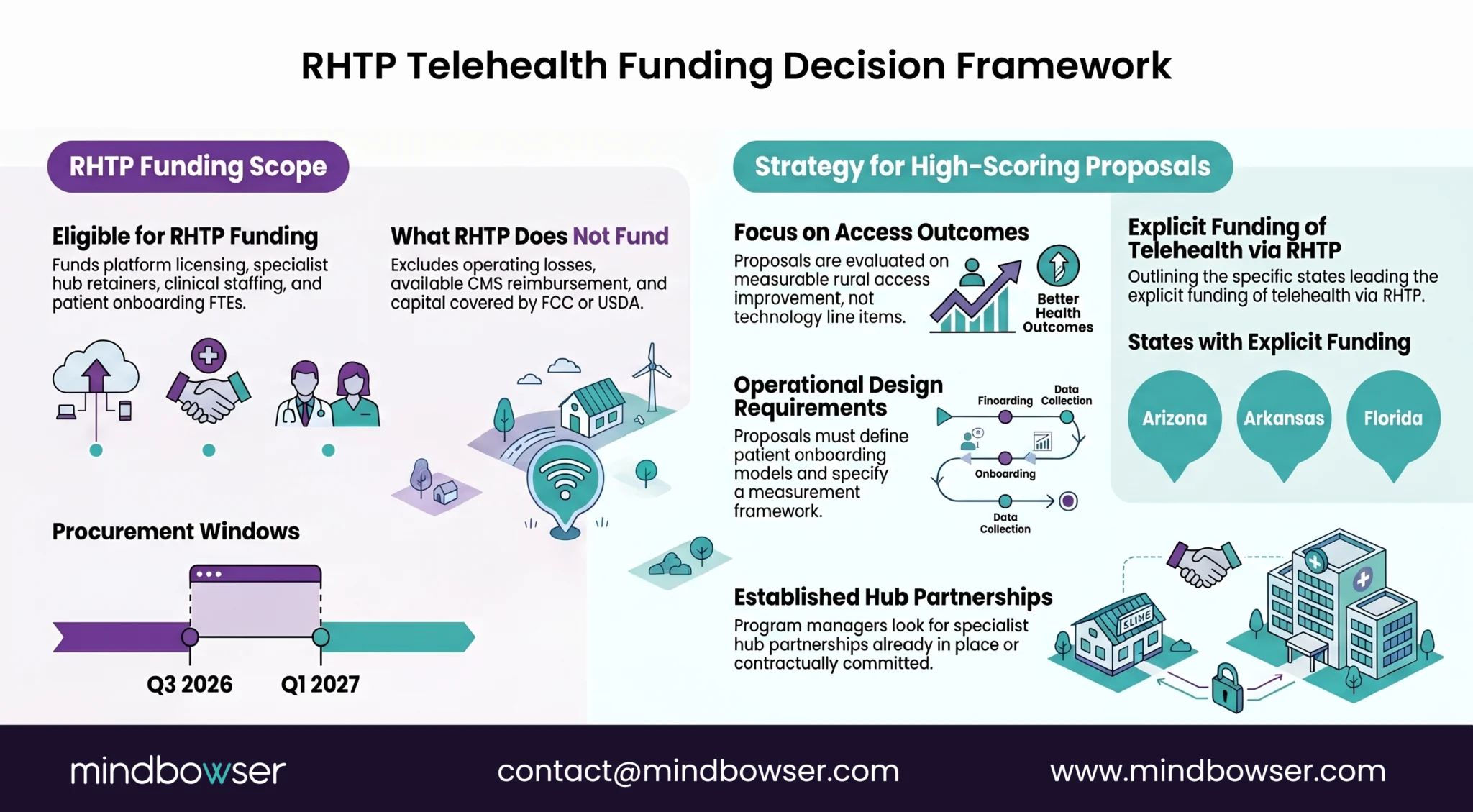
States explicitly funding telehealth activities in their RHTP plans include Arizona, Arkansas, Maine, Florida, and Utah; many others include telehealth under broader rural infrastructure or specialty access initiatives. The procurement windows opened Q3 2026 and extend into Q1 2027.
What RHTP funds for rural telehealth:
- Platform licensing and deployment capital
- Specialist hub contract retainers
- Clinical staffing for telehealth program operations
- Patient onboarding and care coordination FTEs
- Network upgrades not covered by FCC RHCP
- Measurement and quality reporting infrastructure
What RHTP does not typically fund:
- Operating losses on telehealth lines that should be self-sustaining via reimbursement
- Replacement of CMS reimbursement that is already available
- Capital that should come from FCC RHCP or USDA DLT
The rural hospitals positioning for RHTP telehealth funding are scoping their applications as integrated rural specialty access programs rather than as platform purchases. State RHTP program offices are evaluating proposals on measurable rural access improvement, not on technology line items.
State RHTP program managers evaluating telehealth proposals are looking for: specialist hub partnerships already in place or contractually committed, network infrastructure assessments completed, revenue cycle workflow scoped, patient onboarding model defined, and measurement framework specified. Proposals that present “buy a telehealth platform” without the surrounding operational design get scored low.
The RHTP procurement window is the funding event that closes the rural telehealth gap for hospitals that scope their programs honestly. It is also the event that funds platforms-without-programs for hospitals whose state RHTP offices do not screen rigorously. The first cohort of awards in Q4 2026 will reveal which states screened well.

How Mindbowser Helps Rural Hospitals Deploy Telehealth
Mindbowser builds the telehealth infrastructure rural hospitals need to make video visits, store-and-forward consults, and hub-and-spoke specialty access work under real rural network conditions.
Our accelerator stack maps to the operational components rural telehealth deployments need:
- HealthConnect CoPilot: FHIR-based integration between telehealth platforms, EHRs, and care coordination workflows. Connects the rural hospital’s Epic, Meditech, or athenahealth EHR to the telehealth platform and to the specialist hub’s systems.
- AI Medical Summary: Clinical encounter documentation automation for telehealth visits. Reduces clinician documentation burden that otherwise becomes the dominant adoption barrier.
- PHISecure: HIPAA-compliant cloud infrastructure for telehealth video, store-and-forward, and patient data transmission.
- WearConnect: Device data ingestion when telehealth visits incorporate remote monitoring data.
We deploy these as integrated components of a working rural telehealth program, not as standalone software. The integration work, network assessment, revenue cycle workflow design, and hub partnership facilitation are part of the engagement.
For state RHTP program offices, we provide technology partner capability for telehealth activities funded under state plans. Our positioning aligns with the operational rigor RHTP screening favors.
Yes, with the right architecture. H.265/HEVC codecs at 384-512 kbps support usable video at 1.5-2 Mbps. Audio-only and store-and-forward workflows tolerate even lower bandwidth. Adaptive bitrate, jitter buffer tuning, and bonded cellular fallback close the rest of the gap.
A rural hospital (spoke) contracts with an academic medical center or large health system (hub) for specialty consultation services across multiple specialties under one agreement. The hub commits to coverage windows; the spoke routes consultations through the hub’s intake. It works because it solves specialist supply, not just connectivity.
Tele-stroke, tele-psych, and tele-ICU have the strongest evidence base. Tele-derm and tele-radiology work well asynchronously. Cardiology follow-up, infectious disease consultation, and behavioral health all translate. Surgery and procedural specialties do not.
Broadly, yes. Medicare covers synchronous video, audio-only for specific codes, and store-and-forward in defined clinical contexts. Originating site fees apply at the rural facility. Coverage continues to evolve through the CMS Physician Fee Schedule. Code-by-code verification is required.
Coverage and parity vary by payer, plan, and state law. Most states have telehealth parity laws, but with exceptions and limitations. Commercial parity is generally narrower than Medicare. Payer-by-payer contract review is required before deployment.
A federal program providing broadband and telecommunications subsidies to eligible rural healthcare providers. The Healthcare Connect Fund offers a 65 percent discount on broadband services for consortium-participating providers. The application is annual through USAC.
Yes. Most state RHTP plans we have reviewed include telehealth as a named or implicitly funded activity. RHTP can fund platform deployment, hub contract retainers, clinical staffing, care coordination FTEs, and program operations. Procurement windows opened Q3 2026 and extend into Q1 2027.
