



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























Most CCM care plans fail audits or break interoperability because they exist as static Word documents instead of structured data. A care plan template designed correctly drives three measurable outcomes:
- Denial rate from 8% to 3% through audit-ready documentation (consent, time logs, distribution history)
- Enrollment from 20% to 40% by making eligibility and care coordination clearer to staff and patients
- Up to 1% reduction in chronic-cohort readmissions when SDOH referrals run as closed-loop tasks inside the plan
This guide gives you the downloadable template, a fully filled-in sample, and the technical architecture (FHIR CarePlan + EHR integration) so the same plan that prints for a nurse syncs as structured data for IT and compliance.
Every chronic care program lives or dies by its care plan. The clinical work, the billable minutes, the audit defense, and the patient relationship all run through one document. Most teams treat that document as a static form, print it, fill it, file it, and that’s exactly why most CCM programs underperform. A care plan that prints for a nurse but doesn’t sync as structured data fails on two fronts: it can’t drive workflow automation, and it can’t survive the OIG documentation scrutiny that landed in the 2026 Work Plan.
The fix isn’t to abandon the printable format. Nurses still need a clean, scannable summary they can hand to a patient. The fix is to build the plan once as structured data and render it as a printable when needed, same plan, two surfaces. This guide gives you the template, a fully filled-in sample for reference, and the technical architecture for any team that wants to embed the same plan inside Epic, Cerner, Athena, or Meditech.
What a Better CCM Care Plan Pays For Itself With
| Lever | Typical Baseline | Achievable with Structured Template | Annual Revenue Impact (Mid-Size Practice, 600 Enrolled) |
| Denial Rate | 8% | 3% | +$50,000 recovered (assumes $1M CCM program) |
| Enrollment | 20% | 40% | +$167,000 (200 additional enrolled patients × $836/year average) |
| Add-on Capture | 50% | 80% | +$60,000 (99439 add-on more consistently billed) |
| Combined Annual Upside | — | — | ~$275,000 per mid-size practice |
The template doesn’t generate the upside, the discipline it enables does. A practice that adopts a structured template without changing workflow captures maybe 10% of the gain. A practice that uses the template to drive workflow change captures the full amount.
I. Requirements That Make a Printable Care Plan Template for CCM Audit Ready
A. CMS and HCCI Elements to Mirror in Every Template
A care plan must follow the CMS Chronic Care Management Toolkit and the 2025 HCCI template to ensure it withstands billing reviews. For a detailed breakdown, see our guide on CCM care plan requirements.
- Core clinical data: Problems, medications, allergies, vitals, and preventive care.
- Care coordination data: Goals, planned interventions, responsible care team members, community services, and follow-up schedules.
- Administrative data: Consent documentation, plan versioning, and distribution details such as when and how the plan was shared with the patient or caregiver.
Templates that follow these elements make it easier for revenue cycle teams to prove medical necessity and meet payer documentation expectations.
B. Electronic Source of Truth Inside a Certified EHR
CMS guidance and ACP toolkits are clear: printable or Word-based plans do not qualify as the official care plan record. To bill confidently, the source of truth must reside inside a certified EHR as structured data.
- Electronic plan requirement: The care plan must be stored electronically, not as an uploaded file.
- Audit traceability: Each version should carry metadata for author, creation date, and sharing history.
- Integration with quality measures: When fields are linked to HEDIS and NQF metrics, reporting becomes automated and error-free.
Hospitals that keep this structure inside Epic, Cerner, or Meditech through proper EHR integration can easily export both a printable summary and a structured, interoperable record.
Related read: CCM Audit Risk & Protection: A Compliance Playbook for 2026
C. Patient-Centered Structure That Clinicians Actually Use
Many care plans fail because they are designed for compliance officers rather than clinicians. A template that fits the nursing workflow ensures adoption and accuracy.
- Single-page patient summary: A concise printout showing conditions, goals, next steps, and responsible contacts.
- Detailed clinician view: A multi-section plan capturing interventions, care gaps, and task ownership.
- SDOH integration: Use discrete fields or coded entries to record housing, food, or transportation needs without cluttering the main plan.
When the plan supports clinical reasoning and patient dialogue, compliance becomes a byproduct rather than a burden.
If you want to see how this looks in practice, review a CCM care plan example with completed goals, interventions, and follow-up timelines.
II. What a Filled-In CCM Care Plan Actually Looks Like: Mrs. Johnson, 72
A blank template only solves half the problem. The other half is showing what a complete, audit-ready care plan looks like once it’s filled in. Below is a realistic example for a typical CCM patient. Names and details are illustrative: the structure matches the downloadable template above and meets CMS Chronic Care Management documentation requirements.
Patient Snapshot
| Field | Entry |
| Patient | Margaret Johnson (Mrs. Johnson) |
| Age / Sex | 72 / Female |
| MRN | 008-456-2291 (sample) |
| Primary Insurance | Medicare Part B + Medigap Plan G |
| Care Plan Version | v2.1 (2026-04-15) – initial plan v1.0 dated 2025-12-08 |
| CCM Consent | Verbal consent obtained 2025-12-08, documented in EHR |
| Care Coordinator | Sarah W., RN (assigned 2025-12-15) |
Active Problem List
| Condition | ICD-10 | Severity / Status | Last Reviewed |
| Type 2 Diabetes Mellitus, with hyperglycemia | E11.65 | HbA1c 8.4% (last 2026-03-12) – uncontrolled | 2026-04-15 |
| Heart Failure with reduced EF | I50.22 | NYHA Class II, EF 40% (last echo 2025-09-28) | 2026-04-15 |
| Essential Hypertension | I10 | Avg home BP 152/88 – uncontrolled despite 2 meds | 2026-04-15 |
Mrs. Johnson meets CCM eligibility under the standard rule: three chronic conditions, all expected to last 12+ months, all placing her at risk of acute exacerbation if unmanaged.
Current Medications
| Medication | Dose / Frequency | Indication | Adherence |
| Metformin | 1000mg twice daily | T2DM | 95% (pharmacy fill data) |
| Empagliflozin | 25mg once daily | T2DM + HFrEF | 90% |
| Lisinopril | 20mg once daily | HTN + HFrEF | 88% |
| Carvedilol | 12.5mg twice daily | HFrEF | 92% |
| Furosemide | 40mg as needed (per sx) | HFrEF | Variable – patient self-titrates |
Care Plan Goals (SMART format)
Goal 1 – Diabetes control
Reduce HbA1c from 8.4% to <7.5% within 6 months (target reassessment 2026-10-15) through medication adherence, dietary counseling, and home glucose monitoring.
Goal 2 – Blood pressure control
Achieve average home BP <140/90 within 90 days (target reassessment 2026-07-15) through medication titration, sodium restriction, and weekly home BP logging.
Goal 3 – Heart failure self-management
Maintain daily weight log, sodium intake <2g/day, and 90%+ medication adherence for 6 months. Reduce HF-related ED visits and hospitalizations to zero in the next 12 months.
Goal 4 – Functional independence
Maintain ability to perform all ADLs independently. Reassess fall risk and home safety quarterly.
Planned Interventions
| Intervention | Frequency | Owner | Documentation |
| RN care coordination call | Bi-weekly (twice monthly) | Sarah W., RN | EHR call note + minutes log |
| Remote patient monitoring (BP cuff, scale, glucometer) | Daily transmission | Patient + RN review | RPM dashboard, exceptions flagged |
| PCP visit | Quarterly | Dr. Chen, MD | EHR encounter note |
| Diabetes educator session | Monthly x 3, then quarterly | Diabetes educator | Education record + glucose log review |
| Pharmacist medication review | Quarterly | David K., PharmD | Med rec note + adherence summary |
| Cardiology consult | One-time at month 2 | Cardiology referral | Specialist note + plan update |
| SDOH screening | At enrollment + quarterly | RN | Structured SDOH note in EHR |
Care Team
| Role | Name | Contact | Responsibility |
| Primary Care Physician | Dr. Michael Chen | (sample) ext. 4421 | Clinical decisions, plan approval, quarterly visit |
| Care Coordinator (RN) | Sarah W., RN | (sample) ext. 4422 | Monthly outreach, RPM monitoring, plan execution |
| Clinical Pharmacist | David K., PharmD | (sample) ext. 4423 | Quarterly med review, adherence intervention |
| Diabetes Educator | (sample) | (sample) | Patient education, glucose pattern review |
| Cardiology Consult | (sample) | (sample) | HF management consultation |
| Patient | Mrs. Johnson | (patient phone) | Daily monitoring, adherence, and reporting of symptoms |
Follow-Up Schedule
| Month | Touchpoints | Goals Reviewed |
| Month 1 (Dec 2025) | Enrollment, RPM setup, baseline labs, initial RN call | All goals – establish baseline |
| Month 2 (Jan 2026) | 2 RN calls, cardiology consult, RPM review | Goal 3 (HF self-management) |
| Month 3 (Feb 2026) | 2 RN calls, diabetes educator session, PCP visit | Goal 1 (A1c retest), Goal 2 (BP target check) |
| Month 4–5 | Bi-weekly RN calls, monthly diabetes educator | Goals 1–4 progress check |
| Month 6 (May 2026) | Full plan review, A1c retest, all goals reassessed, plan version update to v3.0 | All goals – reassess and revise |
SDOH and Barriers
| Domain | Status | Action |
| Transportation | At risk – patient relies on adult daughter for appointments | Identified local volunteer transport program; referral made 2026-01-10 |
| Food Security | Stable | No action |
| Medication Affordability | Stable on current Medicare + Medigap | Pharmacist reviews quarterly for cost concerns |
| Social Isolation | Lives alone since spouse passed (2024) | Referred to senior center social programs; weekly phone check-in maintained |
| Caregiver Support | Adult daughter involved | Daughter included in care plan, signature, and quarterly updates |
Consent and Distribution
- CCM consent obtained verbally 2025-12-08 by Sarah W., RN. Documented in EHR encounter note.
- Patient acknowledged 20% Medicare coinsurance; supplemental Medigap covers the cost-share.
- Care plan v2.1 distributed to: patient (printed copy 2026-04-15), patient’s daughter (electronic via patient portal 2026-04-15), Dr. Chen (EHR notification 2026-04-15).
- Plan stored in EHR as structured CarePlan resource with linked Goal, Condition, ServiceRequest, and Task elements.
Audit-Readiness Notes
This care plan would withstand an OIG audit because:
1. Eligibility documentation is explicit (three qualifying chronic conditions with ICD-10 codes and severity)
2. Patient consent is documented with date, method, and obtainer
3. Time logs are tied to documented interventions, not estimated retroactively
4. Care plan is stored as structured EHR data, not a Word document upload
5. Plan versioning is visible (v1.0 → v2.1) with clear update dates
6. Distribution history is logged with date, recipient, and method
7. Every billable minute traces back to a planned intervention with a named owner
III. Architecture: Build Once in FHIR, Render as a Clean Printable
A. Two-Surface Pattern for Speed and Safety
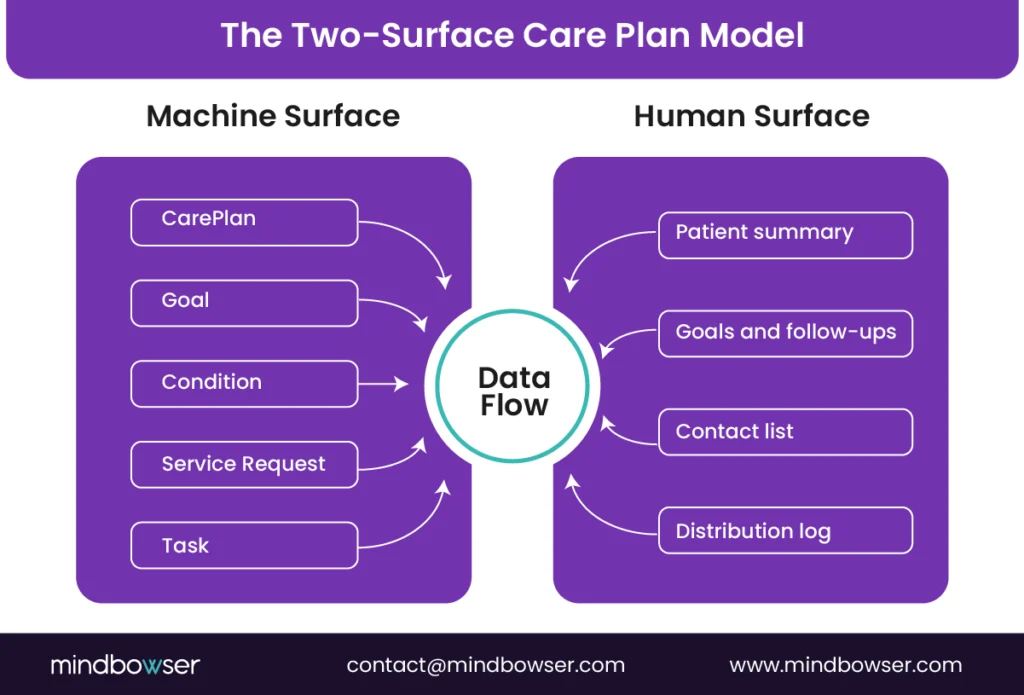
A durable care plan template must exist in two synchronized forms. One is the machine-readable layer that stores structured data. The other is the human-readable layout that prints and communicates clearly to patients and staff.
- Machine surface: Store the plan as an FHIR bundle using resources such as CarePlan, Goal, Condition, ServiceRequest, and Task. This allows the data to flow between systems and meet CMS and ONC interoperability standards.
- Human surface: Create a printable view that summarizes the same data. It should be designed for readability with clear goals, interventions, and follow-up dates.
- Version control: Each update to the plan should include a version and timestamp to maintain traceability across reviews and audits.
This two-surface model ensures that clinical staff have an easy-to-read summary while IT and compliance teams maintain a structured, shareable data record.
B. EHR Implementation Notes for Epic, Cerner, Meditech, and Athena
Hospitals that succeed in CCM documentation design their care plan templates to work seamlessly within their EHR environment.
- SMART on FHIR authoring: Create or edit care plans in a SMART on FHIR app that connects with your EHR and stores data in US Core CarePlan format.
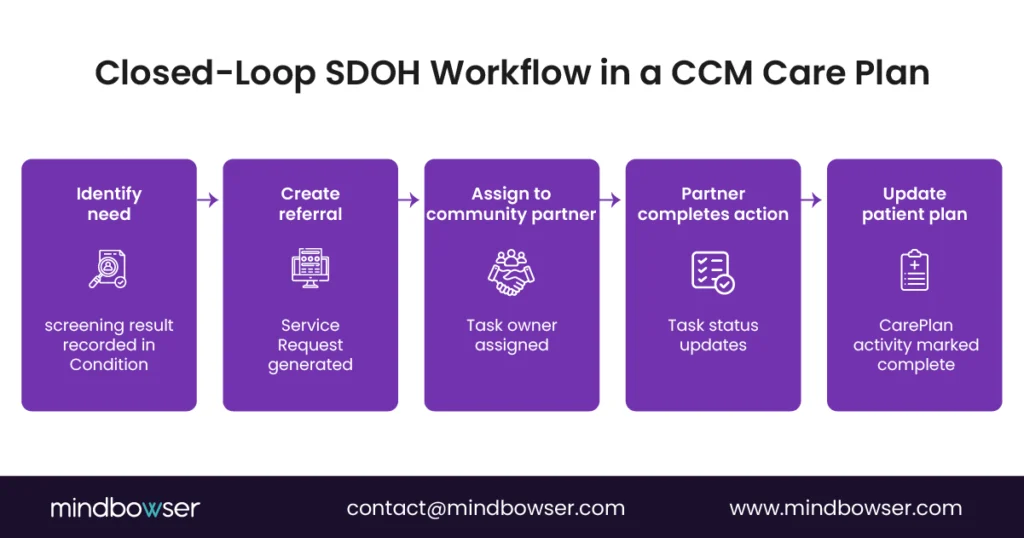
- SDOH tracking: Represent referrals as ServiceRequest objects that generate downstream Tasks. When a community partner closes the referral, the Task updates automatically in the plan.
- Workflow automation: Use BPM+ modeling standards from HIMSS to translate nurse workflows into machine-executable processes, ensuring uniform care coordination.
By building templates that speak FHIR natively, organizations can avoid duplicate entry and make their plans portable across systems.
For a Ready-to-Use Operational Version; Enrollment Form, Consent, Monthly Documentation, and Compliance Checklist
IV. ROI Model and Implementation Playbook for the Printable Care Plan Template for CCM
A. Revenue and Quality Levers
When designed correctly, a care plan template does more than support compliance. It drives measurable financial and quality outcomes by reducing denials, improving adherence, and optimizing staff time.
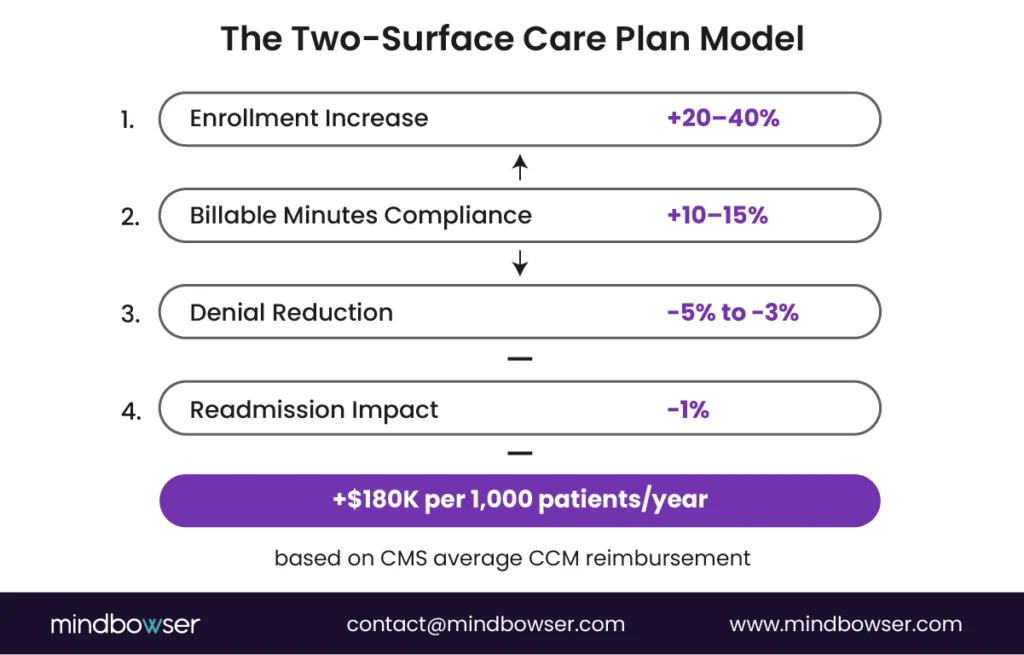
- Enrollment and eligibility: A clear, structured plan increases enrollment rates by enabling clinicians to identify eligible patients easily. Most programs prioritise patients based on conditions that qualify for CCM, such as diabetes, heart failure, and COPD. Hospitals typically enroll 12% to 18% of their Medicare panels when workflows are streamlined.
- Billable minutes attainment: Plans with embedded follow-up tasks help teams consistently meet the 20- and 60-minute thresholds, ensuring full reimbursement under CPT codes. A deeper look at this is covered in our chronic care management billing guide.
- Denial prevention: Audit-ready templates that capture consent, the sharing method, and time logs can lower denial rates from 8% to 3%, as shown in recent CMS reviews.
- Readmission impact: Hospitals that incorporate SDOH referrals and closed-loop follow-ups into the care plan often see a 1% or more reduction in readmissions among chronic cohorts.
By linking every field of the template to an operational or revenue outcome, leadership can tie compliance directly to ROI.
Related read: Chronic Care Management Billing Services: Reducing Burden, Maximizing ROI
B. Operating Model and Staffing
A printable and structured template simplifies day-to-day execution across clinical teams.
- Defined roles: Registered nurses manage interventions and documentation, medical assistants handle vitals and follow-ups, navigators manage SDOH referrals, and pharmacists oversee medication adherence.
- Active worklists: Each active CarePlan and its associated Tasks are displayed in daily dashboards, keeping teams focused on patients who need attention that day.
- Communication rhythm: Weekly huddles and escalation protocols ensure that unresolved issues or delayed tasks move quickly back to the primary care provider.
This operating model turns the care plan from a static record into a living workflow tool that guides every team member’s daily work.
C. Case Proof and Workflows
Across CCM-adjacent builds I’ve worked on, the same four patterns recur. The names of the systems aren’t here, but the deployment shapes are – what was built, on what EHR, and what changed once the care plan ran as structured data instead of as a Word document.
Care Team Automation:
A multi-site health system on Epic integrated remote monitoring data directly into CarePlan workflows. Blood pressure cuffs, glucose meters, and scale readings updated CarePlan activities in real time rather than getting copy-pasted into encounter notes. Nursing teams reported a 35% reduction in manual review hours and faster medication adjustment turnaround for chronic patients. The shift wasn’t from manual to AI – it was from data lookup to data flow.
Financial Navigation Integration:
A population-health platform serving Medicaid patients embedded financial assistance workflows as ServiceRequest elements inside the care plan. Care coordinators could trigger copay assistance, prescription discount programs, and grant referrals directly from the patient plan rather than maintaining a parallel financial-navigation worklist. Medication adherence improved 22% as financial barriers got resolved before they became reasons to skip doses.
Closed-Loop SDOH Tracking:
A community-based care program managing dual-eligible patients used Task resources to track SDOH referrals – transportation, food, housing – through to completion. Each referral was assigned, tracked, and closed inside the care plan. Closure rates improved 90%, which sounds like a marketing number until you realize most SDOH referrals previously sat as PDFs in a shared folder with no follow-up loop. The closure rate moved because someone could finally see what was open.
Multi-EHR Synchronization:
A provider network operating across both Epic and Cerner sites implemented a FHIR-based CarePlan service that unified patient data across both systems. Duplicate plans got eliminated, care coordination visibility improved, and billing accuracy improved across both EHRs because the plan stopped being a two-sources-of-truth.
What These Have in Common:
The pattern that repeats: every program that improved CCM economics did it by treating the care plan as live data, not as a document. The print-friendly version is a render of the data, not the source of truth. Once that flip happens – once the plan exists in FHIR and gets rendered for printing on demand – every downstream metric improves.
The pattern that emerges across these implementations is workflow-level, not product-level: the care plan stops being a document the team maintains and starts being a data structure the workflow runs on. Practices that take this seriously usually start from a small set of pre-built components rather than building everything custom – pieces like CarePlan AI for the structured plan generation, HealthConnect CoPilot for the FHIR-native EHR integration layer, and WearConnect when the program includes RPM. The point isn’t which tools – it’s that pre-built FHIR-aware components shave 6 to 9 months off custom builds and let the team focus on the workflow design rather than the integration plumbing.
What stays custom: the EHR-specific quirks of your Epic or Cerner deployment, the payer-specific billing rules your Rev Cycle team manages, and the care plan content that’s specific to your patient panel. What stays human: the SDOH conversation, the consent dialogue, the end-of-life planning, and any clinical escalation. These don’t automate and shouldn’t – naming them honestly is what separates a credible implementation pattern from a software pitch.
D. Deliverables You Receive in Week One
When hospitals or digital health organizations partner with Mindbowser, the goal is to accelerate compliance and interoperability without slowing clinical workflows. Our team provides production-ready assets from the first week of engagement.
- Printable and electronic templates: Care plan layouts in PDF and Word formats that align with CMS and HCCI standards, along with the corresponding US Core CarePlan JSON bundle.
- EHR build notes: Detailed configuration guides for Epic and Cerner to render and store the plan correctly, including sample templates for print and storage workflows.
- Compliance checklist: An annotated document that maps every section of the plan to CMS, HCCI, and NQF audit requirements for immediate internal validation.
These resources help technical and compliance teams begin structured documentation without waiting for lengthy design cycles.
Many organizations choose to build or extend custom chronic care management software to ensure their templates integrate seamlessly with EHR workflows and billing systems.
E. Implementation in 30 to 60 Days
Our typical implementation timeline transforms a hospital’s care planning process into a fully compliant, interoperable system within 2 months.
- SMART on FHIR authoring application: Deploy a secure interface that lets care managers create and update CarePlans directly within the EHR.
- Closed-loop SDOH referrals: Set up ServiceRequest and Task pipelines that automatically track referral completion with community partners.
- RPM data integration: Use the HealthConnect CoPilot and RPMCheck AI modules to map device data directly to CarePlan activities for continuous updates.
This rapid rollout provides hospitals with an immediate boost in documentation completeness and workflow efficiency.
Related read: CCM Care Plan Example: How to Build a Compliant, FHIR-Ready Model That Improves Outcomes and Revenue
F. Proof and Governance
To ensure long-term value, every implementation includes measurable performance tracking and governance structures.
- ROI model and sensitivity calculator: Tailored to your patient panel size, enrollment targets, and denial rates to estimate expected financial impact.
- Compliance governance: Quarterly audits using CMS and ONC frameworks to maintain certification and interoperability standards.
- Training and runbook: Standard operating procedures for clinicians and IT teams to maintain accuracy, version control, and efficient data sharing.
With this structure in place, your organization can sustain both operational excellence and audit confidence as reimbursement models evolve.
See a real-world implementation in our CCM care plan example guide.
Conclusion
A printable care plan template for CCM is no longer just a clinical form. It is the backbone of revenue integrity, interoperability, and patient engagement. The organizations that succeed in care coordination treat the plan as both a compliance document and a living workflow.
When your care plan is built in FHIR, aligned with CMS and HCCI requirements, and synchronized across EHRs, it becomes more than a checkbox exercise. It improves care continuity, reduces manual work, and supports faster reimbursement. Hospitals using this dual-surface model consistently achieve higher enrollment, lower denials, and better patient outcomes.
The next step is to replace disconnected Word templates with a structured, audit-ready framework that your teams can trust. A printable care plan template designed the right way keeps your organization compliant today and future-ready for the next phase of value-based care.
A compliant care plan must include a complete problem list, current medications, allergies, measurable goals, planned interventions, and designated care team members. It should also record how and when the plan was shared with the patient or caregiver. CMS and HCCI specify these fields as mandatory for reimbursement and audit validation.
Static documents are acceptable for printing, but not as the official electronic record. CMS requires that the source of truth reside inside a certified EHR in structured, electronic form. You can still use a printable layout for patient communication, but it should be generated from a FHIR-based record stored within the EHR.
Represent social needs as coded entries using ServiceRequest and Task resources. This keeps the printable summary concise while ensuring that the underlying data supports SDOH reporting and follow-up tracking. The patient-facing plan should show resolved and pending referrals in a simple checklist format.
Yes. All major EHRs now support FHIR-based data exchange. Care plans authored in US Core CarePlan format can be stored or displayed using native templates or SMART on FHIR applications. The same structure can print cleanly while remaining interoperable for sharing with external providers.
Hospitals that standardize care plans using structured templates typically increase enrollment by 20% to 40%, reduce denial rates to under 5%, and achieve modest readmission reductions within six months. The financial improvement comes from accurate billing, faster documentation, and better patient follow-up.


