



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 
























TL;DR
- COPD killed 141,733 Americans in 2023 (CDC NCHS Data Brief #529, April 2025) and costs the healthcare system $31.3 billion a year in direct medical expenses (CHEST Journal). It is the #2 chronic condition for RPM by patient volume, right behind heart failure.
- Yet almost every RPM program skips it. SpO2 trending is the single most predictive remote biomarker for COPD exacerbation prediction (JMIR systematic review, 2024).
- CMS reimburses COPD RPM identically to cardiac RPM through CPT 99453-99458, generating $160-220 per patient per month. The monitoring protocol is messier than heart failure. That is exactly why the programs that figure it out will own the market.
Heart failure gets all the RPM attention, and I get why: weight scale plus blood pressure cuff, clean protocol, well-documented billing. But 141,733 Americans died from COPD in 2023, and most RPM programs don’t monitor a single one of them.
I’ve spent the last two years watching RPM programs launch with heart failure, hit their stride at month six, and then stall. The clinical team asks, “What’s next?” and someone suggests COPD. Then the conversation dies. The device protocol is more complex. The evidence base is thinner. The payer environment just got murkier with UnitedHealthcare’s 2026 rollback.
But here’s what I keep coming back to: COPD patients are the ones showing up in the ER at 2 a.m. because nobody caught the SpO2 drop that started trending three days earlier. That is a monitoring problem. And monitoring problems have monitoring solutions.
Why Does Every RPM Program Start with Heart Failure and Stop There?
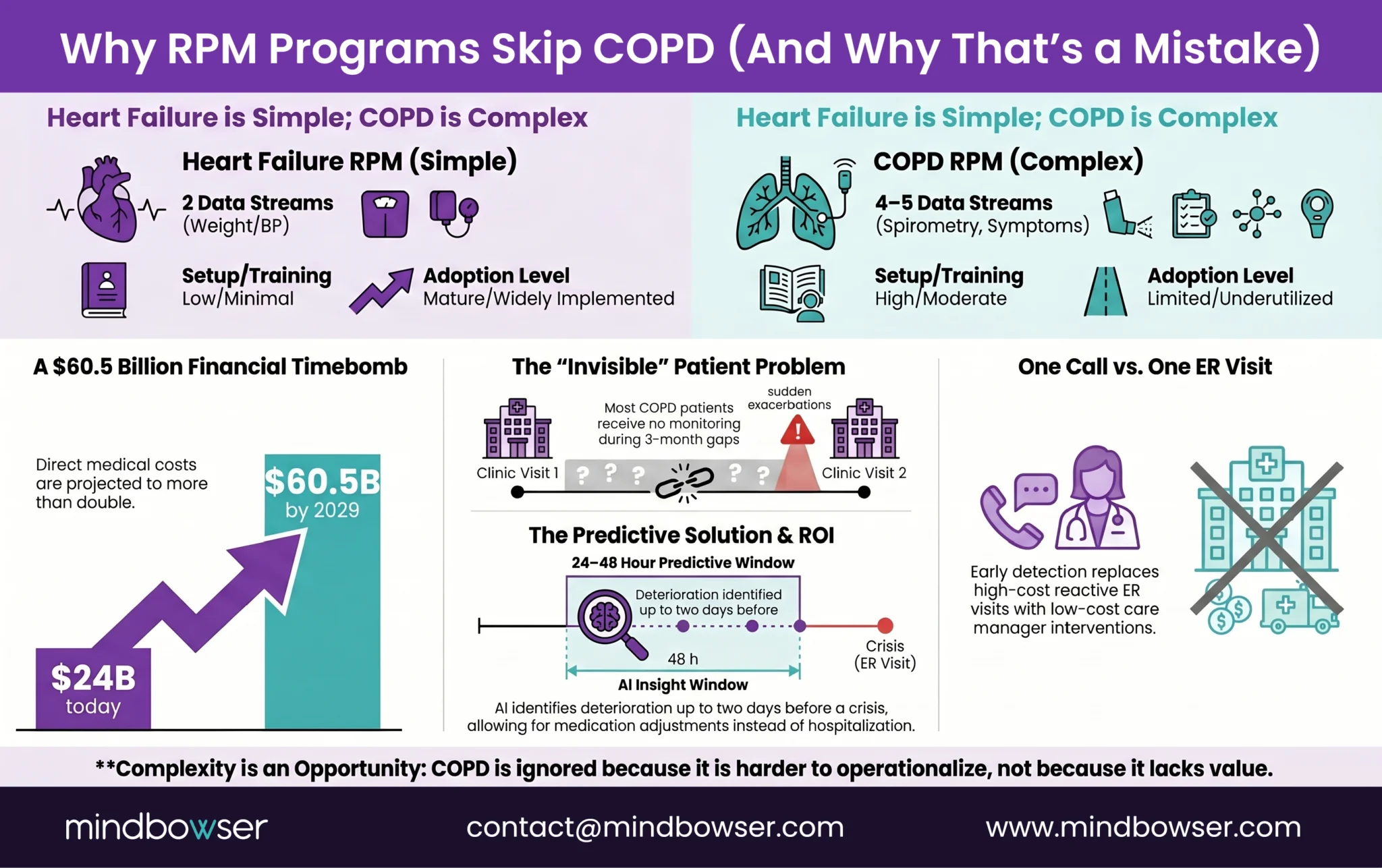
The answer is protocol simplicity. Heart failure RPM runs on two devices: a weight scale and a blood pressure cuff. Patient steps on the scale every morning, takes a BP reading, and data flows to the care team. Clean. COPD RPM needs four or five data streams: pulse oximetry, spirometry, respiratory rate, activity levels, and symptom questionnaires. Each one adds a device, a patient training step, and an alert threshold to configure.
The numbers make the case for building anyway. The CDC’s April 2025 data brief puts age-adjusted COPD prevalence at 3.8% of US adults. Among people 75 and older, it jumps to 10.5%. That’s 141,733 deaths a year, making COPD the fifth leading cause of death in the United States. The American Lung Association estimates $24 billion in annual medical costs for adults 45 and older. CHEST Journal projects direct medical costs will nearly double to $60.5 billion by 2029.
Those numbers represent patients who are largely unmonitored between quarterly clinic visits. ConnectHealth ships the device integration layer for this: Apple HealthKit, BLE medical devices, Fitbit, Dexcom APIs normalized into a single data pipeline. The integration that would take six months of custom BLE development ships in weeks.
At the BRI Network 2026 summit, which our founder, Ayush Jain, attended, Sandra Elliott from Hackensack Meridian Health presented data showing AI can predict clinical deterioration 24 to 48 hours before it becomes an emergency. That finding changes the COPD calculus entirely. If you can see the exacerbation coming two days out, a care manager phone call replaces an ER visit. One call. That is the whole argument for COPD RPM.
What Devices Does a COPD RPM Program Actually Require?
I’ll be direct about this: you don’t need five devices on day one. Start with two. Add more as the program matures.
- Pulse oximeters are non-negotiable. The JMIR 2024 systematic review of RPM and machine learning in COPD exacerbations found that SpO2 emerged as the most useful parameter for predicting exacerbations when combined with ML algorithms. Not respiratory rate. Not spirometry. SpO2. But continuous trending matters here, not spot checks. A single reading tells you almost nothing. A three-day trend tells you everything.
- Spirometers for home-based FEV1 and FVC tracking are the clinical gold standard for COPD monitoring. The problem is patient compliance. Blowing into a spirometer correctly takes coaching, and many COPD patients (especially the elderly) struggle with the technique. Programs that launch with spirometry first often see compliance drop below 40% by month three.
- Respiratory rate monitors are getting better. Wearable chest patches and some newer smartwatches now track respiratory rate continuously. This is the data stream I’m most excited about for COPD, because respiratory rate changes tend to precede SpO2 changes during exacerbation onset.
- The Strados Labs RESP Biosensor deserves mention: it’s FDA-cleared for continuous lung sound monitoring (cough frequency, wheeze detection). This is genuinely new technology. Continuous auscultation from a wearable was science fiction five years ago.
- Activity trackers provide a proxy for the 6-minute walk test through daily step counts and activity patterns. npj Digital Medicine published a 2023 meta-analysis showing wearable technology improved daily step count by 850 steps per day in COPD patients, with a clinically meaningful effect size of 0.42.
- Smart inhalers (Propeller Health, Teva DigiHaler) track medication adherence and inhaler technique. Useful but not essential for the monitoring layer.
My recommendation: launch with pulse oximeter plus a symptom questionnaire app (CAT score or mMRC dyspnea scale). Add spirometry and activity tracking at month three. Add respiratory rate monitoring or lung sound monitoring when the program hits 100+ patients and needs AI triage to manage alert volume.
Get the Print-Ready COPD Device Checklist
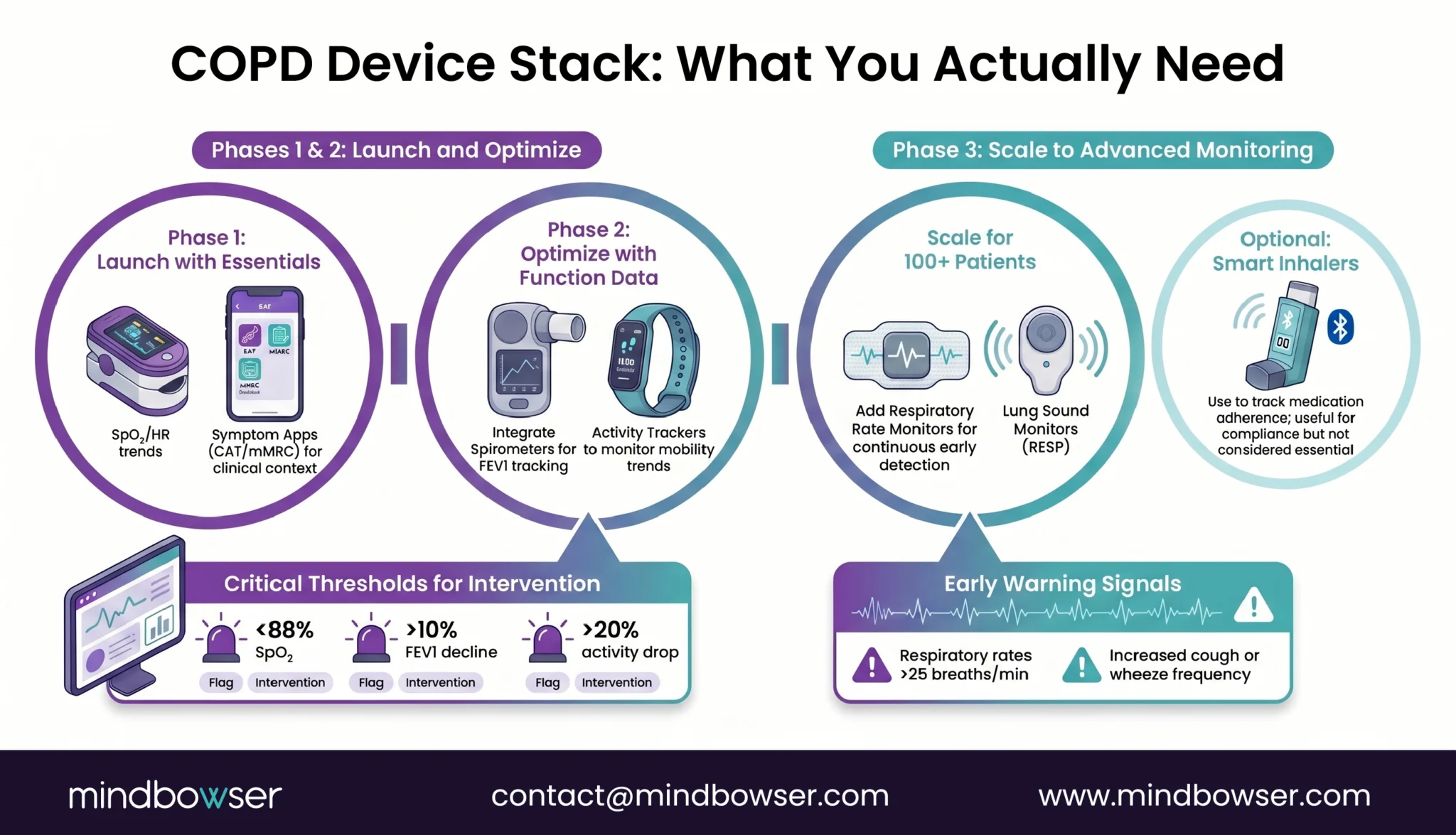
Figure 2: COPD Remote Monitoring Architecture
What SpO2 Thresholds Actually Predict COPD Exacerbations?
This is where most COPD RPM programs get it wrong, and I include early programs I advised in that statement.
The standard approach: set SpO2 alerts at 88% (critical) and 90% (warning), respiratory rate alerts at 25 breaths per minute, and wait. The problem is that COPD patients have wildly different baselines. A patient with severe COPD might live at a baseline SpO2 of 89-91%. Setting a population-wide threshold at 90% means that patients’ monitors scream every single day. By week two, the care team stops looking at COPD alerts. By month two, the program is effectively dead for that patient.
The JMIR 2024 systematic review confirmed what clinical practice has been showing for years: SpO2 is the most useful predictor, but only when combined with machine learning on personalized baselines. The Lancet eBioMedicine published a 2024 study on continuous wearable characterization of exacerbation pathophysiology in free-living COPD outpatients. Their finding: detectable physiological changes appear 2 to 4 days before exacerbations become clinically severe. But those changes are relative to the individual patient’s baseline, not to a population threshold.
Actually, let me refine that. The issue isn’t just personalized thresholds. It’s personalized trend detection. A patient whose SpO2 drops from 94% to 91% over 48 hours is in a different risk category than a patient who’s been stable at 91% for three months. Same number. Completely different clinical meaning. Static thresholds can’t distinguish between these two patients. ML models trained on individual patient data can.
This is where the false alarm problem becomes a program design problem. Without AI triage, a 200-patient COPD panel generates hundreds of alerts daily. Nicole Speeny’s presentation at that same summit on clinician burnout through RPM workflows made this point clearly: care teams don’t burn out from caring for patients. They burn out from triaging noise. A monitoring system that learns each patient’s normal and flags deviations from their personal baseline, not from a population average, cuts false alarms by 60 to 80%.
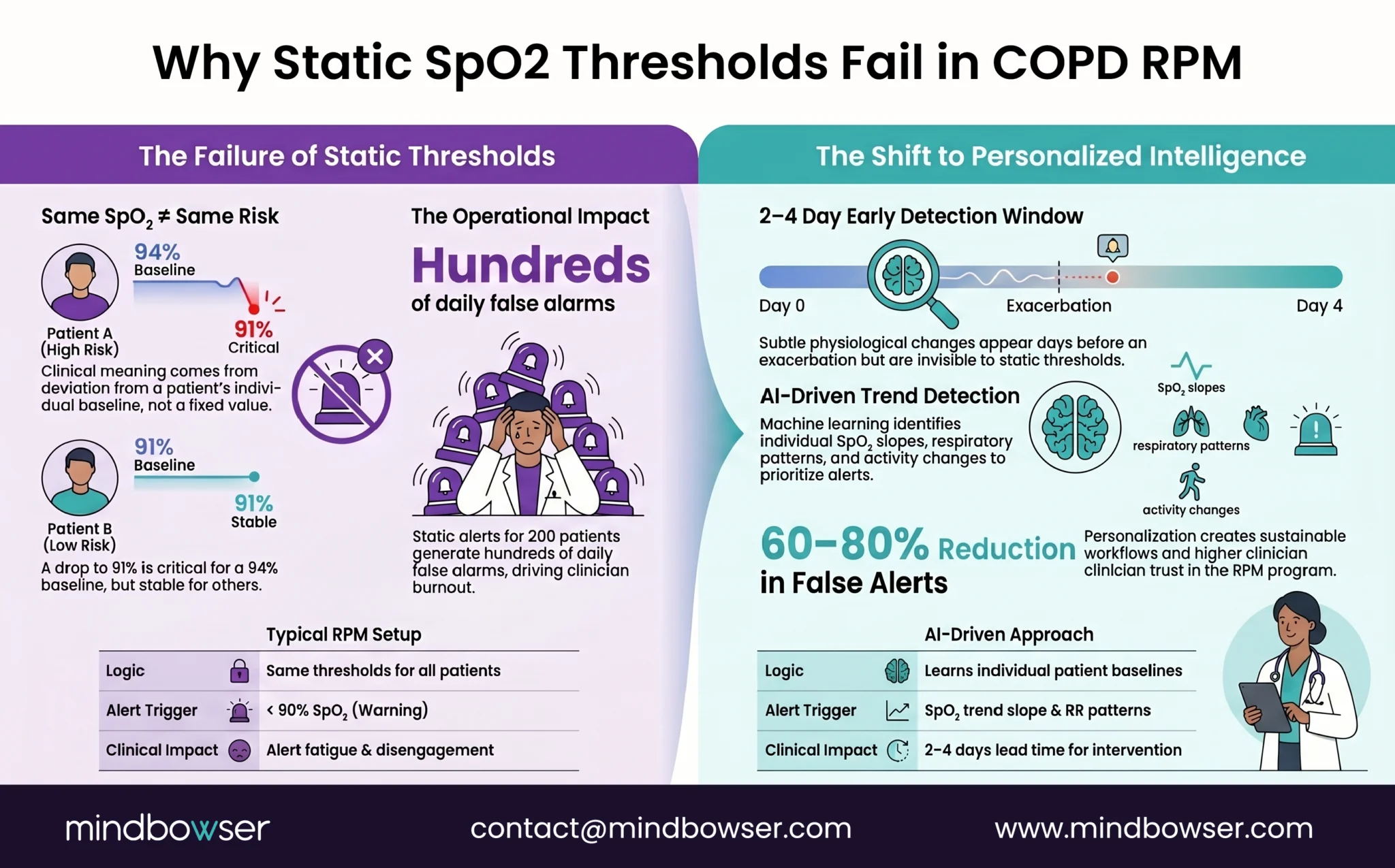
RPMCheck AI is built for exactly this pattern: anomaly detection that learns individual patient baselines and triages alerts before they reach the care team. For COPD specifically, it watches the SpO2 trend slope (not just the absolute value), respiratory rate patterns, and activity level changes as a composite risk score.
How Does CMS Reimburse COPD RPM in 2026?
The billing structure for COPD RPM is identical to heart failure RPM. Same CPT codes, same rates, same rules. This is the part that surprises every CFO I talk to: the reimbursement doesn’t discriminate by condition.
Core RPM CPT codes:
- 99453 (device setup and patient education, one-time): ~$19-21
- 99454 (device supply with daily recordings, monthly): ~$55-64
- 99457 (first 20 minutes of interactive communication per month): ~$50-58
- 99458 (each additional 20 minutes): ~$42-48
2026 changes to know:
- 99453 now requires a minimum of 2 days of monitoring data before it can be billed (changed from prior year)
- New codes 99445 and 99470 expand remote service billing options
- RTM codes 98979, 98984, and 98985 have a 2-day monitoring minimum instead of the traditional 16-day RPM minimum. This matters for COPD: patients who are inconsistent with their monitoring (and many COPD patients are) can still generate billable events under RTM
Revenue math:
A COPD patient on 99457 + 99454 generates roughly $105-122 per month. At 200 patients enrolled, that’s $252,000 to $292,800 per year from RPM alone. Add concurrent CCM enrollment (CPT 99490, ~$62/month) on the same patients, and you’re looking at $167-184 per patient per month combined. Two hundred patients at that rate: $400,000 to $441,600 annually.
Now the honest caveat. Starting January 1, 2026, UnitedHealthcare dramatically scaled back RPM coverage. RPM is now only billable for heart failure and gestational hypertension under UHC plans. COPD is excluded. This is significant because UHC covers roughly 50 million Americans.
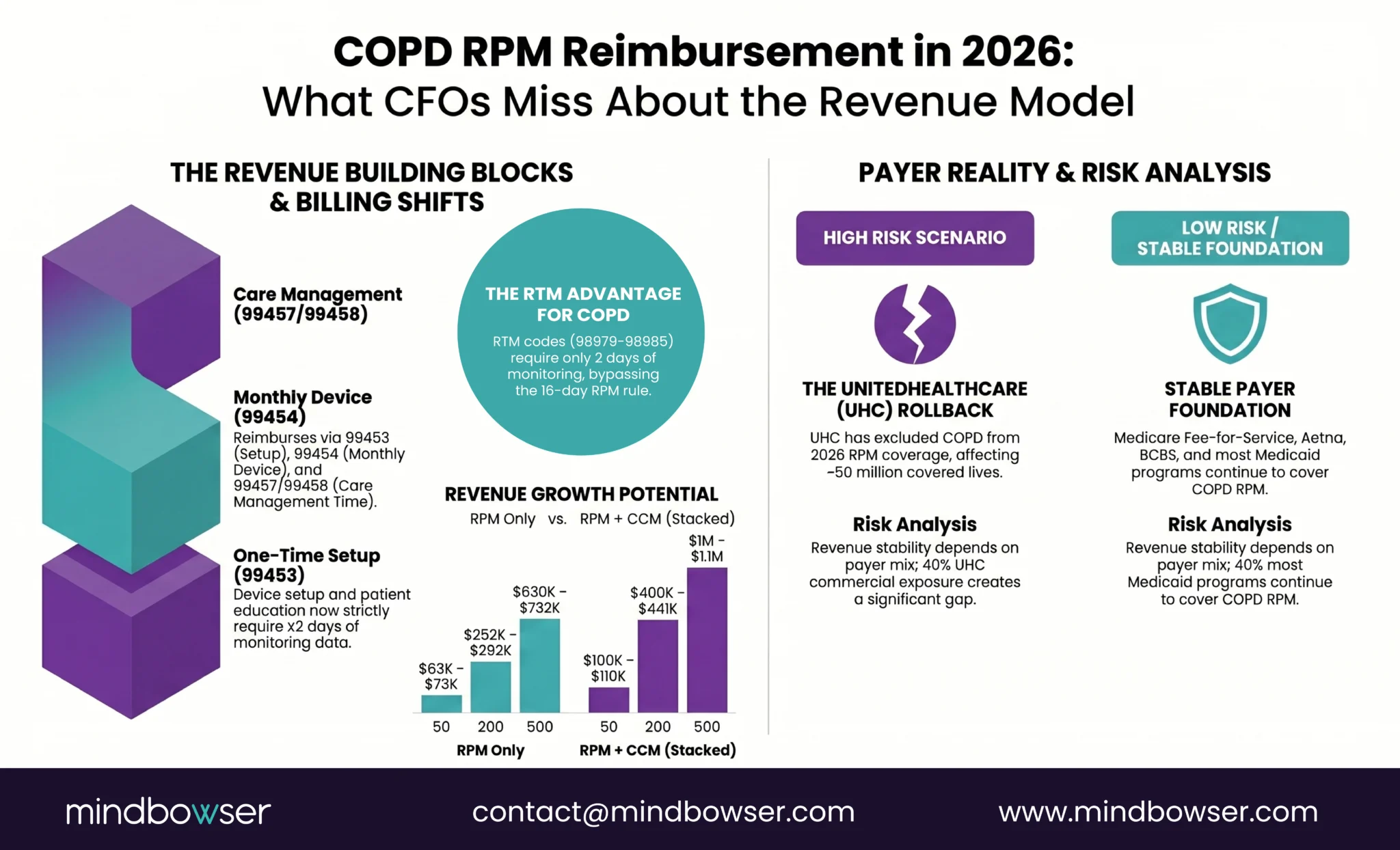
But Medicare fee-for-service still covers COPD RPM. So do Aetna, BCBS, and most state Medicaid programs. Before projecting revenue, run your payer mix. A program where 70% of COPD patients are on Medicare FFS is minimally affected by the UHC rollback. A program where 40% are on UHC commercial plans has a real revenue gap to account for.
Talk to our team about what a custom COPD RPM platform looks like for your organization
What Does a COPD RPM Care Team Workflow Look Like Day to Day?
The workflow question is where COPD RPM either scales or collapses. I’ve seen both outcomes, and the difference is never the device. It is always the workflow design.
- Daily (automated): SpO2 readings and respiratory rate data flow into the monitoring platform. AI triage scores every patient’s readings against their personal baseline and flags deviations. Green means stable. Yellow means watch. Red means call today. Without this triage layer, a 200-patient COPD panel throws off 300 or more alerts per day. With it: 15 to 30 actionable alerts.
- Weekly: Care manager reviews yellow-flagged patients, checks medication adherence data from smart inhalers, and conducts 99457 interactive communication calls. These calls are the billing backbone: 20 minutes of documented interactive time per patient per month.
- Monthly: Physician reviews AI-generated trend reports, adjusts care plans, reconciles medications. This is also when the program coordinator reviews enrollment numbers, compliance rates, and alert accuracy.
- Quarterly: Full spirometry review (home-based or in-clinic), pulmonary rehabilitation progress assessment, smoking cessation check-in. These are the clinical anchors that RPM data feeds into but doesn’t replace.
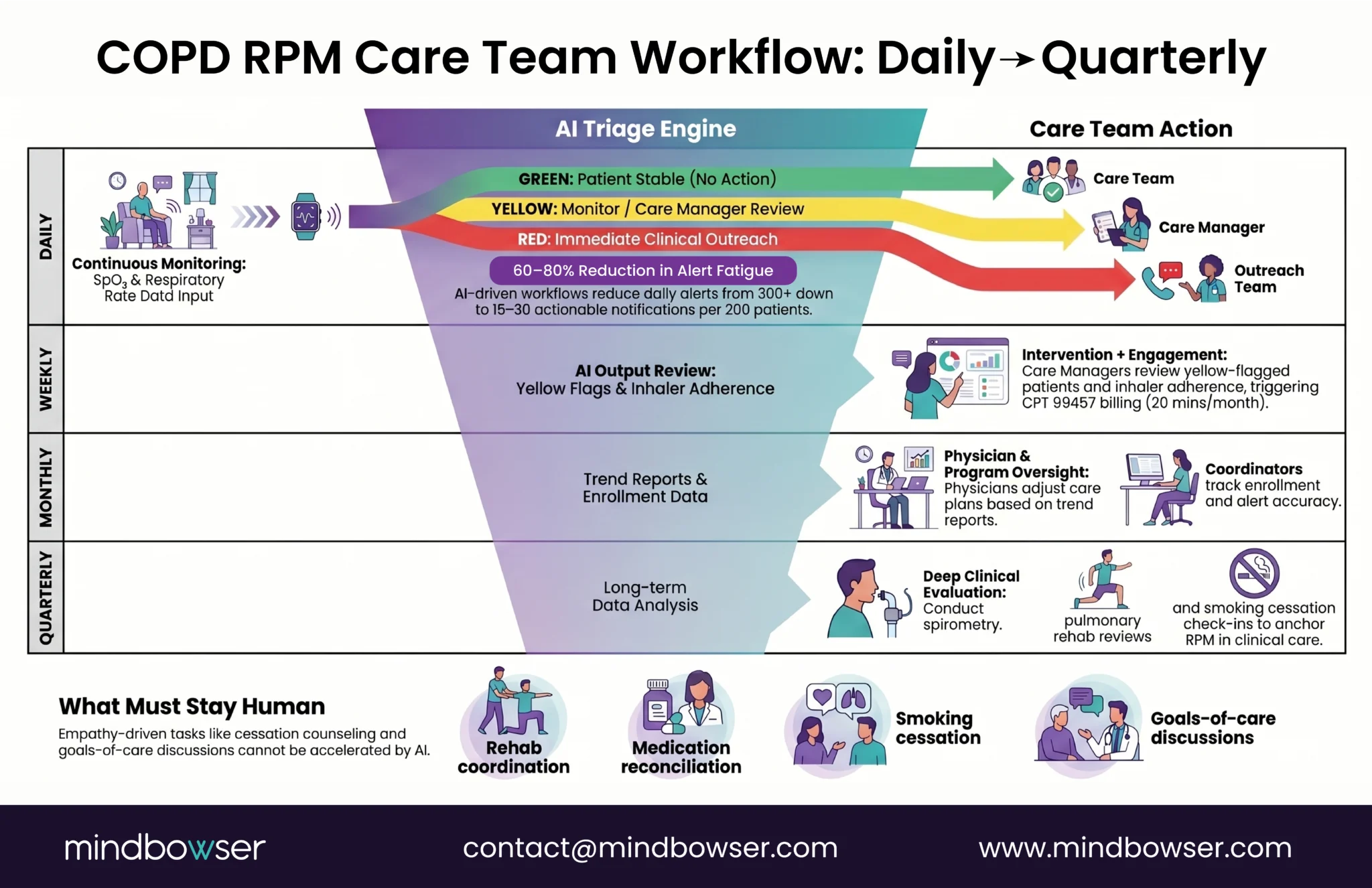
The steps that stay human and should stay human: pulmonary rehabilitation coordination, medication reconciliation during acute changes, smoking cessation counseling, goals-of-care conversations. There is no accelerator for empathy in a cessation conversation. Nor should there be.
Can You Predict a COPD Exacerbation Before It Hits the ER?
The short answer is: increasingly yes, and the prediction window is getting wider.
The Lancet eBioMedicine published a 2024 study that continuously characterized exacerbation pathophysiology using wearables on free-living COPD outpatients. Their core finding: physiological changes (SpO2 decline, respiratory rate elevation, activity reduction) become detectable 2 to 4 days before exacerbations reach clinical severity. That’s a window. Two to four days where a care manager phone call can prevent an ER visit that costs the system $10,000 to $30,000.
Sandra Elliott’s work at Hackensack Meridian Health, presented at BRI Network 2026, narrows the window further for AI-assisted prediction: 24 to 48 hours of advance warning when ML models are trained on individual patient baselines. One line from her talk our team kept coming back to: “Innovation without governance is just noise.” The prediction models work. The question is whether your program infrastructure can act on what they find.
I need to be honest about the evidence base here. A JMIR 2025 systematic review and meta-analysis of digital health interventions for COPD concluded there is “insufficient generalizable evidence to confidently advocate for replacing conventional management strategies” with digital health tools. The evidence is building, not built. Programs launching COPD RPM today are early movers, not followers of established protocols.
But early movers are exactly who capture the outcomes data that justifies continued investment. And the clinical logic is straightforward: if you can see SpO2 trending down 3% from a patient’s personal baseline over 48 hours, you don’t need a randomized controlled trial to tell you that patient needs a call.
Our Health Monitoring Platform case study shows this architecture in practice: AI-driven vitals analysis with a 45% increase in patient interaction rates. The same data ingestion and anomaly detection pipeline that works for multi-device wearable monitoring applies directly to COPD trend detection.
Should You Build Custom COPD RPM or Buy Off-the-Shelf?
This depends on three things: your patient volume, your device complexity, and whether RPM data needs to live inside your EHR.
The off-the-shelf players in COPD RPM are familiar names: Health Recovery Solutions (HRS, ranked #1 by KLAS for RPM 2020-2023), CareSimple, Accuhealth, Tenovi. They do basic vitals collection well. HRS in particular has strong case study data (83% readmission reduction at Frederick Health, $5.1 million in cost savings). If you’re running a single-device program under 50 patients, off-the-shelf handles the job.
Where off-the-shelf breaks: multi-device data ingestion (you need SpO2 plus spirometry plus activity data flowing into one view), COPD-specific personalized baselines (most platforms use static thresholds), and EHR-native dashboards (most platforms require a separate portal the clinical team eventually stops checking).
Custom build makes sense when the program hits scale and complexity. Two hundred or more patients. Three or more device types. Multi-condition monitoring (a patient with COPD and diabetes and hypertension needs unified threshold logic, not three separate apps). EHR integration where RPM data appears as FHIR Observations inside Epic or Cerner, not in a separate tab.
ConnectHealth ships the device integration layer for this: Apple HealthKit, BLE medical devices, Fitbit, Dexcom APIs normalized into a single data pipeline. The integration that would take six months of custom BLE development ships in weeks.
Wellinks’ $25 million Series C raise for the “first-ever virtual integrated COPD solution” (Fierce Healthcare, 2022) validates the market thesis: condition-specific RPM platforms are where the investment is going. The generic RPM platform era is giving way to disease-specific builds.
What Should Your First 90 Days of COPD RPM Look Like?
I’ll break this into three phases. Every number here comes from programs I’ve helped design or observed at close range.
Days 1-30: Foundation
- Select devices: pulse oximeter (continuous) + symptom questionnaire app. Two devices. That’s it for launch
- Set up the data pipeline: device readings flowing into the monitoring platform. If you need EHR integration, ConnectHealth handles the RPM-data-to-EHR connection
- Train the care team: 4 hours of protocol training (alert thresholds, escalation pathways, documentation for 99457 billing)
- Enroll first 25 patients: start with patients who are highest risk (2+ exacerbations in the past 12 months) and highest compliance likelihood
- Configure initial alert thresholds: start with standard static thresholds (SpO2 <88% critical, <90% warning). You’ll personalize these in Phase 2
Days 31-60: Calibration
- Expect high false alarm rates. This is normal. The static thresholds will overfire for patients with lower baselines. Document the false alarm rate; you’ll need it as the baseline when you deploy personalized thresholds
- Refine the care team workflow: which alerts actually lead to clinical action? Which are noise? Adjust escalation rules based on 30 days of real data
- Billing setup: submit first 99453 claims (device setup), begin tracking interactive time for 99457 billing. Verify payer coverage for each enrolled patient (especially UHC commercial plans)
- Add spirometry for compliant patients who are comfortable with the technology
Days 61-90: Scale
- Deploy personalized baselines: ML models now have 60 days of patient-specific data to learn from. Switch from static thresholds to personalized anomaly detection
- First full 99457 billing cycle: 20 minutes of documented interactive communication per patient. This is where revenue starts flowing
- Measure outcomes: exacerbation rate compared to the 12 months prior, ER visit frequency, patient-reported symptom scores (CAT score trends)
- Decision point: at 25 patients with 60 days of data, you know whether to scale to 50, 100, 200
A note on engagement: TodayHealth achieved 90% engagement among elderly users in their RPM platform. Their secret wasn’t the device. It was design-first thinking: large buttons, simplified workflows, proactive care manager outreach in the first 14 days. COPD patients skew older (CDC: 10.5% prevalence in adults 75+). The same UX principles that work for elderly heart failure patients work for elderly COPD patients. Don’t design for tech-savvy 45-year-olds.
What Happens If You Don’t Build COPD Into Your RPM Program?
COPD patients keep showing up in the ER because nobody is watching the SpO2 trend between quarterly clinic visits. The billing revenue, $160 to $220 per patient per month, is identical to heart failure RPM. But almost nobody captures it for COPD.
UHC’s rollback makes this feel risky. I understand the hesitation. But Medicare FFS still covers it, and Medicare FFS is the dominant payer for the 75+ population where COPD prevalence hits 10.5%. The programs that start now build the outcomes data that justifies continued coverage across all payers.
The JMIR 2025 meta-analysis is honest: the evidence for digital health interventions in COPD is still building, not built. But the Lancet eBioMedicine 2024 data on wearable exacerbation characterization and Elliott’s 24-48 hour prediction window at HMH show where this is heading. The trajectory is clear even if the destination isn’t fully mapped.
A year ago I’d have said wait for stronger evidence before launching a COPD RPM program. After reviewing the wearable data from the Lancet eBioMedicine free-living cohort and reviewing the dozen RPM presentations our founder Ayush Jain, brought back from BRI Network 2026, I’ve stopped saying wait. The monitoring technology exists. The billing pathway exists. The clinical need has always existed.
If you’re running heart failure RPM and wondering whether COPD is next, I’d genuinely like to hear what’s holding you back. Reach out.
At minimum, a continuous pulse oximeter and a symptom questionnaire app (CAT score or mMRC dyspnea scale). As the program matures, add a home spirometer for FEV1/FVC tracking, an activity tracker for step count and mobility patterns, and optionally a respiratory rate monitor or lung sound sensor like the FDA-cleared Strados RESP Biosensor. Most successful programs start with two devices and scale to four or five over the first 90 days based on patient compliance data.
Yes. Medicare fee-for-service covers COPD RPM through the same CPT codes used for all RPM conditions: 99453 (device setup), 99454 (device supply), 99457 (interactive communication), and 99458 (additional time). The 2026 RTM codes (98979, 98984, 98985) with a 2-day minimum monitoring requirement also apply to COPD. The exception is UnitedHealthcare, which limited RPM coverage to heart failure and gestational hypertension starting January 2026. COPD is still covered by Medicare, Aetna, BCBS, and most state Medicaid programs.
Standard static thresholds set alerts at SpO2 below 88% (critical) and below 90% (warning). But static thresholds produce excessive false alarms for COPD patients with naturally lower baselines. The more effective approach is personalized baseline monitoring: ML models learn each patient’s normal SpO2 range and flag deviations from their individual pattern. A 3% drop from a patient’s personal baseline over 48 hours is clinically significant regardless of whether the absolute number is 91% or 87%.
Yes. CMS allows concurrent enrollment in RPM (CPT 99457/99458) and Chronic Care Management (CPT 99490) for the same patient. This stacks revenue to roughly $167 to $184 per patient per month combined. The key requirement is that documented time for each program must be distinct and not double-counted. COPD patients with multiple comorbidities (which is the majority) are natural candidates for concurrent program enrollment.
RPM alone (99457 + 99454) generates approximately $105 to $122 per patient per month. With concurrent CCM enrollment, total per-patient revenue reaches $167 to $184 per month. At 200 enrolled patients, that’s $252,000 to $441,600 annually depending on program structure. Revenue projections should account for payer mix, particularly the UHC exclusion of COPD from RPM coverage starting 2026.
RPM codes (99453-99458) require a minimum of 16 days of device data in a 30-day period and 20 minutes of treatment management time. RTM codes (98979, 98984, 98985) have a lower threshold: 2 days of monitoring minimum and 10 minutes of treatment management. For COPD patients who monitor inconsistently (common in the first month of enrollment, especially elderly patients learning new devices), RTM codes capture billable events that would be lost under the 16-day RPM minimum. In 2026, the new short-duration RPM code 99445 also drops to a 2-day minimum, partially closing this gap. Programs should evaluate which code set maximizes revenue for each patient’s monitoring pattern.
Emerging evidence suggests yes, with 2-4 day advance warning. A 2024 Lancet eBioMedicine study on continuous wearable characterization of COPD outpatients found detectable physiological changes (SpO2 decline, respiratory rate elevation, activity reduction) appearing 2-4 days before exacerbations reach clinical severity. Sandra Elliott’s research at Hackensack Meridian Health (presented at BRI 2026) demonstrated 24-48 hour prediction windows using AI trained on personalized patient baselines. A 2024 JMIR systematic review confirmed SpO2 as the most useful predictor when combined with machine learning. The evidence is promising but not yet at the scale of heart failure RPM evidence. Programs launching COPD exacerbation prediction today are early movers building the outcomes data.


