



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
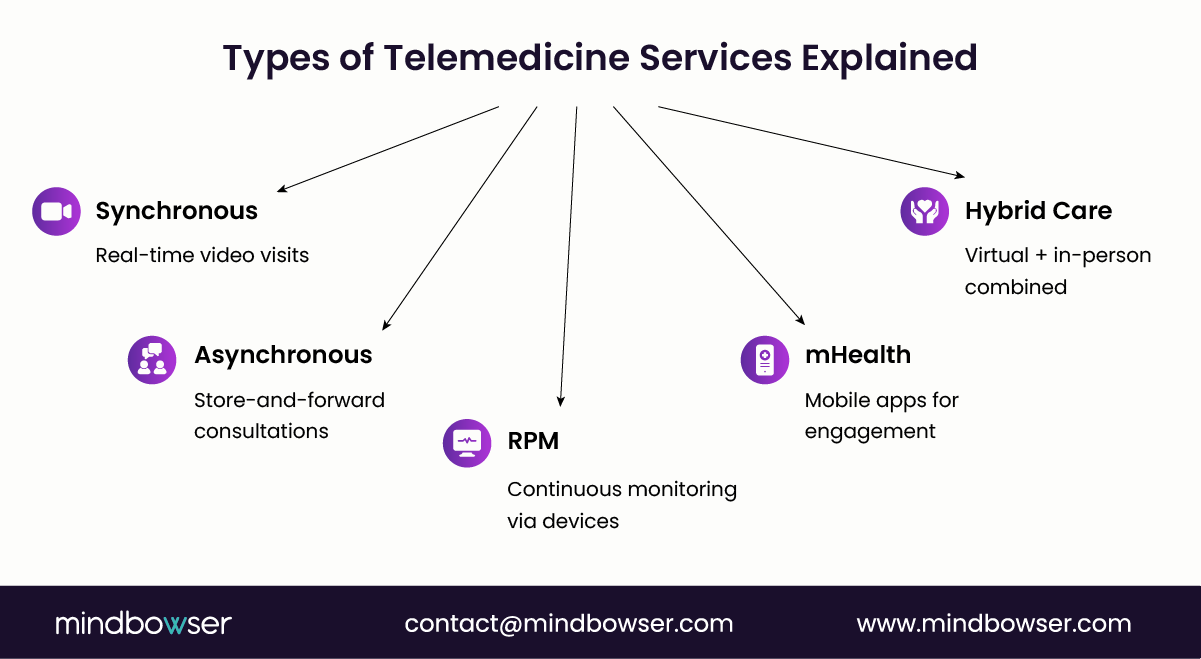
- Telemedicine services include synchronous care, asynchronous care, remote patient monitoring (RPM), mHealth, and hybrid care models, each designed for different clinical needs and workflows.
- Modern digital health platforms combine these services to deliver consultations, diagnostics, and continuous care while integrating data, devices, and clinical systems.
- The real advantage comes from unifying these models into a single platform that supports scalable, coordinated virtual care.
Are you building a telemedicine platform or just adding video visits?
That distinction matters more than most teams realize. The real opportunity lies in understanding the different types of telemedicine services and how they work together to deliver care beyond a single interaction.
From real-time consults to continuous monitoring, each model shapes your product, workflows, and scalability. Get this right, and you are not just enabling virtual visits. You are building the future of care.
I. What Are Telemedicine Services and Why Do They Matter for Digital Health Platforms?
When a founder says, “We’re adding telemedicine,” the real question is not about video. It is about care delivery logic.
Telemedicine services are clinical mechanisms that enable providers to diagnose, monitor, and manage patients at a distance. The distinction matters because digital health platforms are no longer judged on whether they can launch a virtual visit. They are judged on whether they can support the full care workflow: intake, triage, documentation, escalation, follow-up, and data exchange.
The World Health Organization defines telemedicine as the delivery of health care services over distance and notes its value in improving clinical management and extending service coverage.
Telemedicine is no longer a feature layer. It is becoming the operating model for distributed care.
That shift has business consequences. Before the pandemic, telemedicine was often treated as a convenience channel. Today, it sits inside the access strategy, the workforce strategy, and the platform strategy. CDC materials note that telehealth can increase access, reduce costs, and improve outcomes, while also raising critical requirements around privacy, information security, and reimbursement. For product leaders, that is the whole game: access on one side, operational discipline on the other.
A. What Does Telemedicine Mean in Modern Healthcare?
In modern healthcare, telemedicine refers specifically to remote clinical care, while telehealth is the broader umbrella that can also include health education, administrative communication, and non-clinical digital services. WHO describes telemedicine as a specific digital health service for clinical care delivered at a distance, while broader telehealth programs can include a wider set of support functions.
That sounds academic. It is not.
If your platform supports appointment reminders, education modules, and patient messaging, you may be offering telehealth capabilities. If it supports clinician-led diagnosis, treatment decisions, specialist review, or remote ongoing disease management, you are in telemedicine territory. That difference shapes architecture, compliance posture, and workflow depth.
Picture a cardiology startup trying to scale into employer markets. Video visits alone will not do it. The clinical team needs symptom capture, secure data handoff, records access, follow-up logic, and escalation paths when risk rises. In other words, telemedicine is not one interaction. It is a connected clinical workflow.
Telemedicine means remote clinical care. Telehealth is broader. Confuse the two, and you build the wrong product.
B. Why Telemedicine Services Are Critical for Digital Health Startups
Because access is now a product expectation.
CDC reports show that telemedicine became a meaningful part of physician care delivery. In 2021, many primary care physicians and medical specialists said they could provide a similar quality of care during telemedicine visits as during in-person visits, at least to some extent or to a great extent. Specifically, 76.7% of primary care physicians and 73.1% of medical specialists reported similar quality.
That matters for founders and health system buyers alike. It signals that virtual care is no longer limited to edge use cases. It is now part of routine care design.
There is also a real story here. AHRQ notes that telehealth helps address access gaps in underserved areas and can reduce transportation burden while increasing convenience. For startups, that means telemedicine is not only a care delivery model. It is a market expansion model. One platform can extend specialist capacity, reduce no-show friction, and open new geographies without first building a physical footprint.
Ask yourself this: if your growth plan depends on more patients, more providers, and more acuity over time, how could telemedicine not sit at the center of your roadmap?
This works. Period.
Telemedicine services matter because they expand access, widen provider reach, and make hybrid care commercially viable.
C. How Telemedicine Platforms Deliver Virtual Care
A telemedicine platform delivers value when clinical workflows move cleanly from one step to the next.
That usually starts with intake and scheduling, then moves into secure communication, documentation, decision support, and follow-up. The platform must exchange information safely, support the clinician’s workflow, and keep the patient engaged between encounters. CDC highlights privacy and information security as major considerations, while WHO emphasizes implementation design, organizational change, and continuous optimization when scaling telemedicine services.
For a CTO or CIO, the architecture implications are immediate. Real-time consultations need a reliable audio-video infrastructure. Remote diagnostics need structured data capture. Longitudinal care requires persistent patient records, consent management, device feeds, and integration with EHRs or care management systems. Miss one layer, and the care experience breaks. Not always visibly. But operationally, financially, clinically.
A product leader might call it a platform requirement. A clinician might call it workflow integrity. A CFO might call it leakage prevention — same issue.
Virtual care succeeds when the platform supports the visit before it, the decision during it, and the action after it.
Telemedicine platforms do not deliver care solely through video. They deliver care through integrated workflows, secure data exchange, and sustained patient management.
II. What Are the Main Types of Telemedicine Services?
Here’s where most platforms get it wrong.
They build for one care modality and try to stretch it across every use case.
It breaks. Quietly at first. Then at scale.
The reality is simple: telemedicine service types are not interchangeable. Each one solves a different clinical problem, follows a different workflow, and demands a different technical foundation.
Miss that, and your platform becomes a patchwork.
Get it right, and you unlock a true virtual care ecosystem.
Different care moments need different delivery models. One size does not fit clinical reality.
Let’s break them down.
A. What Is Synchronous Telemedicine?
Synchronous telemedicine is a real-time interaction between a clinician and a patient.
Think live conversations. Immediate decisions. Time-bound care.
This is the model most founders start with because it feels closest to traditional care. A scheduled visit. A provider. A patient. A diagnosis.
But here’s the catch.
Real-time care introduces latency sensitivity, scheduling complexity, and clinician time constraints. You are not just building a video. You are building a digital clinic.
A patient logs in. The clinician joins. Symptoms are discussed. Decisions are made. Documentation follows. Prescriptions may be issued.
Simple on the surface. Operationally dense underneath.
1. Examples of synchronous telemedicine services
- Video-based primary care visits
- Telepsychiatry consultations
- Virtual urgent care triage
Picture this: a behavioral health platform scaling across states. Sessions must start on time. Video must not fail. Notes must sync to records. Any delay impacts care quality and provider utilization.
Pressure. Real.
Related read: Behavioral Health Revenue Cycle Management: A Modern Guide
2. Technologies required
To support synchronous care, platforms need:
- Low-latency video infrastructure (WebRTC or similar)
- Real-time messaging and session controls
- Scheduling and provider availability engines
- Clinical documentation workflows
- E-prescription and compliance layers
For CTOs, this is about reliability under load. For clinicians, it is about workflow continuity. For patients, it is about trust.
Synchronous telemedicine mirrors in-person care, but demands high reliability and tight workflow orchestration.
B. What Is Asynchronous Telemedicine (Store-and-Forward)?
Not every clinical decision needs a live interaction.
That is where asynchronous care wins.
Asynchronous telemedicine allows patients and providers to exchange medical information without being present at the same time. Data is captured, stored, and reviewed later.
No scheduling bottlenecks. No real-time dependency.
But new complexities arise: data structures, triage logic, and response workflows.
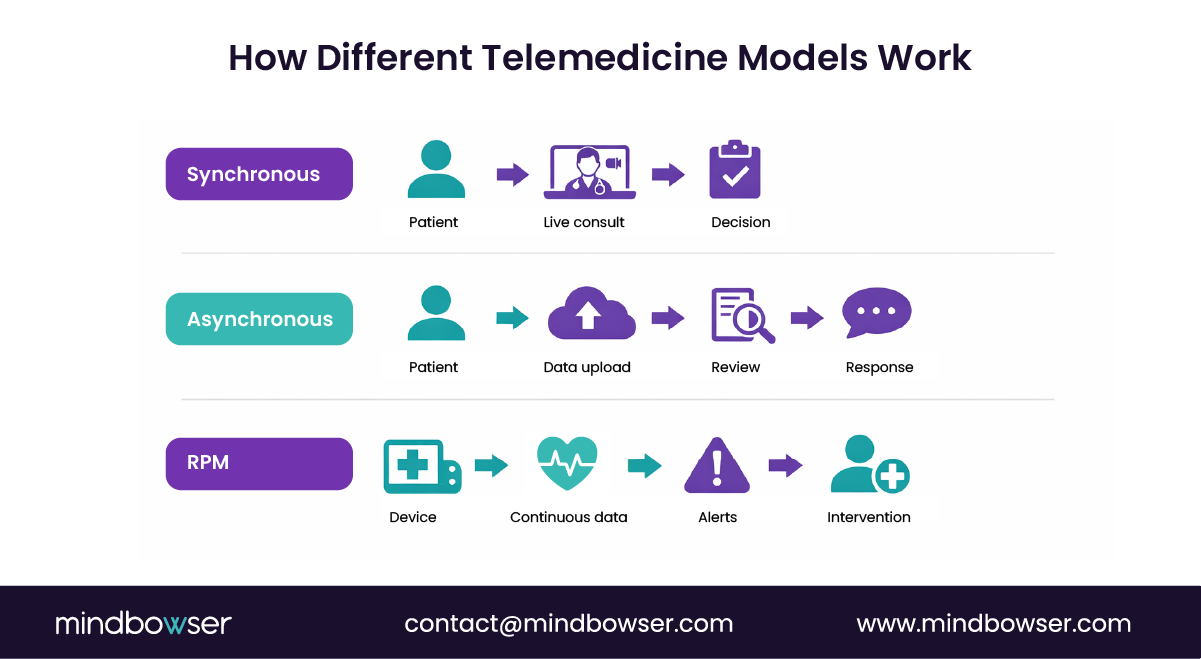
1. How it works
A patient submits symptoms, images, or medical history through a platform.
A clinician reviews the data later, makes a decision, and responds.
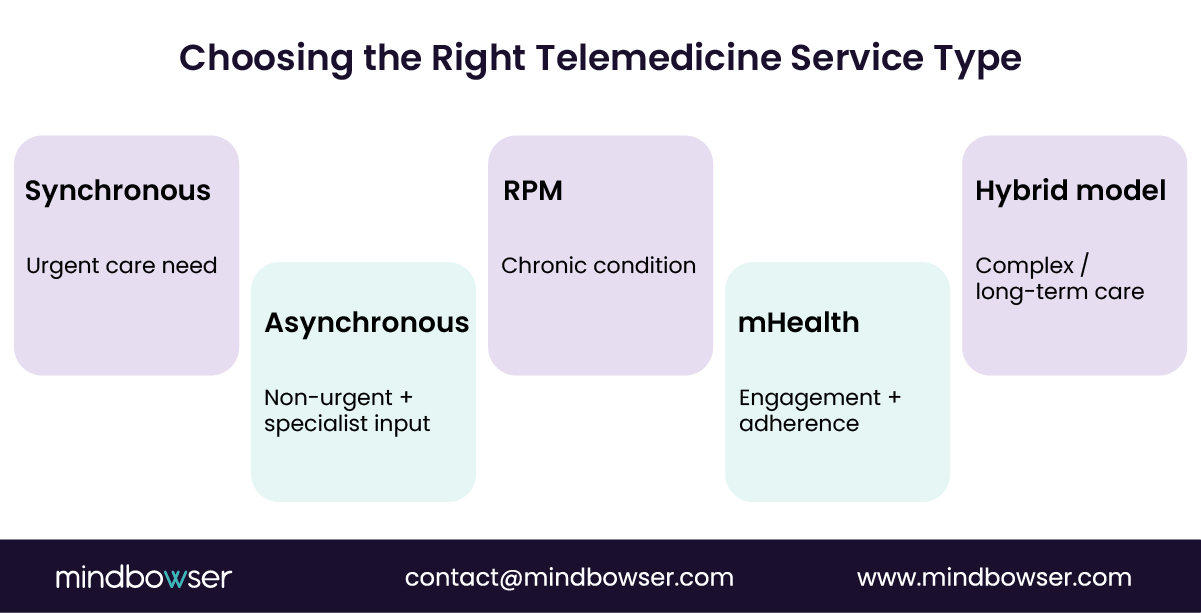
This model works well when:
- The condition is non-urgent
- Visual or structured data is sufficient
- Specialist input is required
It shifts care from time-based to information-based decision-making.
2. Examples
- Teledermatology image reviews
- Radiology or diagnostic interpretations
- Specialist referrals and second opinions
A dermatology startup once scaled 5x without hiring proportionally more clinicians. Why? Asynchronous workflows allowed providers to review cases in batches.
Efficiency. Finally.
Asynchronous telemedicine removes time constraints, but demands structured data capture and disciplined clinical workflows.
C. What Is Remote Patient Monitoring (RPM)?
This is where telemedicine becomes continuous care.
Remote Patient Monitoring (RPM) tracks patient health data in real-time or near-real-time using connected devices — no visit required.
Instead of episodic care, you get longitudinal visibility.
And that changes everything.
The American Heart Association highlights that remote monitoring can improve outcomes in chronic disease management, particularly for conditions like hypertension and heart failure. Continuous data enables earlier intervention. That is the value.
1. Common use cases
- Chronic disease management (diabetes, hypertension)
- Cardiac monitoring and post-discharge care
- COPD and respiratory tracking
Imagine a patient discharged after cardiac surgery. Instead of waiting for a follow-up visit, clinicians receive daily vitals. Alerts trigger if thresholds are crossed.
Care becomes proactive. Not reactive.
2. Technologies used
- Wearable devices (smartwatches, biosensors)
- IoT-enabled medical devices (BP monitors, glucometers)
- Clinical dashboards with alerting systems
- Data ingestion pipelines and analytics layers
Now the challenge shifts to data overload, signal detection, and clinical escalation workflows.
Because collecting data is easy, acting on it is not.
RPM extends care beyond visits, but requires device integration, analytics, and alert-driven workflows.
D. What is Mobile Health (mHealth) in Telemedicine?
The front door to telemedicine is mobile.
mHealth refers to mobile applications that support healthcare delivery, patient engagement, and self-management.
It is not always clinical in isolation. But it is often the entry point into telemedicine services.
1. Examples
- Medication adherence tracking apps
- Digital therapeutics platforms
- Patient monitoring and wellness apps
These tools keep patients engaged between visits. They collect data. They influence behavior.
And behavior is where outcomes live.
2. Role
Mobile platforms act as:
- Engagement layers
- Data collection interfaces
- Communication channels
- Care journey coordinators
A diabetes platform without a strong mobile layer struggles with adherence. A strong one nudges, tracks, reminds, and escalates when needed.
Subtle. Powerful.
mHealth strengthens telemedicine by driving engagement, data capture, and continuity between clinical interactions.
E. What Is Hybrid Care and Hospital-at-Home Telemedicine?
This is the endgame.
Hybrid care combines virtual and in-person services into a single, coordinated care model. Hospital-at-home extends this further by delivering acute-level care at home.
Not theory. Already happening.
According to the American Hospital Association, McKinsey estimates that as much as $265 billion worth of care services could shift from traditional facilities to the home.
That is not incremental change. That is system redesign.
In hybrid models:
- Telemedicine handles triage, follow-ups, and monitoring
- In-person care handles procedures and complex interventions
- RPM bridges the gap with continuous data
A health system building a virtual ward must coordinate devices, clinicians, logistics, and escalation protocols. One failure point can impact outcomes.
High stakes.
Benefits for health systems and digital health providers:
- Reduced hospital burden
- Improved patient experience
- Lower cost of care delivery
- Expanded capacity without physical expansion
Hybrid care is not about replacing hospitals. It is about redefining where care happens.
Hybrid and hospital-at-home models combine multiple telemedicine service types to deliver scalable, patient-centric care ecosystems.
Need a Telemedicine Platform That Supports Video, RPM, and Hybrid Care? Let’s Talk.
III. How Digital Health Platforms Deliver Telemedicine Services
Here’s the shift: telemedicine is no longer a feature stack. It is a platform architecture problem.
If your system cannot support multiple types of telemedicine services in one flow, care breaks between steps. Intake works. Visits work. Follow-ups fail.
Seen it too often.
Virtual care fails in the gaps between systems, not inside them.
A. What Platform Capabilities Are Required for Telemedicine?
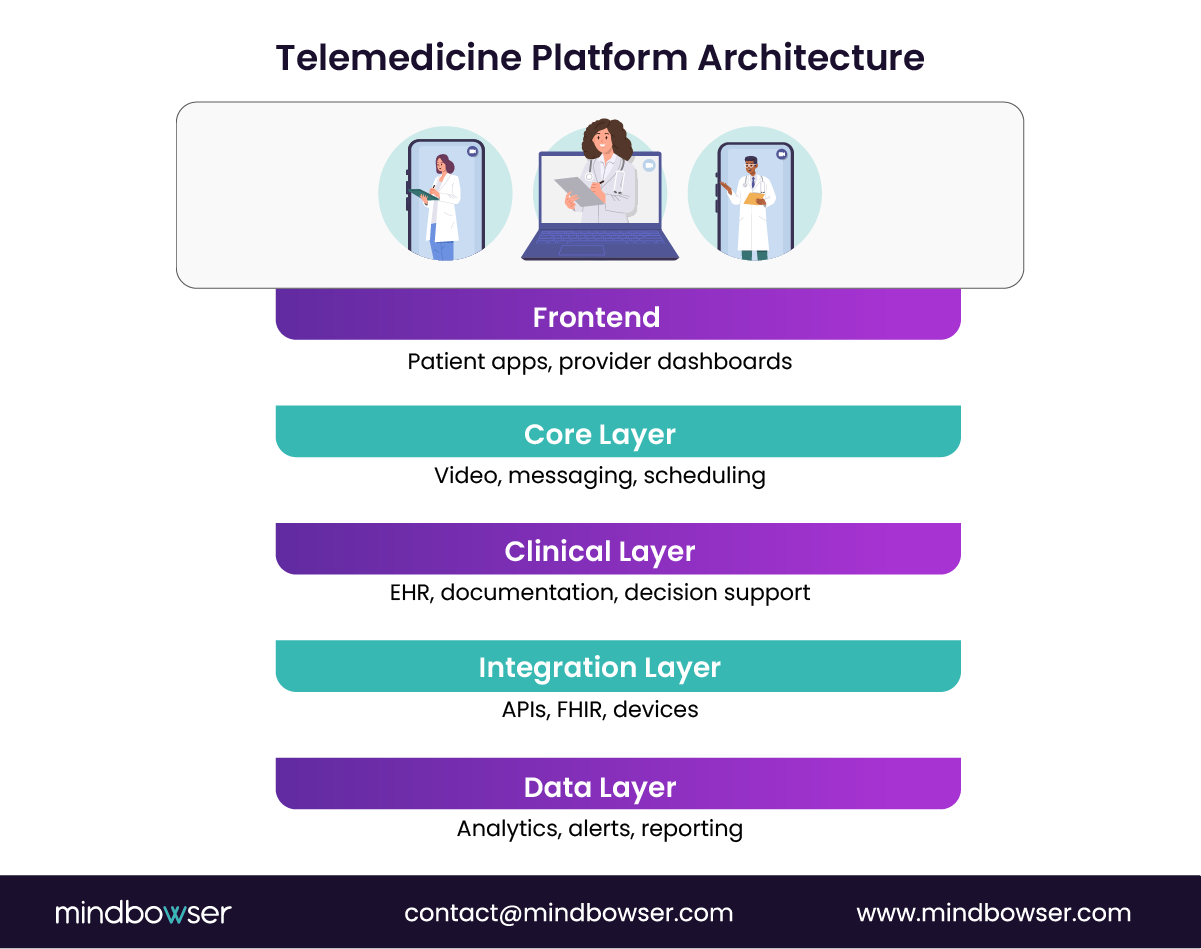
At a minimum, your platform must support three layers:
Care delivery layer → secure video, messaging, async inputs
Care coordination layer → scheduling, triage, routing
Clinical layer → documentation, decision support, orders
Skip one, and workflows fragment.
A CTO at a scaling virtual care company once said, “Video was easy. Coordinating care after the visit was the real challenge.” Friction. Predictable.
Core capabilities include:
- Secure video consultations with low latency
- Appointment scheduling with provider logic
- Digital patient records with structured inputs
- Clinical documentation tied to workflows
And one more thing. Often missed.
Context continuity.
The system must remember what happened before the visit and guide what happens next.
Telemedicine platforms must support the full care loop, not just the interaction.
B. How Telemedicine Platforms Integrate with Healthcare Systems
No platform operates in isolation. Ever.
Telemedicine platforms must connect with:
- EHR systems
- Labs and imaging systems
- Pharmacy networks
- Payer systems
FHIR-based interoperability is now table stakes. Without it, data stays trapped.
And trapped data kills care velocity.
ONC emphasizes interoperability as critical for care coordination and patient outcomes. That is not policy talk. That is product reality.
A patient completes a virtual consult. If that data does not sync to the EHR, the next provider starts blind.
Risk rises. Costs rise. Trust drops.
Integration is not a backend concern. It is a clinical requirement.
C. Key Technologies That Power Telemedicine Platforms
Under the hood, three technology pillars matter:
1. Cloud infrastructure
Supports scale, uptime, and data flow across services
2. Telehealth APIs and SDKs
Enable video, messaging, and scheduling without rebuilding everything
3. Data + intelligence layers
Support triage, alerts, and decision support
Add RPM, and complexity jumps:
- Device integrations
- Data ingestion pipelines
- Alert management systems
Now the question becomes:
- Can your platform handle continuous data, not just episodic visits?
- Because that is where the market is heading.
- Platforms that manage continuous care will outpace those built only for encounters.
The winning platforms are not video-first. They are data-first, workflow-driven, and integration-ready.
IV. How Digital Health Platforms Deliver Telemedicine Services
Here’s the shift: telemedicine is no longer a feature stack. It is a platform architecture problem.
If your system cannot support multiple types of telemedicine services in one flow, care breaks between steps. Intake works. Visits work. Follow-ups fail.
Seen it too often.
Virtual care fails in the gaps between systems, not inside them.
A. What Platform Capabilities Are Required for Telemedicine?
At a minimum, your platform must support three layers:
- Care delivery layer — secure video, messaging, async inputs
- Care coordination layer — scheduling, triage, routing
- Clinical layer — documentation, decision support, orders
Skip one, and workflows fragment.
A CTO at a scaling virtual care company once said, “Video was easy. Coordinating care after the visit was the real challenge.” Friction. Predictable.
Core capabilities include:
- Secure video consultations with low latency
- Appointment scheduling with provider logic
- Digital patient records with structured inputs
- Clinical documentation tied to workflows
And one more thing. Often missed.
Context continuity.
The system must remember what happened before the visit and guide what happens next.
Telemedicine platforms must support the full care loop, not just the interaction.
B. How Telemedicine Platforms Integrate with Healthcare Systems
No platform operates in isolation. Ever.
Telemedicine platforms must connect with:
- EHR systems
- Labs and imaging systems
- Pharmacy networks
- Payer systems
FHIR-based interoperability is now table stakes. Without it, data stays trapped.
And trapped data kills care velocity.
ONC emphasizes interoperability as critical for care coordination and patient outcomes. That is not policy talk. That is product reality.
A patient completes a virtual consult. If that data does not sync to the EHR, the next provider starts blind.
Risk rises. Costs rise. Trust drops.
Integration is not a backend concern. It is a clinical requirement.
C. Key Technologies That Power Telemedicine Platforms
Under the hood, three technology pillars matter:
1. Cloud infrastructure
Supports scale, uptime, and data flow across services
2. Telehealth APIs and SDKs
Enable video, messaging, and scheduling without rebuilding everything
3. Data + intelligence layers
Support triage, alerts, and decision support
Add RPM, and complexity jumps:
- Device integrations
- Data ingestion pipelines
- Alert management systems
Now the question becomes:
Can your platform handle continuous data, not just episodic visits?
Because that is where the market is heading.
Platforms that manage continuous care will outpace those built only for encounters.
The winning platforms are not video-first. They are data-first, workflow-driven, and integration-ready.
V. How Mindbowser Helps Digital Health Companies Build Telemedicine Platforms
Most platforms fail at integration, not intention.
They launch fast. Then stall when adding new telemedicine services, such as RPM or asynchronous care.
That is where a custom-built strategy matters.
Speed gets you to launch. Architecture gets you to scale.
A. Custom Telemedicine Platform Development
Mindbowser designs telemedicine platforms as modular, compliant systems from day one.
That means:
- HIPAA-compliant architecture baked into every layer
- Secure virtual consultation modules (video + messaging)
- Scalable infrastructure designed for multi-service expansion
Not just video visits. Full care delivery.
A common scenario: a startup begins with synchronous care, then needs to add RPM. Without the right foundation, it becomes a rebuild.
With a modular architecture, it becomes an extension.
Build once for multiple care models, not one at a time.
B. Integrating Multiple Telemedicine Services into a Unified Platform
The real value comes from combining services into one experience.
Mindbowser helps platforms unify:
- Video consultations for real-time care
- Asynchronous workflows for specialist review
- Remote patient monitoring for continuous care
All connected through shared patient data and workflows.
No silos. No duplicated systems.
A VP of Product at a digital health company put it simply: “We didn’t need more features. We needed them to work together.”
That is the difference between tools and platforms.
Unified telemedicine platforms drive better outcomes and lower operational friction.
C. Accelerators That Speed Telemedicine Platform Development
Time matters. But so does correctness.
Mindbowser uses pre-built accelerators to reduce build time while maintaining compliance and flexibility:
- Clinical workflow automation frameworks
- AI-driven patient engagement modules
- Integration layers for EHR, devices, and APIs
These accelerators help teams launch faster while avoiding rework later.
From the blueprint: platforms using accelerators can launch up to 40% faster while maintaining full ownership of IP.
That balance matters to Series B+ teams scaling under pressure.
Accelerators reduce time to market, but the architecture ensures long-term scale.
The Future of Telemedicine Services in Digital Healthcare
Telemedicine has moved from isolated video visits to fully connected care ecosystems. The different types of telemedicine services — synchronous, asynchronous, RPM, and hybrid care — now work together to deliver continuous, coordinated care across settings. For digital health platforms, the shift is clear: supporting one model is not enough, and disconnected features will not scale. The future belongs to platforms that unify workflows, data, and care delivery into a single system that supports both virtual and in-person care.
The core types of telemedicine services include synchronous (real-time), asynchronous (store-and-forward), and remote patient monitoring (RPM). Most modern platforms also include mHealth and hybrid care to support continuous and coordinated care delivery.
Most startups begin with synchronous care for a faster go-to-market, then expand into asynchronous workflows and RPM as they scale. The right sequence depends on clinical use case, patient volume, and care complexity.
RPM enables continuous patient visibility without increasing visit load, making it essential for chronic care and value-based models. It shifts care from reactive visits to proactive intervention.
The main challenges include workflow fragmentation, EHR integration, data security, and clinician adoption. Most failures happen not in the visit itself, but in what happens before and after it.
No. Telemedicine works best as part of a hybrid care model, where virtual and in-person services complement each other. The goal is not replacement, but delivering the right care in the right setting.


