



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
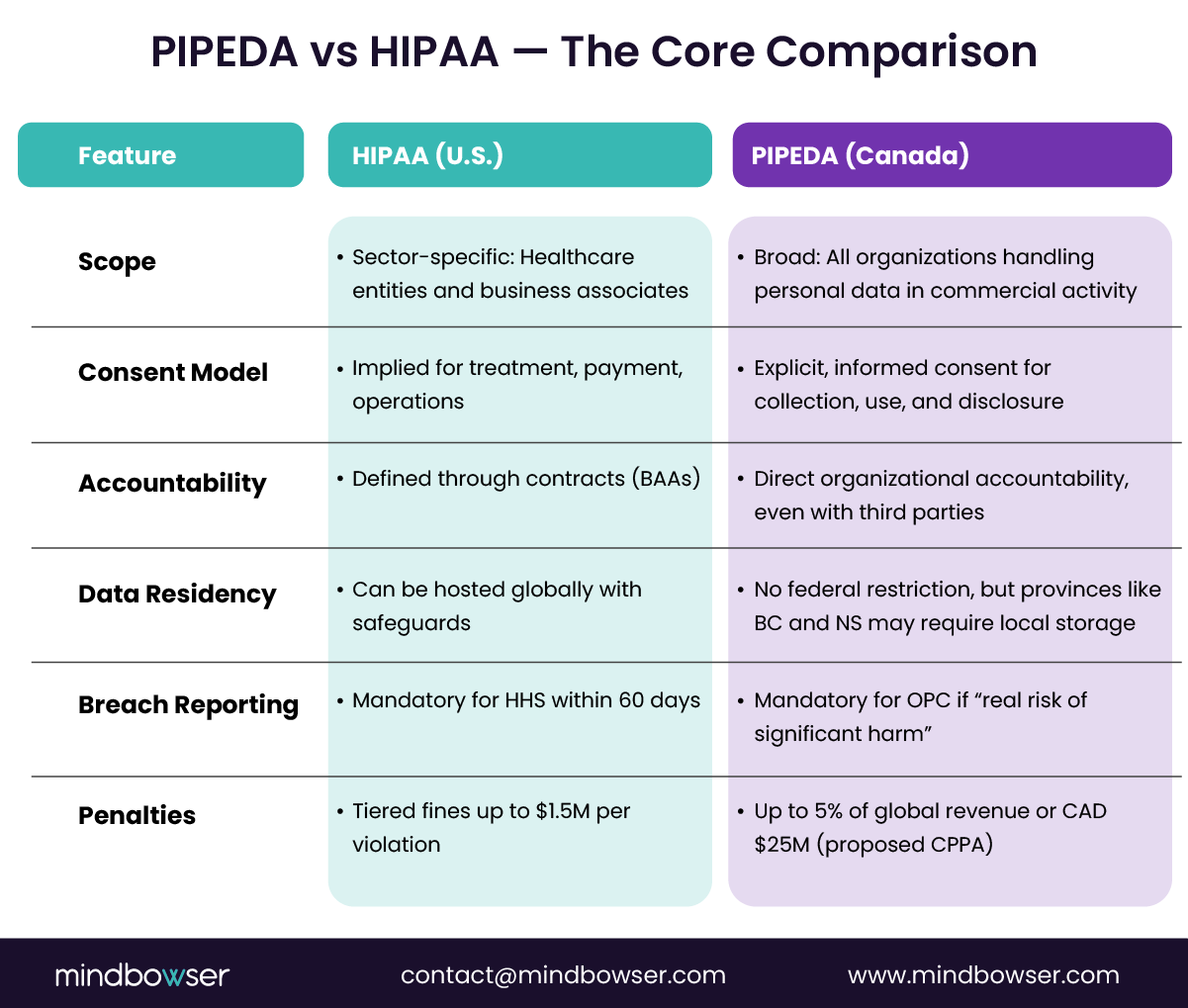
For U.S. healthtech companies eyeing the Canadian market, HIPAA compliance alone will not guarantee approval. Canada’s PIPEDA (Personal Information Protection and Electronic Documents Act) places a stronger emphasis on explicit consent, individual control, and accountability throughout the data lifecycle. While HIPAA focuses on covered entities and contractual enforcement, PIPEDA requires demonstrable privacy practices across all organizations that handle personal information.
This guide outlines a side-by-side comparison of PIPEDA and HIPAA, covering consent models, breach reporting, and data residency, offering a clear roadmap for CTOs, compliance leaders, and business development executives managing cross-border pilots or partnerships in Canadian health systems.
As U.S. digital health platforms expand north into Canada, many discover that HIPAA compliance does not automatically translate to PIPEDA readiness. The two frameworks share a commitment to protecting health data but differ sharply in how they implement it. HIPAA defines who must comply—covered entities and business associates—while PIPEDA governs how any organization collects, uses, and safeguards personal information in commercial activity.
For U.S. firms integrating with Canadian hospitals, EHRs, or provincial telehealth programs, these differences can impact everything from API consent flows to cloud hosting choices. Canadian regulators expect explicit consent, transparent data handling, and accountable governance, even for small pilot programs.
In this landscape, understanding PIPEDA vs HIPAA is not a legal exercise; it is a go-to-market strategy. Teams that align compliance early accelerate integration timelines, reduce renegotiation risks, and strengthen trust with hospital partners and investors.
I. The Compliance Context
A. Understanding the Regulatory Foundations
Two distinct philosophies guide health data governance in the United States and Canada.
HIPAA (Health Insurance Portability and Accountability Act) was designed to regulate specific entities in the healthcare ecosystem—providers, payers, and their business associates. It defines precise roles and responsibilities around the protection, transmission, and use of protected health information (PHI).
PIPEDA (Personal Information Protection and Electronic Documents Act), on the other hand, applies broadly to any organization that collects, uses, or discloses personal information in the course of commercial activity. This includes digital health companies, insurers, clinics, and even wellness platforms operating in Canada. Unlike HIPAA, PIPEDA is not confined to healthcare; it governs personal information of all kinds, including health data, within its scope.
For a U.S. healthtech company expanding to Canada, this means compliance extends beyond “covered entities.” Even if the company is not directly managing patient records through a hospital, it must comply with PIPEDA once it collects identifiable information from Canadian users.
B. The Accountability Principle
PIPEDA’s foundation is the Accountability Principle, which requires organizations to take responsibility for all personal data under their control, including data processed by third parties. This principle shifts compliance from a checklist to an ongoing governance model.
While HIPAA’s framework relies heavily on written policies, training, and contractual controls, PIPEDA expects organizations to demonstrate active accountability—through privacy management programs, audits, and documented consent processes. Canadian regulators expect organizations to prove that safeguards are not only written but functioning effectively.
For example, a U.S. remote patient monitoring company that outsources analytics to a cloud vendor in another country must show that the vendor provides the same level of privacy protection as PIPEDA requires. This level of oversight and documentation distinguishes PIPEDA’s compliance culture from HIPAA’s rule-based model.
C. Why the Difference in Scope Matters
This divergence impacts how digital health companies design workflows, integrations, and data-sharing models. HIPAA defines who must protect data, while PIPEDA dictates how every organization should handle it responsibly.
A telehealth platform that uses both Canadian and U.S. patient data cannot rely solely on HIPAA-driven policies. It must architect its systems to handle explicit consent, enable access logs for individual data requests, and prepare for cross-border audit scrutiny.
In short, the difference between PIPEDA and HIPAA isn’t just in geography—it is in philosophy. One codifies protection through compliance categories, while the other enforces it through accountability and transparency.
II. Consent, Data, and Disclosure Models
A. Consent Mechanics
Consent is the first major point of divergence between HIPAA and PIPEDA.
Under HIPAA, consent is often implied for what the law calls “treatment, payment, and healthcare operations.” Providers and payers can exchange data for these purposes without obtaining new permissions each time. Patients are informed through privacy notices, and while they have the right to access and amend their records, their consent is typically not required for routine operations.
Under PIPEDA, consent is the foundation of lawful data handling. Organizations must obtain meaningful, informed, and explicit consent from individuals before collecting, using, or disclosing personal information. The individual must understand what data is being collected, why it is needed, and how it will be used. Consent cannot be bundled or assumed through inactivity.
This difference requires design teams to reimagine workflows. For example, a digital health platform that collects continuous biometric data must build explicit consent flows for Canadian users—often involving multi-step opt-ins for specific features like data sharing, research use, or integration with third-party wellness tools.
HIPAA compliance teams accustomed to relying on implied consent find that PIPEDA demands both transparency and granularity in how user permissions are structured.
B. Cross-Border Data Sharing Example
Consider a U.S. remote patient monitoring company expanding to Ontario. Its existing platform allows clinicians to view patient vitals through a shared dashboard, relying on implied HIPAA consent for data sharing. In Canada, this same model triggers new requirements under PIPEDA.
The company must ensure that each patient explicitly agrees on how their health data will be collected, transmitted, and viewed by their care team. If any analytics or AI tools are used for data interpretation, those activities must also be disclosed. Moreover, patients have the right to withdraw consent at any time, requiring the system to support dynamic consent management.
For minors or teleconsultations, PIPEDA adds another layer of responsibility: organizations must confirm that a parent or guardian provides consent and that the use of data aligns with the reasonable expectations of the individual.
In effect, HIPAA allows consent to serve as a procedural safeguard, while PIPEDA elevates it to a living, continuous agreement between the user and the organization. This difference directly affects API design, consent storage, and data-sharing logic across both markets.
III. Data Residency and Storage Compliance
A. Data Location Rules
When it comes to data residency, the contrast between the United States and Canada lies in the balance between flexibility and jurisdictional control.
Under HIPAA, data can be stored or processed outside the United States if the hosting vendor maintains the required safeguards and executes a Business Associate Agreement (BAA). The law focuses on ensuring security standards—such as encryption, audit controls, and breach response—are met regardless of location. This allows HIPAA-compliant vendors to use global cloud infrastructure, provided the contractual and technical measures are strong enough.
PIPEDA, however, takes a more contextual approach. It does not explicitly require that personal health data stay in Canada, but organizations remain accountable for data under their control even if it is processed abroad. In practice, this means that if a U.S. healthtech company stores Canadian data in U.S.-based servers, it must notify individuals that their information could be subject to foreign laws.
Adding to this complexity, certain provinces impose additional restrictions. For example, British Columbia’s Freedom of Information and Protection of Privacy Act (FIPPA) and Nova Scotia’s Personal Information International Disclosure Protection Act (PIIDPA) require public-sector data, including healthcare information, to be stored and accessed only within Canada. Ontario’s Personal Health Information Protection Act (PHIPA), while more flexible, still requires organizations to ensure comparable protections through agreements and risk assessments.
For cross-border health platforms, these provincial nuances determine hosting strategies and partner selection. Many U.S. companies entering Canada opt for localized storage through cloud regions such as AWS Canada Central or Azure Toronto to meet both compliance and procurement expectations.
B. Technical Controls
Beyond geography, both frameworks converge on one common requirement—security by design. Encryption, access logging, and key management are critical to proving compliance in both jurisdictions.
HIPAA mandates administrative, physical, and technical safeguards that protect the confidentiality and integrity of PHI. PIPEDA requires “appropriate security measures,” which are interpreted in relation to the sensitivity of the information. For healthcare data, this sets a high bar similar to HIPAA’s technical standards.
Organizations must implement:
- Encryption at rest and in transit, following standards such as AES-256 and TLS 1.2+.
- Access control policies that restrict user permissions based on role and function.
- Comprehensive audit logs to record data access and modification events.
Frameworks such as SOC 2 Type II and ISO 27001 are increasingly used as shared benchmarks to demonstrate compliance readiness across both countries. These certifications serve as proof of disciplined governance and continuous security monitoring.
Mindbowser’s work on FHIR-based healthcare platforms and EHR integrations often incorporates these controls from day one. Encryption layers, role-based authentication, and audit-ready logs are embedded at the architecture level, ensuring that data residency and regulatory alignment are addressed proactively rather than reactively.
For U.S. vendors entering Canada, adopting this dual-compliance posture early not only meets legal requirements but also builds trust with healthcare systems that prioritize privacy as a determinant of partnership.
IV. Breach Notification and Enforcement
A. Notification Timelines and Thresholds
Both HIPAA and PIPEDA have clear expectations around breach reporting, but they differ in scope, timelines, and accountability.
Under HIPAA, covered entities must notify the U.S. Department of Health and Human Services (HHS) and affected individuals within 60 days of discovering a breach that affects more than 500 individuals. Smaller breaches must still be documented and reported annually. The law defines a breach as any unauthorized access, use, or disclosure of protected health information (PHI) that compromises its security or privacy.
PIPEDA requires organizations to report any breach of security safeguards involving personal information that poses a “real risk of significant harm” to individuals. Reports must be filed with the Office of the Privacy Commissioner of Canada (OPC) as soon as feasible after discovery. Organizations must also notify affected individuals and keep detailed records of all breaches for at least two years.
The Canadian model emphasizes impact and accountability over strict timelines. Rather than focusing solely on the number of affected individuals, PIPEDA requires companies to assess and document risk factors, including the sensitivity of the information and the likelihood of misuse. This pushes organizations to strengthen detection, response, and communication practices beyond simple compliance.
B. Enforcement and Penalties
HIPAA violations fall into four tiers based on the level of negligence, ranging from unknowing violations to willful neglect. Fines can reach up to 1.5 million dollars per year per violation type, and enforcement is handled by the Office for Civil Rights (OCR). The OCR also publishes public breach listings, creating reputational risk that often outweighs financial penalties.
PIPEDA’s enforcement historically relied on investigation and recommendation, but upcoming reforms under Bill C-27 and the proposed Consumer Privacy Protection Act (CPPA) will introduce stronger penalties and binding orders. Under the CPPA, organizations could face fines of up to 5 percent of global revenue or 25 million Canadian dollars, whichever is higher, for serious violations.
For U.S. healthtech companies entering the Canadian market, these enforcement shifts signal a new level of regulatory scrutiny. Canadian authorities increasingly expect audit-ready documentation, detailed breach assessment protocols, and proof of corrective measures.
Building proactive controls pays off. Encryption of health data at rest and in transit, detailed audit trails, and least-privilege access policies not only reduce breach risk but also demonstrate operational maturity during due diligence with hospitals and payers.
In both frameworks, transparency is the strongest defense. Organizations that document incidents clearly and act swiftly tend to maintain regulator confidence and preserve trust with patients and partners alike.
V. Business Associate vs. Service Provider Obligations
A. Contractual Parallels
Contracts are the backbone of compliance in both HIPAA and PIPEDA, but they operate through different legal structures.
Under HIPAA, covered entities must sign Business Associate Agreements (BAAs) with vendors or partners that handle protected health information. These agreements define roles, responsibilities, and safeguards for data privacy and security. They ensure that business associates follow the same security standards as the covered entity, including breach notification and audit obligations.
PIPEDA, on the other hand, requires organizations to ensure that any third-party service provider offers a “comparable level of protection.” This obligation is not limited to healthcare entities; it applies to all commercial organizations handling personal information. The organization remains accountable for personal data, even if processing is carried out by another party.
For U.S. vendors expanding into Canada, this means contractual diligence extends beyond the typical HIPAA BAA. Service provider clauses must detail security measures, breach response procedures, cross-border data handling disclosures, and ongoing audit rights.
Practical alignment often includes:
- Data Processing Addendums (DPAs) that meet both HIPAA and PIPEDA standards.
- Confidentiality agreements that reference PIPEDA’s accountability requirement.
- Vendor due diligence questionnaires that assess adherence to Canadian privacy norms.
In Canada, regulators expect documentation proving that downstream vendors follow equivalent standards, even if the vendor itself is located outside the country.
B. API and Integration Implications
Cross-border data exchange introduces additional contractual and technical complexity. APIs and integrations that share data between U.S. and Canadian systems must be designed to enforce consent parameters, limit access, and log data flows.
Under HIPAA, such integrations often operate under BAAs and rely on standardized security protocols. Under PIPEDA, the same integrations must also ensure that individuals are informed of where their data is going and under what terms it is being processed.
Consider a U.S. telehealth platform integrating with a Canadian hospital’s electronic medical record (EMR). The integration may involve transmitting health summaries, lab data, and appointment details through a FHIR (Fast Healthcare Interoperability Resources) API. The system must verify that data is shared only with authorized users and that each transmission complies with consent parameters under both jurisdictions.
A well-structured integration agreement should specify:
- Purpose and scope of data sharing, including permitted data types.
- Security controls and encryption standards are applied to each transaction.
- Responsibilities for consent validation and data correction requests.
In this environment, contractual clarity and technical precision work hand in hand. Mindbowser’s interoperability projects, such as secure Epic integrations, demonstrate how well-designed APIs and agreements can align HIPAA’s operational rigor with PIPEDA’s accountability-driven model, building trust on both sides of the border.
VI. Interoperability and Cross-Border Data Exchange
A. Technical Interoperability
Interoperability is where compliance meets engineering. For organizations expanding across the U.S. and Canadian markets, aligning with HIPAA and PIPEDA requirements within interoperable frameworks such as FHIR (Fast Healthcare Interoperability Resources) and HL7 is critical. These standards define how health information is structured, transmitted, and secured across systems, allowing organizations to maintain both operational efficiency and legal compliance.
HIPAA emphasizes secure transmission through encryption, access controls, and integrity checks, ensuring that PHI remains protected throughout its lifecycle. PIPEDA complements this by requiring transparency and control over data sharing, including consent mechanisms, retention policies, and the ability for patients to request access to or correction of their data.
For cross-border systems, APIs must be designed to verify consent status, authenticate users, and limit disclosures to authorized endpoints. A practical approach involves building privacy-aware FHIR APIs that enforce scoped access, log every transaction, and store consent metadata linked to patient identifiers. This creates an auditable trail of compliance for both U.S. and Canadian regulators.
B. Case Study Insight
Mindbowser’s implementation of Epic integration and wearable data mapping illustrates how compliance-first interoperability drives scalability. In these projects, every data transaction—from wearable sensors to hospital EHRs—passes through encrypted channels governed by access roles and real-time audit checks. This ensures that both HIPAA’s security requirements and PIPEDA’s consent obligations are embedded into the workflow rather than retrofitted later.
For example, during a maternal health pilot, Mindbowser built an Epic integration that consolidated patient vitals from wearable devices into the hospital’s FHIR-based EHR. The design included consent prompts at data capture points, metadata tagging for data lineage, and automated logging to satisfy both HIPAA and Canadian privacy audit expectations.
The outcome was a platform capable of managing health data across jurisdictions without sacrificing speed or usability. Hospitals gained operational assurance, vendors gained regulatory clarity, and patients retained visibility into how their data was used.
C. Lessons for HealthTech Leaders
- Adopt interoperability as a compliance framework, not just a data standard. FHIR APIs that embed consent validation and encryption controls simplify cross-border operations.
- Document every integration touchpoint. Regulators in both countries expect visibility into how data moves, who accesses it, and under what authority.
- Build compliance into design reviews. Product and engineering teams should validate each feature against both HIPAA’s administrative safeguards and PIPEDA’s accountability model.
Cross-border interoperability is no longer just a technical milestone. It has become a market differentiator for healthtech companies aiming to build trusted, scalable systems across North America.
Accelerate readiness, cut costs, and stay compliant — all before you apply
VII. Operationalizing Dual Compliance
A. Building Internal Readiness
Expanding into the Canadian health data landscape requires more than meeting technical checklists. Dual compliance begins with governance.
Organizations must first conduct a gap assessment that maps existing HIPAA controls against PIPEDA’s accountability and consent expectations. This assessment should evaluate policies, vendor agreements, patient communication protocols, and breach management procedures.
The next step is to structure internal policies under recognized security frameworks such as NIST, SOC 2, or ISO 27001. These frameworks serve as unifying baselines that demonstrate both security rigor and operational maturity. While HIPAA focuses on safeguards and documentation, PIPEDA demands proof that privacy is embedded throughout data operations.
Building readiness also means developing a culture of accountability. Regular privacy impact assessments, vendor audits, and internal reviews create documentation that regulators expect to see during investigations or certification processes. Training employees on data privacy is equally critical, especially for support and development teams handling identifiable data from both U.S. and Canadian patients.
B. Workflow Automation
Once governance frameworks are in place, organizations can operationalize compliance through technology.
Tools that automate consent management, access control, and breach detection make dual compliance sustainable at scale. For instance, a patient’s consent choices under PIPEDA must remain traceable through every system touchpoint. Automating this process ensures consistency and audit readiness.
Accelerators such as HealthConnect CoPilot and WearConnect exemplify how workflow automation bridges regulatory frameworks. They help track data lineage, maintain encrypted communication between devices and EHR systems, and log every access event in compliance with both HIPAA and PIPEDA.
Embedding these automated checks reduces administrative burden while increasing regulatory confidence. Hospitals and health systems are more likely to partner with vendors who demonstrate active privacy controls and traceable compliance processes.
C. Scaling Governance Across Jurisdictions
Maintaining compliance across borders requires unified oversight. Many organizations implement a Privacy Governance Committee to review incidents, vendor changes, and new data flows. This body ensures that each decision aligns with both U.S. and Canadian obligations.
Documentation plays a vital role here. Every policy update, vendor onboarding, and data-sharing request should leave an auditable trail. In Canada, this level of documentation demonstrates accountability; in the U.S., it validates HIPAA’s administrative safeguards.
When designed correctly, dual compliance becomes a strategic advantage rather than an operational burden. Vendors who demonstrate privacy maturity are better positioned to close contracts with hospitals, insurers, and public health programs in both countries.

VIII. Strategic Takeaways for U.S. Vendors
A. Comparative Summary
Understanding the key contrasts between HIPAA and PIPEDA helps U.S. vendors build systems that comply across borders without rework or delays.
HIPAA is a structured, contractual framework centered on covered entities and business associates. It focuses on security controls, administrative safeguards, and clear enforcement paths. Compliance is largely demonstrated through documentation, internal policies, and third-party agreements.
PIPEDA, in contrast, is principle-driven and rooted in accountability. It applies to all organizations handling personal data, not just healthcare entities. Consent and transparency are central, requiring companies to demonstrate that their privacy practices are operational and continuously monitored.
For a U.S. digital health company, this means that being HIPAA-compliant provides a foundation, but not a complete solution. To succeed in Canada, the company must also operationalize explicit consent, cross-border data accountability, and ongoing privacy management.
Mapping these two frameworks early during discovery allows vendors to align product design, technical architecture, and governance models with both regulatory expectations.
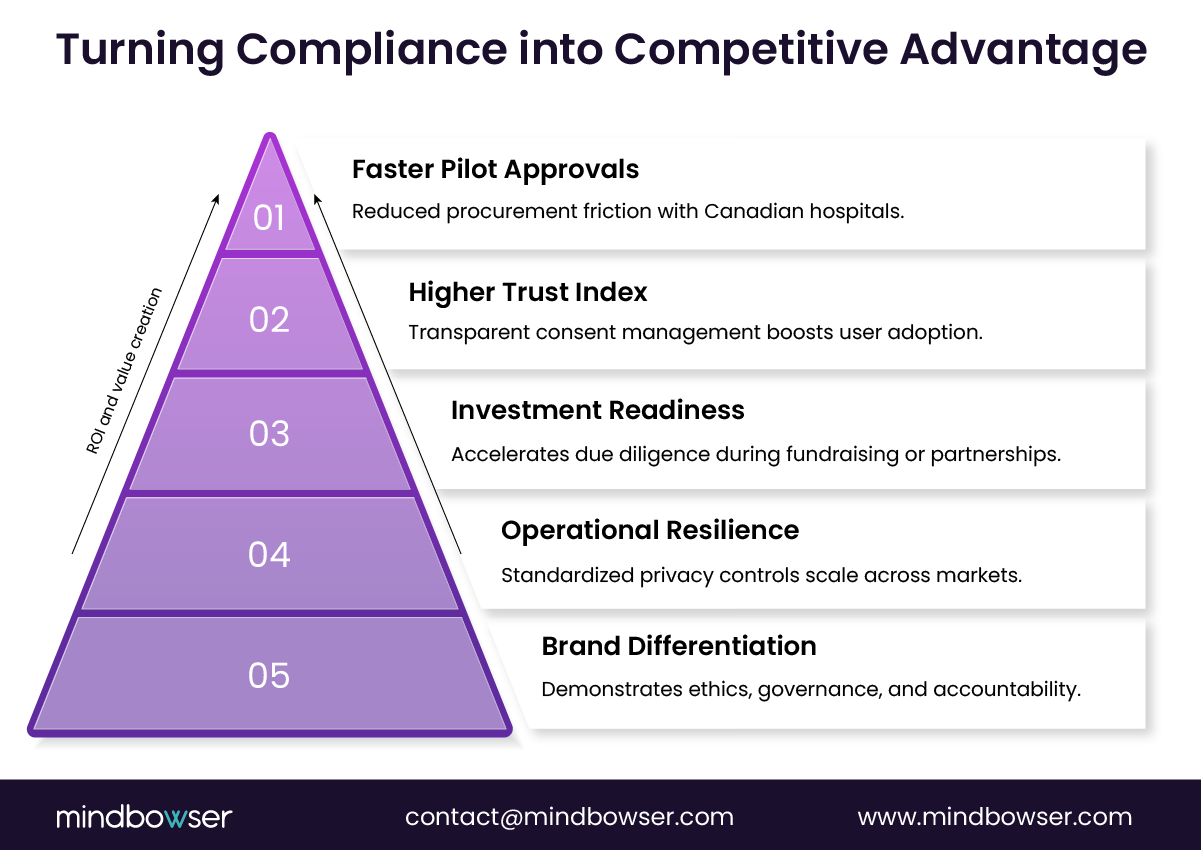
B. Compliance as a Growth Lever
Compliance is no longer a back-office requirement; it is a business advantage.
Hospitals and health systems in Canada increasingly evaluate technology partners on their ability to demonstrate privacy readiness. A vendor that can show dual compliance during early pilot negotiations gains credibility, accelerates contract cycles, and reduces procurement friction.
Implementing a compliance-first discovery process transforms privacy from a constraint into a catalyst. It ensures that design decisions—such as data storage, consent flows, and user access—support scalability from day one. Instead of retrofitting privacy features later, vendors can build systems that align with both U.S. and Canadian requirements from the outset.
For leadership teams, the value is clear. Compliance maturity strengthens investor confidence, streamlines due diligence, and positions the company for faster cross-border expansion.
In essence, PIPEDA vs HIPAA is not just a comparison of two laws; it is a roadmap for operational excellence. Vendors that integrate both frameworks create platforms that are trusted, secure, and ready for growth across North America.
IX. How Mindbowser Can Help?
Mindbowser specializes in helping U.S. digital health and medtech companies navigate the complex path of expanding into Canada with compliance-first engineering and product strategy. The firm’s expertise spans HIPAA, PIPEDA, PHIPA, and other regional privacy frameworks, ensuring that clients enter new markets with confidence and technical readiness.
A. Cross-Border Compliance Expertise
Mindbowser’s team of healthcare technologists and compliance strategists has supported multiple cross-border deployments involving EHR integrations, remote patient monitoring systems, and FHIR-based data platforms. Each implementation embeds privacy and data protection controls at the architectural level, allowing clients to meet both HIPAA and PIPEDA obligations seamlessly.
Examples include:
- Epic and FHIR Integrations that maintain HIPAA-grade encryption while enabling PIPEDA-level consent tracking for Canadian hospitals.
- Wearable Data Platforms designed to synchronize health data through secure APIs with localized data storage in Canadian cloud regions.
- Analytics and AI Solutions configured with dynamic consent models to satisfy PIPEDA’s explicit consent requirements and HIPAA’s permissible use standards.
B. Proven Frameworks and Accelerators
Mindbowser offers a suite of HealthTech accelerators that reduce compliance implementation time and cost:
- HealthConnect CoPilot – Manages FHIR-based data exchange, consent enforcement, and audit reporting.
- WearConnect – Synchronizes data from connected devices under encrypted, compliant pipelines.
- CarePlan AI and AI Medical Summary – Provide secure clinical intelligence while maintaining privacy controls aligned with both regulatory regimes.
These solutions have been deployed in real-world environments, including maternity care management systems, population health programs, and remote patient monitoring platforms.
C. Advisory and Discovery Blueprint
Mindbowser’s Compliance-First Discovery Blueprint helps clients align their data flows, contracts, and technology stack with Canadian and U.S. privacy requirements before development begins. This approach integrates:
- Legal and technical audits of existing architecture.
- Gap analysis between HIPAA and PIPEDA frameworks.
- A roadmap for achieving certification and market readiness.
The result is faster integration with Canadian healthcare partners, reduced legal overhead, and a platform built for long-term scalability.
Mindbowser’s approach ensures that compliance is not an afterthought—it is a design principle that supports innovation and trust across every jurisdiction.
Conclusion
The comparison between PIPEDA and HIPAA reveals more than just regulatory nuance. It reflects two distinct philosophies of protecting health information. HIPAA focuses on defined roles, written policies, and contractual enforcement. PIPEDA emphasizes transparency, accountability, and individual consent as cornerstones of trust.
For U.S. healthtech companies, aligning with both frameworks is not just a compliance exercise; it is a growth strategy. Organizations that design systems around explicit consent, documented accountability, and transparent data practices position themselves to operate confidently in both markets.
The takeaway is simple: build for both from the start. When compliance becomes part of product discovery, integration becomes faster, partnerships become easier, and expansion becomes sustainable. Dual compliance is not a barrier; it is a blueprint for operational excellence in healthcare innovation.
No. PIPEDA is broader and applies to all organizations that handle personal data in commercial activities, while HIPAA governs specific healthcare entities and their associates.
Not federally. However, certain provinces, such as British Columbia and Nova Scotia, require that public-sector health data remain in Canada. Private organizations must still disclose cross-border data storage.
Not automatically. HIPAA compliance ensures security controls, but PIPEDA adds obligations for explicit consent, data access rights, and ongoing accountability.
HIPAA allows implied consent for treatment, payment, and operations. PIPEDA requires explicit, informed consent for any data collection, use, or disclosure.
By integrating consent management, audit logging, and encryption into system architecture, supported by frameworks such as SOC 2 or ISO 27001. Early alignment avoids retrofitting costs and regulatory risk.
