



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR:
Chronic care management software enables hospitals and digital health startups to enhance patient engagement, streamline documentation, and ensure billing compliance. The future lies in API-first builds, seamless RPM integration, and AI-enabled workflows. Mindbowser delivers scalable platforms that not only protect compliance but also drive measurable ROI in value-based care programs.
Chronic care management (CCM) has become one of the fastest-growing segments in U.S. healthcare, projected to expand from $6.63 billion in 2024 to as much as $14.50 billion by 2030. This growth is fueled by the increasing prevalence of chronic diseases, the expansion of CMS reimbursement, and the shift toward value-based care.
For hospitals, CCM presents both opportunities and pressures. While reimbursement creates a new revenue stream, leaders face mounting compliance risks, EHR integration gaps, and limited staff capacity. For startups, the challenge is different. Scaling engagement, proving ROI, and integrating with entrenched health system infrastructure requires more than a simple app.
This is where chronic care management software plays a decisive role. Purpose-built platforms bring together remote patient monitoring, documentation workflows, and billing automation into a single system. More importantly, the best platforms are designed with an API-first mindset, enabling interoperability across Epic, Cerner, Athena, and other EHRs.
In this blog, we will explore what CCM software is, compare off-the-shelf and custom-built solutions, highlight why API-first architecture matters, and examine how future-ready platforms are leveraging RPM and AI to drive sustainable value-based care. Finally, we will outline how Mindbowser helps hospitals and startups design CCM systems that deliver both compliance protection and measurable ROI.
I. What is Chronic Care Management Software?
Chronic care management software refers to technology platforms designed to help providers coordinate ongoing care for patients with multiple chronic conditions. At its core, the software is not just a digital filing cabinet but a living system that manages patient interactions, ensures compliance with CMS requirements, and supports revenue capture for care delivered outside the clinic.
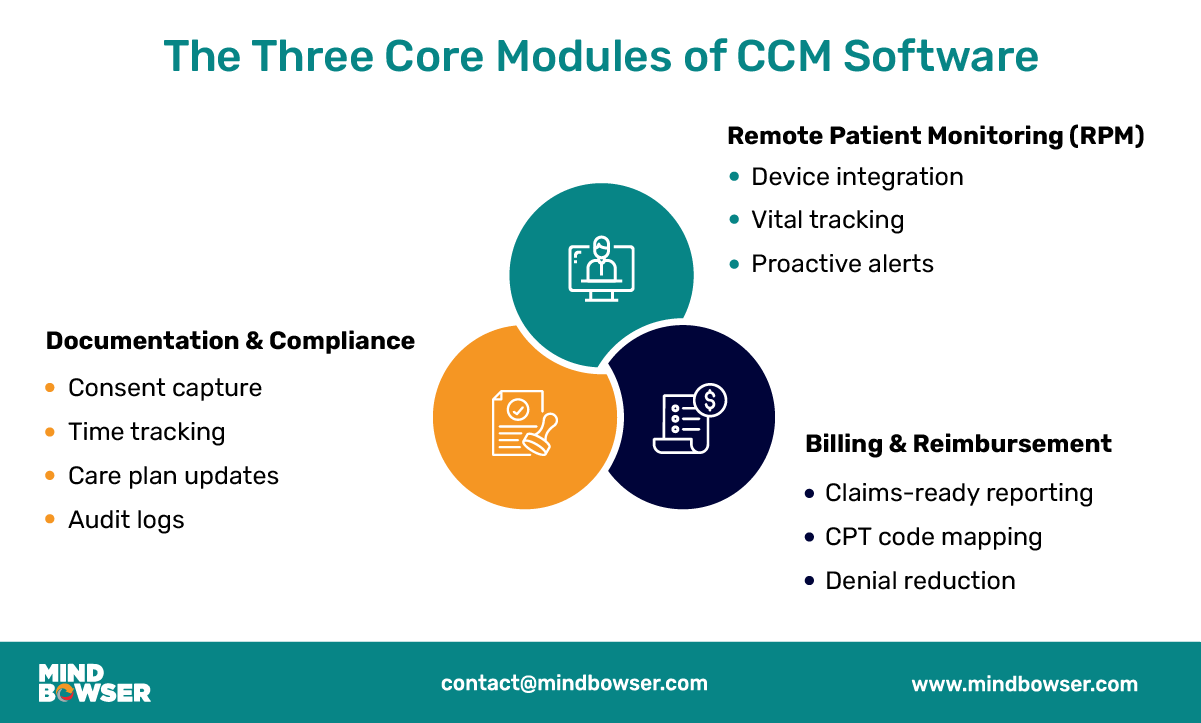
A. Core Modules of CCM Software
- Remote Patient Monitoring (RPM) Integration
The rise of connected devices has made RPM a central feature of CCM platforms. By integrating wearables and Bluetooth-enabled medical devices, care teams gain real-time visibility into vital signs, such as blood pressure, heart rate, and blood glucose levels. These data streams help clinicians detect risk earlier and intervene before conditions escalate. For patients, it improves engagement because they see their progress tracked continuously. - Documentation and Compliance Workflows
Accurate documentation is the backbone of CCM reimbursement. Software platforms standardize consent capture, time tracking, and care plan updates in a way that satisfies CMS audit requirements. Built-in compliance checks reduce the likelihood of denials while providing care managers with essential tools, including task queues, progress notes, and structured reporting. This ensures that every minute spent on patient management can be attributed correctly. - Billing and Reimbursement Automation
The complexity of CPT codes for CCM is a major administrative burden. Software solutions automate the linkage between care tasks, time thresholds, and billing codes, facilitating seamless integration. Instead of relying on manual reconciliation, platforms generate claims-ready reports that map directly to CMS rules. For hospitals and clinics, this means fewer denied claims and faster revenue cycles.
B. Why These Modules Matter
- Compliance with CMS CPT Codes
Chronic care management is governed by strict billing requirements that demand accurate documentation of patient consent, time spent, and the services delivered. Without automation, compliance becomes resource-intensive and prone to error. CCM software provides the audit trail necessary to withstand payer scrutiny. - Supporting Clinical Workflows and Reducing Staff Burden
Clinicians and care coordinators are already stretched thin. By automating documentation, reminders, and outreach, CCM software reduces repetitive tasks and frees up staff to focus on patient interaction. This directly addresses staffing shortages that many hospitals and health systems cite as their biggest operational challenge. - Driving Measurable ROI in Value-Based Care
Chronic conditions account for the majority of U.S. healthcare spending. Platforms that help manage these patients not only unlock CMS reimbursement but also reduce avoidable hospitalizations and readmissions. This creates financial savings for providers while improving quality metrics tied to value-based care contracts. In other words, the right CCM software is both a compliance safeguard and a financial growth lever.
II. Off-the-Shelf vs Custom CCM Platforms
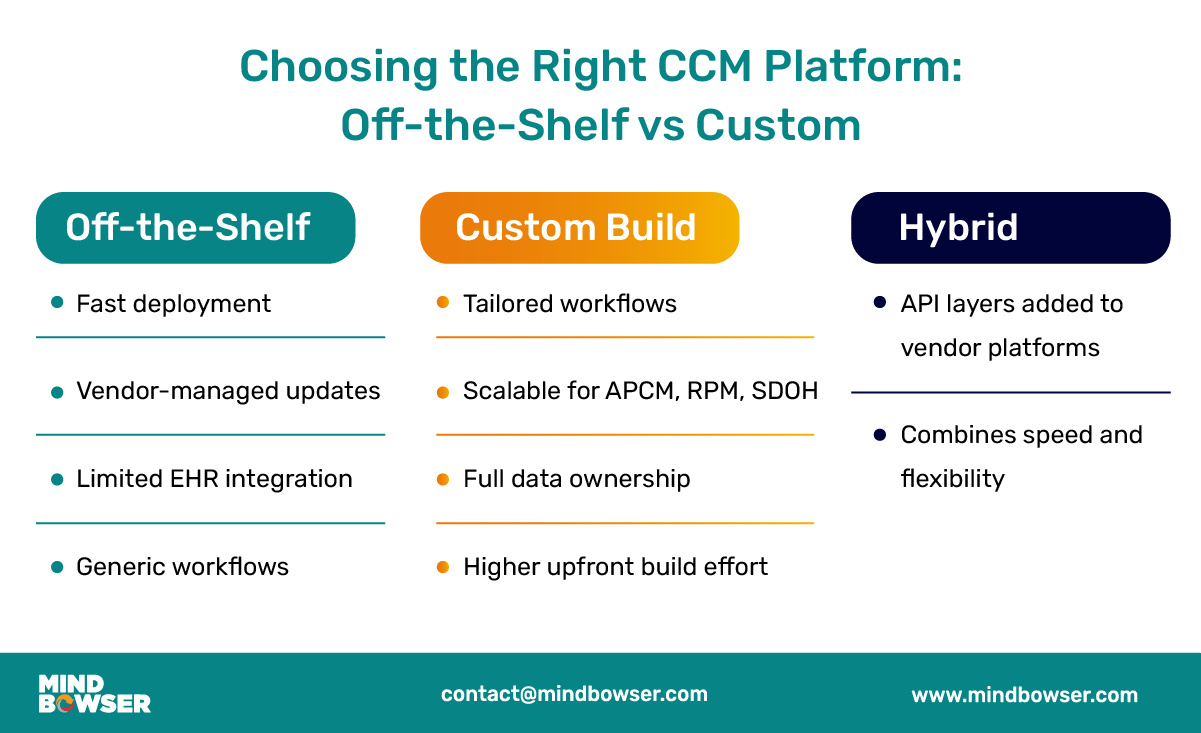
Choosing the right type of chronic care management software is one of the most important decisions for hospitals and digital health startups. The market offers two primary pathways: adopting an off-the-shelf product from a vendor or developing a custom solution tailored to an organization’s specific needs. Increasingly, a hybrid middle ground is also emerging. Each path carries advantages and tradeoffs that leadership teams need to evaluate carefully.
A. Off-the-Shelf Benefits and Tradeoffs
- Faster Deployment, Vendor-Managed Updates
Off-the-shelf CCM platforms can be deployed relatively quickly, often within weeks. Vendors manage regulatory updates and technical maintenance, which can reduce the IT burden on internal teams. For smaller health systems or early-stage startups, this approach enables immediate participation in CMS reimbursement programs without requiring a significant upfront investment. - Limited EHR Integration and Generic Workflows
The tradeoff is flexibility. Many out-of-the-box platforms offer only surface-level EHR integrations, often limited to HL7 feeds or flat-file uploads. This leaves gaps when clinicians expect seamless workflows across Epic, Cerner, or Athena. Additionally, these platforms are designed to serve the broadest market possible, which means their workflows may not align with the unique clinical practices of each organization.
B. Custom Build Advantages
- Tailored to Hospital or Startup Needs
Custom CCM platforms are designed around the specific workflows, staffing models, and patient populations of an organization. A behavioral health network may need intensive coordination tools, while a cardiology-focused startup may prioritize remote patient monitoring integrations. By tailoring the build, organizations ensure that technology supports rather than disrupts care delivery. - Scalable Roadmap for Expansion
As reimbursement evolves, custom platforms can adapt quickly to meet changing needs. New models, such as APCM codes and social determinants of health (SDOH) reporting, require flexible data structures. A custom architecture enables providers to extend their platform, capturing new billing opportunities and expanding beyond basic CCM into principal care management, behavioral health, or integrated SDOH tracking. - Ownership of Data Plane and Workflows
A key benefit of building custom software is data ownership. Rather than being locked into a vendor’s ecosystem, organizations maintain full control of how data flows into analytics platforms, data warehouses, or payer-facing portals. This ownership is increasingly important as hospitals seek to generate predictive insights and prepare audit-ready packets without depending on third parties.
C. Hybrid Approaches Emerging
- API Layers on Top of Off-the-Shelf Platforms
Some organizations are finding success by layering APIs and middleware on top of vendor platforms. This approach enables them to leverage the vendor’s core compliance and billing features while extending functionality to custom workflows, predictive analytics, or device integrations. - Case Study Example
A behavioral health provider utilized a vendor platform for its core documentation and billing features, but integrated it with a custom-built referral and patient engagement layer. By doing so, the organization reduced readmissions by more than 50% while maintaining compliance with Medicaid billing requirements. This demonstrates how hybrid approaches can blend the speed of vendor solutions with the precision of custom builds.
III. Why API-First Architecture Matters
In today’s healthcare environment, chronic care management software cannot operate as a silo. Hospitals and startups are increasingly expected to deliver care coordination across multiple platforms, EHRs, and devices. An API-first architecture ensures that CCM systems are not only interoperable but also future-ready for the rapid policy and technology changes shaping value-based care.
A. Interoperability Imperatives
- Epic, Cerner, Athena, Canvas Integration Challenges
Large health systems operate within complex EHR environments, with Epic being the most common, but also the most restrictive. Off-the-shelf CCM solutions often struggle to connect deeply with Epic’s closed environment. Cerner and Athenahealth offer more open APIs but require significant configuration to achieve full bidirectional data exchange. For newer systems like Canvas or Healthie, API-first platforms facilitate seamless integration by supporting SMART-on-FHIR standards. - SMART-on-FHIR Standards
API-first design allows platforms to meet interoperability requirements using SMART-on-FHIR. This enables CCM platforms to integrate with various EHRs without requiring custom one-off interfaces. For hospitals, this reduces integration costs, and for startups, it shortens time-to-market by eliminating the need for redundant engineering. The result is cleaner data exchange, fewer workflow interruptions, and stronger compliance with ONC interoperability rules.
B. Building an Enterprise Data Plane
- Streaming Encounter Artifacts to Data Lakes
API-first platforms establish the foundation for an enterprise data plane, where every encounter artefact, such as time logs, care plan updates, and consent forms, flows into a secure, centralized data environment. This enables health systems to integrate CCM data with claims, lab results, and social determinants of health data for a more comprehensive view of patients. - Enabling Predictive Analytics and Audit-Proofing
By structuring CCM data for analytics, organizations can deploy predictive models that identify patients at risk of hospitalization, non-adherence, or readmission. Just as important, the same structured data can be used to automatically generate audit-ready packets that include consent forms, time stamps, and care plan deltas. This reduces the risk of denials and protects against compliance audits.
C. ROI and Compliance Benefits
- Audit Packet Automation
One of the top reasons payers deny CCM claims is the lack of documentation. API-first systems can automate the assembly of payer-ready packets, pulling in access logs, consent artifacts, and task completion details in real time. This ensures that billing submissions are both accurate and defensible. - Reduced Rework in Billing and Reporting
Manual reconciliation of care tasks against billing thresholds often results in delays and denials. With API-driven workflows, CCM platforms eliminate duplicate data entry and reduce rework for billing teams, thereby enhancing efficiency and accuracy. Automated reporting tools also help finance teams calculate ROI across service lines, linking patient engagement to both revenue and outcomes.
In short, API-first architecture is not just a technology preference. It is the difference between a platform that grows obsolete as EHR requirements evolve and one that positions hospitals and startups to thrive under value-based care.
Start Building A Compliant, ROI-Driven CCM Platform With Mindbowser Today
IV. The Future of CCM Platforms
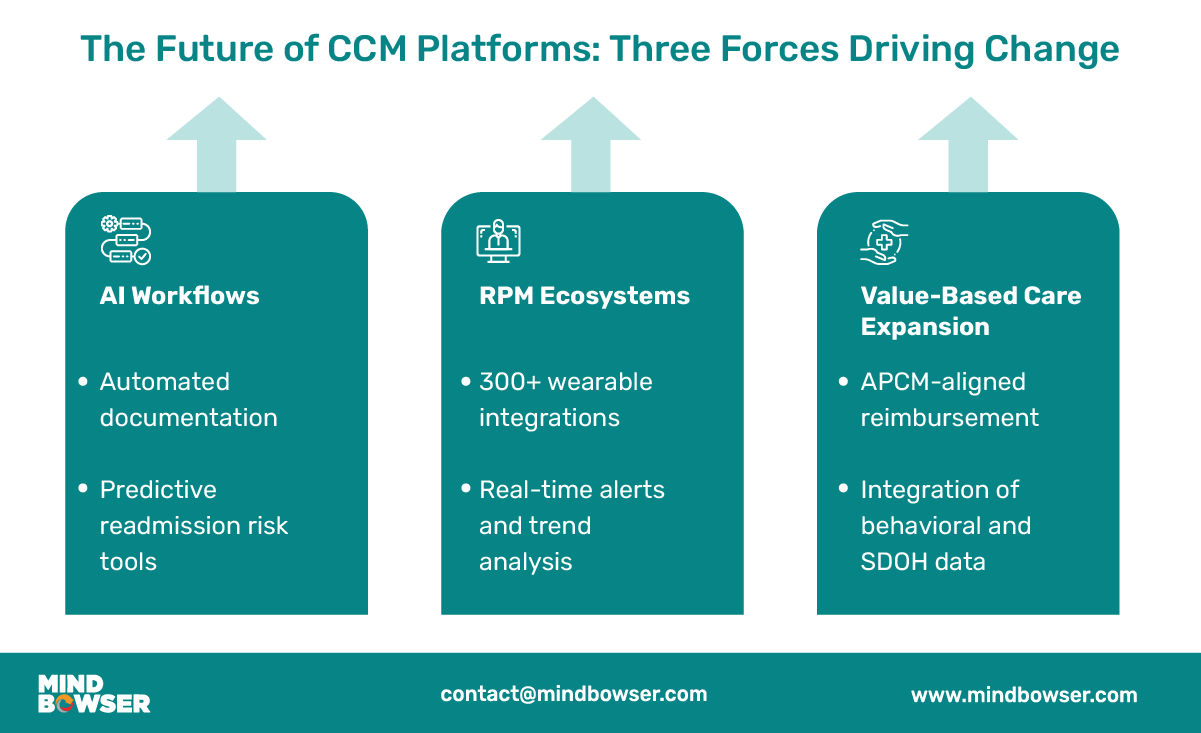
Chronic care management is no longer a back-office billing program. It is becoming a strategic pillar for hospitals and startups navigating value-based care. The next wave of CCM platforms will be defined by three key forces: the integration of AI into clinical workflows, the expansion of remote patient monitoring ecosystems, and the alignment of software with new reimbursement models, such as APCM.
A. AI Workflows in Care Management
- AI-Powered Documentation
Documentation remains one of the heaviest burdens on care teams. AI-enabled workflows, such as the AI Medical Summary, can automatically transform unstructured clinical notes, laboratory results, and patient histories into structured summaries. This allows care managers to spend less time typing and more time engaging with patients. For hospitals, the impact is immediate: shorter documentation cycles, reduced compliance errors, and a higher number of encounters captured for billing. - Predictive Readmission Risk workflows
Preventing readmissions is at the center of value-based care economics. Tools such as the AI Patient Readmission Risk accelerator analyze vital signs, EHR data, and social determinants to identify patients most likely to be rehospitalized within 30 days. Care teams can then target outreach, prioritize interventions, and allocate staff resources more effectively. The result is fewer penalties, lower costs, and measurable improvements in patient outcomes.
B. Remote Patient Monitoring Integration
- Wearable and Device Ecosystems
Future-ready CCM platforms will expand their integrations with wearables and home-based monitoring devices. Through accelerators like WearConnect, software can integrate data from over 300 wearables and health apps. For patients, this means their blood pressure cuff, glucometer, or smartwatch connects seamlessly to their care plan. For providers, it creates a continuous data feed that supports proactive interventions. - Real-Time Alerts and Trend Analysis
The ability to track patients between visits will become a standard expectation. Platforms that aggregate daily vitals and generate risk alerts empower clinicians to act before minor fluctuations turn into hospital-level events. Over time, predictive analytics will shift CCM from reactive documentation to proactive disease management, aligning with population health strategies.
C. Expanded Value-Based Care Models
- Alignment with APCM Reimbursement
CMS is introducing new codes under the Advanced Primary Care Management (APCM) framework that recognize both medical complexity and social complexity. CCM platforms that are flexible enough to capture these new data points will help providers unlock additional reimbursement opportunities. This is especially critical for organizations serving high-need populations where social determinants play a major role. - Supporting Behavioral and Social Determinants of Health
The future of CCM will expand beyond physical health metrics. Platforms will incorporate behavioral health data, housing status, food insecurity, and transportation access as structured inputs into care plans. By embedding social determinants of health into CCM, providers can deliver more holistic care while meeting payer expectations for integrated value-based care.
In short, the future of chronic care management platforms is being shaped by the convergence of various factors. AI will automate the repetitive. RPM will extend care beyond the clinic. And reimbursement frameworks like APCM will reward those who integrate medical and social complexity into care delivery.
V. How Mindbowser Can Help
Hospitals and startups evaluating chronic care management software often face a similar challenge: technology choices appear promising on paper but often fall short in real-world deployment. Mindbowser bridges that gap by building platforms that combine clinical insight, compliance discipline, and engineering strength. Our track record with mid-market hospitals and Series B+ digital health startups shows how custom builds can deliver measurable results.
A. Proven Case Studies
- Elderly Remote Patient Monitoring Engagement
One of our clients needed a digital solution to improve chronic care for elderly patients. We designed a remote patient monitoring application that integrated Bluetooth devices, real-time vital tracking, and secure communication features. The result was 90% patient engagement among elderly users, along with report generation that was twice as fast for administrators and care managers. - AI-Driven Care Coordination
A digital health client needed to cut the documentation overhead slowing down post-visit care coordination. Mindbowser built an AI-powered workflow platform integrated with the client’s existing EHR.Outcomes:
– 60% reduction in post-visit follow-up time
– 70% reduction in documentation time per encounter
These case studies demonstrate that success in CCM software is not solely about features. It is about embedding compliance, clinical workflows, and financial ROI into the core of the build.
B. Workflows for Faster Builds
- CarePlan AI
Streamlines care planning and coordination by capturing patient goals and preferences digitally. Reported outcomes include a 37% increase in patient understanding and a 42% decrease in coordination delays. - MedAdhere AI
Addresses one of the biggest challenges in CCM: medication adherence. Automated reminders, sent via SMS, email, or push notifications, monitor compliance and initiate follow-ups when patients miss doses. - RPMCheck AI
Automates daily remote monitoring check-ins, reducing the need for manual staff outreach. This has boosted daily check-in completion by 38% and cut staff workload by half. - HealthConnect CoPilot
Provides seamless EHR interoperability with Epic, Cerner, and Athenahealth using FHIR/HL7 standards. This ensures that data captured in CCM platforms is seamlessly integrated into core clinical systems without duplication.
By leveraging these accelerators, Mindbowser reduces development timelines, lowers implementation risk, and helps clients achieve compliance milestones more quickly.
C. Compliance and ROI Edge
- Regulatory Readiness
Every build is designed with HIPAA, SOC2, and 42 CFR Part 2 standards in mind. This ensures that platforms are not only secure but also audit-ready from the outset. - ROI Modeling and CPT Compliance
Mindbowser incorporates CPT compliance logic and ROI dashboards into its platforms. Leaders can track the number of billable encounters, monitor revenue growth, and directly connect clinical activity to financial results. This visibility enables organizations to defend reimbursement claims while demonstrating the financial benefits of chronic care management.
Building a CCM platform that survives a CMS audit, integrates with Epic or Cerner, and actually drives ROI is hard to get right the first time. Mindbowser has built CCM platforms for hospitals and digital health startups – API-first, compliance-ready, with AI workflows baked in. Talk to our team to see what a custom build looks like for your program.
Conclusion
Chronic care management software has moved from being a back-office convenience to becoming a strategic necessity for hospitals and digital health startups. As reimbursement programs expand and value-based care contracts gain traction, the ability to coordinate, document, and bill for chronic care services is no longer optional.
The market is clear. Off-the-shelf platforms can get organizations started quickly, but they often lack the deep integrations and custom workflows required for long-term success. API-first, custom, or hybrid platforms provide the flexibility to grow in response to evolving reimbursement models, such as APCM, and the increasing importance of social determinants of health.
The future is already taking shape. AI-powered documentation tools, predictive risk models, and wearable integrations are reshaping how care teams manage chronic conditions. At the same time, audit-proofing, compliance automation, and ROI modeling are becoming essential safeguards in an environment where denials are costly and can have significant financial implications.
Hospitals and startups that make strategic investments in CCM software will not only improve patient outcomes but also build sustainable revenue streams. Mindbowser stands as a trusted partner in this journey, delivering platforms that combine compliance, interoperability, and measurable ROI.
Chronic care management software is a platform that helps providers coordinate and document care for patients with multiple chronic conditions. It typically includes remote patient monitoring, documentation workflows, and billing automation to support compliance with CMS requirements.
The software standardizes time tracking, consent, and care plan updates while linking activities to CPT codes. This creates audit-ready documentation that reduces denials and ensures providers are reimbursed accurately for the services they deliver.
Off-the-shelf platforms enable quick deployment but often lack in-depth EHR integration and customized workflows. Custom builds, on the other hand, give organizations control over their data plane, allow for scalability with evolving reimbursement models, and align more closely with clinical workflows.
API-first architecture ensures interoperability with EHRs like Epic, Cerner, and Athena. It also enables seamless data exchange, automates audits, and allows for the streaming of encounter artifacts into enterprise data lakes for predictive analytics and compliance monitoring.
AI supports CCM by automating documentation, predicting readmission risk, and analyzing wearable data for early intervention. These capabilities reduce staff burden, enhance patient engagement, and enable organizations to thrive under value-based care models.


