BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR
Epic Care Everywhere is not just data exchange. It brings real-time patient data into clinical workflows where decisions happen. That means faster ED decisions, fewer duplicate tests, and better care continuity. But gaps remain, especially with non-Epic systems and data reconciliation. Smart health systems are now extending Care Everywhere using FHIR, AI, and custom integration layers to turn passive data into actionable clinical intelligence.
Missing data + time pressure = clinical risk?
Every day, clinicians make high-stakes decisions with incomplete patient histories and seconds to act. Epic Care Everywhere changes that by bringing external patient data directly into the workflow, where it actually matters.
But access alone doesn’t guarantee better outcomes; the real impact depends on how well that data is integrated, interpreted, and used.
This blog breaks down how Care Everywhere works in practice and where health systems still face critical gaps.
I. What Is Epic Care Everywhere? (And Why It’s Central to Interoperability Strategy)
What happens when a patient shows up in your ED with no history and you have 30 seconds to decide?
That’s not a rare scenario. It’s a daily reality.
Epic Care Everywhere exists for this exact moment.
At its core, Epic Care Everywhere is an interoperability network built into Epic Hyperspace. It allows clinicians to securely query and retrieve patient data from other participating organizations in real time. No switching systems. No manual calls. Just data, where it matters.
Here’s what becomes instantly accessible:
- Diagnoses
- Medications
- Allergies
- Lab results
- Clinical notes
This creates a longitudinal patient record at the point of care. Not fragmented snapshots. Not outdated summaries. A connected clinical story.
According to HIMSS, interoperability is a critical priority for healthcare organizations, enabling effective data exchange and care coordination.
Now here’s the critical distinction.
Traditional HIEs often sit outside clinician workflows—separate portals. Extra steps. Low adoption.
Care Everywhere flips that model.
It is embedded directly into the clinical workflow. The physician does not go looking for data. The data comes to them, inside their existing screens.
That changes behavior.
No friction. No delay. Just context.
A clinician reviewing medications during admission can instantly pull external records. An ED physician can check prior imaging before ordering another scan. A specialist can see what happened across systems without having to guess.
This works. Period.
But here’s the tension.
While Care Everywhere solves intra-Epic interoperability at scale, it still leaves gaps when data originates outside Epic environments. And that’s where most CIOs start asking harder questions.
Care Everywhere is not just an interoperability feature. It is a decision-enabling layer inside clinical workflows. The real question is not whether you have it, but whether you are fully using it.
II. How Epic Care Everywhere Works (Architecture + Data Flow)
It looks simple to the clinician. Behind the scenes, it’s anything but.
Epic Care Everywhere runs on a query-based exchange model. That means data is not pushed continuously. It is pulled when needed, at the moment of care.
Think about the workflow.
A patient arrives. The chart opens. The clinician triggers a Care Everywhere query. Within seconds, external organizations respond with available records.
That interaction depends on three core components:
A. Core Architecture Components
1. Query-Based Exchange (Pull Model)
Instead of flooding systems with unnecessary data, Care Everywhere retrieves information only when requested. This keeps workflows fast and relevant.
2. Patient Matching Algorithms
Accurate matching is critical. The system uses demographic and identifier-based algorithms to ensure the right patient data is retrieved. A mismatch here is not a minor issue. It is a clinical risk.
3. Hybrid Data Exchange (Documents + Discrete Data)
Care Everywhere supports both:
- Document-based exchange (CCD / C-CDA)
- Structured data elements (labs, meds, allergies)
This hybrid model allows clinicians to read context and act on structured data.
B. Integration Standards Behind the Scenes
Care Everywhere does not operate in isolation. It connects through established interoperability standards:
- HL7 for legacy integrations
- CCD / C-CDA for clinical summaries
- FHIR APIs in newer layers for faster, flexible access
FHIR is where things are heading. But most environments still run a mix.
This creates both flexibility and complexity.
C. Real-Time Data Flow in Practice
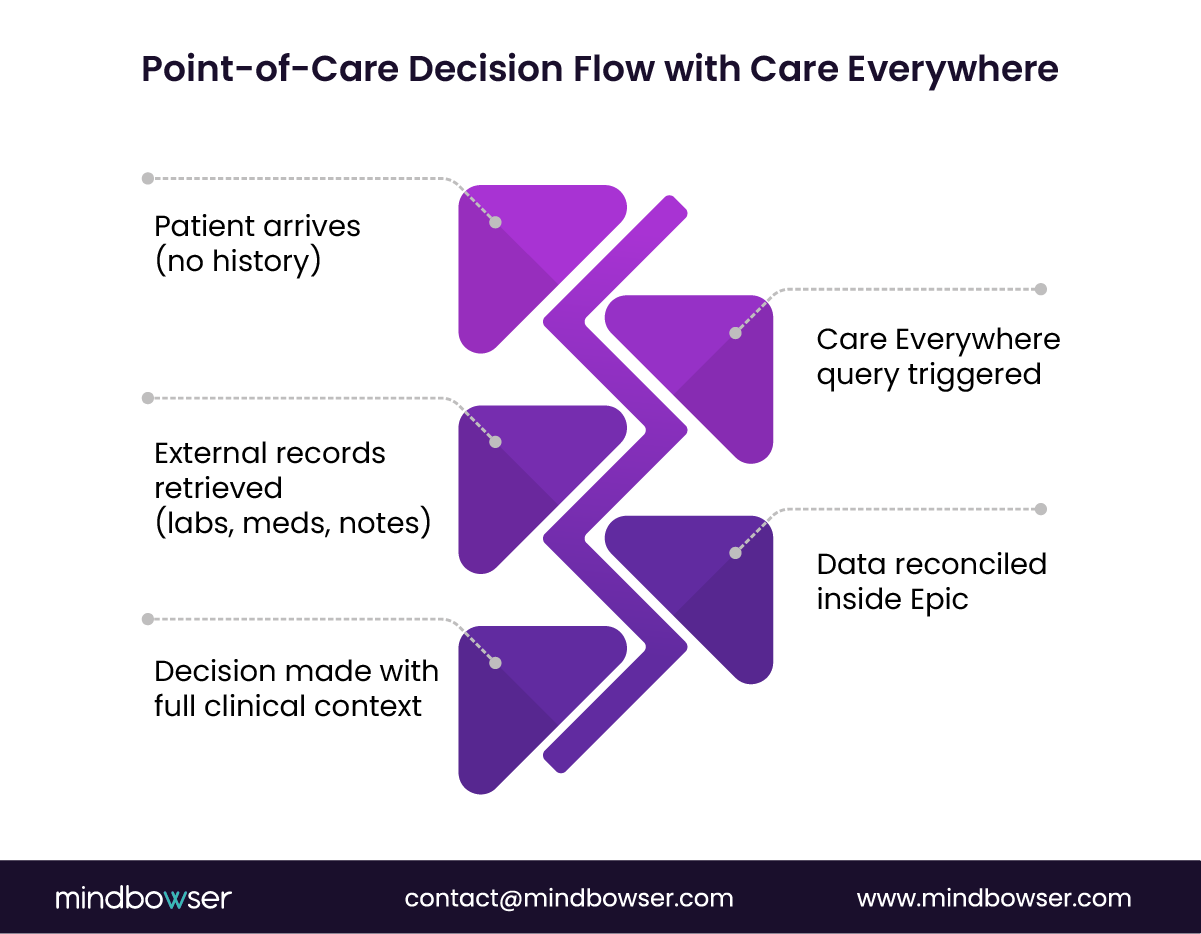
Let’s break it down step by step:
1. Patient Encounter Begins
The clinician opens the patient chart inside Epic.
2. Care Everywhere Query Triggered
The system sends requests to connected organizations.
3. External Records Returned
Participating systems respond with available patient data.
4. Data Reconciliation Inside Epic
Here’s the differentiator.
The data is not just displayed. It is reconciled.
Medications can be reviewed and merged. Allergies validated. Problems added to the chart. This turns external data into clinically usable information.
According to Healthcare IT News, Epic’s interoperability network has seen a significant increase in cross-organizational data exchange volumes. That scale only works because the workflow is embedded.
D. The Real Differentiator: Embedded Reconciliation
Most interoperability tools stop at visibility.
Care Everywhere goes further.
It asks: what will the clinician do with this data?
That’s why reconciliation workflows are built in. Clinicians can act, not just observe.
But here’s the friction point.
Manual reconciliation still adds cognitive load. When data volumes increase, clinicians can feel overwhelmed.
The architecture is strong, the data flow is fast, but without automation, the burden shifts to the clinician. And that’s where the next level of innovation is happening.
III. Where Care Everywhere Fits Across Epic Modules (Real Clinical Workflows)
This is where strategy meets reality.
Care Everywhere is not a single feature. It shows up differently across Epic modules, shaping real clinical decisions in ways most executives underestimate.
Same data. Different impact. Different stakes.
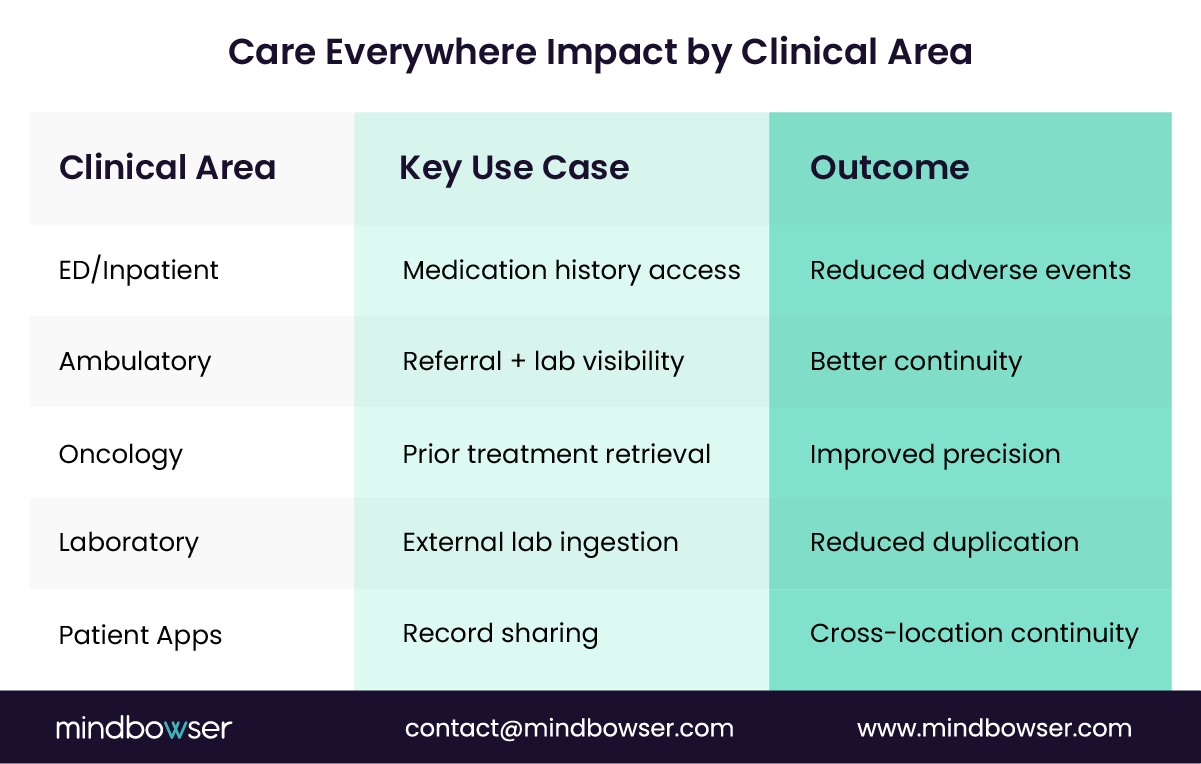
A. Emergency & Inpatient (Epic ClinDoc + Epic ASAP)
Unknown patient. No history. High risk.
In the ED, speed is everything.
Care Everywhere helps clinicians:
- Identify patients with prior encounters elsewhere
- Retrieve medication history during admission
- Detect allergies and prior diagnoses instantly
This directly reduces adverse drug events. The CDC estimates that over 1.5 million preventable adverse drug events occur annually in the U.S.many linked to incomplete medication histories.
Here, interoperability is not convenience. It is safety.
B. Epic Ambulatory Care
Outpatient workflows depend on continuity.
Care Everywhere enables providers to:
- Access specialist notes from external systems
- Review lab results without repeat testing
- Maintain referral continuity across organizations
What happens when referral data is missing? Delays. Redundant work. Patient frustration.
With Care Everywhere, the care journey stays connected.
C. Oncology (Epic Beacon)
Cancer care is longitudinal and complex.
Clinicians need:
- Prior chemotherapy protocols
- Toxicity history
- Treatment response data
Care Everywhere allows oncologists to reconstruct treatment timelines across institutions.
According to WHO, cancer cases are expected to rise by 60% globally over the next two decades. That scale demands continuity, not fragmentation.
Missing one treatment detail can change outcomes.
D. Laboratory (Epic Beaker)
Lab data is one of the most duplicated areas in healthcare.
Care Everywhere supports:
- Ingestion of external lab reports
- Alignment of lab compendiums across organizations
This reduces unnecessary repeat tests.
Less duplication. Lower cost. Faster care.
E. Patient-Facing (Epic MyChart & Epic Care Companion)
Patients are no longer passive participants.
Through MyChart and Care Companion:
- Patients can share records across providers
- Care continuity improves across geographies
A patient moves cities. Care continues. No reset.
That shift is subtle but powerful.
F. Community Access (EpicCare Link)
Not every provider uses Epic.
EpicCare Link extends access by allowing external providers to:
- Query patient data
- View relevant records without a full Epic deployment
This expands the network without forcing standardization.
Here’s the strategic insight most teams miss.
Care Everywhere is not just a backend capability. It is a workflow amplifier.
Same infrastructure. Different outcomes depending on how it is used.
- In ED → speed and safety
- In ambulatory → continuity
- In oncology → precision
- In labs → cost control
So the real question becomes:
Are your clinicians actively using these workflows or bypassing them because they slow things down?
Care Everywhere delivers value only when it is embedded, adopted, and aligned with real workflows. Otherwise, it becomes just another data layer that clinicians ignore.
IV. Epic Care Everywhere vs Share Everywhere vs Interoperability Ecosystem
Most leadership teams get this wrong.
They assume Epic Care Everywhere equals interoperability.
It doesn’t.
And that misunderstanding leads to underutilization, missed ROI, and poor integration strategy.
Let’s break it down clearly.
A. Care Everywhere: System-Driven Provider Exchange
Care Everywhere is designed for:
- Provider-to-provider data exchange
- Automated querying between Epic-connected organizations
- Real-time clinical access during workflows
No patient involvement required.
It operates silently in the background, triggered by clinician actions.
This is your operational backbone.
B. Share Everywhere: Patient-Controlled Access
Share Everywhere works differently.
- Patients generate secure access tokens or links
- External providers use those links to view records
- No deep system integration required
This is patient-mediated interoperability.
It becomes useful when:
- The receiving provider is not part of Epic Networks
- Quick, temporary access is needed
- Formal integrations are not available
Think urgent care visits, second opinions, or out-of-network consults.
C. The Full Interoperability Ecosystem Inside Epic
Epic’s interoperability strategy is not one tool. It is a layered ecosystem:
- Care Everywhere
- Share Everywhere
- Happy Together (multi-Epic instance consolidation)
- FHIR APIs for modern integrations
Each plays a different role.
Together, they define your interoperability maturity.
D. Where Executives Misstep
“We have Care Everywhere, so we’re covered.”
That assumption shows up often. And it creates blind spots.
Here’s what gets missed:
1. Patient-Mediated Gaps
Without Share Everywhere, patients cannot easily bridge non-integrated providers.
2. API-Driven Extensions
Without FHIR, external apps, analytics, and automation layers remain limited.
3. Multi-System Complexity
Without a broader strategy, organizations struggle when dealing with hybrid EHR environments.
E. Strategic Framing for CIOs
Think of it this way:
- Care Everywhere → Clinical workflow interoperability
- Share Everywhere → Patient-driven access
- FHIR APIs → Innovation and extension layer
Three layers. One strategy.
Ignore one, and the system weakens.
Here’s the real takeaway.
Care Everywhere is powerful, but it is not complete on its own.
The organizations seeing the most value are not just using it. They are orchestrating it alongside other interoperability tools.
So ask yourself: Are you running a toolor designing a system?
Interoperability is not a feature. It is an ecosystem. And Care Everywhere is just one piece of it.
V. Adoption Trends & Data Exchange Scale (What the Market Data Shows)
Interoperability is no longer a pilot. It is infrastructure.
Over the past few years, Epic Care Everywhere has moved from a “nice-to-have” feature to a core operational dependency for health systems.
The shift is not subtle. It is measurable.
A. Scale of Data Exchange Is Exploding
Epic reports a sharp rise in:
- Cross-organization patient record exchange
- Daily query volumes across networks
- Total volume of shared clinical data
According to Healthcare IT News, Epic’s network has seen a significant year-over-year increase in data exchange activity, especially post-2020.
COVID changed behavior.
Providers needed access to patient data across locations, fast. That urgency accelerated adoption across:
- Hospitals
- Ambulatory clinics
- Health systems
- Even payer-connected workflows in some cases
What started as optional became essential.
B. Network Effects Are Driving Value
Interoperability scales differently than most technologies.
The more participants, the more value.
As more organizations join Epic’s network:
- Data completeness improves
- Clinical confidence increases
- Decision-making becomes faster
This creates a compounding effect.
More connections → more data → better outcomes
But there is a catch.
Not all systems participate equally. Non-Epic environments still create fragmentation points.
C. Executive Reality: Baseline Expectation, Not Differentiator
A few years ago, interoperability was a competitive advantage.
Today, it is expected.
According to HIMSS, interoperability maturity is a critical component of digital health advancement and care coordination across health systems.
If you cannot access external data, you are already behind.
That changes how CIOs should think about Care Everywhere.
It is not the finish line. It is the starting point.
D. The Hidden Shift: From Access to Action
Here’s where leading organizations are moving next.
Access to data is no longer enough.
The focus is shifting to:
- Making data actionable inside workflows
- Reducing clinician burden during reconciliation
- Using external data for predictive insights
Can your clinicians act on the data, or just see it?
That question defines maturity.
Adoption is rising fast, and interoperability is now table stakes. The real opportunity is not in accessing more data, but in turning exchanged data into faster, smarter clinical decisions.
Talk to our Epic integration team
VI. Clinical and Financial ROI of Epic Care Everywhere
This is where interoperability stops being IT and starts being a financial strategy.
Most CIOs know Care Everywhere improves access. Fewer quantify what that access actually delivers.
Let’s make it concrete.
A. Clinical Impact: Faster, Safer Decisions
When external data is available at the point of care, clinicians move faster with more confidence.
Care Everywhere directly enables:
- Faster decision-making in emergency settings
- Reduced duplicate testing
- Improved medication reconciliation
- Better coordination for chronic conditions
What changes when the full medication list is visible instantly?
Errors drop. Decisions improve. Outcomes follow.
This is not an incremental improvement. It is risk reduction at scale.
B. Financial Impact: Cost Reduction Across the Care Journey
Every duplicate test is avoided. Every readmission is prevented. Every unnecessary delay is removed.
That is where ROI shows up.
Care Everywhere contributes to:
- Lower cost per patient encounter
- Reduced readmissions
- Improved quality scores tied to reimbursement
Translation: better data equals lower cost.
C. Example ROI Model (What Leaders Actually Measure)
Let’s break this into operational metrics:
1. Avoided Duplicate Labs
If even 10–15% of labs are avoided through external visibility, savings compound quickly across high-volume systems.
2. Reduced Length of Stay (LOS)
Faster access to prior records means fewer delays in diagnosis and discharge decisions.
Even a small LOS reduction drives major financial impact.
3. Fewer Adverse Events
Better medication reconciliation reduces complications, which lowers both cost and compliance risk.
D. The Hidden ROI Lever: Clinician Efficiency
This often goes unmeasured.
How much time does a clinician spend chasing missing information?
Without interoperability:
- Calls to external providers
- Manual record requests
- Delayed decisions
With Care Everywhere:
- Data appears instantly
- Less administrative friction
- More time for patient care
Better interoperability reduces cognitive load.
That is ROI you feel, even if it is harder to quantify.
Here’s the executive takeaway.
Care Everywhere does not just improve care. It improves unit economics of healthcare delivery.
- Better outcomes
- Lower costs
- Faster workflows
Three levers. One system.
But, and this is critical, these outcomes only materialize when the system is actively used and optimized.
The ROI is real, but it is not automatic. It depends on workflow adoption, data quality, and how well you extend the platform beyond its default capabilities.
VII. Limitations and Challenges CIOs Must Address
This is where most implementations stall.
On paper, Care Everywhere looks complete. In practice, gaps appear quickly once you move beyond ideal workflows.
The issue is not access. It is consistency, usability, and control.
A. Interoperability Gaps Beyond Epic
Care Everywhere performs best inside Epic ecosystems.
But healthcare is not uniform.
Key challenges include:
- Limited participation from non-Epic systems
- Inconsistent data availability across networks
- Variable data quality depending on source systems
What happens when half the patient story is missing?
Clinicians hesitate. Decisions slow down.
Partial interoperability is still fragmentation.
B. Data Inconsistency and Normalization Issues
Even when data is available, it is not always usable.
Different organizations structure data differently:
- Medication naming variations
- Lab value formatting inconsistencies
- Duplicate or conflicting problem lists
The burden shifts to clinicians to interpret and reconcile.
That is not sustainable at scale.
C. Operational Burden on Clinicians
More data should help. But what if it overwhelms?
Manual reconciliation remains a major source of friction.
Clinicians must:
- Review external records
- Validate relevance
- Merge or discard information
This adds cognitive load during already time-constrained workflows.
Too much unstructured data becomes noise, not value.
D. Governance and Consent Complexity
Interoperability introduces governance challenges:
- Patient consent management across jurisdictions
- Data sharing policies between organizations
- Compliance with evolving regulations
Who owns the data? Who can access it? Under what conditions?
These are not technical questions. They are strategic and legal.
E. Technical Constraints Slowing Progress
Many environments still depend on legacy standards:
- HL7-based integrations limit flexibility
- CCD/C-CDA documents lack granularity
- FHIR adoption is growing, but not universal
This creates a hybrid architecture that is harder to scale and extend.
F. The Strategic Risk: Passive Interoperability
Here’s the biggest risk.
Care Everywhere becomes a passive data viewer.
- Data is available
- But not fully trusted
- Not easily actionable
- Not embedded deeply enough into workflows
So clinicians ignore it.
And when adoption drops, ROI disappears.
This is the inflection point for CIOs.
Do you accept these limitations as “good enough”?
Or do you treat them as signals to evolve your interoperability strategy?
Care Everywhere solves access, but not intelligence. Without addressing data quality, workflow burden, and cross-system gaps, its impact remains limited.
VIII. How to Extend Epic Care Everywhere (Beyond Native Capabilities)
This is where leading health systems pull ahead.
Care Everywhere gives you access. But access alone does not drive transformation.
The real question is simple: What do you do with the data once you have it?
Forward-thinking organizations are extending Care Everywhere into a connected, intelligent interoperability layer.
A. FHIR-Based Integrations for Broader Ecosystems
Care Everywhere works best within Epic networks. But real-world environments are hybrid.
FHIR changes that.
With FHIR APIs, organizations can:
- Connect non-Epic systems
- Integrate third-party applications
- Enable real-time data exchange beyond traditional boundaries
This expands interoperability from network-based to ecosystem-wide.
Without FHIR, you are limited. With it, you extend reach.
B. AI-Driven Clinical Summarization
What happens when a clinician receives 50 pages of external records?
They skim. Or worse, ignore.
AI solves this.
By layering AI on top of Care Everywhere data, organizations can:
- Summarize external patient histories
- Highlight critical events (admissions, allergies, abnormal labs)
- Surface actionable insights in seconds
Less noise. More signal.
This directly reduces cognitive burden and improves decision speed.
C. Automated Reconciliation Workflows
Manual reconciliation is one of the biggest sources of friction.
Automation changes the equation.
- Auto-match medications across sources
- Flag discrepancies intelligently
- Suggest reconciliation actions within workflows
The system assists. The clinician validates.
This shifts interoperability from manual effort to guided intelligence.
D. Population Health Insights from Aggregated Data
Care Everywhere data is not just useful at the individual level.
Aggregated, it becomes a powerful asset for:
- Risk stratification
- Care gap identification
- Chronic disease management
According to McKinsey, data-driven population health strategies can significantly improve outcomes while reducing cost.
More data sources → better predictive accuracy.
E. Real-World Enhancement Examples
Leading systems are already being built:
1. Real-Time Alerts from External Data
Notify care teams when external encounters occur, such as ED visits or hospitalizations.
2. Multi-Source Risk Scoring
Combine internal and external data to predict readmissions or complications.
3. Cross-Org Care Gap Identification
Detect missed screenings, follow-ups, or medication adherence issues across systems.
Here’s the shift that matters.
Care Everywhere started as a data access layer.
It is evolving into a decision intelligence platform.
But only if you extend it.
Organizations that stop at native capabilities get visibility.
Organizations that extend it get actionable insight, automation, and measurable ROI.
The future of interoperability is not just connected data. It is interpreted, prioritized, and operationalized data delivered exactly when clinicians need it.
IX. How Mindbowser Builds Custom EHR with Epic Integration Capabilities
Epic is powerful. But it is not complete on its own.
Most health systems treat Epic as a closed environment. That mindset limits what interoperability can actually deliver.
We take a different approach.
At Mindbowser, Epic is not the endpoint. It is the foundation of a connected care platform tailored to your workflows.
A. Our Positioning: Extend, Don’t Replace
We do not replace Epic.
We help extend it.
That means:
- Preserving your existing workflows
- Enhancing interoperability across systems
- Turning static data into actionable intelligence
The goal is simple: make Epic work the way your organization actually operates.
B. What We Build: Custom Interoperability Layers
We help extend integration layers that sit on top of Epic and connect it to the broader ecosystem.
Core capabilities include:
1. FHIR API Integrations
Enable real-time, flexible data exchange across modern applications and non-Epic systems.
2. HL7 Integrations
Support legacy environments while ensuring continuity across existing infrastructure.
3. SMART on FHIR Applications
Embed custom apps directly into clinician workflows inside Epic.
This ensures adoption without disrupting usability.
C. Middleware for Data Normalization and Aggregation
Data from multiple sources is only useful if it is consistent.
We support organizations by:
- Normalizing data across systems
- Aggregating multi-source patient records
- Ensuring consistency for clinical decision-making
This removes the burden from clinicians.
D. AI-Powered Clinical Modules
This is where interoperability becomes intelligence.
We help enable integration use cases such as:
- Clinical summarization (AI Medical Summary)
- Readmission prediction (AI Readmission Risk)
These models:
- Analyze data from Care Everywhere and other sources
- Highlight critical insights
- Support faster, more informed decisions
Instead of reading everything, clinicians see what matters.
E. Integration Across the Digital Health Stack
We help organizations connect Epic beyond traditional boundaries:
- Epic Care Everywhere + external HIEs
- Epic + Salesforce Health Cloud
- Epic + Remote Patient Monitoring platforms (WearConnect, RPMCheck AI)
This creates a unified, longitudinal patient view across touchpoints.
F. Real-World Outcomes
Health systems adopting these approaches often see measurable impact:
- Faster clinician decision times
- Reduced manual reconciliation effort
- Improved interoperability with non-Epic ecosystems
This is the shift.
From EHR → to platform
From data → to intelligence
From access → to action
So the question becomes:
Are you using Epic as a system of record or evolving it into a system of insight?
The value of Care Everywhere multiplies when you extend it with custom integrations, AI, and workflow-driven design.
X. Implementation Checklist for CIOs Evaluating Care Everywhere
Before you invest more, pause and assess.
Many organizations “have” Care Everywhere. Fewer are actually using it effectively.
The difference shows up in outcomes, not implementation status.
This checklist helps you evaluate where you stand and what needs to change.
A. Key Strategic Questions
Start with reality, not assumptions.
1. Are Clinicians Actively Using Care Everywhere?
Or are they bypassing it?
Adoption is the first signal.
- Low usage often means workflow friction
- High usage with low impact signals poor data quality
Usage without value is a red flag.
2. Is Reconciliation Manual or Assisted?
Manual reconciliation slows everything down.
- Are clinicians manually reviewing every external record?
- Is there any automation or prioritization?
If it is fully manual, scalability is limited.
3. How Well Does It Integrate with Non-Epic Systems?
Most environments are hybrid.
- Are you capturing data from non-Epic providers?
- Is that data usable or fragmented?
Interoperability that excludes part of your network is incomplete.
4. Are You Leveraging FHIR for Extensions?
FHIR is no longer optional.
- Are APIs being used for external integrations?
- Are third-party apps embedded into workflows?
If not, your interoperability layer is static.
B. Readiness Checklist for Optimization
Beyond questions, you need structural readiness.
1. Data Governance Framework
Clear policies for:
- Data accuracy
- Source validation
- Usage standards
Without governance, trust breaks.
2. Consent Management Policies
Interoperability must align with:
- Regulatory requirements
- Patient consent preferences
- Cross-organization agreements
Compliance is not optional. It is foundational.
3. Integration Architecture Maturity
Evaluate your stack:
- Legacy HL7 vs modern FHIR mix
- Middleware capabilities
- Data normalization processes
The architecture defines what is possible.
4. AI and Automation Roadmap
Are you planning for intelligence or just access?
- Clinical summarization
- Automated reconciliation
- Predictive analytics
Organizations that plan early move faster.
Here’s the key insight.
Implementation is not the milestone.
Adoption, usability, and extension define success.
So ask yourself: Are you measuring deployment or outcomes?
A structured evaluation reveals whether Care Everywhere is delivering value or merely serving as infrastructure. The gap between those two is where transformation happens.
XI. Future of Epic Interoperability (What’s Next)
The next phase of interoperability is not about access. It is about intelligence.
Care Everywhere solved the first problem: getting data across organizations.
Now the industry is shifting toward making that data actionable, predictive, and embedded deeper into care delivery.
So what comes next?
A. FHIR-First Interoperability Becomes Standard
FHIR is moving from “emerging” to expected.
Health systems are adopting FHIR to:
- Enable real-time integrations
- Support third-party innovation
- Reduce dependency on legacy HL7 structures
This shifts interoperability from document exchange to data fluidity.
B. TEFCA and Nationwide Data Exchange
The Trusted Exchange Framework and Common Agreement (TEFCA) is expanding interoperability at a national level.
This means:
- Broader data sharing across networks
- Standardized exchange frameworks
- Reduced fragmentation between systems
Interoperability is no longer organization-to-organization. It is becoming network-to-network.
C. AI-Driven Clinical Insights from Exchanged Data
Here’s where things change fast.
Instead of clinicians reviewing raw external data, AI will:
- Summarize patient histories automatically
- Highlight critical risks
- Recommend next-best actions
Data becomes guidance, not just information.
According to McKinsey, AI-driven healthcare solutions could unlock significant improvements in both clinical outcomes and cost efficiency.
D. Growth of Patient-Mediated Data Exchange
Patients are gaining more control over their data.
With tools like Share Everywhere and API-driven apps:
- Patients can share records across providers
- Data moves with the patient, not the system
- Continuity improves across geographies
The patient becomes an active node in the interoperability network.
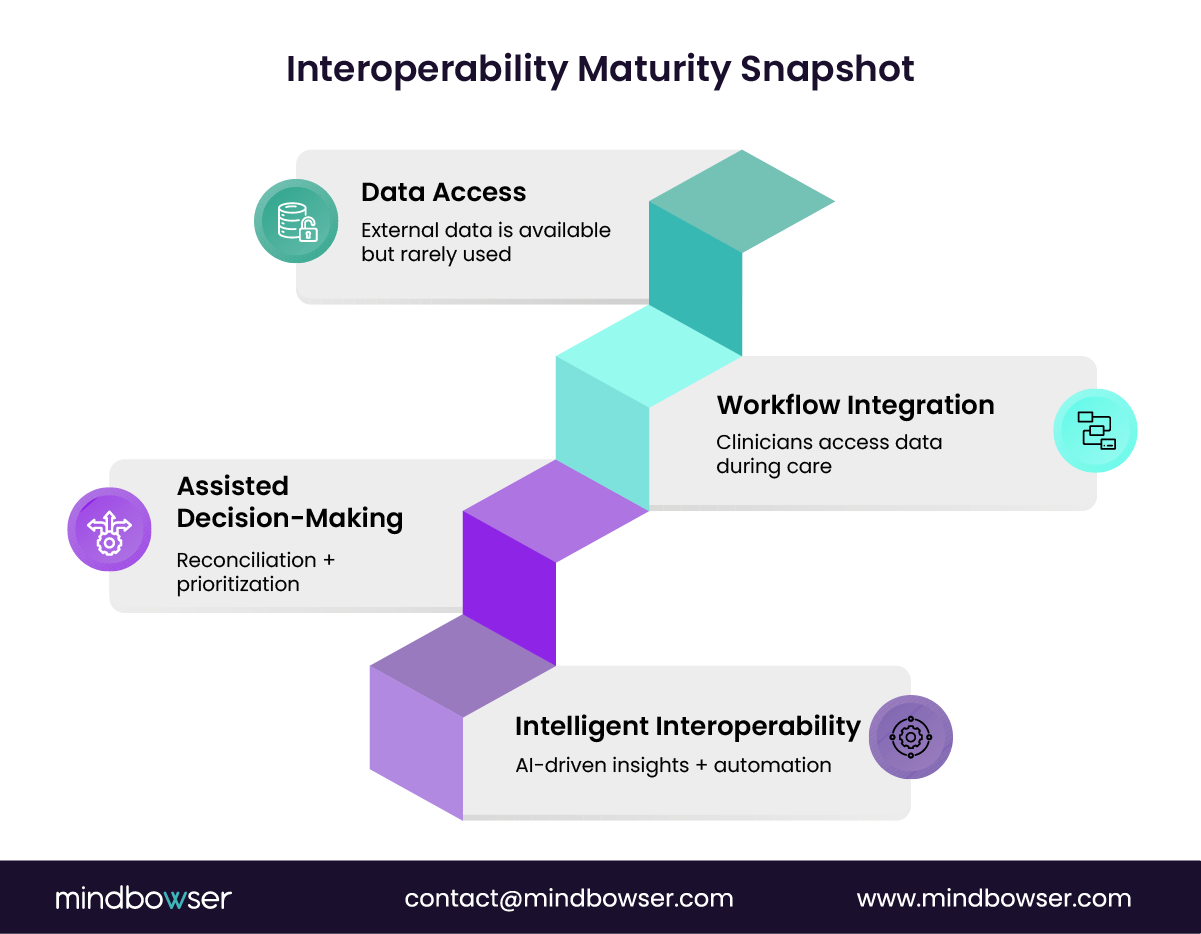
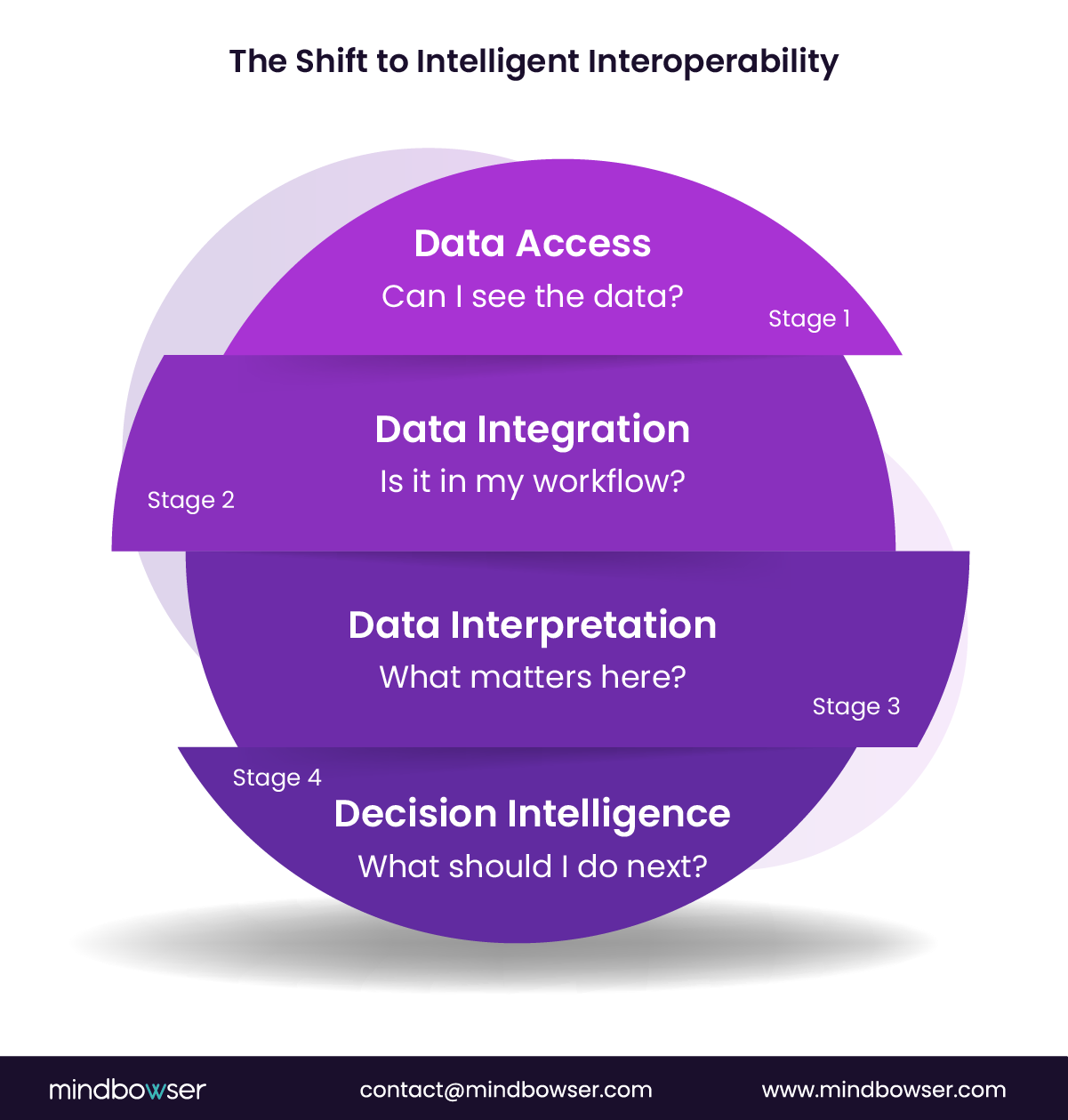
E. From Interoperability to “Intelligent Interoperability”
This is the real shift.
- Past → Access to data
- Present → Integration into workflows
- Future → Actionable intelligence at the point of care
Systems will not just show data. They will interpret it.
Before you move forward, ask this:
Are you building for today’s interoperability or preparing for what it will become over the next 2–3 years?
Unlock faster care decisions today
XII. The Strategic Shift Healthcare Leaders Can’t Ignore
Interoperability has crossed a threshold.
It is no longer an IT initiative. It is a clinical, operational, and financial lever.
Care Everywhere plays a central role, but only when used fully and extended intelligently.
Here is the reality most leaders face:
- Data is available, but not always usable
- Workflows exist, but are not always optimized
- Tools are deployed, but not always adopted
The gap is not technology. It is execution.
Organizations that succeed will:
- Treat interoperability as a system, not a feature
- Extend Epic beyond native capabilities
- Embed intelligence into clinical workflows
- Reduce burden, not increase it
Those that don’t will:
- Struggle with fragmented data
- See low clinician adoption
- Miss expected ROI
The difference is not subtle. It shows up in cost, quality, and speed.
Epic Care Everywhere gives you visibility.
What you build on top of it determines whether you achieve true connected care.
The future belongs to organizations that move from data exchange → to decision intelligence → to workflow transformation.
From Data Access to Clinical Intelligence
Epic Care Everywhere has moved interoperability from theory into daily clinical reality by bringing external patient data directly into workflows where decisions happen.
It reduces duplication, improves safety, and enables faster care, but only when actively used and thoughtfully extended.
The real opportunity lies beyond access: health systems that layer in FHIR integrations, automation, and AI-driven insights transform fragmented data into actionable intelligence.
Those who don’t risk turning a powerful capability into a passive viewer. In the end, success comes down to this: not whether you have Care Everywhere, but whether you’ve evolved it into a system that drives decisions, not just displays data.
Epic Care Everywhere enables real-time sharing of patient data across healthcare organizations. It helps clinicians access external records like medications, labs, and notes directly within their workflow, improving decision speed and care continuity.
Unlike standalone HIEs, Care Everywhere is embedded inside Epic workflows. Clinicians don’t need to log into separate systems, which increases adoption and makes data immediately usable during care delivery.
Yes, but with limitations. Integration with non-Epic systems often depends on FHIR APIs, HL7 interfaces, or custom integrations, and data quality can vary across sources.
Common challenges include manual data reconciliation, inconsistent data formats, and limited interoperability with non-Epic environments . Without optimization, it can become a passive data viewer.
Organizations should extend Care Everywhere using FHIR integrations, AI-driven summarization, and workflow automation. This turns raw data into actionable insights and improves both clinical and financial outcomes.